

Abstract
Background:
Neonatal hypoglycemia is more prevalent and can cause severe neurological sequelae. The objective of this study was to assess the patterns of neuroradiologic changes in neonatal hypoglycemia.
Methods:
A retrospective cohort study was conducted on 66 neonatal hypoglycemia patients, and the magnetic resonance imaging (MRI) and clinical records were reviewed.
Results:
Magnetic resonance imaging showed evidences of abnormality in 54.54% (36 of 66) of hypoglycemic infants. The most common abnormal findings were located on the parietal and occipital lobes of the brains. The number of days with hypoglycemia was significantly higher for abnormal MRI infants (P < .001), and prolonged/recurrent hypoglycemia was remarkably distinguished for abnormal MRI infants (P < .001). Patients with abnormal MRI findings did not have a lower blood glucose than infants without abnormal MRI findings (P > .05), but the lowest blood glucose was significantly lower for the patients with seizures (P < .01).
Conclusions:
The pattern of bilateral occipital cortical injury is the most common abnormality for neonatal hypoglycemia. The number of days with hypoglycemia, not the lower blood glucose, was significantly related to abnormal MRI infants.
Keywords: Hypoglycemia, neonate, magnetic resonance imaging, brain injury
Introduction
At birth, the glucose provides the newborn baby with approximately half the total energy needs, and glucose is a vital fuel for the brain metabolism. Blood sugar level has been measured in neonatal infants for more than 100 years, and the neonatal hypoglycemia was first reported 80 years ago.1 However, the definition of neonatal hypoglycemia remains controversial and there is a lack of rational evidence.2 The usual distribution of neonatal blood glucose concentrations varies with birth weight, postnatal age, nutritional intake, and other factors. Clinical signs occur in some but not all babies with low blood glucose concentrations, but such signs lack specificity.
Recently, Tam et al3 report that neonatal hypoglycemia (glucose <2.6 mmol/L) was associated with 3.72-fold increased odds of neonatal encephalopathy and with 4.82-fold increased odds of increased adverse motor and cognitive outcomes. Moreover, hypoglycemia in infants can be associated with brain damage such as seizures, developmental delay, or long-term neuronal loss, and frequently occurs in neonatal infants with birth asphyxia, diabetic mothers, or low birth weight for gestational age (GA).4 Many babies with low blood sugar have no clinical symptoms, while others have symptoms that can cause permanent brain damage. Previous reports indicated that magnetic resonance imaging (MRI) test could help to identify the differential diagnoses to hypoglycemic brain damage5 and had higher positive predictive values for the hypoglycemia.6 However, the abnormal imaging findings in hypoglycemia of newborn might be more common seen than the insult suspected, and symptomatic neonatal hypoglycemia after observed damage on MRI features are various, and the severity of hypoglycemia was not significantly related to specific injury characteristics on MRI.7 Due to the risk factors of hypoglycemia such as preterm, small for GA or intrauterine growth retardation, maternal diabetes mellitus or large for GA, neonatal hypoglycemia is prone to occur and needs to be closely managed. Therefore, as discussed in this study, neonatal hypoglycemia is more common than is believed and may lead to more serious neurological sequelae. The purpose of this study was to evaluate the neuroimaging characteristics and special radiographic characteristics of hypoglycemia in neonates.
Patients and Methods
All the infants who were admitted to the neonatal department of the Children’s hospital, Zhejiang University School of Medicine, with at least 1 episode of hypoglycemia, were imaged. Our study was approved by the Hospital’s Ethics Committee. Every patient has a statement of informed consent of parents for this study. Between June 2013 and June 2015, 66 cases of neonatal hypoglycemia were enrolled and underwent MRI and cranial ultrasound (US) study. Blood glucose concentration was monitored 30 minutes after admission, once every 3 to 4 hours before feeds for the first day of hospitalization and once every 6 to 8 hours after the second day. The length of time to continue screening depended on the glucose level measured and the etiology of hypoglycemia. Hypoglycemia was defined as blood or plasma glucose level ⩽2.6 mmol/L,8 and infusion of glucose at a rate of 6 to 8 mg/kg/min, rechecked glucose level 30 minutes after intravenous (IV) bolus, and then hourly until stable, to determine whether additional therapy was needed. The glucose level, duration of blood glucose instability, and any clinical manifestations were recorded. Transient hypoglycemia was defined if it resolved spontaneously or responded to the first intervention, and prolonged/recurrent hypoglycemia was defined if it did not resolve after intervention within 3 days. Clinical manifestations included poor feeding, vomiting, jitteriness or irritability, cyanosis, seizures, high-pitched cry, and apnea. Other relevant information and data taken from patients’ charts included infant GA, birth weight, birth length, Apgar scores at 1 and 5 minutes, lowest serum glucose, and clinical manifestation. The patient charts and cranial MRI or US imaging studies of 66 patients were reviewed retrospectively.
