

Abstract
Background
Angiopoietin-like protein 8 (ANGPTL8), a newly identified hormone, has been recently characterized as a metabolic regulator which can affect energy homeostasis and has interesting potentials as a metabolic disease therapy. However, little is as yet known as to whether circulating ANGPTL8 levels are altered in thyroid dysfunction. This study measured serum ANGPTL8 levels in patients with Graves’ disease and explored the correlations between its serum levels and thyroid index in Graves’ disease.
Methods
The concentration of ANGPTL8 was analyzed in blood samples of 128 well-characterized individuals whose anthropometric parameters, biochemical parameters, and thyroid index were measured. The participants were divided into Graves’ disease patients (n = 60) and healthy control subjects (n = 68). Logistic regression was used to evaluate the relationship between ANGPTL8 and Graves’ disease.
Results
Serum ANGPTL8 levels were more significantly decreased in Graves’ disease patients than in healthy control subjects (177.67 ± 135.07 vs 326.41 ± 194.72 pg/mL; p < 0.001). Serum ANGPTL8 was negatively correlated with free triiodothyronine (FT3), free thyroxine (FT4), and thyroid peroxidase antibodies (TPOAb) while being positively correlated with thyrotropin (TSH). Logistic regression analyses demonstrated that serum ANGPTL8 was significantly associated with Graves’ disease (p < 0.05).
Conclusions
Circulating concentrations of ANGPTL8 showed a significant reduction in Graves’ disease patients. Thus, it is suggested that thyroid function should be taken into consideration when evaluating the results of ANGPTL8.
Keywords: ANGPTL8, Graves’ disease
Introduction
Angiopoietin-like protein 8 (ANGPTL8), which is also known as TD26 [1], refeeding-induced fat and liver protein (RIFL) [2], lipasin [3], and betatrophin [4], is an atypical member of the ANGPTL family [5]. It is a newly identified protein, composed of 198 amino acids, which is predominantly expressed in liver in humans, while mouse ANGPTL8 is highly enriched in adipose tissue and liver. Over the past few decades, increasing numbers of researchers have focused on the study of ANGPTL8. Recent studies have revealed that ANGPTL8 plays a significant role in several metabolic diseases, in particular, type 2 diabetes mellitus (T2DM) [6–8], obesity [9–11], non-alcoholic fatty liver disease (NAFLD) [12], and polycystic ovary syndrome (PCOS) [13].
Hyperthyroidism is a pathological disorder in which excess thyroid hormone is synthesized and secreted by the thyroid gland. Prevalence of hyperthyroidism is 0.8% in Europe [14] and 1.3% in the USA [15]. The most common cause of hyperthyroidism is Graves’ disease, followed by toxic nodular goiter. Graves’ disease is an autoimmune thyroid disease with such symptoms as weight loss, heat intolerance, tachycardia, and mental disturbances. Recently, many studies have demonstrated that changes in thyroid function are associated with changes in energy metabolism [16–18]. Graves’ disease has deleterious metabolic effects on lipid, carbohydrate, and amino acids metabolism [19, 20].
Previous research has shown that the levels of circulating hepatocyte- and adipocyte-derived metabolic regulators were altered in patients with thyroid diseases, such as leptin, resistin, adiponectin, and FGF21 [21, 22]. Recently, Han et al. reported that circulating ANGPTL8 was elevated in patients with overt hypothyroidism and subclinical hypothyroidism [23]. However, little is to date known as to whether circulating ANGPTL8 levels are altered in Graves’ disease. In this study, we aimed to determine the levels of serum ANGPTL8 in normal control subjects and patients with Graves’ disease while further exploring the factors associated with ANGPTL8 levels.
Materials and methods
Subjects
A total of 128 subjects were recruited in this study: 68 healthy control subjects and 60 patients diagnosed with Graves’ disease who were prepared to receive 131I treatment. GD patients were required to discontinue antithyroid drug (ATD) therapy for more than 2 weeks before the treatment. Pretreatment protocol also included obtainment of informed consent, negative pregnancy test, ultrasound measured thyroid or nodule volume, hormonal status, and thyroid scintigraphy. All patients were placed on a low-dose iodine diet 10 days prior to therapy. Individuals with diabetes mellitus, renal disease, nephritic range proteinuria, coronary heart disease, heart failure, peripheral artery disease, cerebrovascular event and malignancy, or other known major diseases were precluded from the study.
