

Abstract
Background:
Influenza like Swine flu virus has posed a greater risk of occupational transmission to dental professionals as it can spread through the aerosols.
Aim:
To assess knowledge and awareness of private dental health care professionals regarding swine flu of a Tricity in India.
Materials and Methods:
A cross-sectional study was conducted among 255 private dentists practising in the Tricity. A self-administered, anonymous, multiple choice type questionnaire was administered to gather information. The questionnaire contained 12 questions on knowledge and awareness regarding swine flu keeping in view the time constraints. Statistical analysis was done using ANOVA and student t-test.
Results:
Awareness regarding mode of transmission of swine flu were reported positively by 88.5% of subjects. About 24.6% of subjects reported about having encountered a swine flu patient at their clinic. Preventive measures to prevent spread of swine flu were known to 71.2% of subjects. Statistically significant association of mean knowledge scores was noted with education level (P = 0.015) and working profile (P = 0.017) of the subjects.
Conclusion:
The results of the present review showed that some knowledge gaps existed among dentists regarding some important aspects of swine flu. Therefore, there is an urgent need for training and continuous education programs regarding infectious diseases.
Keywords: Awareness, dentists, influenza A virus, knowledge, preventive measures
Introduction
Swine Flu or the influenza A (H1N1) Flu, is a highly contagious acute respiratory disease of pigs, caused by one of the several strains of swine influenza A.[1] This virus is spreads from person-to-person, probably in a similar manner like that of regular seasonal influenza viruses. The symptoms of swine flu in humans are similar to those of influenza namely chills, fever, sore throat, muscle pains, severe headache, coughing, weakness, and general discomfort. However, some persons having flu have shown serious respiratory illness, including pneumonia or respiratory failure leading to death.[2,3]
World Health Organization (WHO) On June 11, 2009, raised its pandemic alert level to the highest one indicating that a pandemic of H1N1 flu was underway.[4] There have been reporting of cases from mid-western United States, Kenya, Mainland China, Taiwan, Japan, and other parts of eastern Asia and in various parts of India.[5] In India, the states of Rajasthan and Gujarat were worst affected. India had reported 937 cases and 218 deaths from swine flu in the year 2014. According to recent data released by the Union Health Ministry, death toll across India due to swine flu has soared to 312 with the number of deaths till the first week of Feb 2019 recorded at 86.[6]
Dental environment exposes dental professionals to a variety of microorganisms that are transmittable via blood, oral or respiratory secretions. Dental health professionals are at a significant risk of exposure because of aerosol spread of swine flu.[7] Hence, they should have sound knowledge regarding the mode of symptoms, mode of transmission, and preventive measures so that there would be no infection spreading through the dental operatory. Therefore, the present study was conducted to:
Assess the knowledge and awareness of private dental health care professionals regarding swine flu in India.
Suggest possible measures to increase knowledge among dental professionals if required.
Materials and Methods
Ethical clearance and informed consent
The present study was conducted after obtaining ethical clearance from the Institutional Review Board of the college. Prior permission was obtained from the concerned health authorities and informed consent was obtained from the subjects for their willingness to participate in the study.
Study population and study sample
The present descriptive cross-sectional study was conducted among dental health professionals who are engaged in private practice in the Tricity (Chandigarh, Panchkula and Mohali). Local Indian Dental Association (IDA) bodies provided the list of all private dental practitioners of the Tricity. A pilot study was done on 30 subjects to check the feasibility of the study.
The sample size required for the study was calculated using the following equation:

where Z is the standard normal score with 95% confidence interval (CI) (a = 0.05), S is the standard deviation of the variable, and d is maximum acceptable error. To take account of potential errors and sample loss, which is common in cross-sectional studies, a final sample size was estimated to be 255. Simple random sampling methodology was employed to pick the study subjects from our sampling frame (list of all practicing dentists).
Research Instrument
A self-designed questionnaire written in English language (assessment by a specialist) was made specifically for the study. The questionnaire was pre-tested for validity and reliability. The reliability of the questionnaire was good (0.84). The questionnaire was divided into two sections- Section A was ‘General section’ which comprised of socio-demographic and professional details of the subjects (gender, educational status, type of practice, etc.) Section B comprised on 12 questions depicting knowledge and awareness regarding swine flu (mode of transmission, availability of vaccine, various preventive measures, complications, etc.) The questionnaire was handed over personally to study subjects after visiting them and collected next day so that the subjects get adequate time to fill. Total knowledge/awareness score was calculated on the basis of each participant's response. Each positive response was scored as “1” and negative as “0”. The total score of the participant was calculated by adding the sum of responses which ranged from 1 to 12, on a Likert Scale. The final scores were categorized at three levels- low (0-4), medium (5-8), and high (8-12).
