

Abstract
Adolescents in sub-Saharan Africa are highly vulnerable to HIV, other sexually transmitted infections (STIs) and unintended pregnancies. Evidence for the effectiveness of individual behaviour change interventions in reducing incidence of HIV and other biological outcomes is limited, and the need to address the social conditions in which young people become sexually active is clear. Adolescents’ peers are a key aspect of this social environment and could have important influences on sexual behaviour. There has not yet been a systematic review on the topic in sub-Saharan Africa.
We searched 4 databases to find studies set in sub-Saharan Africa that included an adjusted analysis of the association between at least one peer exposure and a sexual behaviour outcome among a sample where at least 50% of the study participants were aged between 13 and 20 years. We classified peer exposures using a framework to distinguish different mechanisms by which influence might occur.
We found 30 studies and retained 11 that met quality criteria. There were 3 cohort studies, 1 time to event and 7 cross-sectional. The 11 studies investigated 37 different peer exposure-outcome associations. No studies used a biological outcome and all asked about peers in general rather than about specific relationships. Studies were heterogeneous in their use of theoretical frameworks and means of operationalizing peer influence concepts. All studies found evidence for an association between peers and sexual behaviour for at least one peer exposure/outcome/sub-group association. Of all 37 outcome/ exposure/sub-group associations tested, there was evidence for 19 (51%). There were no clear patterns by type of peer exposure, outcome or adolescent sub-group.
There is a lack conclusive evidence about the role of peers in adolescent sexual behaviour in Sub-Saharan. We argue that longitudinal designs, use of biological outcomes and approaches from social network analysis are priorities for future studies.
Keywords: Systematic review, Young people, Peer exposure, Social networks, Sexual behavior, Sub-Saharan Africa
1. Introduction and rationale
HIV prevalence remains high in sub-Saharan Africa and reducing incidence in adolescence is critical (UNAIDS, 2014). The majority of HIV transmission in sub-Saharan Africa occurs via sex and risk of infection varies by sexual behaviour, including early sexual debut (Stöckl et al., 2013; Wand and Ramjee, 2012), having multiple partners, and inconsistent condom use (Pettifor et al., 2005). The characteristics of young people’s sexual partners might also influence risk and some studies have found having older partners to increase risk among young women (Gregson et al., 2002; Kelly et al., 2003; Pettifor et al., 2005).
However, individuals’ behaviours take place within a wider social environment and in the context of their social relationships. Adolescents’ peers have been found to be influential on sexual behaviour in other settings (Ali and Dwyer, 2011; Billy and Udry, 1985). Peers, who grow in importance as children transition to adolescence (Berndt, 1979; Steinberg and Monahan, 2007), might also play an important role in influencing the sexual behaviour and thus the long-term health of adolescents in sub-Saharan Africa.
There are a variety of mechanisms by which peers could be influential on sexual behaviour. Adolescents could be influenced via normative mechanisms, with norms being either ‘descriptive’, that is the perceived prevalence of a behaviour amongst peers, or ‘injunctive’, that is the perceived peer approval of a behaviour (Cialdini and Reno, 1990). Alternatively, adolescents’ connections to their peers could help to buffer them against stresses and potentially decrease risky sexual behaviours (Alloway and Bebbington, 1987; Barker, 2007; Markham et al., 2010). Communication might enforce norms or provide information. Peers provide social connections to other individuals, and older peers might in turn introduce adolescents to older partners. Meanwhile, an adolescent’s position within the overall structure of social ties (Ellen et al., 2001; Moody, 2009; Prinstein et al., 2003; Valente, 1995) might influence, or be reflective of, decisions about sexual behaviour.
Despite their potential for influence, and the importance of sexual behaviour in the context of the high risk of acquiring HIV among young people in the region, there has been no review of peer exposures on adolescent sexual behaviour in sub-Saharan Africa. One review of factors affecting adolescent sexual behaviour globally found that most but not all studies found that perceiving more peers to be sexually active increased the likelihood that 11–18 year-olds reported ever having had sex themselves (Buhi and Goodson, 2007). Another examining the role of ‘connectedness’, defined as bonding, or emotional attachment and commitment in social relationships, found both protective and risk-promoting associations between peer connectedness and sexual behaviour across studies (Markham et al., 2010). Neither included studies from sub-Saharan Africa.
Here we examine the quantitative evidence for the role of peers in shaping young people’s sexual behaviour in sub-Saharan Africa across different types of sexual behaviour important to risk of becoming infected with HIV and categorised by type of peer influence exposure.
2. Methods
Review methodology was guided by the PRISMA checklist, designed to improve the reporting of systematic reviews in health (Moher et al., 2009). We included studies set in or partially (and distinguishably) in Sub-Saharan Africa and where at least 50% of the age range of participants fell between 13 and 20 years. Out-comes of interest included HIV or STI infection, pregnancy, sexual debut, condom use and characteristics of sexual partners. Exposure measure(s) related to participants’ peers and/or friends, including those who shared demographic characteristics with participants, for example other young people whom participants might know and interact with and who therefore could be a plausible source of influence. While studies generally took their own definition of ‘peer’ or did not define it clearly, exposures that included only parents, teachers, or family were not included. Studies were included if they reported a measure of effect between a peer exposure and an outcome of interest adjusted for confounders, and stratified or adjusted for gender. Evaluations of peer-led HIV prevention or sexual health interventions, which have been reviewed elsewhere (Maticka-Tyndale and Barnett, 2010; Medley et al., 2009), were not included except where these examined peer influence at baseline. Only articles in English were included. Unpublished and non-peer reviewed literature were not included. We searched Pubmed, Web of Science, Global Health and Adolescent Health databases, last updating in April 2014, using search terms 1) for adolescents/young people; 2) for sexual behaviour or outcomes of sexual behaviour (pregnancy, HIV, STIs); 3) for peers or social influence; 4) and for sub-Saharan African location. Details are given in Appendix 1.
An initial shortlist of articles was determined by title and abstract review and then refined by reading the full articles. If studies using the same datasets were found to be using the same exposures and outcomes, only one paper was retained. We adapted criteria for assessing the methodological quality of non-randomised studies, using the Newcastle—Ottawa Scale (Wells et al.), (also adapted for use with cross-sectional studies (Anglin et al., 2013)), and checked these against frameworks for assessing evidence for peer influence (Ali and Dwyer, 2011; Bramoullé et al., 2007; Manski, 1993). We included only those studies that had a cohort design and/or met higher quality in 6 out of the 10 criteria described in Table 1 to strike a balance between breadth of studies and quality of estimates.
Table 1.