Magnetic resonance imaging
Magnetic resonance imaging scans were performed in the first week after admission using a 1.5 Siemens Magnetom magnetic resonance system (Siemens AG, Erlangen, Germany). The infants were imaged during postprandial sleep under sedation with Chloral hydrate. Magnetic resonance imaging scans included sagittal T1 weighted (repetition time/echo time [TR/TE], 500/8.4 ms), T2 weighted (TR/TE 4000/89 ms), fluid-attenuated inversion recovery (FLAIR) sequences, and diffusion-weighted imaging (DWI), and the location and extent of abnormal signals in the brain were also recorded. Patients with other severe anomalies were excluded from the study, such as severe hydrocephalus, macrogyrus, cortical dysplasia, or other severe brain malformations. The findings were read separately by neuroradiologist, and the radiologic diagnosis was made without any information of the laboratory glucose values.
Ultrasonography
All patients went through initial cranial US scans through the anterior fontanelle. Scans were performed by an experienced pediatric radiologist using a Philips scanner (Philips Medical Systems, Best, The Netherlands) with a transducer frequency of 7 MHz during the first week after admission.
Statistical analyses
The clinical features from the abnormal MRI cases and the normal MRI cases were compared by chi-square test, Fisher exact test, or Student t test when appropriate. The Mann-WhitneyU test was used for variables with a nonnormal distribution. Statistical significance was set at P < .05.
Results
Clinical data
A total of 66 neonatal infants with hypoglycemia were studied. The age of the infants was 1 to 22 days. Of the 66 infants, 8 were premature and 58 were full term, and the mean GA at birth was 38.52 ± 1.71 weeks. The 8 preterm babies were not very preterm, and the range of GA was 35 to 36 weeks. Patients were male in 42 cases (63.6%) and female in 24 cases (36.4%), and the male to female ratio was 1.75:1. Mean birth weight of the whole cases was 3155.70 ± 847.70 g, and mean birth length was 49.09 ± 2.98 cm. As to the cause of hypoglycemia, 4 cases were eventually identified as neonatal hyperinsulinemia; 8 cases were estimated to have limited glycogen stores associated with prematurity; 1 patient was related to have genetic metabolic encephalopathy disorder, and the diagnosis was glutaric acidemia type II; and the rest were suggested to have inadequate stores of glycogen and gluconeogenic precursors subsequent to intrauterine growth restriction: 16 cases were SGA (small for gestational age) and the others (37 cases) had poor feeding.
Prolonged/recurrent hypoglycemia was diagnosed in 34 cases, and the duration of hypoglycemia ranged from 3 to 18 days. Moreover, in all 66 hypoglycemic patients, 30 infants were defined as severe hypoglycemia and their lowest blood glucose was less than 1.5 mmol/L.
Neuroimaging
The median age of MRI scan was 9 days (range: 1-28 days); 36 of 66 hypoglycemic infants (54.54%) had abnormal MRI. The neuroimaging studies have shown significant brain damage, typically involving the parietal and occipital lobes of the brain hemisphere; 20 of 66 hypoglycemic infants (30.30%) had abnormal cranial sonography during admission period; and 14 of 66 cases (21.21%) had subependymal cysts. No relation was found between the preterm infants (4/36, 11.11% vs 4/30, 13.33%; P = 1.000) or SGA (10/36, 27.78% vs 6/30, 20.20%; P = .463) and the abnormal MRI findings (Table 1).
Table 1.