Statistical analysis
Completed questionnaires were collected on the same day and prospectively analyzed. The present study conducted descriptive statistical analysis. Number and percentages were used to compute results on categorical measurements. Results were statistically analyzed using SPSS package version 15.0 (SPSS, Chicago, IL, USA). Analysis of Variance (ANOVA) was employed to find the significance of study parameters between three or more groups of participants and Student's t-test was used to find significance between two groups. The significance was set at < 0.05.
Results
Socio-demographic and professional profiles
Male subjects comprised two-third (166, 65%) of the total study population as compared to the female subjects (89, 35%) [Table 1]. Also, majority of the study subjects were graduates (152, 59.9%) as compared to post-graduates. Working profile of the subjects depicted that 63.5% (162) were engaged in both academic and private practice. 24.3% (62) of subjects were seeing more than 15 patients per day.
Table 1.
Socio-demographic and professional profile of study participants
| Profile | Number | Percentage | |
|---|---|---|---|
| Gender | Male | 166 | 65 |
| Female | 89 | 35 | |
| Educational status | Graduate (BDS) | 152 | 59.9 |
| Postgraduate (MDS) | 98 | 40.4 | |
| Working profile | Private | 93 | 36.5 |
| Combined (Private& Academic) | 162 | 63.5 | |
| Average no. of patients seen per day | Up to 7 | 107 | 41.9 |
| 8-15 | 86 | 33.7 | |
| More than 15 | 62 | 24.3 | |
Subjects’ response to the questionnaire
Figure 1 depicts the response of study subjects towards the questionnaire. Awareness regarding mode of transmission of swine flu were reported positively by 88.5% of subjects. When asked about the availability of vaccine to prevent flu, two-thirds of the subjects, 75% gave the correct answer. Surprisingly, only 24.6% of subjects reported about having encountered a swine flu patient at their clinic. Regarding preventive measures to prevent spread of swine flu, 71.2% of subjects answered correctly. More than 80% of subjects were of the opinion that government health care authorities can effectively deal with swine flu spread. Only few (32.5%) subjects were aware regarding government designated hospital to treat swine flu neat their clinic.
Figure 1.
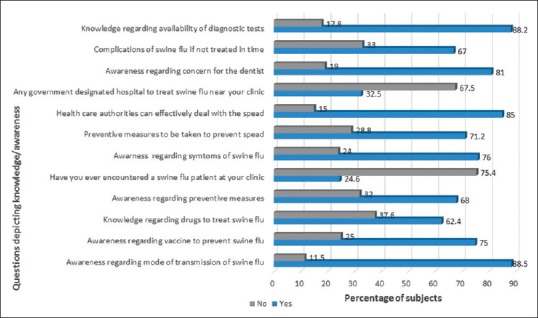
Subjects’ response to various questions regarding Swine Flu (H1N1 Influenza)
Knowledge score/awareness level of subjects
Among the study population, 44% (112) were having low knowledge scores, 32% (82) were having medium knowledge scores and high knowledge score were reported by only 24% (61) study subjects [Table 2]. When educational qualification of subjects was compared with their knowledge regarding swine flu, it was revealed that 52.4% of graduates were having low knowledge scores. Strangely, only 30.8% of post-graduate dental practitioners were having comprehensive knowledge (high scores) regarding swine flu [Figure 2]. Statistically significant association of mean knowledge scores was noted with education level (P = 0.015) and working profile (P = 0.017) [Table 3].
Table 2.
Knowledge scores regarding swine flu among study subjects (according to Likert scale)
| Knowledge score | Number of subjects | Percentage of subjects | 95% CI |
|---|---|---|---|
| Low | 112 | 44 | 46.12-53.46 |
| Medium | 82 | 32 | 28.55-36.48 |
| High | 61 | 24 | 17.61-25.62 |
| Total | 255 | 100 |
Figure 2.
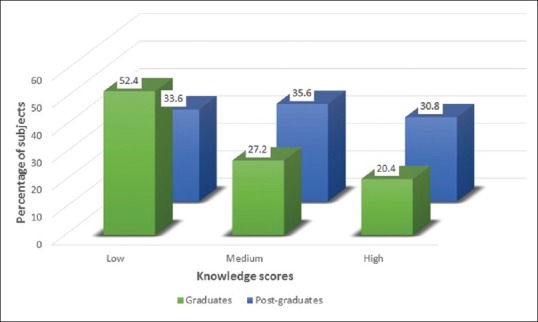
Knowledge scores regarding swine flu among graduates (BDS) and postgraduates (MDS)
Table 3.