Methodological quality criteria.
| Characteristics of studies | Higher quality | Lower quality |
|---|---|---|
| Selection | ||
| Representativeness of sample to population | Randomly selected sample of population of interest | Non-random sample of population of interest |
| Response rate and lost to follow-up (cohort studies) | Response rate > 80%, follow-up rate > 80% if a cohort study | Low response rate |
| Sample size | Justified sample size or sample size >1000 | Not justified or unsatisfactory |
| Data collection | Self-administered surveys or other adequate measures to reduce social desirability bias | High likelihood of bias (e.g., questionnaire administered by authority figure), or no description |
| Ascertainment of peer exposures | Clear definition of peer exposures, situated within a theoretical framework. | No theoretical explanation for choice of peer exposure/unclear measurement |
| Comparability | ||
| Participants in different outcome and exposure groups comparable | Adequate adjustment for possible confounders to establish comparability | Problems with adjustment strategy for establishing comparability |
| Outcome | ||
| Assessment of outcome | Biological outcome | Self-reported behaviour |
| Ability to distinguish selection from influence effects | Cohort study or other justified method | Outcome and exposure assessed at same time point, no justified approach to distinguishing selection and influence |
| Statistical tests | Appropriate and justified | Some problems with analytical approach |
| Avoidance of over-adjustment | Justified approach for adjustment and accounting for possible causal pathways | Backwards selection of variables, no justification given |
Each study was scored 0 for meeting lower or 1 for meeting higher quality for each criterion.
We classified peer exposures as belonging to one of six types:
Peer socio-demographic attributes, such as age, gender, or in-school status. We hypothesised these could influence the behaviour of adolescents perhaps by influencing perceived norms about their behaviours, or they might affect whom an adolescent comes into contact with, potentially acting as social network bridges to influential people or situations.
Perceived peer behaviours (descriptive norms) could provide models of behaviour to be emulated, and are most often assessed by asking adolescents to indicate the number of their peers, classmates or friends who engage in particular behaviours.
Peer approval (injunctive norms) might cause adolescents to adapt their behaviour in a process similar to that involved with descriptive norms, but injunctive norms might or might not differ from the behaviours that adolescents perceive their friends to actually be engaged in.
Peer communication could play a role in diffusing information, perceived peer behaviours or norms, or provide a context in which adolescents could question or re-negotiate dominant norms.
Peer connectedness, or social and emotional support. This is sometimes measured as a count of relationships, a scale of their quality, or a score to indicate the degree to which an adolescent’s peers are connected to each other might influence behaviour. We include self-esteem in the domain of peer relationships to be in this category.
Status and position within the network of peer relationships could determine an adolescent’s exposure to information, resources and behaviours that might influence their behaviour. Additionally, given the normative pressures on behaviour, network position might reflect popularity and status amongst peers.
We did not conduct a formal meta-analysis due to study heterogeneity, but explored trends across findings by sub-groups, exposures and outcomes. We first considered statistical evidence for effects investigated (p < 0.05 was ‘good evidence’) and then further discuss these findings in the context of study design and possible biases.
3. Results
We screened 4512 abstracts (including duplicates) and 487 full papers, identifying 30 studies meeting the inclusion criteria, and 11 meeting quality appraisal criteria (Fig. 1). We dropped two studies (Rudatsikira et al., 2007; Siziya et al., 2008) because they analysed smaller subsets of the same data as a larger study (Peltzer, 2010), two studies because reported results were inconsistent in tables and text (Adedimeji et al., 2008; Negeri, 2014) and one because it was unclear how the outcome variable was operationalized (Abebe et al., 2013). We then retained only those 11 studies meeting higher methodological quality criteria.
Fig. 1.
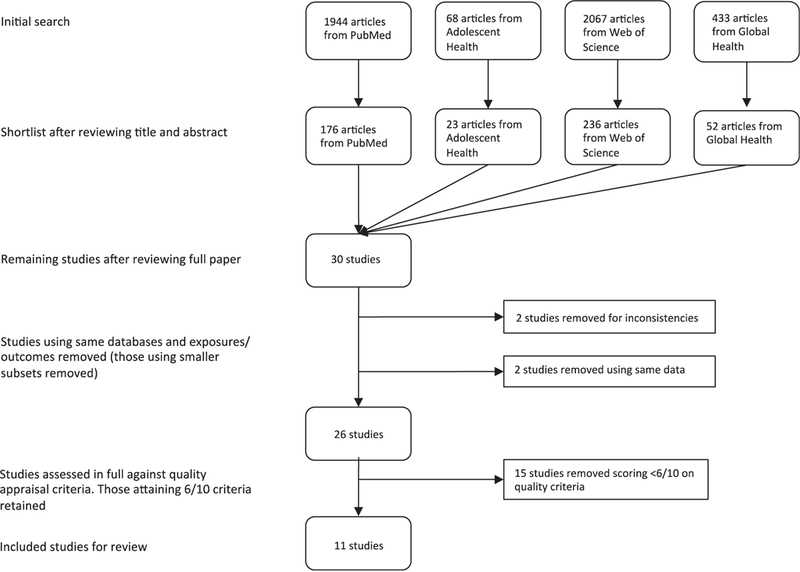
Studies found at each stage of search.
3.1. Study characteristics
The 11 included studies (Table 2) collected data between 2001 and 2009 from urban and rural locations in eastern, southern and western Africa. Three cohort studies examined transition to first sex, and one time-to-event study investigated factors associated with time to first sex. The rest were cross-sectional. The age range included 12–24 year-olds, and all studies included both male and female participants. Sample sizes ranged from 633 to 3840.
Table 2.
Overview of included studies.