Clinical features of the hypoglycemic patients between abnormal MRI and normal MRI.
| Clinical features | Abnormal MRI (n = 36) | Normal MRI (n = 30) | χ2
t/z |
P |
|---|---|---|---|---|
| Sex | ||||
| Male, n (%) | 26 (72.22%) | 16 (53.33%) | 2.523 | .112 |
| Female, n (%) | 10 (27.78%) | 14 (46.67%) | – | – |
| Birth weight (g) | 3001.11 ± 743.36 | 3341.33 ± 923.91 | 1.658 | .102 |
| Birth length (cm) | 48.72 ± 3.56 | 49.53 ± 1.99 | 1.165 | .249 |
| Gestational age (weeks) | 38.44 ± 1.80 | 38.60 ± 1.61 | 0.367 | .715 |
| SGA, n (%) | 10 (27.78%) | 6 (20.00%) | 0.539 | .463 |
| Preterm, n (%) | 4 (11.11%) | 4 (13.33%) | – | 1.000 |
| 1-minute Apgar scores | 8.72 ± 1.54 | 9.27 ± 0.58 | 1.826 | .072 |
| 5-minute Apgar scores | 9.50 ± 1.34 | 9.87 ± 0.35 | 1.602 | .117 |
| Number of days with hypoglycemia (day) | 1.00 (1.00-18.00) | 1.00 (0.04-3.00) | 3.548 | <.001 |
| Lowest serum glucose (mmol/L) | 1.52 ± 0.36 | 1.69 ± 0.39 | 1.929 | .058 |
| Severe hypoglycemia (<1.5 mmol/L), n (%) | 20 (55.56%) | 10 (33.33%) | 3.259 | .071 |
| Prolonged/recurrent hypoglycemia | 26 (72.22%) | 8 (26.67%) | 13.596 | <.001 |
| Cranial US findings | ||||
| Normal | 26 (72.22%) | 20 (66.67%) | 0.239 | .625 |
| Abnormal | 10 (27.78%) | 10 (33.33%) | – | – |
| Poor feeding | 12 (33.33%) | 6 (20.00%) | 1.467 | .226 |
| Irritability | 26 (72.22%) | 10 (33.33%) | 9.981 | .002 |
| Cyanosis | 10 (27.78%) | 8 (26.67%) | 0.010 | .920 |
| Seizures | 10 (27.78%) | 2 (6.67%) | 4.902 | .027 |
| Vomiting | 4 (11.11%) | 0 (0.00%) | – | .120 |
| High-pitched cry | 2 (5.56%) | 4 (13.33%) | – | .399 |
| Apnea | 8 (22.22%) | 0 (0.00%) | – | .006 |
Abbreviations: MRI, magnetic resonance imaging; SGA, small for gestational age; US, ultrasound.
Variables with normally distribution were described as mean ± standard deviation; variables with a nonnormal distribution were described as median and range; categorical variables were described as number and percentage.
Patterns of injury
Normal findings
In total, 30 patients with neonatal hypoglycemia showed normal MRI performance, 46 hypoglycemia cases had normal US findings, and 20 cases had all the normal findings. The rate of normal findings was higher for US (46/66, 69.70% vs 30/66, 45.45%; P = .625), but the difference was not statistically significant.
Abnormal findings
Most of the infants had some changes of white matter (WM); 4 infants (4/66, 6.06%) with severe WM injury had focal hemorrhage. All cases with WM injury showed lesions in the occipital and parietal lobe (Figure 1); 22 cases with moderate abnormality in high signal, and 12 cases with severe changes in the posterior WM; 14 infants (14/66, 21.21%) had abnormal signal intensity, associated with cortical infarction and hemorrhage. They were more likely adjacent to WM injury. Moreover, 6 infants (6/66, 9.09%) presented different degrees of basal ganglia abnormal signals and had an abnormal appearance in the posterior limb of the internal capsule (PLIC) (Figures 2 and 3). Injury in other parts of the brain was not so common; 1 had abnormal small cerebellum vermis and 1 had small hematoma on the right side of the scalp.
Figure 1.
