

Abstract
Introduction
In past biomechanical studies, repetitive motion of lumbar extension, rotation, or a combination of both, frequently seen in batting or pitching practice in baseball, shooting practice in soccer, and spiking practice in volleyball, have been considered important risk factors of lumbar spondylolysis. However, clinically, these have been identified in many athletes performing on a running track or on the field, which requires none of the practices described above. The purpose of this study was to verify how much impact running has on the pathologic mechanism of lumbar spondylolysis.
Methods
In study 1, 89 consecutive pediatric patients diagnosed with lumbar spondylolysis at a single outpatient clinic between January 2012 and February 2017 were retrospectively analyzed. In study 2, motion analysis was performed on 17 male volunteers who had played on a soccer team without experiencing low back pain or any type of musculoskeletal injury. A Vicon motion capture system was used to evaluate four movements: maximal effort sprint (Dash), comfortable running (Jog), instep kick (Shoot), and inside kick (Pass).
Results
In study 1, 13 of the 89 patients with lumbar spondylolysis were track and field athletes. In study 2, motion analysis revealed that the hip extension angle, spine rotation angle, and hip flexion moment were similar in Dash and Shoot during the maximum hip extension phase. The pelvic rotation angle was significantly greater in the kicking conditions than in the running conditions.
Conclusions
Kinematically and kinetically, the spinopelvic angles in Dash were considered similar to those in Shoot. Dash could cause mechanical stress at the pars interarticularis of the lumbar spine, similar to that caused by Shoot, thus leading to spondylolysis.
Keywords: Lumbar spondylolysis, Track and field athlete, Dash, Three-dimensional analysis
Introduction
Lumbar spondylolysis is a defect of the pars interarticularis and is considered to occur subsequent to stress fracture1). Biomechanical studies have shown that hyperextension and rotation of the trunk causes greater mechanical stress at the pars interarticularis, which may lead to stress fractures of the pars2-4). Such movements are frequently seen in baseball batting and pitching practice as well as in soccer shooting practice. Furthermore, a higher prevalence of lumbar spondylolysis has been found in adolescent baseball and soccer players5).
However, lumbar spondylolysis has also been identified in many track and field athletes, whose practice sessions do not include any of the above-mentioned practices. During a soccer game, maximal- and high-intensity sprints (Dash) by players are mixed with moderate- and low-intensity running (Jog). In the 2014 World Cup, the mean number of sprints per player in a soccer game was 33.25 ± 10.676). Thus, most players engaged in various sports activities, such as baseball, basketball, volleyball, and soccer, require the Dash. Thus, we hypothesized that Dash would augment extension and rotation of trunk forces, thereby increasing the risk of lumbar spondylolysis.
The purpose of this study was to verify how much impact Dash has on the pathologic mechanism of lumbar spondylolysis. First, we investigated how many patients engaged in track and field were identified among consecutive pediatric patients who had been diagnosed with lumbar spondylolysis within a period of time. Second, we analyzed kinetic and kinematic data for two running conditions (Dash and Jog), thus comparing two kicking conditions (Shoot and Pass) to simulate the movements that occur in a soccer game.
Materials and Methods
Study participants
Study 1
Eighty-nine consecutive pediatric patients (72 boys, 17 girls) diagnosed with lumbar spondylolysis at a single outpatient clinic between January 2012 and February 2017 were retrospectively investigated to identify how many were track and field athletes. The mean patient age was 13.9 (range, 6-17) years.
Study 2
Motion analysis was performed on 17 male volunteers who had played on a soccer team but had not experienced low back pain or any musculoskeletal injuries. Demographic and anthropometric data for these subjects were as follows: age, 24.1 ± 4.1 years; body weight, 69.8 ± 12.7 kg; height, 175.5 ± 5.4 cm; leg length (right, 885 ± 32.3 mm; left, 885 ± 32.3 mm), knee width (right, 107.1 ± 10.1 mm; left, 105.1 ± 6.3 mm), and ankle width (right, 70.1 ± 3.9 mm; left 70.2 ± 3.8 mm).
Both studies were approved by the Medical Ethics Committee of Tokushima University, Japan. Informed consent was obtained from all subjects in study 1 and 2.
Motion analysis
Motion analysis was performed to record kinematic and kinetic data during comfortable running (Jog), maximal effort sprint (Dash), instep kick (Shoot), and inside kick (Pass) using the Vicon MX systemⓇ (Vicon Motion Systems, Oxford, UK). Three-dimensional kinematic data were collected at 150 Hz using a passive eight-camera system (Vicon MX T20; Vicon Motion Systems). Kinetic parameters were recorded at 1500 Hz using a ground force platform with four embedded force transducers (AMTI model OR-06; Advanced Mechanical Technology Inc., Watertown, MA). The kinematic and kinetic systems were synchronized to allow simultaneous data collection. Nexus 2.0 software (Vicon Motion Systems) was used to derive the kinematic and kinetic parameters when standing for 30 seconds and performing the Jog, Dash, Shoot, and Pass (three times each).