| Study, year published, country |
Year data collected | Study sample size | Study population | Study design | Outcomes | Peer exposures types investigated |
Number of peer exposure associations investigated |
|---|---|---|---|---|---|---|---|
| Kabiru et al., 2010, Kenya | 2005–2006 | 2134 | Ages 12–19, girls and boys Slum and non-slum settlements, Nairobi. | Cohort, 12 months follow-up time. | Transition to first sex | Peer behaviours | 8 (male and female, two peer exposures, two age groups) |
| Lam et al., 2013, South Africa | 2002–2006 | 1491 | Ages 14–17, girls and boys who had never had sex of baseline. Subset of 14–22 year-olds participating in the Cape Area Panel Study. Two-stage probability sample, oversampling of White and African participants. | Cohort, 4 years follow-up time. | Transition to first sex; age difference with first sexual partner | Peer socio-demographic attributes | 4 (2 outcomes, male and female) |
| Kawai et al., 2008, Tanzania | 2004–2005 | 2477 | 12–14 year-old girls and boys, never sexually active at baseline. Participants were part of a school-based RCT to prevent HIV. 24 schools were randomly selected from 108 in one of three districts in Dar es Salaam. | Cohort, 6 months follow-up time. | Transition to first sex | Peer behaviours, peer norms | 2 (two peer exposures) |
| Mkandawire et al., 2013, Malawi | 2009 | 1214 | Males and females aged 12 −18 year-olds randomly selected from households enumerated in a population census in Mzuzu city, northern Malawi. | Time to event | Age at first sex | Peer connectedness | 2 (male and female) |
| Balabola et al., 2002, Rwanda | 2001 | 1327 | Males and females aged 15 −24 randomly selected from households from 4 Rwandan provinces using multi-stage sampling. | Cross-sectional | Sexual abstinence (ever sex), condom use at last sex | Peer approval norms | 3 (male and female, 2 peer exposures) |
| Brook et al., 2006, South Africa | 2001–2002 | 633 | 12–17 year-olds in recruited from households in Durban. Multi-stage sampling to be representative of ethnic and socioeconomic composition of city. | Cross-sectional | Risky sex (ever sex, multiple partners, condom use, sex while drunk/ stoned) | Peer behaviours | 3 (male and female and combined gender analyses) |
| Cherie and Berhane, 2012, Ethiopia | Not reported | 3840 | 15–24 year-old youth attending high school in Addis Ababa recruited using multi-stage sampling among city districts, schools and grade sections. | Cross-sectional | Ever anal sex, ever oral sex | Peer behaviours | 2 (2 outcomes) |
| Harrison et al., 2012, South Africa | 2003 | 983 | 14–17 year olds from rural Kwa-Zulu Natal recruited in preparation for a school-based HIV prevention. Participants selected by multi-stage sampling limited to areas in which an African Youth Alliance programme was delivered. | Cross-sectional | Ever sex, condom use at last sex | Peer behaviours | 6 (male and female, 2 outcomes, peer exposures by peer gender) |
| Kakoko, 2013, Tanzania | Not reported | 2820 | Students in primary schools from 22 randomly selected district, Tanzania. Final sample included those aged 12–14 years from the 3180 total surveyed in Standard (grades) 5 and 6. | Cross-sectional | Ever sex | Peer approval norms | 1 |
| McQuestion et al., 2012, Ghana | 2006 | 3416 | Young women and men aged 17–22. The sampling procedure was designed to assess an African Youth Alliance programme. Municipalities were chosen from the 2000 census and from a list of areas with AYA interventions. Within municipalities, two-stage sampling was used to select enumeration areas. | Cross-sectional | Ever sex, age at first sex | Peer approval norms | 4 (male and female, 2 outcomes) |
| Wild et al., 2004, South Africa | Not reported | 939 | Students in Grades 8–11 from public high schools in Cape Town. Schools stratified by postal code and selected proportional to the number of students in the stratum. 2 classes per grade were randomly selected. | Cross-sectional | Risky Sex (>2 partners in previous 12 months, not using contraception, knowing most recent partner <7 days before intercourse) | Peer connectedness | 2 (male and female) |
No studies measured biological outcomes, nine investigated sexual debut outcomes, two condom use, one age difference with first sexual partner, and two created composite variables to describe risky sex. One study examined perceived behaviour by same and opposite sex peers (Harrison et al., 2012). Only one study examined a main effect of peer socio-demographic attributes, cumulative exposure to older classmates over time (Lam et al., 2013). In all other studies, peer exposures were participant-reported. Peer connectedness was examined in two studies as peer self-esteem (Wild et al., 2004) and as number of close friends (Mkandawire et al., 2013). No included study investigated communication with peers about sex and sexual behaviour outcomes, nor peer connectedness, nor popularity/position amongst peers.
Nine studies placed peer exposures within a theoretical framework: three studies (Cherie and Berhane, 2012; Kawai et al., 2008; McQuestion et al., 2012) used individual behavioural theories such as social cognitive theory or the Theory of Planned Behaviour to explain adolescent sexual behaviour, four used ecological frameworks, two used concepts of ‘risks clustering’, one cited a ‘protection-risk’ and one drew on a social networks or contagion theoretical framework (Lam et al., 2013).
Perceived peer behaviour (descriptive norms) was incorporated into a variety of theoretical frameworks. In three studies, the peer behaviour matched the outcome of interest (Cherie and Berhane, 2012; Kawai et al., 2008; McQuestion et al., 2012), while in two studies composite measures of peer behaviours were developed and employed in a ‘protection-risk framework’ (Kabiru et al., 2010) and as mediators of more distal socioeconomic factors (Brook et al., 2006). Peer approval norm exposures played a similar role as descriptive norms (Kawai et al., 2008; McQuestion et al., 2012). Classmate age, the only peer attribute exposure examined, was viewed as determining the normative influences that adolescents would be exposed to, as older peers would be more likely to have had sex (Lam et al., 2013). Peer connectedness was considered to be a facet of social support in one study without a named theoretical framework (Mkandawire et al., 2013) and similarly peer self-esteem, which was seen as a trait giving rise to clustered risk behaviours including risky sex (Wild et al., 2004).
We next turn our attention to the findings of each of the selected studies, reported in Table 3 and organised first by sexual behaviour outcome and secondly by type of peer exposure.
Table 3.
Study findings by outcome and peer exposure type.