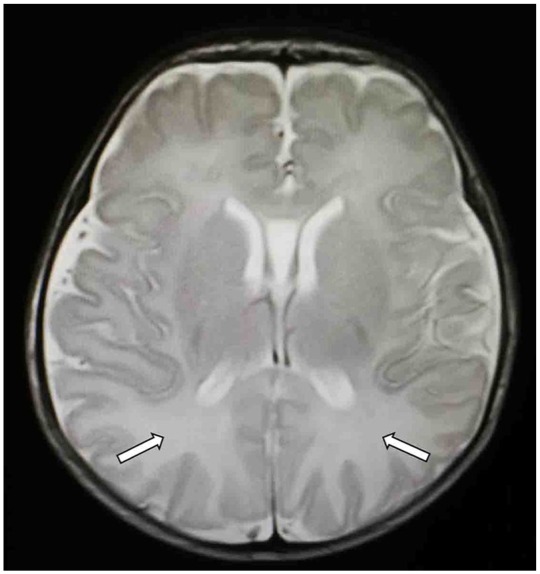
T2-weighted MRI scan in the transverse plane obtained 13 days after birth; GA: 34 weeks. There is multiple abnormal high signal white matter differentiation bilaterally in the posterior parietal and occipital lobes. GA indicates gestational age; MRI, magnetic resonance imaging.
Figure 2.
T2-weighted MRI scan in the transverse plane obtained 7 days after birth; GA: 40 weeks. Image showed abnormal hyperintensity in the globus pallidus and mixed hypointensity and hyperintensity in the occipital cortex and white matter. GA indicates gestational age; MRI, magnetic resonance imaging.
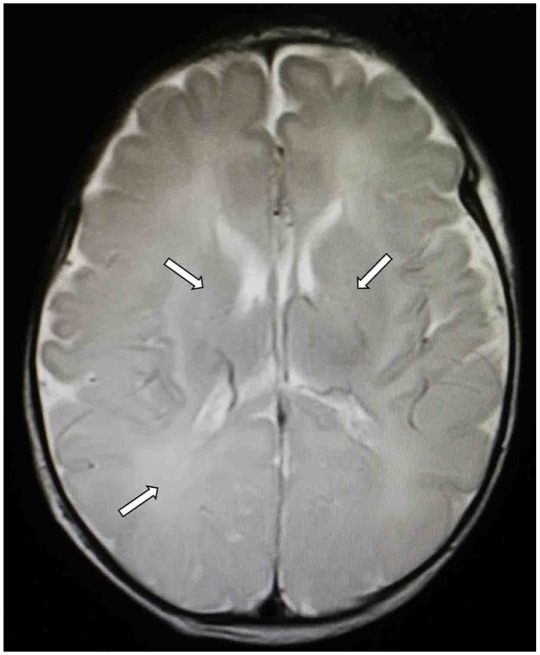
Figure 3.

MRI of the patient born at postconceptional age of 40 weeks, MRI performed at age of 5 days. Abnormal hyperintensity (white arrow) is presented in the corpus callosum, posterior limb of the internal capsule, occipital cerebral cortex, and posterior white matter on DWI. DWI indicates diffusion-weighted imaging; MRI, magnetic resonance imaging.
Brain injury and severe hypoglycemia
The mean level of lowest blood glucose was 1.60 ± 0.38 mmol/L (range: 0.8-2.3 mmol/L), and 30 infants had severe hypoglycemia (blood glucose <1.5 mmol/L) (Table 1). When comparison was made among abnormal MRI infants (n = 36) and the normal MRI infants (n = 30), the number of days with hypoglycemia was significantly higher for abnormal MRI infants (mean day: 3.39 ± 4.20 vs 1.01 ± 0.80; median day: 1.00 [1.00-18.00 days] vs 1.0 day [0.04-3.00 days]; P < .001). However, patients with abnormal MRI findings did not have a lower blood glucose (1.52 ± 0.36 vs 1.69 ± 0.39 mmol/L, P = .058) and did not have severe hypoglycemia (the lowest blood glucose < 1.5 mmol/L) (20/36, 55.56% vs 10/30, 33.33%; P = .071) more frequently as compared with patients with normal MRI findings. Moreover, there was also no difference in sex, gestation age, birth weight, birth length, and Apgar scores (1 or 5 minutes) between the patients with and without abnormal MRI findings (P > .05); 32 neonates showed transient hypoglycemia and responded quickly to treatment and the other 34 cases were prolonged or recurrent. Although we found the number of days with hypoglycemia was strongly related to abnormalities in MRI findings, our study also clarified that the MRI features for infants with transient versus infants with prolonged/recurrent hypoglycemia were remarkably distinguished (26/36, 72.22% vs 8/30, 26.67%; P < .001).
