

Abstract
Introduction:
Deep vein thrombosis (DVT) is a common cause of admission to the emergency departments (ED). Doppler ultrasonography of the entire lower limb is the first-line imaging modality. But most EDs do not access to full-time radiologists which can lead to delayed diagnosis.
Aim:
The aim of this study was to evaluate the diagnostic accuracy of three-point compression ultrasonography performed by emergency medicine resident for diagnosis of DVT.
Methods:
This prospective diagnostic study was carried out at Imam Khomeini Hospital in Sari from March 2018 to November 2018. For all patients with suspected lower extremity DVT, first bedside 3-point compression ultrasound were performed by a third year emergency medicine resident at ED. Then Doppler ultrasonography were performed by a radiologist in the radiology department, as a reference test. Sensitivity, specificity, and positive predictive value of the three-point compression ultrasound performed by emergency medicine resident was calculated.
Results:
Of the 72 patients enrolled in our study, 50% of the patients were male, with an average age of 36±19 years. The mean of patient admission time to perform ultrasonography by an emergency medicine resident and radiologist were 14.05±19 and 216±140.1 minutes, respectively. The two groups had a statistically significant difference (P<0.0001). In ultrasonography performed by emergency medicine resident and doper ultrasonography by radiologist, 91.67% and 36.1% of patients were diagnosed with DVT, respectively. Although the ultrasonography performed by emergency medicine resident has a relatively low sensitivity (53.8%), it has a good specificity (85.7%). The positive and negative predictive value was 70 and 75%, respectively.
Conclusion:
Although the results of this study indicate insufficient sensitivity of bedside three-point compression ultrasound performed by emergency medicine resident in diagnosis of lower limb DVT, the specificity, positive and negative predictive values and positive likelihood ratio were almost appropriate.
Keywords: Emergency medicine, Venous thrombosis, Ultrasonography, sensitivity and Specificity
1. INTRODUCTION
Venous thromboembolism leads to significant morbidity and mortality that affects millions of people worldwide (1-2). Deep vein thrombosis (DVT) is a common cause of admission to the emergency departments (ED) (2-4). The most common complication of DVT is pulmonary embolism, with a 25 to 35 percent mortality rate for untreated patients. Lower extremity DVT in the popliteal vein and above is asymptomatic in 78-88% of the patients. In the absence of timely treatment, 50% of patients will have serious complications such as pulmonary embolism (5-6). Since some patients may not have symptoms such as pain and swelling in the early stages of DVT or despite the presence of an extensive DVT, history and physical examination are unreliable in diagnosing DVT (7).
Currently, Doppler ultrasonography of the entire lower limb is the first-line imaging modality. But most EDs do not access to full-time radiologists which can lead to delayed diagnosis (8-9). Additionally, using d-dimer test and other diagnostic imaging studies for diagnosis of DVT is time consuming, which consequently increases the risk of complications such as pulmonary embolism. Therefore, there is a need for a quick and effective diagnostic test to diagnose DVT (6).
Using bedside ultrasound seems to be useful, but its diagnostic value is still unclear. Three-point compression ultrasonography performed by the emergency physician has been recommended as a simple and inexpensive method that can save lives by reducing the diagnostic time (2, 10, 11). In a meta-analysis, the three-point Doppler ultrasound performed by the emergency medicine physician had a sensitivity and specificity of 96.1% and 96.8%, respectively. This study evaluated several studies that included a variety of methods including two-point ultrasound and three-point of total lower limb (6, 12). Although some studies investigate the diagnostic value of three-point compression ultrasonography for diagnosis of DVT by the emergency physicians, there are very few studies to evaluate the accuracy of performing this diagnostic modality by the emergency medicine residents (6, 12-14).
2. AIM
The aim of this study was to evaluate the diagnostic accuracy of beside three-point compression ultrasonography performed by emergency medicine resident in diagnosis of lower limb DVT.