Diagnostic criteria
The diagnosis of Graves’ disease was documented by clinical and biochemical evidence of hyperthyroidism, diffused goiter, and the presence of positive thyrotropin (TSH) receptor autoantibody tests, diffusely increased 131I (iodine-131) uptake in the thyroid gland, or the presence of exophthalmos.
Anthropometric and biochemical measurements
Height and weight of all patients were measured to the nearest 0.1 cm and 0.1 kg, respectively, and BMI was calculated as weight divided by height squared (kg/m2). Blood samples were withdrawn from an antecubital vein after a 10-h overnight fasting. After clotting, blood specimens were separated by centrifugation. Serum samples were subsequently stored at − 80 °C until immediate analysis of ANGPTL8. Serum glucose levels were determined using the glucose oxidase method. Alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma glutamyl transpeptidase (GGT), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), total cholesterol (TC), apolipoprotein A (APOA), apolipoprotein B (APOB), and triglycerides were measured by the kinetic method (Beckman Coulter Inc., Brea, CA, USA). Serum free thyroxine (FT4), free triiodothyronine (FT3), thyrotropin (TSH), thyroid peroxidase antibody (TPOAb), thyroglobulin (Tg), antithyroglobulin antibody (TgAb), and TSH receptor autoantibody (TRAb) were tested with a chemiluminescence immunoassay (Beckman Coulter Inc., Brea, CA, USA). The radio iodine uptake (RAIU) value was obtained 2, 6, and 24 h after an oral tracer dose (about 1850 kBq) of 131I through a nuclear multifunctional instrument (MN-6110XTThyroid function instrument). Thyroidal 131I uptake was calculated according to the following equation: RAIU (%) = (neck counts − background counts) × 100/ (standard counts – background counts).
Measurement of ANGPTL8
Serum levels of ANGPTL8 were determined using a commercially available human ELISA Kit (catalog no. E11644h; Wuhan Eiaab Science, Wuhan, China) with an intra-assay coefficient of variation (CV) of ≤ 4.8% and an inter-assay CV of ≤ 7.2%. A calibration curve was constructed by plotting the absorbance values at 450 nm versus the ANGPTL8 concentrations of the calibrators, by which concentrations of samples were determined.
Statistical analysis
All statistical analyses were performed using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). Data were summarized as means ± standard deviations for normally distributed variables, medians plus percentiles (25th; 75th) for non-normally distributed variables, and frequencies for categorical variables. For comparisons between case and control subjects, the independent Student’s t test was used for normally distributed variables, while the non-parametric test was used for non-normally distributed variables. Categorical variables were examined by the x2 test. Partial correlation coefficients were calculated to evaluate the associations between serum ANGPTL8 and clinical and laboratory measurements. Partial correlation was used to determine the associations after adjusting for the effects of age, sex, and BMI. Binary logistic regression analyses were performed on the association of ANGPTL8, which were stratified in quartiles to estimate the odds ratio of Graves’ disease in each quartile, using the lowest quartile as the reference category. All calculated p values were two-sided and p values < 0.05 were considered statistically significant.
Results
Clinical and biochemical characteristics between the two groups
The clinical and biochemical characteristics of the subgroups studied (control and Graves’ disease) are summarized in Table 1. There were no statistically significant differences between Graves’ disease patients and control subjects with respect to age, sex, BMI, SBP, DBP, FPG, and APOA. Compared with those in the control group, pulse pressure, GGT, ALT, AST, triglycerides, FT3, FT4,TgAb, TPOAb, and Tg in the Graves’ disease group were significantly increased (p < 0.01 or p < 0.05), while TC, HDL-C, LDL-C, APOB, and TSH were significantly decreased (p < 0.01 or p < 0.05). The average of RAIU value and TRAb is above the normal range in the Graves’ disease group.
Table 1.