Brain injury and seizures
Moreover, 12 infants were documented to have experienced seizures over several days: 10 of them had moderate WM injury and basal ganglia involvement (Table 1), and 2 had normal MRI findings. When comparing patients with (n = 12) and without (n = 54) seizures, the lowest serum glucose was significantly lower for the former (1.22 ± 0.22 vs 1.68 ± 0.36 mmol/L; P < .001). Infants with abnormal MRI findings were more likely to have experienced seizures (10/36, 27.78% vs 2/30, 6.67%; P = .027), and these findings were statistically significant. Moreover, there was no difference in other clinical features such as poor feeding, cyanosis, vomiting, and high-pitched cry between the patients with and without abnormal MRI findings (P > .05), but irritability and apnea were found statistically significant (irritability: 26/36, 72.33% vs 10/30, 33.33%; P = .002; apnea: 8/36, 22.22% vs 0/30, 0%; P = .006).
Discussion
The failure of metabolic adaptation after birth is the most common cause of neonatal hypoglycemia. There is no principally “safe” blood glucose level for newborns, and in 2000, Cornblath et al9 recommended the use of an “operational threshold” for blood glucose management in neonatal infants. In addition, as mentioned earlier, inadequate control of neonatal hypoglycemia can lead to adverse neurological consequences, including severe psychomotor retardation and epilepsy.10 However, so far, the number of low blood sugar levels or the duration that can lead to a baby’s brain damage is still unclear,11 and there is no single value to determine whether it can cause brain damage.
There are few studies on the characteristics of cerebral histopathological changes in neonatal hypoglycemia, and the characteristics of neuroradiological changes after severe hypoglycemia injury in adults are different from those of neonatal brain injury.12 Adult hypoglycemic encephalopathy was characterized by bilateral distribution in the basal ganglia, hippocampus, temporal and occipital gray matter of the brain cortex, and/or the substantia nigra, and these lesions in the acute phase on T1-weighted and T2-weighted images were characterized by hypointensity and hyperintensity, respectively.13 Early imaging examination of neonatal hypoglycemia is important for early detection and prognosis evaluation of brain injury.14 Moreover, Arhan et al15 found the results of MRI in the patients who developed epilepsy after neonatal hypoglycemia at the median age of 1.5 years, and the neuroradiological findings were gliosis in occipital WM bilaterally, occipital cortical atrophy, gliosis in the parietal WM, parietal cortical atrophy, or pulvinar scarring. This is different from the neonatal period. Thus, diffusion imaging could detect lesions more early in neonatal hypoglycemic patients, while later hypoglycemic brain damage could assess using FLAIR and T2-weighted images.
Neonatal hypoglycemia is closely associated with extensive later cortical thinning, especially in the occipital lobe, which can be confirmed by computed tomography or MRI.16 Kinnala et al17 reported MRI found that 39% babies with hypoglycemia had abnormal imaging, and the brain abnormalities detected by MRI were more significant than those detected by US. Ultrasonography is less sensitive to cerebral cortex damage, and other studies have reported that MRI is superior in detecting non-hemorrhagic brain parenchyma damage.18 This is mainly because MRI is more sensitive to detect diffuse lesions and WM abnormalities, as well as its ability to show small structural changes, neuronal migration disorders, delays, or myelin abnormalities.19 Therefore, the parieto-occipital injuries caused by hypoglycemia in neonates are difficult to be detected by US.19 In recent years, studies have been conducted on the vulnerability of the WM and cortex of the posterior parietal and occipital lobes, and it is found that this site is more likely to be damaged in neonatal hypoglycemia. It was also believed that the damage in parietal and occipital cortex and subcortical WM may be the most serious one.20 Cakmakci et al21 also reported that MRI showed T1 and T2 shortening of WM lesions in the occipital and frontal lobes. MRI abnormalities in the occipital region were consistent with previous studies on transient neonatal hypoglycemia.17
According to these studies, hypoglycemia in newborns can cause delayed myelination, especially in the parieto-occipital lobe; deep WM; and periventricular WM, and even lead to cortical atrophy, especially in the occipital lobe.22,23 Alkalay et al22 found that 82% hypoglycemia infants had imaging manifestations and neurological sequelae of the occipital lobe, 50% had visual abnormalities, and 26% infants had transient brain edema. We testified that MRI can accurately distinguish the changes of brain injury caused by hypoglycemia. Therefore, imaging studies have become an important tool for the diagnosis and prognosis of hypoglycemia brain injury.