Before data collection, each subject performed a 5-min dynamic warm-up, including a series comprising the four tasks. The subjects performed maximal effort Dash and Jog on a floor at our rehabilitation center. The camera and ground force platform were centered 10 m from the start line. All subjects preferred to kick the ball using the right leg. After a short warm-up period, they were instructed to perform inside kicks and instep kicks using the preferred leg and kicking with maximum effort to the center of the goal, which was located 5 m in front of them.
Using the Plug-in Gait model, 35 markers (diameter, 14 mm) that reflected infrared rays were placed on anatomic landmarks for all body segments, including the head (n = 4), trunk (n = 5), pelvis (n = 4), upper limbs (n = 10), and lower limbs (n = 12)7). Eight MX cameras captured the motion of the markers, and the Nexus 2.0 software processed the motion data as stick images from the marker positions in three dimensions. The software extracted three-dimensional coordinate data for the parameters in the Plug-in Gait model. The reliability of flexion, extension, rotation, and lateral bending of the spine of the Plug-in Gait model has been studied, and high reliability has been reported8).
The following parameters were identified and calculated: ground reaction force, kinematics (thorax, spine, pelvis, hip, knee, and ankle angles), and kinetics (hip moments). The angles of the thorax and pelvis reflect the absolute movement in space, whereas the spine angles reflect the relative movement between the thorax and pelvis. A positive angle corresponds to a posterior movement, whereas a negative angle corresponds to an anterior movement. The hip and knee kinematics correspond to the flexion/extension angles; a positive value is a flexion movement, and a negative value is an extension movement.
Statistical analysis
The kinematic and kinetic parameters were analyzed using one-way analysis of variance with Tukey-Kramer correction. Statistical analysis was performed using SPSS version 22.0 for Windows (IBM Corp., Armonk, NY). Statistical significance was set at P < 0.05.
Results
Study 1
Sports-related activities of the patients in study 1 are shown in Table 1. Thirteen (15.0%) of the 89 patients with lumbar spondylolysis had participated in track and field sporting activities; this group comprised 9 sprinters, 3 long-distance runners, and 1 hurdler.
Table 1.
Cases of Active Spondylolysis according to Patients’ Sports-Related Activities.
| Sports | No. of Patients, Total (%) |
|---|---|
| Baseball/Softball | 30 (34) |
| Soccer | 22 (25) |
| Track/Road race | 13 (15) |
| Basketball | 7 (8) |
| Volleyball | 5 (6) |
| Field | 4 (4) |
| Judo | 3 (3) |
| Tennis | 2 (2) |
| Swimming | 2 (2) |
| Karate | 1 (1) |
| Total | 89 |
Study 2
Dash and Jog parameters
The average running speeds during the kinetic and kinematic analyses were 25.9 ± 1.9 km/h during Dash and 12.9 ± 1.9 km/h during Jog.
Kinematic and kinetic analysis
Changes in the kinematic and kinetic parameters are shown in Figure 1, 2. There were no significant differences in hip extension angle values between Dash and Shoot; however, there were significant differences between Jog and Dash (13.1° ± 6.6° vs. 22.6° ± 6.8°), Jog and Shoot (13.1° ± 6.6° vs. 30.3° ± 10.8°), and Pass and Shoot (20.5° ± 12.2° vs. 30.3° ± 10.8°).
Figure 1.
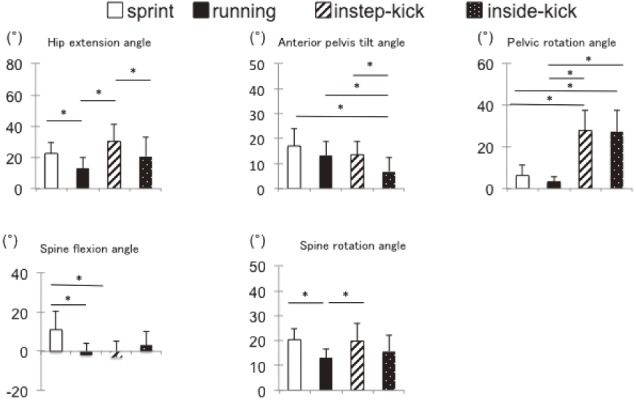
Mean values for movement of the hip, pelvis, and spine (°) during tasks. *P<0.05 indicates a statistically significant difference between conditions.
Figure 2.