Subjects’ mean knowledge scores according to different socio-demographic variables
| Socio-demographic variable | Knowledge score | P | |
|---|---|---|---|
| Mean | Standard Deviation | ||
| Gender | |||
| Male | 5.36 | 2.34 | |
| Female | 4.62 | 1.78 | F=1.634 |
| Total | 4.85 | 2.76 | P=0.074 |
| Education level | |||
| Graduate (BDS) | 5.22 | 3.21 | F=2.876 |
| Postgraduate (MDS) | 4.87 | 2.26 | P=0.015* |
| Total | 5.03 | 1.87 | |
| Working Profile | |||
| Private | 4.78 | 2.65 | F=2.765 |
| Combined | 5.12 | 1.44 | P=0.017* |
| Total | 4.88 | 2.65 | |
| No. of patients seen per day | |||
| Up to 7 | 3.54 | 2.62 | |
| 8-15 | 4.67 | 3.87 | F=2.653 |
| More than 15 | 4.86 | 3.21 | P=0.065 |
| Total | 4.42 | 4.34 | |
P<0.05 (Statistically significant), Tests used -Student-t test, ANOVA
Discussion
Pandemic outbreak caused by H1N1 virus and other infectious disease agents still remains the biggest threat to human beings due to high mortality rate associated with their infections.[7] The study revealed that majority of the subjects had fair knowledge regarding swine flu, yet there were notable deficiencies in some of the important aspects. To avoid recall bias, the study used a close ended questionnaire as these are easy to analyze and may achieve a quicker response from subjects.[8]
H1N1 influenza virus appears to be transmitted from one person to another through close contact as other influenza viruses does. A substantial no. of subjects had awareness regarding mode of transmission of swine flu in the present study which is in congruence to the findings of some other study[9] and another study conducted in Saudi Arabia.[10] However, hardly 50% of subjects had correct knowledge regarding this aspect in a study conducted on urban dental fraternity.[11] This information is crucial as not knowing about this may lead dentists to inappropriately triage patients.[12]
Following the pandemic alert by WHO, Government of India provided diagnostic and treatment facilities at designated hospitals in the endemic states.[13] However, only one-third of subjects were aware of such a facility in the present study. It is a concern in our study that hardly two-third of the subjects had knowledge regarding drugs (Tamiflu) which are used to treat flu. This is in contrast to findings of some other study conducted on health care providers in Delhi in which more than 90% of subjects had proper knowledge.[14] As per the Center for Disease Control and Prevention (CDC), Tamiflu is very effective among swine flu-positive patients.[15]
The main aim of any healthcare provider should be to prevent or limit the transmission of influenza virus to other health care providers as well as to the patients. More than 70% of subjects were aware regarding various preventive measures to be taken to prevent spread and more than 80% knew the reason for concern to the dentist in our study.
Swine flu infection is usually mild in most of the cases, but some patients with swine flu develop serious respiratory illness, including pneumonia or respiratory failure which could prove fatal.[16] This highlights the importance of providing appropriate care at the right time. Astonishingly, one-third of subjects in the present study were unaware regarding these complications.
Subjects who were post-graduates had more knowledge as compared to graduates. This might be due to the reason that with more education, knowledge also increases. Moreover, subjects doing combined practice had more knowledge as compared to subjects doing private practice (P = 0.017). This could be due to the reason that subjects engaged in academic teaching are exposed to more learning experiences as compared to subjects doing only private practice. Also, there was a statistically significant relationship of overall knowledge scores with education level (0.015) and working profile of the subjects (P = 0.017). However, knowledge scores were not influenced by number of patients seen or treated per day by the dentists in the study.
In the present study, there were a few limitations. Keeping in view the time constraints with respect to scheduled appointments of the dentist, a brief questionnaire was used in the study. Therefore, certain aspects related to swine flu (virus characteristics and treatment) could have been possibly left behind. Second, the study relied upon self-reported data; some subjects could have given socially acceptable responses and it is unknown whether the responses would accurately reflect the respondents’ real-world response.