| Study | Study design | Outcome | Exposure type | Exposure | Other factors adjusted for |
Gender | Age in years at baseline |
Analysis sample size |
Estimate of peer exposure |
|---|---|---|---|---|---|---|---|---|---|
| Sexual debut | |||||||||
| Lam et al., South Africa | Cohort | Transition to first sex | PA | Estimated cumulative exposure to peers 2 + years older in school since age 12. (Cumulative exposure is equal to 1.0 if there was a 25% increase in the number of classmates 2 + years older each year for 4 years, or of 50% for 2 years, for example). | Quadratic age of participants in months, enrolled in school in 2002, grade enrolled in 2002, mother’s and father’s education, race, living with mother/father in 2002, household income, number of months between follow-up interviews, literacy/numeracy test score. | Female | 14–17 | 808 | 13.8% more likely to have had sexual debut during follow-up for each 1.0 cumulative exposure to classmate peers aged 2 + years older since age 12, p < 0.05 |
| PA | Male | 14–17 | 683 | 7.1% more likely to have had sexual debut for each 1.0 cumulative exposure to classmate peers aged 2 + years older since age 12, p > 0.05 | |||||
| Kabiru et al., Kenya | Cohort | Transition to first sex | PB | Proportion of peers engaging in unconventional behaviour (sex, substances, trouble with police, run away from home) at baseline. | Slum residence, school enrolment, number of adolescents in household, perceived parental modelling, peer models for conventional behaviour, whether had nonpenetrative sexual contact, delinquent behaviour, substance use. | Female | 12–15 | 357 | aOR 0.9, 95% CI 0.7–1.1 |
| PB | 16–19 | 93 | aOR = 1.8, 95% CI 1.1–2.8 | ||||||
| PB | Male | 12–15 | 336 | aOR = 0.8, 95% CI 0.5–1.2 | |||||
| PB | 16–19 | 94 | aOR = 1.2, 95% CI 0.8–1.6 | ||||||
| PB | Proportion of peers engaging in conventional behaviour (get good marks at school, go to church/mosque, participate in sports/school activities, want to go to secondary school/university/ college) at baseline. | As above | Female | 12–15 | 357 | aOR = 0.8, 95% CI 0.6–1.1 | |||
| PB | 16–19 | 93 | aOR 0.8, 95% CI 0.5–1.1 | ||||||
| PB | Male | 12–15 | 336 | aOR = 0.8, 95% CI 0.6–1.1 | |||||
| PB | 16–19 | 94 | aOR = 0.8, 95% CI 0.6–1.1 | ||||||
| Kawai et al., Tanzania | Cohort | Transition to first sex | PB | Perceived prevalence of students in their age group who had ever had sex. 6 point scale, measured at baseline. | Age, gender, living with mother, have a boyfriend/girlfriend, alcohol use, attitudes towards delayed sex, intention to have sex, intervention control group, social norms about delayed sex. | Both | 12–14 | 2477 | High (5–6 points) compared to low (1–2 points): aOR = 1.99, 95% CI 1.3–3.06 Moderate (3–4 points) to low (1–2 points): aOR = 1.31, 95% CI 0.83–2.08. Test for trend p = 0.002 |
| Harrison et al., South Africa | Cross-sectional | Ever sex | PB | Perception of proportion of same sex peers that have had sex: “Of the girls/boys that you know, how many do you think have had sex?” Measured lower/higher. | Not included in adjusted model because p > 0.10 for bivariate model | Female | 14–17 | 449 | Not shown (not found to be statistically significant) |
| PB | Age, participant’s gender norms and values. | Male | 14–17 | 329 | aOR = 1.48, 95% CI (1.05–2.03) | ||||
| PB | As above for opposite sex peers. | Not included in adjusted model because p > 0.10 for bivariate model | Female | 14–17 | 449 | Not shown (not found to be statistically significant) | |||
| PB | Age, participant’s gender norms and values. | Male | 14–17 | 329 | aOR = 1.32 95% CI 1.11–1.60 | ||||
| Cherie et al., Ethiopia | Cross-sectional | Ever anal sex | PB | Perception that best friend has had anal sex. | Age, gender, attitude, college aspiration, self-esteem, living with parents, parent’s education. | Both | 15–24 | 3543 | aOR = 9.7, 95% CI 5.4–17.7 |
| Ever oral sex | PB | Perception that best friend has had oral sex. | Both | 15–24 | 3543 | aOR = 5.7, 95% CI 3.6–11.2 | |||
| Balabola et al., Rwanda | Cross-sectional | Sexual abstinence | PB | Perception that most friends are having sex | Age, religion, urban/rural residence, whether live with father, school enrolment, alcohol use, perceived self-efficacy to refuse sex, self-esteem, beliefs about premarital sex, perceived social support for abstinence (nonpeer). | Female | 15–24 | 533 | aOR = 0.30, p < 0.001 |
| PB | Male | 15–24 | 790 | aOR = 0.37, p < 0.001 | |||||
| Kawai et al., Tanzania | Cohort | Transition to first sex | PAN | Favourable social norms about delayed sex, e.g. ’Most friends perceive that one should be older to have sex’0. 6 point scale, more favourable has higher score. Measured at baseline. | Univariate analysis only presented. | Both | 12–14 | 2477 | High (5–6 points) compared to low (1–2 points): OR = 0.84, 95% CI 0.58–1.23 Moderate (3–4 points) to low (1–2 points): OR = 0.74, 96% CI 0.5–1.08 |
| Kakoko, Tanzania | Cross-sectional | Ever sex | PAN | Disagree/agree that will lose some of friends if do not have sexual intercourse. | Age, gender, parental education level. | Both | 12–14 | 2658 | aOR 1.7, 95% CI 1.2–2.3, agree compared to disagree that will lose friends if do not have sex |
| McQuestion et al., Ghana | Cross-sectional | Ever sex | PAN | Permissive attitudes about sex: Three Likert-scaled statements formed the best additive scale for perceived peer attitudes toward sex (perceived peer norms): “Most of my friends believe it is OK to have sex with a steady girlfriend or boyfriend”; “Most of my friends believe it is OK to have sex with more than one partner in one month”; “Most of my friends believe that one should have regular sex to avoid health problems”. | Age, ethnic group, household wealth, father’s occupation, parents married, ever worked for a wage, attends church weekly, reproductive knowledge, home sex communication, adult support, interactions between adults support and knowledge and between knowledge and home sex communication | Female | 17–22 | 1484 | aOR = 0.98, p < 0.05 for unit score increase in peer permissive attitudes to sex scale |
| PAN | Male | 17–22 | 1396 | aOR = 0.99, p < 0.05 for one unit score increase in peer permissive attitudes to sex scale | |||||
| Cross-sectional | Age at first sex in years | PAN | Female | 17–22 | 923 | Increase of 0.014 years on age at first sex for unit increase in permissive peer attitudes towards sex scale, p < 0.05 | |||
| PAN | Male | 17–22 | 600 | Not shown (not found to be statistically significant) | |||||
| Mkandawire et al., Malawi | Time to event | Time to first sex | PC | Number of close friends: 1, 2–5, >5 | Orphan status, knowledge and myths about HIV, food security, has close relatives, sibling residence, school enrolment, household structure. | Female | 12–18 | 641 | aHR 0.99, 95% CI 0.93–1.04 (2–5 close friends compared to 1 close friend); aHR 0.97, 95% CI 0.93–1.02 (>5 close friends compared to 1 close friend) |
| PC | Male | 12–18 | 573 | aHR 1.03, 95% CI 0.94–1.12 (2–5 close friends compared to 1 close friend); aHR 1.06, 95% CI 0.98–1.11 (>5 close friends compared to 1 close friend) | |||||
| Condom use | |||||||||
| Balabola et al., Rwanda | Cross-sectional | Condom use at last sex | PAN | Best friend approves of condom use | Age group, gender, education, religion, urban/rural residence, type of sexual relationship, lives with father, perceived self-efficacy, advocacy and knowledge for condom use, self-esteem, discusses condoms or HIV/AIDS with partner. | Both | 15–24 | 474 | aOR = 1.62, p > 0.1 |
