

Abstract
Background
Appendicitis is the most common cause of acute abdomen. The diagnosis of appendicitis can be easy when it presents with the classical symptoms or is very challenging when present with atypical presentation. Around 20–30% of patients operated on for appendicitis have appendicolithiasis. Appendicolithiasis are usually small in size, and are called giant when more than 2cm in size.
Case Detail
A 36 years old man was referred from a district hospital with a diagnosis of cecal cancer. His complaints were right lower quadrant (RLQ) abdominal mass of 03 months and pain of 18 months duration. Colonoscopy was normal but abdominal CT showed a RLQ mass with a dense radio-opaque shadow at its center.
Conclusions
Giant appendicolith is a rare condition. A high index of suspicion and careful review of imaging findings is the key in early diagnosis and improved patient outcomes.
Keywords: Appendicitis, Appendicolithiasis, Appendiceal mass, Giant appendicolithiasis, Ethiopia
Introduction
Appendicitis is the most common cause of acute abdomen. Mortality and morbidity of appendicitis have declined in the last few decades. The diagnosis of appendicitis can be easy when it presents with the classical symptoms or very challenging when present with atypical symptoms (1,2). Patients with appendiceal mass present with a preceding symptom suggestive of appendicitis with some delay of diagnosis and treatment. The mass can be palpated or diagnosed with imaging studies.
Around 30% of patients operated on for appendicitis have appendicolithiasis (3). Appendicolithiasis is a term used to describe concretions or calcified deposits in the appendix. These could be either a tightly packed fecal material or true calculi. Although appendicolithiasis may not be necessary for developing appendicitis, its presence is associated with more perforation of the vermiform appendix. Appendicolithiasis are usually small in size. There is no definite relationship between size of the appendicolith and risk of appendicitis or its complications. When appendicoliths are more than 2cm in diameters they are defined giant (4). Understanding and documenting the possible uncommon presentation of common clinical conditions like appendicitis is an important consideration for physicians. Here, we present a 36 years old man who presented with right lower quadrant abdominal mass of 3 months duration and intra-operative finding confirmed a mass formed by a perforated appendix with a 2.5cm long appendicoliths in it.
The Case
A 36 years old man who had RLQ abdominal pain and mass was referred to us from a district hospital with a diagnosis of cecal cancer. The patient had the pain for the last 18 months and the mass for the last 03 months. The patient had significant but unquantified weight loss. Otherwise, he has no fever, vomiting, abdominal distension or bowel habit changes. The only abnormal finding on examinations was a tender 4x5cm RLQ intra-abdominal mass.
Laboratory values including tumor markers were all normal. With a diagnosis of rule out, cecal cancer abdominal ultrasound was done. The ultrasound showed a RLQ mass measuring 5x6cm with a central echogenic foci with distal acoustic shadow. The rest of the abdominal viscera were normal. Abdominal CT revealed a RLQ 6x6cm mass with a 2.5cmx 2.4cm radio-opaque shadow at its center. Figure 1 shows the radiologist made a diagnosis of heterotopic mesenteric calcification.
Figure 1.

Abdominal CT, showing Right lower quadrant dense structre with accompanying inflammatory mass
Patient was prepared and operated with long midline incision. The finding was a retroperitoneal RLQ mass measuring 6x6cm. Right colon was mobilized to the left exposing the retro-peritoneum starting at the distal ascending colon. Due to extensive adhesion mobilization, the colon was difficult around the mass. Hence, the mass was mobilized with the distal ileum and the right colon. Careful evaluation revealed an inflammatory mass formed by perforated retroperitoneal appendix, a giant appendicoliths (2.5cm) and surrounding inflammatory tissues. The mass had very little pus (Figure 2). The diagnosis of missed perforated appendix was made, the stone removed and classical appendectomy performed and specimen sent for pathology. The prophylaxis antibiotics started continued as therapeutic. Post-operatively, the patient had superficial surgical site infection which responded for wound care. The patients stayed in hospital for a total of 5 days. Specimen Biopsy confirmed acute appendicitis. Six months after the surgery, the patient was in good health.
Figure 2.
