

Abstract
INTRODUCTION:
Food handlers with poor personal hygiene and lack of awareness in preventing foodborne diseases working in hospitality sectors or hospitals could spread foodborne infections.
OBJECTIVE:
Our study objective was to ascertain the impact of a video-based educational intervention program and administrative measures on improvement in personal hygiene of food handlers in hospital.
METHODOLOGY:
We conducted this pilot study among all 103 food handlers who were working in a tertiary care hospital. A checklist-based scoring and physical examination were conducted by the investigator for the food handlers. After baseline scoring S1, intervention 1 and 2 was implemented, and score was obtained as S2 and S3, respectively. Descriptive statistics was calculated, and score was compared by repeated measures ANOVA test using SPSS-22 software.
RESULTS:
Our study revealed that a total of 19.2% of food handlers had health complaints. More than half (54.8%) admitted that they had suffered from any kind of illness since last 6 months. Common illness was viral fever (40.3%) followed by typhoid (5.7%), dengue (4.8%) and urinary tract infection (3.8%). Most of the food handlers had long hair (62.5%) followed by long nail (57.69%). Nearly, one-fifth (20.1%) of food handlers nail was infected with fungus. Worm was found in 14.4% cases by stool examination. Statistically significant (P < 0.05) improvement in score was observed after each intervention.
DISCUSSION:
Poor hygiene (Score-1 = 23.76) was observed at baseline study although there was a mechanism in place for a yearly health checkup and regular (6 monthly) hygiene training. After interventions (video-based training and administrative measures), the score was improved to Score-3 (42.57). Statistically significant (P < 0.05) differences in hygiene score were observed for variables such as state of residence, education level, and working experiences (inside or outside the hospital).
CONCLUSION:
It is possible to improve personal hygiene among food handlers using video-based interactive training methods and administrative measures with no extra or minimal cost.
RECOMMENDATIONS:
This “piggyback” approach of training can be imparted in addition to routine training measures among the food handlers for improving their personal hygiene in the hospital setting.
Keywords: Food handlers, food hygiene, hospital kitchen, personal hygiene, skill development
Introduction
Food is an important basic necessity for sustenance of life, and food safety is a scientific discipline describing handling, preparation, and storage of food in ways that prevent foodborne infections.[1] Food handler is defined as a person in food trade or someone professionally associated with it, such as an inspector, who in his/her routine work comes into direct contact with food in the course of production, processing, packaging, or distribution; its procurement, preparation, and consumption are vital.[2]
The term “food safety” is increasingly being used in place of food hygiene and encompasses a whole range of issues that must be addressed for ensuring safety of the prepared food.[3] Accordingly, food handlers with poor personal hygiene and lack of awareness of important issues in preventing foodborne diseases, working in food establishments could be potential sources of infections of many intestinal helminths of protozoa and enterogenic pathogens. More than 250 foodborne diseases are caused by either bacteria (Clostridium, Botulinum, Escherichia coli, Salmonella, Listeria, Vibrio cholerae); viruses (Enterovirus, hepatitis A, Rotavirus, Norovirus); or parasites (Entamoeba histolytica, Cryptosporidiosis, Giardia, Trichinosis).[4,5,6,7] The various foodborne diseases are botulism, campylobacteriosis, hepatitis A, Norovirus infection, salmonellosis, shigellosis, diarrhea, typhoid, food poisoning, amoebiasis, ascariasis, hook worm infections, etc.[6] Therefore, a good working environment and periodic training should be provided by upper management to food handlers.[8]
The World Health Organization (WHO) estimated that in developed countries, up to 30% of the population suffer from foodborne diseases each year, whereas in developing countries, up to 2 million deaths are estimated per year. Moreover, in developing countries, up to an estimated 70% of cases of diarrheal diseases are associated with the consumption of contaminated food. WHO estimated 16 million new cases and 600,000 deaths of typhoid fever each year.[9]
The Food Safety and Standards Authority of India (FSSAI) has been established under Food Safety and Standards Act, 2006 which consolidates various acts and orders that have hitherto handled food-related issues in various ministries and departments. FSSAI has been created for laying down science-based standards for articles of food and to regulate their manufacture, storage, distribution, sale, and import to ensure availability of safe and wholesome food for human consumption.[10]
Modern context of food safety is described by the “Farm to Fork” model.[11] This covers in all areas of food handling right from harvesting, storage, transport, distribution, and lastly in kitchen. There are several stakeholders who are involved to make food safe, precisely from raw to finally prepared food to be consumed, i.e., from “Farm to Fork”/”Farm to Plate.”[12] Among them, food handlers play a major role both in hospitality and hospital sector. Any lacunae in the personal hygiene of food handlers in any sector can be detrimental to the health of people who consume the prepared food. Further, it becomes a major concern when food handling is related to patient care, and it is in this setting when we require healthy workers.[7]
When skills of food handlers are compromised (improper hand washing, dressing, cutting, cooking, etc.), along with other factors, it poses significant risk of the development of foodborne infections in hospital settings and increases the risk of food poisoning.[11,13,14] In a hospital setting, nosocomial infection is a common problem that increases the average length of hospital stay and hospital cost and often affects patients’ quality of life, survival, and response to treatment.[13]
As a hospital administrator, it is our moral duty to prevent nosocomial infections and the maintenance of a high degree of hygiene in hospital settings. For this reason, improvement in personal hygiene among food handlers is very important.