| Harrison et al., South Africa | Cross-sectional | Condom use at last sex | PB | Perception that male peers are using condoms (lower/higher) | Not included in adjusted model because p > 0.10 for bivariate model | Female | 14–17 | 59 | not given |
| PB | Age, participant condom attitudes and perceptions. | Male | 14–17 | 106 | aOR 1.79, 95% CI 1.22–2.59 | ||||
| Risky sex, composite variables | |||||||||
| Brook et al., South Africa | Cross-sectional | Risky sex: ever sex, multiple partners, condom use, sex while drunk/stoned | PB | Peer deviancy (latent variable combining alcohol, drug use, and perceived sexual behaviours) | Structural equation model: age and latent variables for family poverty, parent/child relationship, and vulnerable personality traits. | Both | 12–17 | 633 | Parameter estimate = 0.49, p < 0.001 |
| PB | Female | 12–17 | 368 | Parameter estimate = 0.10, p < 0.001 | |||||
| PB | Male | 12–17 | 265 | Parameter estimate = 0.24, p < 0.001 | |||||
| Wild et al., South Africa | Cross-sectional | Risky Sex: >2 partners in previous 12 months, no contraception, knowing most recent partner <7 days | PC | Peer self-esteem sub-scale (Likert responses to statements such as ‘I am as popular with kids my own age as I want to be’), 6 point scale. | Grade, race, other self-esteem indices (school, family, body, sports, global self-esteem). | Female | Grades 8–11 | 448 | aOR = 0.25 for scoring above the median peer self-esteem score, 95% CI 0.12–0.52, p < 0.001 |
| PC | Male | Grades 8–11 | 333 | aOR = 0.54 for scoring above the median peer self-esteem score, 95% CI = 0.54–2.01 | |||||
| Age difference with first sexual partner | |||||||||
| Lam et al., South Africa | Cross-sectional | Linear regression | PA | As Lam et al. above. | As Lam et al. above. | Female | 14–17 | 348 | Partner was 0.87 years older than participant for each cumulative exposure of 1.0, p = 0.06 |
| PA | Male | 14–17 | 280 | Partner was 0.06 years older than participant for each cumulative exposure of 1.0, p > 0.05 | |||||
Findings by gender include all those reported by the studies, whether stratified by male/female and or combined.
Peer exposure types: PA = peer socio-demographic attributes, PB = peer behaviour, PAN = peer approval norms, PC = peer connectedness.
3.2. Sexual debut
Studies investigating sexual debut used transition to first sex when longitudinally designed (Kabiru et al., 2010; Kawai et al., 2008; Lam et al., 2013), time to first sex in the case of a time-to-event study (Mkandawire et al., 2013) and otherwise ever having had sex (Harrison et al., 2012; Kakoko, 2013; McQuestion et al., 2012) or sexual abstinence (Balabola et al., 2002), and one study investigated ever having had oral sex or anal sex (Cherie and Berhane, 2012).
There was good evidence for an effect of estimated age of classmates, classified as a peer socio-demographic attribute exposure, on transition to first sex among young women in a cohort study in urban South Africa: young women were 13.8% more likely to transition for each additional year or exposure (p < 0.05, Lam et al., 2013). However, there was little evidence for effect seen among young men in the same study. This was the only study examining this peer exposure.
Findings were mixed as to whether perceived peer behaviours were associated with ever having had sex (or conversely, sexual abstinence). One study pooling young men and women found large effects for perceiving that best friends had engaged in oral (adjusted OR = 5.7, 95% CI 3.6–11.2) or anal sex (aOR = 9.7, 95% CI 5.4–17.7) on participant’s corresponding behaviours (Cherie and Berhane, 2012). Another similarly found strong negative associations between sexual abstinence and perceiving most friends to have had sex for both genders (aOR = 0.30 for young women and 0.37 for young men, both p < 0.001, Balabola et al., 2002). A smaller but still statistically strong effect was found in a cohort examining the perception at baseline that a high compared to low proportion of friends were sexually active on transition to first sex (aOR = 1.99 for young men and women together, 95% CI 1.30–3.06), (Kawai et al., 2008). On the other hand, another study found a similar effect only among boys (Harrison et al., 2012), and a second cohort study only among one age/gender/residence subgroup of many examined (Kabiru et al., 2010).
Among studies that examined associations between peer approval norms and ever having had sex, evidence was again inconsistent. One study found an aOR of 0.85, 95% CI 0.58–1.23 for favourable peer norms towards delayed sex on transition to first sex over the study period (Kawai et al., 2008), and another found that participants had 1.7 times the odds of reporting ever having had sex if they thought they would lose friends if they did not have sex compared to those who disagreed with this statement, (Kakoko, 2013; McQuestion et al., 2012). However, another study found a small but statistically significant effect of peer norms on reported ever sex, whereby participants actually had reduced odds (aOR 0.95, p < 0.001) of reporting sex for every additional unit score increase in permissive peer sexual attitudes (McQuestion et al., 2012). In fact, McQuestion et al. was the only study to have found that reported participant sexual behaviour was discordant with perceived peer behaviour or the behaviour favoured by peers, that is, participants engaged in behaviour opposite to what peers approved of.
There was little evidence that peer connectedness, here operationalized as number of close friends (Mkandawire et al., 2013), was associated with ever having had sex, though only one study examine this outcome-peer exposure combination.
3.3. Age of first sexual partner
There was evidence from one study for an association between peer socio-demographic attributes and age of first sexual partner. Among girls, but not boys, there was somewhat weak evidence that each additional year’s estimated exposure to older classmates was associated with 0.87 years increased age of the first reported sexual partner, p = 0.06 (Lam et al., 2013). No other studies were found that investigated this outcome.
3.4. Condom use
Two studies investigated reported condom use as an outcome. One investigated peer approval norms and found little evidence for an effect on condom use at last sex (Balabola et al., 2002), and the other found that perceiving a higher number of male peers to have had sex increased the odds of participant condom use at last sex among boys (aOR 1.79, 95% CI 1.22–2.59) but not among girls (effect measure not given, Harrison et al., 2012).
3.5. Combined sexual behaviour outcomes
There were two studies that examined whether peer exposures were associated with a combined ‘risky’ sexual behaviour variable, composed variously of ever having had sex, sex with multiple partners, sex while drunk/high and length of time sexual partners were known before intercourse. There was strong evidence form a study in urban South Africa that a combined peer behaviour exposure was associated with risky sex in both boys and girls and in a combined gender analysis (Brook et al., 2006). Another study from South Africa found a strong association between risky sex and peer self-esteem, classified as peer connectedness, but only among girls (aOR 0.25 for scoring above the median self-esteem score, 95% CI 0.12–0.52, Wild et al., 2004).