Clinical and biochemical characteristics
| Control | Graves’ disease | p | |
|---|---|---|---|
| Age (year)a | 44.43 ± 13.39 | 41.97 ± 13.1 | 0.297 |
| Sex (F/M)b | 68(36/32) | 60(41/19) | 0.076 |
| BMI (kg/m2)a | 21.88(19.93–23.1) | 21.03(19.72–22.58) | 0.115 |
| SBP (mmHg)a | 120.32 ± 13.83 | 123.06 ± 12.19 | 0.265 |
| DBP (mmHg)a | 75.53 ± 10.83 | 72.48 ± 7.88 | 0.090 |
| Pulse pressure (mmHg)a | 44.79 ± 10.03 | 50.57 ± 10.84 | 0.003* |
| FPG (mmol/L)a | 5.11 ± 0.41 | 5.12 ± 0.44 | 0.987 |
| GGT (U/L)a | 16.3(13–22.78) | 25.15(17.6–40.78) | < 0.001* |
| ALT (U/L)a | 12.65(10–21.23) | 28.55(19.68–45.93) | < 0.001* |
| AST (U/L)a | 1.17(1.08–1.23) | 19.3(13.7–29.1) | < 0.001* |
| Triglyceride (mmol/L) | 0.96 ± 0.28 | 1.13 ± 0.35 | 0.004* |
| TC (mmol/L)a | 4.35 ± 0.44 | 3.35 ± 0.62 | < 0.001* |
| HDL-C (mmol/L)a | 1.37 ± 0.26 | 1.11 ± 0.25 | < 0.001* |
| LDL-C (mmol/L)a | 2.24 ± 0.33 | 1.58 ± 0.47 | < 0.001* |
| APOA (g/L)a | 1.11(1.02–1.17) | 1.11(1–1.24) | 0.921 |
| APOB (g/L)c | 0.88(0.78–0.93) | 0.68(0.58–0.78) | < 0.001* |
| FT3 (pmol/L)c | 5.2(4.29–5.67) | 18.25(11.22–27.51) | < 0.001* |
| FT4 (pmol/L)c | 12.56(10.96–16.37) | 49.2(34.94–65.52) | < 0.001* |
| TSH (mIU/L)c | 1.86 ± 1.09 | 0.02 ± 0.04 | < 0.001* |
| TgAb (IU/mL)c | 0.35(0.1–11.16) | 4.85(0.73–69.83) | < 0.001* |
| TPOAb (IU/mL)c | 1.36(0.83–2.48) | 278.8(67.53–821.22) | < 0.001* |
| Tg (ng/mL)c | 8.35(4.6–12.49) | 18.35(2.13–75.05) | 0.007* |
| TRAb (IU/mL)a | – | 26.05(16.9–65.5) | – |
| RAIU (%) | |||
| 2ha | – | 46.03 ± 1.96 | – |
| 6ha | – | 67.65(54.53–76.18) | – |
| 24ha | – | 72.45(64.05–81.65) | – |
| ANGPTL8 (pg/mL)a | 326.41 ± 194.72 | 177.67 ± 135.07 | < 0.001* |
Data are presented as means ± SD, n (%), and median (25th and 75th percentiles). A p value of < 0.05 was considered significant (*)
F female, M male, BMI body mass index, SBP systolic blood pressure, DBP diastolic blood pressure, FPG fasting plasma glucose, GGT gamma glutamyl transpeptidase, ALT alanine aminotransferase, AST aspartate aminotransferase, TC total cholesterol, HDL-C high-density lipoprotein cholesterol, LDL-C low-density lipoprotein cholesterol, APOA apolipoprotein A, APOB apolipoprotein B, FT3 free triiodothyronine, T4 free thyroxine, TSH thyrotropin, TgAb anti-thyroglobulin antibody, TPOAb thyroid peroxidase antibody, Tg thyroglobulin, TRAb TSH receptor
aIndependent Student’s t test was used
bχ2 test was used
cNon-parametric test was used
Serum ANGPTL8 levels
Serum ANGPTL8 levels between the two groups were 326.41 ± 194.72 pg/mL for the control group as opposed to 177.67 ± 135.07 pg/mL for the Graves’ disease group. Compared with those in the control subjects, the levels of ANGPTL8 in Graves’ disease patients were significantly decreased (p < 0.001) (Fig. 1).
Fig. 1.