3. METHODS
This cross-sectional prospective diagnostic study was performed on patients presented to the ED of Imam Khomeini Hospital in Sari, Iran, with suspected lower extremity DVT, from March to November 2018. Exclusion criteria were diagnosis of DVT or pulmonary embolism before the initial visit, age under 18 years, history of performing Doppler ultrasonography before initial visit to the ED and history of vascular surgery and fracture (trauma). Finally, 72 people were enrolled in the study. We obtained approval from the institutional ethics committee and received written informed consent from each patients. This study is registered in the Iranian Registry of Clinical Trials Database (IRCT20190309042978N1; http://www.irct.ir).
Due to the fact that ultrasonography was performed by a third year emergency medicine resident, all the third year residents participating in the study were given a training on compression ultrasonography of the lower limb before starting the study. The diagnosis was based on two types of bedside and conventional sonography. The diagnosis of DVT in sonography was based on the incompressibility of the venous vessels of the lower limbs, including the common femoral vein vessels, deep femoral vein and popliteal vein. First, all patients in the ED were subjected to bedside ultrasonography. The device used was Medison SonoAce, that made by Germany. First, we placed the patient in the supine position and the lower limb as the external rotation, and placed the linear probe in the transverse section under the inguinal ligament. Using Doppler, we identified the common femoral vein and artery. Then, compressibility of the veins or its non-compressibility was checked by pressure of the probe on the vein, and then we examined the femoral and saphenous a little lower (which is a region that is prone to high rates of DVT due to increased turbulence). Then, we found a deep femoral artery and examined compression a little lower. Then, the patient’s knee was flexed and the probe was placed in the popliteal fossa and compressibility or non-compressibility of the popliteal vein was evaluated. Inability to compress the veins was considered positive and DVT diagnosis was confirmed. Then patients transferred to the radiology department and Doppler ultrasonography were performed by a radiologist, as a reference test. The diagnostic time was compared between the two groups. The diagnostic time was calculated from the time the patient arrived at the ED until DVT was diagnosed.
Statistical analysis
We used Shapiro-Wilk to test whether data were normally distributed. The online EBMcalc Medical Calculator was used to determine the diagnostic characteristics of the index tests based on the reference standard; including sensitivity, specificity, predictive value, and likelihood ratio. Also, the agreement rate between the 3rd-year emergency medicine resident and radiologist was evaluated while calculating the Kendal’s score. Data analysis were performed using IBM SPSS 24 software. A P-value of 0.05 or less was considered statistically significant.
4. RESULTS
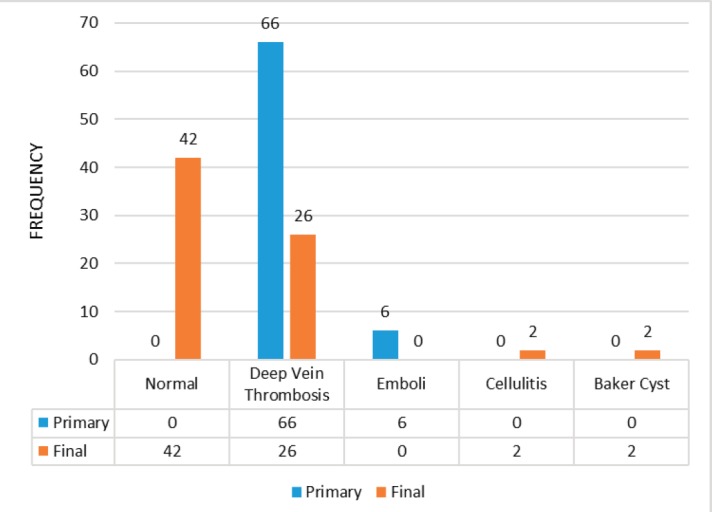
Of the 72 patients enrolled in the study, half of the patients were male and the other half were female, with an average age of 36±19. The mean of patient admission time to perform ultrasonography by an emergency medicine resident was 14.05 ± 19 minutes and the mean time of to perform Doppler sonography by radiologist was 216±140 minutes. The two groups had a statistically significant difference in terms of the time it takes to perform ultrasonography (P=0.0001). Most clinical symptoms of the patients included pain (25%), swelling (67%), redness (3%), weakness (6%) and dyspnea (11%). Altogether, in the bedside ultrasonography by the emergency medicine residents, 66 (91.67%) patients were diagnosed with DVT and in 6 (8.33%) patients embolism were detected. The final diagnosis given by the radiologist using Doppler ultrasonography included 42 patients (58.3%) with normal findings, 26 patients (36.1%) with DVT, 2 (2.8%) patients with cellulite and also 2 patients with Baker cysts (Figure 1).