3.6. Summary of findings
Overall, findings as to the evidence for an association between peer exposures and sexual behaviour among young people in sub-Saharan Africa were inconsistent, Table 4. We examined findings to investigate patterns by outcome type, peer exposure type, gender, and age, and did not find clear patterns for the conditions in which peer exposures might be more or less effective.
Table 4.
Summary of evidence for effect by outcome types, exposure types and gender.
| Peer exposure type | Studies | Outcome types |
|||
|---|---|---|---|---|---|
| Sexual debut | Condom use | Combined ‘risky’ sexual behaviour | Age difference with first sexual partner | ||
| Peer socio-demographic attributes | Lam et al. | ♦ f, 0m | ♦ f**, 0m | ||
| Perceived peer behaviours | Kabiru et al. | ♦ f, 0f* 0m | |||
| Kawai et al. | ♦b | ||||
| Harrison et al. | 0f,♦m | ♦ m,0f | |||
| Balabola et al. | ♦ f,♦m | ||||
| Cherie et al. | ♦b | ||||
| Brook et al. | ♦ f, ♦ m, ♦ b | ||||
| Peer approval norms | Kawai et al. | 0b | |||
| Balabola et al. | 0b | ||||
| Kakoko | ♦b | ||||
| McQuestion et al. | ♦ f,♦m | ||||
| Peer connectedness | Wild et al. | ♦ f,0m | |||
| Mkandawire et al. | 0f,0m | ||||
Key
Good statistical evidence for effect (p < 0.05, 95% Cl’s do not cross the null).
Lack of statistical evidence for an effect (p > 0.05, 95% Cl’s cross the null).
Among females.
Among males.
Among both males and females in a pooled analysis.
Significant for just one female sub-group.
Weaker evidence, p = 0.06.
Sexual debut outcomes were the most commonly studied, but their findings were heterogeneous. Within each outcome category, there was mixed evidence as to their associations with a peer exposure. Nor did considering the findings by type of peer exposure illuminate a clear pattern as to whether one type showed greater evidence for influence on sexual behaviour than another. There was more research investigating perceived peer behaviours, but across and within outcomes the findings as to its influence were inconsistent. There were also mixed results for associations between sexual behaviours and peer approval norms and peer connectedness. Only one study examined peer socio-demographic attributes (Lam et al., 2013) and found evidence for effects on transition to first sex among girls but not boys.
By gender, there were again differences across studies and it was not clear that peer exposures were more or less salient for either boys or girls. Nor did there appear to be a pattern by the age of participants.
4. Discussion
Many observational studies have explored the association between peer exposures and adolescent sexual behaviours in sub-Saharan Africa, driven by a range of different theoretical perspectives. Each of the eleven higher quality included studies found evidence for at least one association between a peer exposure and sexual behaviour outcome in at least one combination of outcome, peer exposure type and gender. However, including all findings reported in the studies, there were mixed results. We did not discern patterns by outcome or peer exposure types, nor by gender or age. There was a high level of heterogeneity in the peer exposures examined and the means by which the same constructs were operationalized. It is therefore difficult to draw strong conclusions overall on the association between peer exposures and adolescent sexual behaviour.
4.1. Strengths and limitations of the review
This review is the first collation of the quantitative evidence for peer influences on adolescent sexual behaviour in Sub-Saharan Africa. We have dealt with the heterogeneity of peer influences studied by classifying different types of peer exposures and examining how they have fit into the theoretical frameworks employed by studies.
Our review has not included non-peer reviewed literature or articles published in a language other than English. Using a cut-off for methodological quality could imply that all criterion carry equal weight and some studies may have been misclassified as regards their overall quality.
4.2. Strengths and limitations in the evidence base
In our review, 30 studies were found before exclusions for inconsistencies between text and tables and only 11 retained for higher quality, Fig. 1. Many studies did not focus only on peer exposures but examined a range of factors theorised to influence sexual behaviour. Studies employed different variables and adjustment strategies, which made comparing effects of peer exposures across studies difficult, including strength of effect. Over-adjustment, whereby factors on a causal pathway between a peer exposure and outcome are adjusted for, was a potential problem. If such mediation was present, the effect of the peer exposures would likely have been under-estimated (Victora et al., 1997).
The strongest available evidence came from three cohort studies, which were better able to distinguish possible influence from peers from reverse causality, such as the selection of peers based on an established sexual behaviour. However, their results still were not uniform. One study included many sub-group analyses but found statistical evidence for an association in only one (Kabiru et al., 2010). Attribution of selection effects as influence, whereby friends are chosen on the basis of behaviour, has been found to inflate estimates of peer influence on adolescent sexual behaviour in other populations (Go et al., 2010; Mercken et al., 2012). The other studies, which measure peer exposures and sexual behaviours at the same point in time, would have been prone to this problem.
No studies used a biologically measured outcome of sexual behaviour. Self-reported sexual behaviour is subject to social desirability and recall biases, especially in adolescents (Buve et al., 2001; Cowan et al., 2002). There is evidence from other populations that study participants tend to estimate peer behaviour as being more like their own, which could bias the evidence for associations upwards (Iannotti and Bush, 1992).
While the majority of included studies did include a theoretical framework in which to situate the role of peers, the heterogeneity of findings makes if difficult to comment on the relative validity of frameworks for adolescents in sub-Saharan Africa.
Most studies asked participants to describe peers in general, rather than collecting data about specific individuals. This meant that there was little information about peer socio-demographic characteristics, and made controlling for a shared environment difficult. Information about what neighbourhood a peer resides in or what school they attend allows researchers to control for factors at these levels that could affect the behaviour of both participants and their friends (Ali and Dwyer, 2011). Data about specific relationships can also be used to investigate the evidence for a dose—response relationship by relationships strength (Sieving et al., 2006), one of the classic epidemiological indicators of a causal relationship (Bradford Hill, 1965). Additionally, while a cross-sectional design still presents problems for causal understanding, knowing something about the duration of the relationship versus the initiation of behaviour can help in determining whether influence or selection is most likely.
5. Conclusions
The quantitative evidence for an effect of peer exposures on adolescent sexual behaviour in sub-Saharan Africa is inconclusive. While we found some evidence supporting the role of peers influencing sexual behaviours of adolescents, and peers are reported to be important to romantic and sexual behaviour in qualitative studies (Gevers et al., 2012; Harrison, 2008; MacPhail and Campbell, 2001; Selikow et al., 2009), there are significant gaps in our current understanding. Future research should investigate biological, non-self-reported sexual behaviour outcomes, and we suggest that approaches such as social network analysis, which collects information about specific peers and their inter-relationships, could be a useful way forward.
Acknowledgements
Elizabeth Fearon was supported by a Bloomsbury Colleges/ London International Development Centre PhD studentship.