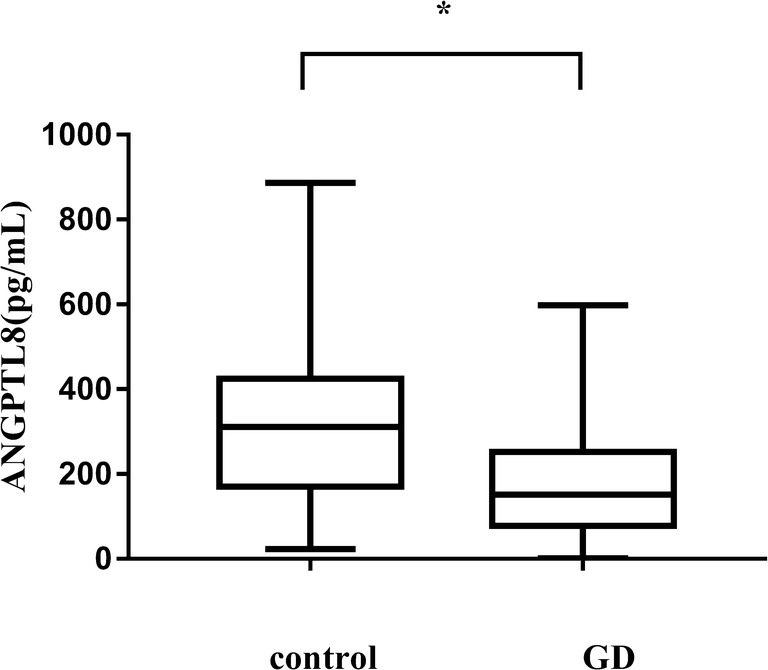
Serum ANGPTL8 was significantly decreased in the Graves’ disease (GD) group compared with the control group. *Statistically significant difference of ANGPTL8 levels between the two groups
The prevalence of Graves’ disease in the study subjects according to the quartiles of ANGPTL8
When ANGPTL8 concentrations were stratified in quartiles (Q1, 86.16 ± 33.24 pg/mL; Q2, 184.72 ± 29.29 pg/mL; Q3, 315.59 ± 43.87 pg/mL; Q4, 564.73 ± 147.12 pg/mL), the association was most pronounced for the fourth quartile, with an OR of 0.111 (95% CI 0.034–0.357, p < 0.001) in the age-, BMI-, and sex-adjusted model. This association was already present but less pronounced in the third quartile (age-, BMI-, and sex-adjusted: OR = 0.273 [95% CI 0.091–0.821], p = 0.021) (Fig. 2).
Fig. 2.

Forest plot illustrating the association of ANGPTL8 with Graves’ disease and providing data on ANGPTL8 divided into quartiles. ORs and 95% CLs are shown, and all the data are age-, sex-, and BMI-adjusted
Relationships between serum ANGPTL8 levels and biochemical variables
Table 2 depicts a correlation analysis between the biochemical variables and ANGPTL8 after adjustment for age, sex, and BMI. ANGPTL8 was negatively correlated with FT3 (r = − 0.302, p = 0.001), FT4 (r = − 0.386, p < 0.001), and TPOAb (r = − 0.304, p < 0.001), but positively correlated with LDL-C (r = 0.302, p = 0.006), TC (r = 0.267, p = 0.006), APOB (r = 0.246, p = 0.011), and TSH (r = 0.324, p < 0.001). It was also shown that ANGPTL8 had no correlation with SBP, DBP, pulse pressure, FPG, triglycerides, HDL-C, TgAb, Tg, TRAb, and RAIU.
Table 2.
Partial correlations analysis of variables associated with circulating ANGPTL8 levels in study subjects
| ANGPTL8 | ANGPTL8(age, sex, and BMI adjusted) | |||
|---|---|---|---|---|
| r | p | r | p | |
| Agea | 0.375 | < 0.001* | ||
| BMIa | 0.184 | 0.053 | ||
| SBPa | 0.203 | 0.029* | − 0.01 | 0.920 |
| DBPa | 0.185 | 0.046* | 0.02 | 0.843 |
| Pulse pressurea | 0.081 | 0.390 | − 0.028 | 0.776 |
| FPGa | 0.109 | 0.222 | − 0.044 | 0.647 |
| GGTa | − 0.046 | 0.603 | 0.003 | 0.979 |
| ALTa | − 0.119 | 0.182 | − 0.106 | 0.272 |
| ASTa | − 0.056 | 0.533 | − 0.069 | 0.476 |
| Triglyceridea | 0.095 | 0.290 | 0.014 | 0.888 |
| TCa | 0.333 | < 0.001* | 0.267 | 0.006* |
| HDL-Ca | 0.064 | 0.478 | 0.177 | 0.069 |
| LDL-Ca | 0.32 | 0.001* | 0.302 | 0.006* |
| APOAa | 0.05 | 0.578 | 0.117 | 0.232 |
| APOBb | 0.451 | < 0.001* | 0.246 | 0.011* |
| FT3b | − 0.323 | 0.001* | − 0.198 | 0.039* |
| FT4b | − 0.386 | < 0.001* | − 0.281 | 0.003* |
| TSHb | 0.324 | < 0.001* | 0.195 | 0.043* |
| TgAbb | − 0.196 | 0.027* | − 0.095 | 0.325 |
| TPOAbb | − 0.304 | < 0.001* | − 0.282 | 0.003* |
| Tgb | 0.085 | 0.342 | − 0.127 | 0.189 |
A p value of < 0.05 was considered significant (*)
BMI body mass index, SBP systolic blood pressure, DBP diastolic blood pressure, FPG fasting plasma glucose, GGT gamma glutamyl transpeptidase, ALT alanine aminotransferase, AST aspartate aminotransferase, TC total cholesterol, HDL-C high-density lipoprotein cholesterol, LDL-C low-density lipoprotein cholesterol, APOA apolipoprotein A, APOB apolipoprotein B, FT3 free triiodothyronine, FT4 free thyroxine, TSH thyrotropin, TgAb anti-thyroglobulin antibody, TPOAb thyroid peroxidase antibody, Tg thyroglobulin, TRAb TSH receptor autoantibody
aPearson’s correlation analysis was used
bSpearman’s correlation analysis was used
Discussion