Poor hygiene of food handlers in hospital kitchens has been reported to be the cause of outbreaks of infections in hospitals, some of them resulting in death of patients. Almost all of cases (88%) and deaths in outbreaks of listeriosis in Canada were people from the hospital or older people who were living in a long-term care home, because deli meats contaminated with listeria were distributed to hospitals. Listeria was found in niches deep inside two slicing machines. The most common reasons of foodborne infection in hospitals are improper holding time or temperature, contaminated equipment, poor personal hygiene, and food from unsafe sources.[14]
To the best of our knowledge, most of the studies conducted in the past to assess the knowledge, attitude, and practice among the food handlers about their food hygiene are cross-sectional, which had a very little scope of behavior change for the food handlers. As an example, Adane et al. (2014) conducted a cross-sectional study in Ethiopia to know the food hygiene and safety measures among food handlers. The study revealed that almost three-quarter (72%; 84/116) of food handlers in food establishments had a good level of food hygiene and safety practices compared to nearly half (53%; 10/19) of street food vendors.[15]
Akabanda et al. (2014–2015) conducted a cross-sectional study to evaluate the food safety knowledge, attitudes, and practices among institutional food handlers in Ghana. That study revealed that almost all of the food handlers were aware of the critical role of general sanitary practices in the work place, such as hand washing (98.7% correct answers), using gloves (77.9%), proper cleaning of the instruments/utensils (86.4%), and detergent use (72.8%). On disease transmission, the results indicate that 76.2% of the food handlers did not know that Salmonella is a foodborne pathogens and 70.6% did not know that hepatitis A is a foodborne pathogen.[16]
Rationale
The Department of Dietetics and Nutrition has a vital role to play in the overall improvement of health status of patients in any hospital. However, a very little focus has been given on the research and development in this aspect. Still more scarce is the administrative operational research studies on this subject. So far, food handlers have been the focus of research in this area in public health mainly for observational study. Very few interventional studies have been conducted. With this background, we intended to do this operational research for overall improvement in personal hygiene of food handlers working in the tertiary care hospital. This study was quite topical since it has been more than 5 years after Food Safety and Standards Authority of India 2011(FSSR 2011) was promulgated and 1 year after WHO day's theme on food safety (2015) was declared.[12]
This study aimed to test the efficacy of an educational intervention packages to improve the personal hygiene practices in Department of Dietetics and Nutrition, in a tertiary care hospital. Our objective was to ascertain the impact of a video-based educational intervention program and administrative measures on improvement in personal hygiene of food handlers in that hospital.
Methodology
It was a single group before after intervention (pilot) study. The study period was 1 year divided into 3 phases – I, II, and III. The study was conducted in Dietetics Department of a tertiary care hospital. For administrative purpose, we kept a sample size of 103 (all the food handlers working in that hospital were included).
The baseline assessment of personal hygiene of food handlers was done by a checklist-based food handlers’ evaluation pro forma (observation-1). Physical examination and observation of food handlers were done by the investigator. Initial scoring was done for grading personal hygiene of food handlers. After that, intervention-1 was implemented. Same process was repeated till observation-3. Based on the data collected, an intervention package was devised. Various strategies were evolved to encourage and motivate the food handlers for improving their personal hygiene. This package included the following:
Video-based interactive training. It was given to the food handlers in separate batches by the investigator in the dietetics department
A booklet was designed to educate food handlers for improvement in their hygiene practices while working in the hospital kitchen
Continuous supply of logistics (soap, nail cutter, and tray) required for maintaining personal hygiene of food handlers was ensured
Do's and Don’ts were displayed in the hospital kitchen
“Zero Tolerance” was promoted among the food handlers regarding unacceptable personal hygiene practices, for example, long hair, long nail, and dirty hairs. It was displayed on the notice board of kitchen.