The London School of Hygiene and Tropical Medicine provided funding for Gold Open Access publishing.
Appendix 1. Literature search terms
(adolescen* OR youth* OR young people OR young person* OR teen* OR young women OR young men).
AND
(sex* OR virgin* OR condom* OR HIV* OR AIDS OR human immunodeficiency virus* OR acquired immune deficiency syndrome OR STI OR STD OR pregnan*).
AND
(peer* OR friend* OR social influence).
AND
(Africa* OR Cape Town OR Johannesburg OR Durban OR Zimbabwe OR Zambia OR Botswana OR Swaziland OR Lesotho OR Mozambique OR Namibia OR Kenya OR Tanzania OR Uganda OR Nigeria OR Ghana OR Malawi OR Angola OR DRC OR Congo* OR Rwanda* OR Burundi* OR Cameroon* OR Gambia* OR Senegal* OR Ethiopia* OR Somalia* OR Gabon* OR Guinea* OR Togo* OR B enin* OR Burkina* OR Liberia* OR Cote* OR ivory coast OR sierra OR Eritrea* OR Mali* OR Chad* OR Sudan* OR Niger* OR Central African Republic OR Madagascar*)
References
- Abebe M, Tsion A, Netsanet F, 2013. Living with parents and risky sexual behaviors among preparatory school students in Jimma zone, South west Ethiopia. Afr. Health Sci. 13, 498–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adedimeji AA, Heard NJ, Odutolu O, Omololu FO, 2008. Social factors, social support and condom use behavior among young urban slum inhabitants in southwest Nigeria. East Afr. J. Public Health 5, 215–222. [DOI] [PubMed] [Google Scholar]
- Ali MM, Dwyer DS, 2011. Estimating peer effects in sexual behavior among adolescents. J. Adolesc 34, 183–190. [DOI] [PubMed] [Google Scholar]
- Alloway R, Bebbington P, 1987. The buffer theory of social support—a review of the literature. Psychol. Med. 17, 91–108. [DOI] [PubMed] [Google Scholar]
- Anglin RE, Samaan Z, Walter SD, McDonald SD, 2013. Vitamin D deficiency and depression in adults: systematic review and meta-analysis. Br. J. Psychiatry 202, 100–107. [DOI] [PubMed] [Google Scholar]
- Balabola S, Awasum D, Quennum-Renaud B, 2002. The correlates of safe sex practice amongst Rwandan youth: a positive deviance approach. Afr. J. AIDS Res. 1,11–21. [DOI] [PubMed] [Google Scholar]
- Barker G, 2007. Adolescents, Social Support and Help-seeking Behaviour: An International Literature Review and Programme Consultation with Recommendations for Action: An International Literature Review and Programme Consultation with Recommendations for Action, WHO Discussion Papers on Adolescence Department of Child and Adolescent Health and Development, World Health Organization. [Google Scholar]
- Berndt TJ, 1979. Developmental changes in conformity to peers and parents. Dev.Psychol. 15, 608–616. [Google Scholar]
- Billy JO, Udry JR, 1985. The influence of male and female best friends on adolescent sexual behavior. Adolescence 20, 21–32. [PubMed] [Google Scholar]
- Bradford Hill A, 1965. The environment and disease: association or causation? Proc. R. Soc. Med. 58, 295–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bramoullé Y, Djebbari H, Fortin B, 2007. Identification of Peer Effects Through Social Networks. University of Laval Working Paper. [Google Scholar]
- Brook DW, Morojele NK, Zhang C, Brook JS, 2006. South African adolescents: pathways to risky sexual behavior. Aids Educ. Prev. 18, 259–272. [DOI] [PubMed] [Google Scholar]
- Buhi ER, Goodson P, 2007. Predictors of adolescent sexual behavior and intention: a theory-guided systematic review. J. Adolesc. Health 40, 4–21. [DOI] [PubMed] [Google Scholar]
- Buve A, Lagarde E, Carael M, Rutenberg N, Ferry B, Glynn JR, et al. , 2001. Interpreting sexual behaviour data: validity issues in the multicentre study on factors determining the differential spread of HIV in four African cities. AIDS 15 (Suppl. 4), S117–S126. [DOI] [PubMed] [Google Scholar]
- Cherie A, Berhane Y, 2012. Oral and anal sex practices among high school youth in Addis Ababa, Ethiopia. BMC Public Health 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cialdini RB, Reno RR, 1990. A focus theory of normative conduct: recycling the concept of norms to reduce littering in public places. J. Personal. Soc. Psychol. 58, 1015–1026. [Google Scholar]
- Cowan FM, Langhaug LF, Mashungupa GP, Nyamurera T, Hargrove J, Jaffar S, et al. , 2002. School based HIV prevention in Zimbabwe: feasibility and acceptability of evaluation trials using biological outcomes. AIDS 16, 1673–1678. [DOI] [PubMed] [Google Scholar]
- Ellen JM, Dolcini M, Bir ND, Harper GW, Watson S, Valente T, 2001. Social network centrality and sexual experience among a household sample of urban African American adolescents. Connections 24, 76–8. [Google Scholar]
- Gevers A, Jewkes R, Mathews C, Flisher A, 2012. ‘I think it’s about experiencing, like, life’: a qualitative exploration of contemporary adolescent intimate relationships in South Africa. Cult. Health Sex. 14, 1125–1137. [DOI] [PubMed] [Google Scholar]
- Go MH, Green HD Jr., Kennedy DP, Pollard M, Tucker JS, 2010. Peer influence and selection effects on adolescent smoking. Drug Alcohol Depend. 109, 239–242. [DOI] [PubMed] [Google Scholar]
- Gregson S, Nyamukapa CA, Garnett GP, Mason PR, Zhuwau T, Carael M, et al. , 2002. Sexual mixing patterns and sex-differentials in teenage exposure to HIV infection in rural Zimbabwe. Lancet 359, 1896–1903. [DOI] [PubMed] [Google Scholar]
- Harrison A, 2008. Hidden love: sexual ideologies and relationship ideals among rural South African adolescents in the context of HIV/AIDS. Cult. Health Sex. 10, 175–189. [DOI] [PubMed] [Google Scholar]
- Harrison A, Smit J, Hoffman S, Nzama T, Leu C-S, Mantell J, et al. , 2012. Gender, peer and partner influences on adolescent HIV risk in rural South Africa. Sex. Health 9, 178–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iannotti RJ, Bush PJ, 1992. Perceived vs actual friends use of alcohol, cigarettes, marijuana, and cocaine — which has the most influence. J. Youth Adolesc. 21, 375–389. [DOI] [PubMed] [Google Scholar]