In this study, we have demonstrated for the first time, to our knowledge, that serum ANGPTL8 concentrations were significantly decreased in Graves’ disease patients compared with the control subjects. Our data showed that ANGPTL8 was negatively correlated with FT3, FT4, and TPOAb, but positively correlated with TSH. Furthermore, the trend in the presence of Graves’ disease was more apparent in the lower serum ANGPTL8 quartile group. Recently, Han et al. reported that ANGPTL8 was increased in patients with overt and subclinical hypothyroidism. In that study, a total of 122 subjects were recruited, including patients with overt hypothyroidism (n = 31), subclinical hypothyroidism (n = 30), isolated TPOAb positivity (n = 30), and healthy controls (n = 31), according to thyroid function. Furthermore, they observed that ANGPTL8 was negatively correlated with FT4 (r = − 0.212, p = 0.02), and FT3 (r = − 0.225, p = 0.01), but positively correlated with TSH (r = 0.438, p < 0.001) [23]. Tseng et al. evaluated gene expression changes in T3-stimulated cells by DNA microarray analysis with the aim of identifying the genes in liver cells regulated by T3. In that study, however, they observed that the stimulation of FT3 led to upregulation of both mRNA and protein levels of ANGPTL8, which was dependent on the thyroid hormone receptor that binds to the ANGPTL8 upstream element [24]. Further studies are needed to elucidate the mechanisms underlying decreased ANGPTL8 levels in Graves’ disease patients.
In our research, we observed that serum ANGPTL8 concentrations were positively correlated with LDL-C, TC, and APOB, which suggested that ANGPTL8 might also be involved in lipid metabolism. A study performed by Fenzl et al. found that serum ANGPTL8 is significantly associated with TC, LDL-C, and APOB in patients with long-duration T2DM [25]. In a study of 559 subjects aged 14–28 years, Fu et al. observed that participants in the highest quartile of ANGPTL8 levels had the highest levels of TC, triglycerides, and LDL-C [26]. Sequence variants of the ANGPTL8 gene have been correlated with decreased HDL and LDL levels in Hispanic and African Americans [5]. This observation is in line with the positive correlation between ANGPTL8 and LDL-C in Graves’ disease participants reported here. Another study has shown that ANGPTL8 is a stress-response protein that regulates fat metabolism by suppressing adipose triglyceride lipase (ATGL) expression, revealing a mechanistic connection between ANGPTL8 and lipid homeostasis in mammalian cells [27]. It has been widely accepted that thyroid hormone has major effects on the metabolism of lipids [28–30]. Elevated levels of thyroid hormone in hyperthyroidism are associated with increased clearance of lipolysis and cholesterol. Investigations need to be carried out into whether the low levels of LDL-C, TC, and APOB in Graves’ disease might be mediated by decreased ANGPTL8 release. Given that ANGPTL8 is attracting ever more attention among researchers in the field of metabolic diseases, we recommend that further studies be conducted to elucidate the role of ANGPTL8 in the development of Graves’ disease.
The limitations of our study also require comment. Firstly, this study is limited by its cross-sectional design; thus, only associations (not causation) between serum ANGPTL8 and thyroid function could be addressed. Secondly, we divided subjects into groups according to thyroid function prior to random selection, which may have caused selection bias. Thirdly, serum ANGPTL8 levels may be affected by possible and variable acute stress experienced by the individual subjects. Due to these limitations, more large-scale population-based prospective studies are warranted.
In summary, our results indicate that circulating ANGPTL8 concentrations were significantly decreased in Graves’ disease patients. Moreover, serum ANGPTL8 was negatively correlated with FT3, FT4, and TPOAb, but positively correlated with TSH, TC, LDL-C, and APOB. ANGPTL8 may hence play a role in the pathogenesis of Graves’ disease.