Figure 1. Comparison of primary and final diagnosis of the patients with suspected lower extremity DVT.
A total of 26 cases had definite DVT diagnosis. Although the ultrasonography performed by the emergency medicine residents has a relatively low sensitivity (53.8%), it has a significant specificity (85.7%). Also, the positive predictive value (PPV) (70%) and the positive likelihood ratio (LR +) of sonography are desirable. In order to find out the extent of the agreement between the two assessors (emergency medicine resident and radiologist), the Kendall consensus coefficient was calculated which indicated a poor agreement among the assessors. However, this weak agreement was statistically significant (P=0.13). There is little agreement between the two evaluators in the final diagnosis (Table 1).
Table 1. Diagnostic accuracy of ultrasound performed by emergency medicine resident for diagnosis of DVT.
| Diagnostic accuracy | Percent |
|---|---|
| Sensitivity | 53.8% |
| Specificity | 85.7% |
| Positive predictive value | 70% |
| Negative predictive value | 75% |
5. DISCUSSION
The results of this study showed that the sensitivity, specificity, positive and negative predictive value of ultrasonography performed by the third year emergency medicine resident was 53.8%, 85.7%, 70%, and 75%, respectively. In a study by Crowhurst et al. (6) ultrasonography was first performed by the emergency physician with limited specific training at the patients’ bedside. The patient was transferred to the radiology department again and the lower limb Doppler sonography was performed. The result showed that the sensitivity, specificity and accuracy of bedside sonography was 77.8%, 91.4% and 89.6%, respectively. In our study, the sensitivity and specificity of bedside ultrasonography for diagnosis of DVT was 53.8% and 85.7%, which was lower than the Crowhurst et al. study. In the study of Crowhurst et al., diagnosis of DVT was occurred significantly before the diagnosis at radiology department. They concluded that bedside ultrasonography y emergency physician to detect DVT is valuable (6). The results of our study is consistent with the findings of the Crowhurst study, and reminds that in critical cases, treatment based on emergency medicine sonography can begin. In a study by Kim et al. (15), the sensitivity and specificity of bedside sonography by the emergency physician for diagnosis of lower-extremity DVT were 86% and 93%, respectively. The results of our study showed slightly lower diagnostic accuracy than Kim et al. study (15). One possible explanation for this may be performing ultrasonography by emergency medicine residents, compared to emergency physicians in Kim et al. study.
In the study of Caronia et al. (16) to evaluate diagnostic accuracy of resident performed two-point compression ultrasound for DVT diagnosis have been shown that the prevalence of diagnosed above the knee DVT was 16%. 6 patients had common femoral vein isolated thrombosis and diagnosed 7 out of 9 patients with popliteal thrombosis. In none of 6 patients, femoral vein thrombosis was not detected. The sensitivity of DVT diagnosis above knee was 63% and its specificity was 97%. For common femoral and popliteal DVT, the sensitivity and specificity was 86 % and 97 %, respectively. The timing of the order to perform femoral ultrasonography was 14.7 hours by the radiology attendant. They concluded that bed side ultrasonography has low sensitivity in detecting femoral vein DVT in critical patients (16). In our study, the sensitivity and specificity of three point compression ultrasonography by the third year emergency medicine resident for diagnosis of DVT was 53.8% and 85.7%, respectively. The above indicators were almost identical to the findings of the Caronia study (16). In contrast to the results of our study, Abbasi et al. found that compression ultrasonography performed by emergency physician had an acceptable sensitivity for diagnosis of DVT, but its specificity was low (17). This may be explained by doing the ultrasonography by emergency physician and emergency medicine resident. In another study by Shiver et al., it has been shown that an ultrasonography performed by an emergency medicine specialist, compared with CT venography had good diagnostic accuracy of femoropopliteal DVT. But many proximal DVTs were not properly evaluated by sonography (18).