- Kabiru CW, Beguy D, Undie C-C, Zulu EM, Ezeh AC, 2010. Transition into first sex among adolescents in slum and non-slum communities in Nairobi, Kenya. J. Youth Stud. 13, 453–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kakoko DC, 2013. Reported heterosexual intercourse and related behaviours among primary school pupils in Kinondoni district, Dar es Salaam, Tanzania. Cult. Health Sex. 15, 235–245. [DOI] [PubMed] [Google Scholar]
- Kawai K, Kaaya SF, Kajula L, Mbwambo J, Kilonzo GP, Fawzi WW, 2008. Parents’ and teachers’ communication about HIV and sex in relation to the timing of sexual initiation among young adolescents in Tanzania. Scand. J. Public Health 36, 879–888. [DOI] [PubMed] [Google Scholar]
- Kelly RJ, Gray RH, Sewankambo NK, Serwadda D, Wabwire-Mangen F, Lutalo T, et al. , 2003. Age differences in sexual partners and risk of HIV-1 infection in rural Uganda. J. Acquir. Immune Defic. Syndr. 32, 446–451. [DOI] [PubMed] [Google Scholar]
- Lam D, Marteleto LJ, Ranchhod V, 2013. The influence of older classmates on adolescent sexual behavior in Cape Town, South Africa. Stud. Fam. Plan. 44, 147–167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacPhail C, Campbell C, 2001. ‘I think condoms are good but, aai, I hate those things’: condom use among adolescents and young people in a Southern African township. Soc. Sci. Med. 52, 1613–1627. [DOI] [PubMed] [Google Scholar]
- Manski CF, 1993. Identification of endogenous social effects: the reflection problem. Rev. Econ. Stud. 60, 531–542. [Google Scholar]
- Markham CM, Lormand D, Gloppen KM, Peskin MF, Flores B, Low B, et al. , 2010. Connectedness as a predictor of sexual and reproductive health outcomes for youth. J. Adolesc. Health 46, S23–S4. [DOI] [PubMed] [Google Scholar]
- Maticka-Tyndale E, Barnett JP, 2010. Peer-led interventions to reduce HIV risk of youth: a review. Eval. Progr. Plan. 33, 98–112. [DOI] [PubMed] [Google Scholar]
- McQuestion M, Ahiadeke C, Posner J, Williams T, 2012. Psychosocial processes and sexual initiation among Ghanaian youth. Health Educ. Behav. 39, 268–275. [DOI] [PubMed] [Google Scholar]
- Medley A, Kennedy C, O’Reilly K, Sweat M, 2009. Effectiveness of peer education interventions for HIV prevention in developing countries: a systematic review and meta-analysis. AIDS Educ. Prev. 21, 181–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mercken L, Steglich C, Sinclair P, Holliday J, Moore L, 2012. A longitudinal social network analysis of peer influence, peer selection, and smoking behavior among adolescents in British schools. Health Psychol. 31, 450–459. [DOI] [PubMed] [Google Scholar]
- Mkandawire P, Tenkorang E, Luginaah IN, 2013. Orphan status and time to first sex among adolescents in Northern Malawi. AIDS Behav 17, 939–950. [DOI] [PubMed] [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, Altman DG, 2009. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J. Clin. Epidemiol. 62, 1006–1012. [DOI] [PubMed] [Google Scholar]
- Moody J, 2009. Network Structure and Diffusion. Duke Population Research Institute Online Working Papers Series. [Google Scholar]
- Negeri EL, 2014. Assessment of risky sexual behaviors and risk perception among youths in Western Ethiopia: the influences of family and peers: a comparative cross-sectional study. BMC Public Health 14, 301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peltzer K, 2010. Early sexual debut and associated factors among in-school adolescents in eight African countries. Acta Paediatr. 99, 1242–1247. [DOI] [PubMed] [Google Scholar]
- Pettifor AE, Rees HV, Kleinschmidt I, Steffenson AE, MacPhail C, Hlongwa-Madikizela L, et al. , 2005. Young people’s sexual health in South Africa: HIV prevalence and sexual behaviors from a nationally representative household survey. AIDS 19, 1525–1534. [DOI] [PubMed] [Google Scholar]
- Prinstein MJ, Meade CS, Cohen GL, 2003. Adolescent oral sex, peer popularity, and perceptions of best friends’ sexual behavior. J. Pediatr. Psychol. 28, 243–249. [DOI] [PubMed] [Google Scholar]
- Rudatsikira E, Ogwell AEO, Siziya S, Muula AS, 2007. Prevalence of sexual intercourse among school-going adolescents in Coast Province, Kenya. Tanzan. Health Res. Bull. 9, 159–163. [DOI] [PubMed] [Google Scholar]
- Selikow T-A, Ahmed N, Flisher AJ, Mathews C, Mukoma W, 2009. I am not “umqwayito”: a qualitative study of peer pressure and sexual risk behaviour among young adolescents in Cape Town, South Africa. Scand. J. Public Health 37, 107–112. [DOI] [PubMed] [Google Scholar]
- Sieving RE, Eisenberg ME, Pettingell S, Skay C, 2006. Friends’ influence on adolescents’ first sexual intercourse. Perspect. Sex. Reprod. Health 38, 13–19. [DOI] [PubMed] [Google Scholar]
- Siziya S, Muula AS, Kazembe LN, Rudatsikira E, 2008. Harmful lifestyles’ clustering among sexually active in-school adolescents in Zambia. BMC Pediatr. 8, 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L, Monahan KC, 2007. Age differences in resistance to peer influence. Dev. Psychol. 43, 1531–1543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stöckl H, Kalra N, Jacobi J, Watts C, 2013. Is early sexual debut a risk factor for HIV infection among women in sub-Saharan Africa? A systematic review. Am. J. Reprod. Immunol 69 (Suppl. 1), 27–40. [DOI] [PubMed] [Google Scholar]
- UNAIDS, 2014. The Gap Report. UNAIDS, Geneva. [Google Scholar]
- Valente TW, 1995. Network Models of the Diffusion of Innovations. Hampton Press. [Google Scholar]
- Victora CG, Huttly SR, Fuchs SC, Olinto MT, 1997. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. Int. J. Epidemiol. 26, 224–227. [DOI] [PubMed] [Google Scholar]
- Wand H, Ramjee G, 2012. The relationship between age of coital debut and HIV seroprevalence among women in Durban, South Africa: a cohort study. BMJ Open 2, e000285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle—Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses, Available from http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp [accessed 14.10.15.].
- Wild LG, Flisher AJ, Bhana A, Lombard C, 2004. Associations among adolescent risk behaviours and self-esteem in six domains. J. Child Psychol. Psychiatry 45, 1454–1467. [DOI] [PubMed] [Google Scholar]