The severity of hypoglycemia and the duration of persistent hypoglycemia were not consistent with the characteristics of specific brain injury on MRI.7 In our result, we also found patients with abnormal MRI findings did not have lower blood glucose and did not have severe hypoglycemia. However, we found the number of days with hypoglycemia was significantly higher for abnormal MRI infants. Moreover, there was also no difference in sex, gestation age, birth weight, birth length, and 1- or 5-minute Apgar scores between the patients with and without abnormal MRI findings. In our research, the lowest serum glucose was significantly lower for the patients with seizures, and the infants with abnormal MRI findings had shown a greater likelihood of seizures. Therefore, for patients with seizures, the MRI examination should be performed as early as possible to detect the extent of brain damage. Babies with abnormal MRI results should be closely followed to improve the neurodevelopmental status and prognosis. Moreover, we also found that there was no difference in other clinical features such as poor feeding, cyanosis, vomiting, and high-pitched cry between the patients with and without abnormal MRI findings, although irritability or apnea was found statistically significant. Thus, the clinical presentation of hypoglycemia may not be associated with the injury on MRI.
Conclusions
We have described the imaging findings in 66 cases of neonatal hypoglycemia. The most common observed abnormal findings were injury primarily to the parietal and occipital lobes, and some abnormalities are located on the posterior aspects of the cerebral cortex associated with periventricular WM lesions. However, in this observational study, a lack of sample size and the lack of a healthy control group may affect the accuracy of the results, and our results did not allow drawing conclusions on causality. Moreover, the 66 cases were not followed up for assessment of long-term outcome, and further research requires greater numbers and an understanding of the implications of these findings for optimal cognitive and motor function to predict the outcome of proper clinical context.
Footnotes
Funding:The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grants from National Natural Science Foundation of China (81571466) and sponsored by Zhejiang Provincial Program for the Cultivation of High-Level Innovative Health Talents.
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions: M-HG and FA contributed to conception and design, acquisition of data,analysis, drafting, revision and final approval. T-MY contributed to conception and design, analysis, drafting revision and final approval of the manuscript. All authors critically revising article and approved the final manuscript.
ORCID iD: Tian-Ming Yuan  https://orcid.org/0000-0003-2593-606X
https://orcid.org/0000-0003-2593-606X
References
- 1. Cornblath M. Neonatal hypoglycemia 30 years later: does it injure the brain? historical summary and present challenges. Acta Paediatr Jpn. 1997;39:S7-S11. [PubMed] [Google Scholar]
- 2. Sinclair JC. Approaches to the definition of neonatal hypoglycemia. Acta Paediatr Jpn. 1997;39:S17-S20. [PubMed] [Google Scholar]
- 3. Tam EW, Haeusslein LA, Bonifacio SL, et al. Hypoglycemia is associated with increased risk for brain injury and adverse neurodevelopmental outcome in neonates at risk for encephalopathy. J Pediatr. 2012;161:88-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Rozance PJ. Update on neonatal hypoglycemia. Curr Opin Endocrinol Diabetes Obes. 2014;21:45-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Boardman JP, Wusthoff CJ, Cowan FM. Hypoglycaemia and neonatal brain injury. Arch Dis Child Educ Pract Ed. 2013;98:2-6. [DOI] [PubMed] [Google Scholar]