Author contributions
Haoxiang Li, Mengjiao Xu, Li Zhao, Hong Xia, Yanyan Li, Xiafei Hong, Xia Deng, Jing Yuan, Yi Ding, Chang Guo, Ruirong Pan, Dong Wang, Jifang Wang, Wei Yin, Ling Yang, and Guoyue Yuan participated in the study design; and Chang Guo performed ELISA. Haoxiang Li, Mengjiao Xu, Li Zhao, and Hong Xia participated in the study design, analyzed the data, and wrote, reviewed, and edited the manuscript. Yanyan Li, Xiafei Hong, Xia Deng, Jing Yuan, Yi Ding, Chang Guo, Ruirong Pan, Dong Wang, Jifang Wang, and Wei Yin provided serum samples and contributed to discussions of data interpretation. All authors reviewed and edited the manuscript. Guoyue Yuan and Ling Yang are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding information
This study was supported in part by grants from the National Natural Science Foundation of China (81870548, 81570721), the Natural Science Foundation of Jiangsu Province, China (BK20151331), the High Caliber Medical Personnel Foundation of Jiangsu Province (LGY2016053), the Six Talent Peaks Project in Jiangsu Province (2015-WSN-006), the Scientific Research Projects of Jiangsu Health and Family Planning Commission (Y2018109) and the Social Development Project of Jiangsu Province (BE2018692).
Compliance with ethical standards
The study was approved by the Clinical Research Ethics Committee, Affiliated Hospital of Jiangsu University. Informed consent was obtained from participants.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Haoxiang Li and Mengjiao Xu contributed equally to this work.
Contributor Information
Haoxiang Li, Phone: +86 18260625726, Email: nfmlihaoxiang@163.com.
Mengjiao Xu, Phone: +86 15295086928, Email: xumengjiaojsdx@163.com.
Li Zhao, Phone: +86 15800578209, Email: zhaoli863@163.com.
Hong Xia, Phone: +86 18352862507, Email: jsdxxh@163.com.
Yanyan Li, Phone: +86 18352863766, Email: lyyface11@sian.com.
Xiafei Hong, Phone: +86 18352586939, Email: hxaifei@foxmail.com.
Xia Deng, Phone: +86 18252586949, Email: dengxia11@outlook.com.
Jing Yuan, Phone: +86 18260623823, Email: ycyj1993@outlook.com.
Yi Ding, Phone: +86 18260623342, Email: dingyi007@126.com.
Chang Guo, Phone: +86 13914557151, Email: ujsguochang@126.com.
Ruirong Pan, Phone: +86 15896382511, Email: ruirong123@163.com.
Dong Wang, Phone: +86 13605282460, Email: zjdongdonghao@aliyun.com.
Jifang Wang, Phone: +86 13646105408, Email: 13646105408@163.com.
Wei Yin, Phone: +86 13812457700, Email: yw0511@sohu.com.
Ling Yang, Phone: +86 13775329971, Email: lingyang70@163.com.
Guoyue Yuan, Phone: +86 13505289352, Email: yuanguoyue@hotmail.com, Email: yuanguoyue08@163.com.