Conclusion and Recommendations
The findings of the study revealed that most of the subjects had fair knowledge regarding swine flu, yet there were notable deficiencies in some of the important aspects as very few subjects possessed high knowledge scores. The present study highlights the need for suitable training regarding infectious diseases in the undergraduate and post graduate dental curriculum and continuous education programs so that the disease is contained at the early stage. Government can also help to spread awareness by organizing health campaigns and educational programs regarding transmission and prevention of swine flu in educational institutions. It is the responsibility of the primary care physician that various myths and misconceptions about this disease are cleared from the minds of the people. A primary care physician can diagnose this disease early, can give advice on various preventive measures to control the outbreak to prevent epidemic and can provide invasive support to deal with the complications if any by early utilization of available healthcare resources. Blood testing should be done in suspected cases by the primary care physician especially during the winter season in India for early diagnosis and intervention.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Rajao DS, Vincent AL, Perez DR. Adaptation of human influenza viruses to swine. Front Vet Sci. 2019;5:347. doi: 10.3389/fvets.2018.00347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rewar S, Mirdha D, Rewar P. Treatment and prevention of pandemic H1N1 influenza. Ann Glob Health. 2015;81:645–53. doi: 10.1016/j.aogh.2015.08.014. [DOI] [PubMed] [Google Scholar]
- 3.Verma R, Chayal V, Kumar R, Bhalla K, Dhankar M, Dhaka R, et al. Community perception about swine flu in an urban slum of Haryana: A cross-sectional study. J Family Med Prim Care. 2018;7:1515–20. doi: 10.4103/jfmpc.jfmpc_151_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kamate SK, Agrawal A, Chaudhary H, Singh K, Mishra P, Asawa K. Public knowledge, attitude and behavioural changes in an Indian population during the Influenza A (H1N1) outbreak. J Infect Dev Ctries. 2010;4:7–14. doi: 10.3855/jidc.501. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. World Health Statistics. [Last accessed on 2019 Feb 12]. Available from: http://www.who.int/gho/publications/world_health_statistics/2015/en .
- 6.Ministry of Health and Family Welfare, Government of India. [Last accessed on 2019 Feb 12]. Available from: http://mohfw.nic.in/press_releases_on_swine_flu.htm .
- 7.Kshatriya RM, Khara NV, Ganjiwale J, Lote SD, Patel SN, Paliwal RP. Lessons learnt from the Indian H1N1 (swine flu) epidemic: Predictors of outcome based on epidemiological and clinical profile. J Family Med Prim Care. 2018;7:1506–9. doi: 10.4103/jfmpc.jfmpc_38_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hasan F, Khan MO, Ali M. Swine flu: Knowledge, attitude, and practices survey of medical and dental students of Karachi. Cureus. 2018;10:e2048. doi: 10.7759/cureus.2048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kaipa S, Epari V, Gupta S. Knowledge and attitude towards swine influenza (2009) among dental practitioners in Nellore district of Andhra Pradesh, India. J Educ Ethics Dent. 2011;1:52–8. [Google Scholar]
- 10.Balkhy HH, Abolfotouh MA, Al-Hathlool RH, Al-Jumah MA. Awareness, attitudes, and practices related to the swine influenza pandemic among the Saudi public. BMC Infect Dis. 2010;10:42. doi: 10.1186/1471-2334-10-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Palwankar P, Mehta V, Sheokand V, Palwankar D, Anand P. Knowledge, awareness, perception of H1N1 flu in urban dental fraternity. Res J Pharm Biol Chem Sci. 2015;6:1566–72. [Google Scholar]
- 12.Di Giuseppe G, Nobile CG, Marinelli P, Angelillo IF. A survey of knowledge, attitudes, and behavior of Italian dentists toward immunization. Vaccine. 2007;25:1669–75. doi: 10.1016/j.vaccine.2006.10.056. [DOI] [PubMed] [Google Scholar]
- 13.Media release, Ministry of health and family welfare, Government of India. [Last accessed on 2019 Feb 18]. Available from: http://mohfw-h1n1.nic.in/link6.html .
- 14.Rajoura OP, Roy R, Agarwal P, Kannan AT. A study of the swine flu (H1N1) epidemic among health care providers of a medical college hospital of Delhi. Indian J Community Med. 2011;36:187–90. doi: 10.4103/0970-0218.86518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kmietowicz Z. Tamiflu reduces complications of flu, new review finds. BMJ. 2015;350:h537. doi: 10.1136/bmj.h537. [DOI] [PubMed] [Google Scholar]
- 16.Paccha B, Neira-Ramirez V, Gibbs S, Torremorell M, Rabinowitz PM. Swine worker precautions during suspected outbreaks of influenza in swine. J Environ Health. 2016;78:22–6. [PubMed] [Google Scholar]