Mean movement (°) values of for hip moment and ground reaction force during tasks. *P<0.05 indicates a statistically significant difference between conditions.
There were no significant differences in the anterior pelvic tilt angles between Dash, Jog, and Shoot; however, the angles for Pass were significantly higher than those for the other three movements. There was also no significant change in the pelvic rotation angle between the two running conditions (Dash and Jog) or between the two kicking conditions (Shoot and Pass); however, the angles for both kicking conditions were significantly higher than those for the running conditions.
There was a significant difference in the spine flexion angle between Dash and Jog (11.1° ± 9.6° vs. −1.9° ± 6.2°) and between Dash and Shoot (11.1° ± 9.6° vs. −3.1° ± 8.1°). The spine rotation angles for Dash (20.4° ± 4.2°) and Shoot (19.8° ± 7.3°) were similar, and both were significantly greater than that for Jog (13.2° ± 3.4°).
The hip flexion moment was not significantly different between Dash and Shoot but was significantly different between Jog and Dash (999.6 ± 398.4 Nmm vs. 3072.5 ± 1768.8 Nmm), Jog and Shoot (999.6 ± 398.4 Nmm vs. 3708.5 ± 1352.0 Nmm), and Pass and Shoot (2033.2 ± 1123.8 Nmm vs. 3708.5 ± 1352.0 Nmm). There were no significant differences in the vertical ground force reaction between the four conditions.
Discussion
Lumbar spondylolysis was first identified to be caused by a stress fracture of the pars interarticularis by Wiltse et al. in 19751). Biomechanically, hyperextension and rotation of the trunk have been recognized to cause greater mechanical stress at the pars interarticularis, which may lead to stress fracture of the pars2). These movements are frequently seen in batting or pitching practice drills in baseball and in shooting practice in soccer. The high prevalence of lumbar spondylolysis in baseball and soccer players is consistent with these biomechanical observations. However, clinically, lumbar spondylolysis has also been identified in many track and field athletes who do not undertake the above-mentioned types of practice. In this study, we found that 15% of our patients with lumbar spondylolysis were track and field athletes, followed by baseball and soccer players. This finding was proportionally high compared with previous studies that reported a 7%-11% prevalence of lumbar spondylolysis in track and field athletes9,10), thus suggesting that movements required during running may be involved in the pathogenetic mechanism of spondylolysis in track and field athletes.
In this study, we used kinetics and kinematics motion analyses to explore the impact of running on the spinopelvic angle by analyzing two running (Dash and Jog) and two kicking conditions (Shoot and Pass) frequently seen in soccer games. We found that the data for hip extension angles, spine rotation angles, and hip flexion moments were similar for Dash and Shoot during the maximum hip extension phase.
The maximum hip extension angle during Shoot was 9.3°, with a significantly greater hip extension angle than for Pass11). In the past report, maximum hip extension was found to be 23.8° during sprinting12). The mean hip extension angle value in this study was 22.6 ± 6.8°, which was considered similar to the value obtained in previous research because it was within 1 SD.
There have been several studies of the kinetics and kinematics of the lower limbs during running, all of which reported results similar to those of our present study12,13). However, there have been no reports focusing on spinopelvic movements. We found in our study that the rotation angles of the spine and the hip flexion moment were greater for Dash and Shoot than for Jog and Pass.
In soccer, kicking requires greater involvement of the iliacus, gastrocnemius, vastus medialis, and hip adductor muscles11); however, the iliopsoas has been shown to have greater influence on running speed than on any other muscle in terms of generating power during sprinting14). The iliopsoas is considered one of the most active muscles in soccer players. Functionally, the psoas and iliacus are anatomically different muscles having individual- and task-specific activation patterns depending on the specific demands for stability or movement at the lumbar spine, pelvis, and hip15). Our present results indicate that the hip flexion moment is increased during Dash and Shoot, which may cause extension of the spine.
We acknowledge that our study has several limitations. All values were measured using a camera and a ground force platform centered 10 m from the start line; thus, evaluation beyond 10 m was not possible. In addition, the motion analysis system, while calculating angular motion in all three planes, used surface-mounted markers. Thus, despite using high-resolution cameras, consistent and careful calibrations, and standardized models and joint coordinate systems, all calculations were ultimately influenced by the underlying movement of the soft tissues16). Even with the consistent placement of markers and use of algorithms to calculate joint angles, the lower extremity alignment values only have acceptable rather than perfect agreement and validity.
The main findings of this study were that the hip extension angle, spine rotation angle, and hip flexion moment data were similar between Dash and Shoot during the maximum hip extension phase. Our results support the theory that fast Dash increases the hip extension angle, spine rotation angle, and hip flexion moment during Dash. We infer that greater hip extension angle, spine rotation angle, and hip flexion moment values could occur as a result of running fast during the Dash phase, and could thus be risk factors for spondylolysis. The findings of this research may help therapists, coaches, and trainers, who could now strategize training programs, to reduce the risk of spondylolysis.