References
- 1.Dong XY, Pang XW, Yu ST, Su YR, Wang HC, Yin YH, Wang YD, Chen WF. Identification of genes differentially expressed in human hepatocellular carcinoma by a modified suppression subtractive hybridization method. Int J Cancer. 2004;112:239–248. doi: 10.1002/ijc.20363. [DOI] [PubMed] [Google Scholar]
- 2.Santulli G. Angiopoietin-like proteins: a comprehensive look. Front Endocrinol. 2014;5:4. doi: 10.3389/fendo.2014.00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhang R. Lipasin, a novel nutritionally-regulated liver-enriched factor that regulates serum triglyceride levels. Biochem Biophys Res Commun. 2012;424:786–792. doi: 10.1016/j.bbrc.2012.07.038. [DOI] [PubMed] [Google Scholar]
- 4.Yi P, Park JS, Melton DA. Betatrophin: a hormone that controls pancreatic beta cell proliferation. Cell. 2013;153:747–758. doi: 10.1016/j.cell.2013.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 5.Quagliarini F, Wang Y, Kozlitina J, Grishin NV, Hyde R, Boerwinkle E, Valenzuela DM, Murphy AJ, Cohen JC, Hobbs HH. Atypical angiopoietin-like protein that regulates ANGPTL3. Proc Natl Acad Sci U S A. 2012;109:19751–19756. doi: 10.1073/pnas.1217552109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hu H, Sun W, Yu S, Hong X, Qian W, Tang B, Wang D, Yang L, Wang J, Mao C, Zhou L, Yuan G. Increased circulating levels of betatrophin in newly diagnosed type 2 diabetic patients. Diabetes Care. 2014;37:2718–2722. doi: 10.2337/dc14-0602. [DOI] [PubMed] [Google Scholar]
- 7.Chen X, Lu P, He W, Zhang J, Liu L, Yang Y, Liu Z, Xie J, Shao S, Du T, Su X, Zhou X, Hu S, Yuan G, Zhang M, Zhang H, Liu L, Wang D, Yu X. Circulating betatrophin levels are increased in patients with type 2 diabetes and associated with insulin resistance. J Clin Endocrinol Metab. 2015;100:E096–E100. doi: 10.1210/jc.2014-2300. [DOI] [PubMed] [Google Scholar]
- 8.Yi M, Chen RP, Yang R, Guo XF, Zhang JC, Chen H. Betatrophin acts as a diagnostic biomarker in type 2 diabetes mellitus and is negatively associated with HDL-cholesterol. Int J Endocrinol. 2015;2015:479157. doi: 10.1155/2015/479157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wu S, Gao H, Ma Y, Fu L, Zhang C, Luo X. Characterisation of betatrophin concentrations in childhood and adolescent obesity and insulin resistance. Pediatr Diabetes. 2016;17:53–60. doi: 10.1111/pedi.12233. [DOI] [PubMed] [Google Scholar]
- 10.Barja-Fernandez S, Folgueira C, Seoane LM, Casanueva FF, Dieguez C, Castelao C, Aguera Z, Banos R, Botella C, de la Torre R, Fernandea-Garcia JC, Fernandez-Real JM, Fruhbeck G, Gomez-Ambrosi J, Jimenez-Murcia TFI, Estivill X, Fernandez-Aranda F, Nogueiras R. Circulating betatrophin levels are increased in anorexia and decreased in morbidly obese women. J Clin Endocrinol Metab. 2015;100:E1188–E1196. doi: 10.1210/JC.2015-1595. [DOI] [PubMed] [Google Scholar]
- 11.Tuhan H, Abaci A, Anik A, Catli G, Kume T, Calan OG, Acar S, Bober E. Circulating betatrophin concentration is negatively correlated with insulin resistance in obese children and adolescents. Diabetes Res Clin Pract. 2016;114:37–42. doi: 10.1016/j.diabres.2016.02.008. [DOI] [PubMed] [Google Scholar]
- 12.Lee YH, Lee SG, Lee CJ, Kim SH, Song YM, Yoon MR, Jeon BH, Lee JH, Lee BW, Kang ES, Lee HC, Cha BS. Association between betatrophin/ANGPTL8 and non-alcoholic fatty liver disease: animal and human studies. Sci Rep. 2016;6:24013. doi: 10.1038/srep24013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sahin Ersoy G, Altun Ensari T, Vatansever D, Emirdar V, Cevik O. Novel adipokines WISP1 and betatrophin in PCOS: relationship to AMH levels, atherogenic and metabolic profile. Gynecol Endocrinol. 2017;33:119–123. doi: 10.1080/09513590.2016.1223286. [DOI] [PubMed] [Google Scholar]
- 14.Garmendia Madariaga A, Santos Palacios S, Guillen-Grima F, Galofre JC. The incidence and prevalence of thyroid dysfunction in Europe: a meta-analysis. J Clin Endocrinol Metab. 2014;99:923–931. doi: 10.1210/jc.2013-2409. [DOI] [PubMed] [Google Scholar]