- 6. Wong DS, Poskitt KJ, Chau V, et al. Brain injury patterns in hypoglycemia in neonatal encephalopathy. Am J Neuroradiol. 2013;34:1456-1461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Burns CM, Rutherford MA, Boardman JP, Cowan FM. Patterns of cerebral injury and neurodevelopmental outcomes after symptomatic neonatal hypoglycemia. Pediatrics. 2008;122:65-74. [DOI] [PubMed] [Google Scholar]
- 8. Cloherty JP, Eichenwald EC, Hansen AR, Stark AR. Manual of Neonatal Care. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:284-285. [Google Scholar]
- 9. Cornblath M, Hawdon JM, Williams AF, et al. Controversies regarding definition of neonatal hypoglycemia: suggested operational thresholds. Pediatrics. 2000;105:1141-1145. [DOI] [PubMed] [Google Scholar]
- 10. Menni F, de Lonlay P, Sevin C, et al. Neurologic outcomes of 90 neonates and infants with persistent hyperinsulinemic hypoglycemia. Pediatrics. 2001;107: 476-479. [DOI] [PubMed] [Google Scholar]
- 11. Boluyt N, van Kempen A, Offringa M. Neurodevelopment after neonatal hypoglycemia: a systematic review and design of an optimal future study. Pediatrics. 2006;117:2231-2243. [DOI] [PubMed] [Google Scholar]
- 12. Lee BW, Jin ES, Hwang HS, Yoo HJ, Jeong JH. A case of hypoglycemic brain injuries with cortical laminar necrosis. J Korean Med Sci. 2010;25:961-965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Fujioka M, Okuchi K, Hiramatsu KI, Sakaki T, Sakaguchi S, Ishii Y. Specific changes in human brain after hypoglycemic injury. Stroke. 1997;28:584-587. [DOI] [PubMed] [Google Scholar]
- 14. Finelli PF. Diffusion-weighted MR in hypoglycemic coma. Neurology. 2001;57:933. [DOI] [PubMed] [Google Scholar]
- 15. Arhan E, Öztürk Z, Serdaroğlu A, Aydın K, Hirfanoğlu T, Akbaş Y. Neonatal hypoglycemia: a wide range of electroclinical manifestations and seizure outcomes. Eur J Paediatr Neurol. 2017;21:738-744. [DOI] [PubMed] [Google Scholar]
- 16. Spar JA, Lewine JD, Orrison WW., Jr. Neonatal hypoglycemia: CT and MR findings. Am J Neuroradiol. 1994;15:1477-1478. [PMC free article] [PubMed] [Google Scholar]
- 17. Kinnala A, Rikalainen H, Lapinleimu H, Parkkola R, Kormano M, Kero P. Cerebral magnetic resonance imaging and ultrasonography findings after neonatal hypoglycemia. Pediatrics. 1999;103:724-729. [DOI] [PubMed] [Google Scholar]
- 18. Hung PC, Wang HS. Hemimegalencephaly: cranial sonographic findings in neonates. J Clin Ultrasound. 2005;33:243-247. [DOI] [PubMed] [Google Scholar]
- 19. Barkovich AJ. The encephalopathic neonate: choosing the proper imaging technique. Am J Neuroradiol. 1997;18:1816-1820. [PMC free article] [PubMed] [Google Scholar]
- 20. Barkovich AJ, Ali FA, Rowley HA, Bass N. Imaging patterns of neonatal hypoglycemia. Am J Neuroradiol. 1998;19:523-528. [PMC free article] [PubMed] [Google Scholar]
- 21. Cakmakci H, Usal C, Karabay N, Kovanlikaya A. Transient neonatal hypoglycemia: cranial US and MRI findings. Eur Radiol. 2001;11:2585-2588. [DOI] [PubMed] [Google Scholar]
- 22. Alkalay AL, Flores-Sarnat L, Sarnat HB, Moser FG, Simmons CF. Brain imaging findings in neonatal hypoglycemia: case report and review of 23 cases. Clin Pediatr (Phila). 2005;44:783-790. [DOI] [PubMed] [Google Scholar]
- 23. Yalnizoglu D, Haliloglu G, Turanli G, Cila A, Topcu M. Neurologic outcome in patients with MRI pattern of damage typical for neonatal hypoglycemia. Brain Dev. 2007;29:285-292. [DOI] [PubMed] [Google Scholar]