

Abstract
Background
Lumbo-costo-vertebral syndrome is a set of rare abnormalities involving vertebral bodies, ribs, and abdominal wall.
Case
We present a case of Lumbo-costo-vertebral syndrome in a 6-month old female infant who had a progressive swelling over the right lumbar area since birth. Clinical examination revealed a reducible swelling on the right flank with positive cough impulse. Ultrasonography showed a defect containing bowel loops in the right lumbar region. Chest X-ray revealed scoliosis and hemivertebrae with absent lower ribs on the right side. Computer tomography scan showed hernia sac containing the bowel and the right lobe of the liver with cross fused kidney.
Conclusion
Lumbo-costo-vertebraly syndrome is a rare condtion which could be associated with different organ malformations. Simple closure or meshplasty could be done depending on the size of the defect.
Keywords: lumbar hernia, lumbo-costo-vertebral, hemivertebrae
Introduction
Congenital lumbar hernia (CLH) is rare in children, and the patients with CLH generally have other associated congenital anomalies. The most common clinical entity associated with CLH is the so-called “lumbo-costo-vertebral syndrome, (LCVS)”, which includes hemivertebrae, absent ribs, and abdominal wall muscle hypoplasia, presenting as CLH (1).
Most commonly, they appear through superior lumbar triangle of Grynfeltt, and rarely through inferior lumbar triangle of Petit. It may be present at birth or noticed at an older age. Lower backache is the commonest symptom, although small hernias may be asymptomatic or present with visible swellings which become more prominent during crying (2). We report a case of LCVS on account of its rarity.
Case Report
A 6-month old female infant was presented with a swelling in the right lumbar region, which was noticed by the parents at birth. The swelling was initially small but gradually increased to attain the current size which became more prominent up on crying and decreased while in supine position. On examination, there was a globular painless swelling, 6cm x10cmin size, which was soft and reducible below the right costal margin lateral to the dorso-lumbar spine. Bowel sound was heard over the mass (Figure 1). X-ray of the chest showed absent ribs (T10, T11) on the right side with hemi-vertebrae. There was also scoliosis with convexity to the left and overcrowding of the ribs on the right chest on the chest X-ray (Figure 2). Ultrasound of the abdomen showed hernial defect in the right lumbar region measuring 4.5cm x 2.9cm, containing bowel loops and right ectopic kidney, which was visible on the right hypogastric area in other words fused kidney on the right side. CT scan also showed crossed fused kidney (ectopic kidney) on the same side with the hernia sac, containing bowel and the right lobe of the liver. It also showed absentribs (T10, T11) with right hemivertebrae of the corresponding vertebral bodies on the same side (Figure 3). Renal function tests showed normal values creatinine-0.4mg/dl and BUN-16.1mg/dl.
Figure 1.

Mass of 6cm x 10cm occupying the right flank
Figure 2.
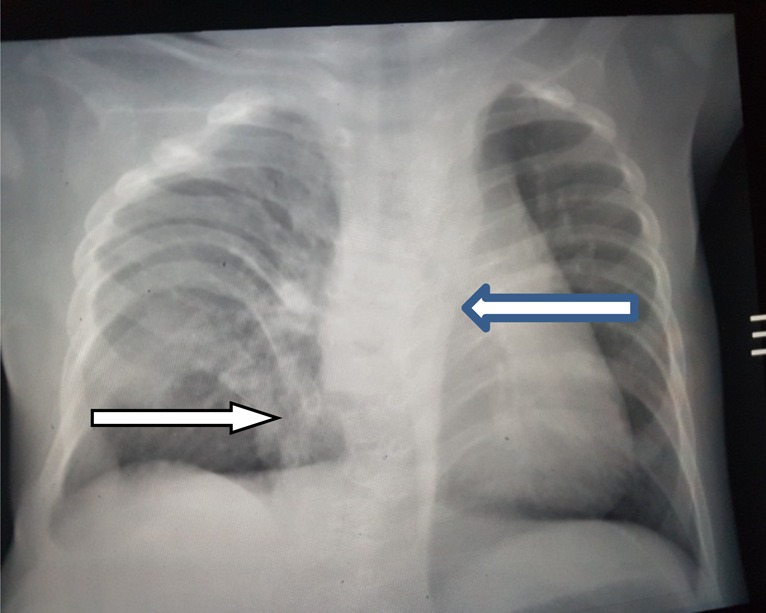
Chest x-ray showing scoliosis with absent ribs
Figure 3.