- 15.Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, Braverman LE. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III) J Clin Endocrinol Metab. 2002;87:489–499. doi: 10.1210/jcem.87.2.8182. [DOI] [PubMed] [Google Scholar]
- 16.Silva JE. The thermogenic effect of thyroid hormone and its clinical implications. Ann Intern Med. 2003;139:205–213. doi: 10.7326/0003-4819-139-3-200308050-00010. [DOI] [PubMed] [Google Scholar]
- 17.Pontikides N, Krassas GE. Basic endocrine products of adipose tissue in states of thyroid dysfunction. Thyroid. 2007;17:421–431. doi: 10.1089/thy.2007.0016. [DOI] [PubMed] [Google Scholar]
- 18.Knudsen N, Laurberg P, Rasmussen LB, Bülow I, Perrild H, Ovesen L, Jørgensen T. Small differences in thyroid function may be important for body mass index and the occurrence of obesity in the population. J Clin Endocrinol Metab. 2005;90:4019–4024. doi: 10.1210/jc.2004-2225. [DOI] [PubMed] [Google Scholar]
- 19.Duntas LH, Biondi B. The interconnections between obesity, thyroid function, and autoimmunity: the multifold role of leptin. Thyroid. 2013;23:646–653. doi: 10.1089/thy.2011.0499. [DOI] [PubMed] [Google Scholar]
- 20.Han C, He X, Xia X, Li Y, Shi X, Shan Z, Teng W. Subclinical hypothyroidism and type 2 diabetes: a systematic review and meta-analysis. PLoS One. 2015;10:e0135233. doi: 10.1371/journal.pone.0135233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lee Y, Park YJ, Ahn HY, Lim JA, Park KU, Choi SH, Park DJ, Oh BC, Jang HC, Yi KH. Plasma FGF21 levels are increased in patients with hypothyroidism independently of lipid profile. Endocr J. 2013;60:977–983. doi: 10.1507/endocrj.EJ12-0427. [DOI] [PubMed] [Google Scholar]
- 22.Oge A, Bayraktar F, Saygili F, Guney E, Demir S. TSH influences serum leptin levels independent of thyroid hormones in hypothyroid and hyperthyroid patients. Endocr J. 2005;52:213–217. doi: 10.1507/endocrj.52.213. [DOI] [PubMed] [Google Scholar]
- 23.Han C, Xia X, Liu A, Zhang X, Zhou M, Xiong C, Liu X, Sun J, Shi X, Shan Z, Teng W. Circulating betatrophin is increased in patients with overt and subclinical hypothyroidism. Biomed Res Int. 2016;2016:5090852. doi: 10.1155/2016/5090852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Tseng YH, Ke PY, Liao CJ, Wu SM, Chi HC, Tsai CY, Chen CY, Lin YH, Lin KH. Chromosome 19 open reading frame 80 is upregulated by thyroid hormone and modulates autophagy and lipid metabolism. Autophagy. 2014;10:20–31. doi: 10.4161/auto.26126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fenzl A, Itariu BK, Kosi L, Fritzer-Szekeres M, Kautzky-Willer A, Stulnig TM, Kiefer FW. Circulating betatrophin correlates with atherogenic lipid profiles but not with glucose and insulin levels in insulin-resistant individuals. Diabetologia. 2014;57:1204–1208. doi: 10.1007/s00125-014-3208-x. [DOI] [PubMed] [Google Scholar]
- 26.Fu J, Hou C, Li L, Feng D, Li G, Li M, Li C, Gao S, Li M. Vitamin D modifies the associations between circulating betatrophin and cardiometabolic risk factors among youths at risk for metabolic syndrome. Cardiovasc Diabetol. 2016;15:142. doi: 10.1186/s12933-016-0461-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang Y, Li S, Donelan W, Xie C, Wang H, Wu Q, Purich DL, Reeves WH, Tang D, Yang LJ. Angiopoietin-like protein 8 (betatrophin) is a stress-response protein that down-regulates expression of adipocyte triglyceride lipase. Biochim Biophys Acta. 2016;1861:130–137. doi: 10.1016/j.bbalip.2015.11.003. [DOI] [PubMed] [Google Scholar]
- 28.Abdel-Gayoum AA. Dyslipidemia and serum mineral profiles in patients with thyroid disorders. Saudi Med J. 2014;35:1469. [PMC free article] [PubMed] [Google Scholar]
- 29.Risal P, Maharjan B, Koju R, Makaju R, Gautam M. Variation of total serum cholesterol among the patient with thyroid dysfunction. Kathmandu Univ Med J. 2010;8:265–268. doi: 10.3126/kumj.v8i2.3573. [DOI] [PubMed] [Google Scholar]
- 30.Lai Y, Wang J, Jiang F, Wang B, Chen Y, Li M, Liu H, Li C, Xue H, Li N, Yu J, Shi L, Bai X, Hou X, Zhu L, Lu L, Wang S, Xing Q, Teng X, Teng W, Shan Z. The relationship between serum thyrotropin and components of metabolic syndrome. Endocr J. 2011;58:23–30. doi: 10.1507/endocrj.K10E-272. [DOI] [PubMed] [Google Scholar]