“Piggyback” training
The above-mentioned strategies were implemented for 1 month. After that, observation-2 was made and intervention-2 was implemented for 2 months followed by end line observation (observation-3).
After the training, adherence of food handlers to the advice given was checked by the chief dietician in the presence of the investigator.
Maximum possible hygiene score was 46. We considered a score of <24 as poor, 25–35 as average, and >35 as good. Impact of the intervention was assessed by analyzing the score differences through repeated measures ANOVA test using Statistical Package for the Social Sciences version 22, Chicago, USA (SPSS-22 software). Descriptive statistics (mean, median, mode, and standard deviation) was also calculated. Clearance was taken from Institute Ethical Committee. An informed written consent was taken from each participant.
Results
Demographic details are given in Table 1. Our results showed that all (n = 103) the participants were male with mean age 45.23 ± 1.53 years. Most of them were kitchen helper (82.69%), followed by head cook (11.53%) and waiter (5.76%). During the baseline survey, we found that all (100%) food handlers were trained for food handling, they had undergone yearly health checkups, and they were provided uniforms for cooking. Most (76.9%) of them had staff clinic card. The mean years of cooking experience in hospital kitchen was 4.3 ± 1.2 years and outside the hospital was 4.9 ± 1.3 years [Table 2].
Table 1.
Demography of the study subjects
| Demography | n(%) |
|---|---|
| Age (years), mean | 45.23±SD1.53 |
| Sex (male), n (%) | 103 (100) |
| Designation (%) | |
| Head cook | 12 (11.53) |
| Waiter | 6 (5.76) |
| Bearer | 85 (82.69) |
| State wise workers (%) | |
| Uttarakhand | 50 (46.15) |
| Himachal Pradesh | 20 (20.19) |
| Jammu and Kashmir | 13 (12.5) |
| Punjab | 8 (7.69) |
| Haryana | 8 (7.69) |
| West Bengal | 4 (3.8) |
| Education (%) | |
| <5th class | 27 (25.96) |
| 8th class | 27 (25.96) |
| 10th class | 20 (19.2) |
| 12th class | 27 (25.96) |
| Graduate | 2 (1.9) |
Table 2.
Details of administrative measures
| Administrative measures | n(%) |
|---|---|
| Training (%) | 103 (100) |
| Cloth supply (%) | 103 (100) |
| Medical checkup (%) | 103 (100) |
| Cooking experience in Hospital (years), mean | 4.3±SD1.2 |
| Cooking experience outside Hospital | 4.9±SD1.3 |
PGI=Post Graduate Institute
Regarding health and hygiene, it was found that 19.2% of food handlers had health complaints. The most common was low back pain (10.57%) followed by short sightedness (5.76%) and hypertension (2.8%). More than 50% of them were smokers. No other addiction was reported. No hepatitis A virus, hepatitis C virus, and hepatitis B virus positive was documented among them, as per the reports available. Most participants (>85%) were exposed to animals in their home surroundings.
Among all food handlers, 54.8% admitted that they had suffered of any kind of illness. Most common was viral fever 40.3% followed by typhoid 5.7%, dengue 4.8%, and urinary tract infection (UTI) 3.8%.
Most of the food handlers had long hair (62.5%) followed by long nails (57.69%). Some (4.8%) of them had long beard. Nearly one-fifth (20.1%) of food handlers’ nail was infected with fungus. Worm was found in 14.4% cases by stool examination during the baseline survey [Table 3].
Table 3.
Health and hygiene-related components
| Health and hygiene components | n(%) |
|---|---|
| Present health complaint (%) | 20 (19.2) |
| Low back pain | 11 (10.57) |
| Short sightedness | 6 (5.76) |
| HTN | 3 (2.8) |
| Past complaint - suffered of any kind of illness (%) | 56 (54.8) |
| Viral fever (%) | 42 (40.3) |
| Dengue (%) | 5 (4.8) |
| Typhoid (%) | 6 (5.7) |
| UTI (%) | 4 (3.8) |
| Long hair (%) | 64 (62.5) |
| Long beard (%) | 5 (4.8) |
| Long nails (%) | 60 (57.69) |
| Dirty + long nail (%) | 21 (20.1) |
| Fungal infection (%) | 1 (0.96) |
| Permanent/having staff clinic card (%) | 80 (76.9) |
| Worm found in stool (%) | 15 (14.4) |
HTN=Hypertension, UTI=Urinary tract infection
The mean of the baseline score was 23.76 ± 1.71 (Score-1). After the intervention-1, the mean hygiene score was increased to 34.04 ± 2.01 (Score-2) and after the intervention-2, the mean score was increased to 42.57 ± 1.80 (Score-3) out of total score of 46 [Table 4].