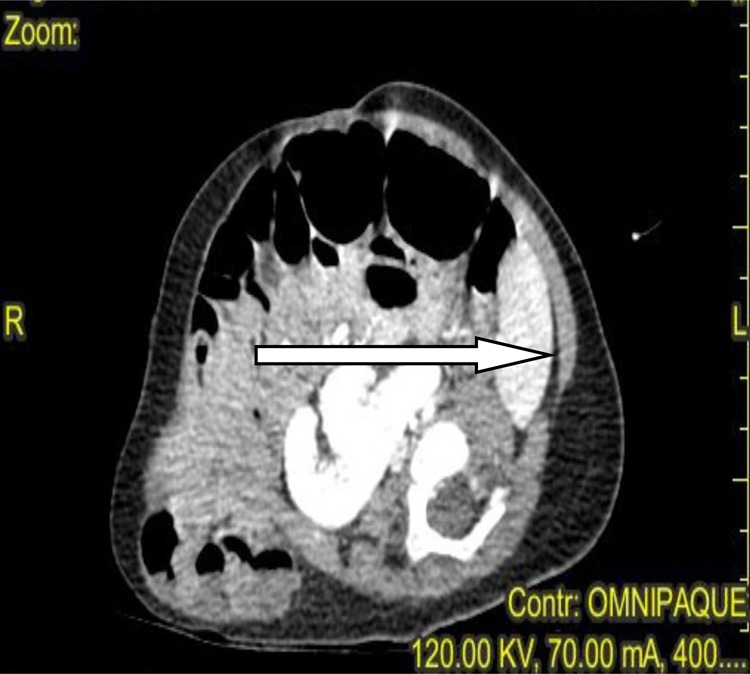
CT scan of a right lumbar hernia with visible bowl in the sac
Discussion
We found a case of LCVS on a 6-month old infant with right side hemi-vertebrae, scoliosis and fused kidney on the same side. LCVS is a rare condition, and few cases have been reported in the literature so far (3). LCVS was first described by Touloukian in 1972 who believed that these defects are due to a single somatic defect occurring during 3–5 weeks of gestational age, resulting in a defective formation of the vertebral bodies, ribs, and abdominal wall musculature (2).
The pathogenesis of LCVS is not known. Lafer (1994) reported the association with intrathoracicneuroblastoma, postulating that a localized neuropraxia caused by the tumor led to the lumbar hernia. Touloukian (1972) attributed the LCVS to a somatic defect occurring during the 3rd to 5th week of human embryogenesis, possibly as a result of transient anoxia, which in turn, results in significant malformation of the vertebral bodies, ribs and the musculature. In agreement with this,Touloukian (1972) and Ingalls et al., (1952) suggested that transient anoxia at the 3rd week of embryogenesis causes thesemalformations (1). Multiple congenital anomalies such as inguinal hernia, telipusequinovarus, absence of kidney and congenital heart disease might also be seen in association with LCVS (4).
Neurulation occurs at 3–5 weeks of gestational age, during which the formation of the neural groove, closure of the anterior and posterior neuropores, appearance of the ventral horn cells, formation of anterior and posterior roots and disjunction of the neuroectoderm from the surface ectoderm takeplace. Therefore, the defect of LCVS could also be associated with spinal cord malformations. This has been reported by G. Samson Sujit Kumar et. al from India, on an 18-month old patient, who had left superior lumbar hernia, hemivertebrae with absent left ribs and posterior spinal dysraphism with a dorsal lipoma and tetherd cord at L4 level.
Previously published studies also suggest an association between the lumbar hernias and LCVS defects. Other abnormalities associated with congenital lumbar hernia, reported so far include congenital sciatic hernia, absent tibia, posterior meningomyelocele, focal nodular hyperplasia of the liver and absent kidney (3). LCVS may also be associated with VACTREL anomaly as seen in a term neonate with clinical findings of large abdominal wall hernia, imperforate anus, vestibular fistula, absent right rib, vertebral anomalies, tethered cord, syringomyelia and two sacral dimples, which was reported by K. Harris, 2009(5).
LCVS may be present at birth or noticed at an older age. Small hernias may remain asymptomatic and are rarely present as acute bowel obstruction. CT scan and Magnetic Resonance Imaging (MRI) are investigation of choice to confirm the diagnosis, know hernia contents, and muscular trophies. Contents of hernial sac are usually small or large intestine, mesentery, omentum, appendix, caecum, stomach, ovary, spleen or kidney rarely. In our case, the hernial sac content was the small bowel (2).
The goal of repair is to close the defect and build a strong and elastic abdominal wall. Wide varieties of materials have been used to close the defect. The simple tissue approximation-closure can be sufficient for small defects while larger defects may need meshplasty. The surgical correction should be done early when the size of the defect is small, and the defect can be repaired either by open surgery or laparoscopic methods (2). Since the defect was large, our patient was referred to another hospital for meshplasty.
Acknowledgements
We would like to acknowledge the parents for giving us their consent to publish this case report. We would also like to acknowledge Mr. Mesfin Zewdu and Dr. Elias Kedir for their contribution to this case report.
References
- 1.Okumus N, Bas AY, Demirel N, Zenciroglu A, Surmeli S, Ceylaner S. Lumbocostovertebral Syndrome in an Infant of a diabetic mother. American journal of Medical genetics. 2010;152A(6):1374–1377. doi: 10.1002/ajmg.a.33465. [DOI] [PubMed] [Google Scholar]
- 2.Gupta L, Mala TA, Gupta R, Malla SA. Lumbo-Costo-Vertebral Syndrome with Congenital Lumbar Hernia. APSP J Case Rep. 2014;5(1):5. [PMC free article] [PubMed] [Google Scholar]
- 3.Kumar GS, KulKarani V, Haran RP. Lumbo - Costo- vertebral syndrome with posterior spinal dysraphism. Neurology india. 2005;53(3):351–353. doi: 10.4103/0028-3886.16943. [DOI] [PubMed] [Google Scholar]
- 4.Sisodiya RS, Shekhar Panda S, Ratan SK. Lumbo-costo-vertebral syndrome with inguinal hernia and other anomalies. BMJ. 2017:bcr2016216974. doi: 10.1136/bcr-2016-216974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Harris K, Dorn C, Bloom B. Lumbocostovertebral_syndrome_with VACTREL anomalad. J Perinatol. 2009;29(12):826–827. doi: 10.1038/jp.2009.82. [DOI] [PubMed] [Google Scholar]