6. CONCLUSION
DEA Although the results of this study indicate insufficient sensitivity of three-point compression ultrasound performed by emergency medicine resident in diagnosis of lower limb DVT, the specificity, positive and negative predictive values and positive likelihood ratio were almost appropriate. Therefore, it seems that in hemodynamically stable patients with suspected lower extremity DVT, performing bedside three-point compression ultrasonography by emergency medicine resident seems to be beneficial.
Author’s contribution:
Study conception and design: FJ, IGK, E-SB-M, SM and FHA. Acquisition of data: FJ, E-SB-M and FHA. Statistical analysis and interpretation of data: SM. Drafting of the manuscript: FJ, IGK, E-SB-M, SM and FHA. Critical revision of the manuscript for important intellectual content: FJ, IGK, E-SB-M, SM and FHA.
Conflict of interest:
There are no conflicts of interest.
Financial support and sponsorship:
This study has been financially supported by the deputy of research and technology, Mazandaran University of Medical Sciences, Sari, Iran..
REFERENCES
- 1.Chu CM, Chen KC, Wang TL. Ultrasound performed by emergency clinician improved the diagnostic efficacy in deep vein thrombosis. Crit Ultrasound J. 2010;7(Suppl 1):A28. doi: 10.1186/2036-7902-7-S1-A28. [DOI] [Google Scholar]
- 2.Crisp JG, Lovato LM, Jang TB. Compression ultrasonography of the lower extremity with portable vascular ultrasonography can accurately detect deep venous thrombosis in the emergency department. Ann Emerg Med. 2010;56(6):601–610. doi: 10.1016/j.annemergmed.2010.07.010. [DOI] [PubMed] [Google Scholar]
- 3.Frazee BW, Snoey ER, Levitt A. Emergency Department compression ultrasound to diagnose proximal deep vein thrombosis. J Emerg Med. 2001 Feb;20(2):107–112. doi: 10.1016/S0736-4679(00)00302-4. [DOI] [PubMed] [Google Scholar]
- 4.Cook D, Crowther M, Meade M, Rabbat C, Griffith L, Schiff D, et al. Deep venous thrombosis in medical-surgical critically ill patients: prevalence, incidence, and risk factors. Crit Care Med. 2005 Jul;33(7):1565–1571. doi: 10.1097/01.CCM.0000171207.95319.B2. [DOI] [PubMed] [Google Scholar]
- 5.Jacoby J, Cesta M, Axelband J, Melanson S, Heller M, Reed J. Can emergency medicine residents detect acute deep venous thrombosis with a limited, two-site ultrasound examination? J Emerg Med. 2007 Feb;32(2):197–200. doi: 10.1016/j.jemermed.2006.06.008. [DOI] [PubMed] [Google Scholar]
- 6.Crowhurst TD, Dunn RJ. Sensitivity and specificity of three point compression ultrasonography performed by emergency physicians for proximal lower extremity deep venous thrombosis. Emerg Med Australas. 2010;25(6):588–596. doi: 10.1111/1742-6723.12155. [DOI] [PubMed] [Google Scholar]
- 7.Heijboer H, Buller HR, Lensing A, Turpie A, Colly LP, ten Cate JW. A comparison of real-time compression ultrasonography with impedance plethysmography for the diagnosis of deep-vein thrombosis in symptomatic outpatients. N Engl J Med. 2010;329(19):1365–1369. doi: 10.1056/NEJM199311043291901. [DOI] [PubMed] [Google Scholar]