Disclaimer: Shinsuke Katoh is the Editor of Spine Surgery and Related Research and on the journal's Editorial Committee. He was not involved in the editorial evaluation or decision to accept this article for publication.
Conflicts of Interest: The authors declare that there are no relevant conflicts of interest.
Author Contributions: Tsuyoshi Goto wrote and prepared the manuscript, and all authors participated in the study design. All authors have read, reviewed, and approved the article.
References
- 1.Wiltse LL, Widell EH Jr, Jackson DW. Fatigue fracture: the basic lesion in isthmic spondylolisthesis. J Bone Joint Surg Am. 1975;57(1):17-22. [PubMed] [Google Scholar]
- 2.Sakai T, Yamada H, Nakamura T, et al. Lumbar spinal disorders in patients with athetoid cerebral palsy: a clinical and biomechanical study. Spine. 2006;31(3):66-70. [DOI] [PubMed] [Google Scholar]
- 3.Terai T, Sairyo K, Goel VK, et al. Spondylolysis originates in the ventral aspect of the pars interarticularis: a clinical and biomechanical study. J Bone Joint Surg Br. 2010;92(8):1123-7. [DOI] [PubMed] [Google Scholar]
- 4.Sairyo K, Katoh S, Sasa T, et al. Athletes with unilateral spondylolysis are at risk of stress fracture at the contralateral pedicle and pars interarticularis: a clinical and biomechanical study. Am J Sports Med. 2005;33(4):583-90. [DOI] [PubMed] [Google Scholar]
- 5.Sakai T, Sairyo K, Suzue N, et al. Incidence and etiology of lumbar spondylolysis: review of the literature. J Orthop Sci. 2010;15(3):281-8. [DOI] [PubMed] [Google Scholar]
- 6.Chmura P, Andrzejewski M, Konefał M, et al. Analysis of Motor Activities of Professional Soccer Players during the 2014 World Cup in Brazil. J Hum Kinet. 2017;12:187-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Orendurff MS, Segal AD, Klute GK, et al. The effect of walking speed on center of mass displacement. J Rehabil Res Dev. 2004;41(6A):829-34. [DOI] [PubMed] [Google Scholar]
- 8.Rast FM, Graf ES, Meichtry A, et al. Between-day reliability of three-dimensional motion analysis of the trunk: A comparison of marker based protocols. J Biomech. 2016;49(5):807-11. [DOI] [PubMed] [Google Scholar]
- 9.Debnath UK, Scammell BE, Freeman BJC, et al. Predictive Factors for the Outcome of Surgical Treatment of Lumbar Spondylolysis in Young Sporting Individuals. Global Spine J. 2018;8(2):121-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yamazaki K, Kota S, Oikawa D, et al. High defect stage, contralateral defects, and poor flexibility are negative predictive factors of bone union in pediatric and adolescent athletes with spondylolysis. J Med Invest. 2018;65(1.2):126-30. [DOI] [PubMed] [Google Scholar]
- 11.Brophy RH, Backus SI, Pansy BS, et al. Lower Extremity Muscle Activation and Alignment During the Soccer Instep and Side-foot Kicks. J Orthop Sports Phys Ther. 2007;37(5):260-8. [DOI] [PubMed] [Google Scholar]
- 12.Kratky S, Müller E, Pfusterschmied J, et al. Effects of a Body-Weight Supporting Kite on Sprint Running Kinematics in Well-Trained Sprinters. J Strength Cond Res. 2013;27(5):1215-22. [DOI] [PubMed] [Google Scholar]
- 13.Schache AG, Blanch PD, Murphy AT. Relation of anterior pelvic tilt during running to clinical and kinematic measures of hip extension. Br J Sports Med. 2000;34(4):279-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Andersson E, Oddsson L, Grundström H, et al. The role of the psoas and iliacus muscles for stability and movement of the lumbar spine, pelvis and hip. Scand J Med Sci Sports. 1995;5(1):10-6. [DOI] [PubMed] [Google Scholar]
- 15.Mann RA, Moran GT, Dougherty SE. Comparative electromyography of the lower extremity in jogging, running, and sprinting. Am J Sports Med. 1986;14(6):501-10. [DOI] [PubMed] [Google Scholar]
- 16.Benoit DL, Ramsey DK, Lamontagne M, et al. Effect of skin movement artifact on knee kinematics during gait and cutting motions measured in vivo. Gait Posture. 2006;24(2):152-64. [DOI] [PubMed] [Google Scholar]