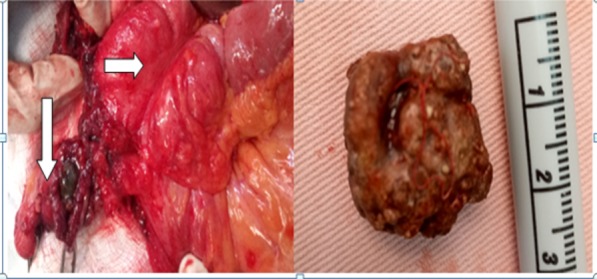
Left: intra-operative pictures, the perforated appendix with surrounding inflammatory changes, the stone inside (down arrow) and the Cecum (right side arrow), Right: The stone outside the appendix
Discussion
The etiology of appendicitis is not clearly understood, but luminal obstruction is believed to play a significant role in the pathogenesis. Obstruction could be due to appendicoliths, lymphoid hyperplasia, parasite infestations etc….(3) . Our patient's appendicitis is likely to be due to obstruction of the lumen by the appendicoliths.
Due to late presentation or misdiagnosis, acute appendicitis patients could present with appendiceal mass. Because clinical examination is not enough to detect or differentiate appendiceal mass from other RLQ masses or abscess, imaging is essential for its diagnosis.
Our patient was referred and evaluated with impression of cecal cancer, which was a reasonable consideration. Colonoscopy ruled out the diagnosis of cecal cancer but did not diagnose the appendiceal mass related to the extra-luminal nature of the pathology. Hence, abdominal CT was needed to consider the possibility of appendicoliths. The difficulty of diagnosing the patient is likely from the rarity of seeing such huge radio-opaque intra-abdominal lesion. In addition, the duration of presentation of the patient also contributing for the confusion.
The effect of appendicolith in the pathogenesis of appendicitis has been described in variable ways. JP Singh and et al reported appendicolith to be more common in pediatrics age group than adults and that rate of perforation was higher on patients with appendicoliths (3). Confusions and difficulties in diagnosing patients with appendicoliths have been reported by different authors. Zafer and Kaushik separately reported patients presenting with symptoms similar to ureteric colic which was later found to be an appendicitis caused by giant stone (larger than 2 cm) in the appendix (1,2). Igwe P.O. reported three patients who were operated with a diagnosis of acute appendicitis and later found to have appendicoliths measuring 2.1- 4.5cm (4). Most appendicoliths are small and present with acute appendicitis. To the best of our knowledge, there are no reports of an appendicoliths which presented as a RLQ mass staying for several months.
Why patients develop appendicoliths is not clear, but its effect has been described in different ways. It can be a cause of non-specific long standing RLQ abdominal pain or acute appendicitis. Adrian Harris, et al compared the rate RLQ abdominal pain relief after appendectomy for a normal looking appendix with appendicoliths and found surgery to significantly improve patient's outcome. They recommended routine removal of a normallooking appendix at laparoscopy in patients with recurrent symptoms in the absence of any other obvious pathology (5).
The exploration is better done through long midline incision to get better access into the whole abdomen and retro-peritoneum.
Due to the extensive adhesion that develops from the prolonged inflammation, it is prudent to anticipate difficulty in mobilization of the right colon. Once mobilized, understanding what the problem should be very easy and subsequent appendectomy straight forward. In such uncommon clinical presentation and radiological finding, a high index of suspicion and with careful review of findings is the key in improving patient's outcome.
References
- 1.Kumar K, Lewis D. Diagnostic Confusion Caused by a Giant Appendicolith : A Case Report. J Med Cases. 2015;6(2):71–73. [Google Scholar]
- 2.Teke Zafer, Kabay Burhan, Halil Erbis OLT. Appendicolithiasis causing diagnostic dilemma : a rare cause of acute appendicitis ( report of a case ) Tanısal ikileme neden olan apandikolitiyazis. Turkish J Trauma Emerg Surg. 2008;14(4):323–325. [PubMed] [Google Scholar]
- 3.Singh JP, Mariadason JG. Role of the faecolith in modern-day appendicitis. Ann R Coll Engl. 2013;95:48–51. doi: 10.1308/003588413X13511609954851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Igwe PO, Okpani CP. Giant calculus of the appendix — Report of three cases. Gaz Med. 2016;4(1):382–386. [Google Scholar]
- 5.Grimes C, Chin D, Bailey C, Gergely S, Harris A. Appendiceal faecaliths are associated with right iliac fossa pain. Ann R Coll Engl. 2010:61–64. doi: 10.1308/003588410X12518836439524. [DOI] [PMC free article] [PubMed] [Google Scholar]