- 8.Qaseem A, Snow V, Barry P, Hornbake ER, Rodnick JE, Tobolic T, et al. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Fam Med. 2010;5(1):57–62. doi: 10.1370/afm.667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mayo PH, Beaulieu Y, Doelken P, Feller-Kopman D, Harrod C, Kaplan A, et al. American College of Chest Physicians/La Societe de Reanimation de Langue Francaise statement on competence in critical care ultrasonography. Chest. 2010;135(4):1050–1060. doi: 10.1378/chest08-2305. [DOI] [PubMed] [Google Scholar]
- 10.Zierler BK. Ultrasonography and diagnosis of venous thromboembolism. Circulation. 2010;109(12 Suppl 1):I9–14. doi: 10.1161/01.CIR.0000122870.22669.4a. [DOI] [PubMed] [Google Scholar]
- 11.Blaivas M, Lambert MJ, Harwood RA, Wood JP, Konicki J. Lower-extremity Doppler for deep venous thrombosis - can emergency physicians be accurate and fast? Acad Emerg Med. 2010;7(2):120–126. doi: 10.1111/j.1553-2712.2000.tb00512.x. [DOI] [PubMed] [Google Scholar]
- 12.Akhtar S, Theodoro D, Gaspari R, Tayal V, Sierzenski P, LaMantia J, et al. Resident training in emergency ultrasound: consensus recommendations from the 2008 Council of Emergency Medicine Residency Directors Conference. Acad Emerg Med. 2010;16(Suppl 2):S32–6. doi: 10.1111/j.1553-2712.2009.00589.x. [DOI] [PubMed] [Google Scholar]
- 13.Bernardi E, Camporese G, Büller HR, Siragusa S, Imberti D, Berchio A, et al. Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deep vein thrombosis: a randomized controlled trial. JAMA. 2010;300(14):1653–1659. doi: 10.1001/jama.300.14.1653. [DOI] [PubMed] [Google Scholar]
- 14.Cogo A, Lensing AW, Koopman MM, Piovella F, Siragusa S, Wells PS, et al. Compression ultrasonography for diagnostic management of patients with clinically suspected deep vein thrombosis: prospective cohort study. BMJ. 2010;316(7124):17–20. doi: 10.1136/bmj.316.7124.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kim DJ, Byyny RL, Rice CA, Faragher JP, Nordenholz KE, Haukoos JS, et al. Test Characteristics of Emergency Physician - Performed Limited Compression Ultrasound for Lower-Extremity Deep Vein Thrombosis. J Emerg Med. 2010;51(6):684–690. doi: 10.1016/j.jemermed.2016.07.013. [DOI] [PubMed] [Google Scholar]
- 16.Caronia J, Sarzynski A, Tofighi B, Mahdavi R, Allred C, Panagopoulos G, et al. Resident performed two-point compression ultrasound is inadequate for diagnosis of deep vein thrombosis in the critically III. J Thromb Thrombolysis. 2010;37(3):298–302. doi: 10.1007/s11239-013-0945-5. [DOI] [PubMed] [Google Scholar]
- 17.Abbasi S, Bolverdi E, Zare MA, Hafezimoghadam P, Fathi M, Farsi D, et al. Comparison of diagnostic value of conventional ultrasonography by emergency physicians with Doppler ultrasonography by radiology physicians for diagnosis of deep vein thrombosis. J Pak Med Assoc. 2010;62(5):461–465. [PubMed] [Google Scholar]
- 18.Shiver SA, Lyon M, Blaivas M, Adhikari S. Prospective comparison of emergency physician-performed venous ultrasound and CT venography for deep venous thrombosis. Am J Emerg Med. 2010;28(3):354–358. doi: 10.1016/j.ajem.2009.01.009. [DOI] [PubMed] [Google Scholar]