Table 4.
Comparison of hygiene scores with regard to different variables
| Variables | Mean | Significance value | ||
|---|---|---|---|---|
| Hygiene Score-1 | Hygiene Score-2 | Hygiene Score-3 | ||
| State | ||||
| Uttarakhand | 24.36 | 33.16 | 42.32 | 0.000 |
| Himachal Pradesh | 23.35 | 35.45 | 42.80 | |
| Jammu and Kashmir | 22.71 | 33.00 | 45.00 | |
| Punjab | 22.77 | 35.08 | 43.00 | |
| Haryana | 24.17 | 34.17 | 41.00 | |
| West Bengal | 23.29 | 35.43 | 41.86 | |
| Education | ||||
| <5th class | 24.23 | 33.05 | 42.14 | 0.000 |
| 8th class | 23.33 | 31.67 | 44.17 | |
| 10th class | 24.22 | 34.11 | 42.07 | |
| 12th class | 23.45 | 34.50 | 43.45 | |
| Graduate | 23.29 | 34.96 | 42.43 | |
| Coking experience in hospital (years) | ||||
| ≤10 | 24.40 | 32.57 | 42.46 | 0.000 |
| ≤20 | 23.82 | 35.06 | 42.45 | |
| >20 | 23.09 | 34.57 | 42.80 | |
| Previous cooking year experience outside | ||||
| No experience | 24.39 | 32.53 | 42.42 | 0.000 |
| 1-10 | 23.47 | 34.98 | 42.93 | |
| >10 | 23.27 | 34.86 | 42.14 | |
| Designation | ||||
| Kitchen helper | 24.21 | 32.21 | 41.50 | 0.017 |
| Cook | 24.00 | 34.00 | 42.67 | |
| Waiter | 23.67 | 34.36 | 42.75 | |
It was noticed from our results that hygiene score was dependent on factors such as state, age, experience in cooking, designation, and others. Details are provided in [Table 5].
Table 5.
Comparison of hygiene scores with regard to different variables
| Variables | Observation Hygiene (mean) | Significance | ||
|---|---|---|---|---|
| Observation 1 | Observation 2 | Observation 3 | ||
| Typhoid | ||||
| No | 24.10 | 31.57 | 36.56 | 0.016 |
| Yes | 23.63 | 34.23 | 42.57 | |
| Complaints | ||||
| Yes | 24.15 | 32.75 | 45.00 | 0.519 |
| No | 23.67 | 34.36 | 42.55 | |
| Past history of illness | ||||
| Yes | 24.11 | 36.00 | 42.80 | 0.262 |
| No | 23.36 | 33.91 | 42.56 | |
| Tetanus toxoid | ||||
| Don’t know | 24.12 | 34.11 | 41.45 | 0.066 |
| Yes | 23.86 | 34.02 | 42.57 | |
| No | 23.26 | 35.50 | 41.34 | |
| Clean hands | ||||
| Dirty | 24.29 | 32.25 | 36.34 | 0.223 |
| Clean | 23.73 | 34.12 | 42.57 | |
| Trimmed hair | ||||
| Yes | 24.09 | 35.43 | 39.00 | 0.235 |
| No | 23.12 | 33.53 | 42.64 | |
| Trimmed nails | ||||
| Long nails | 24.08 | 35.50 | 43.00 | 0.000 |
| Dirty long nails | 24.43 | 37.00 | 41.25 | |
| Fungal infection on nails | 23.09 | 34.81 | 41.75 | |
| Normal trimmed nails | . | 33.33 | 42.60 | |
| Having staff clinic card | ||||
| Present | 23.95 | 33.97 | 42.62 | 0.445 |
| Absent | 23.23 | 35.60 | 40.00 | |
| Systemic examination | ||||
| Normal | 23.80 | 34.02 | 42.62 | 0.490 |
| Abnormal | 23.57 | 35.00 | 40.00 | |
| Stool test | ||||
| Worm not found | 23.80 | 33.95 | 42.62 | 0.768 |
| Worm found | 23.57 | 35.43 | 40.00 | |
Our study found that state of residence, age, experiences in working inside or outside the hospital kitchen, designation, and long nails had played a significant role in hygiene score [Table 4].
It was also observed that after each intervention, hygiene score was improved. Decrease in health complaints, decrease in worm infestations among food handlers, increased coverage of vaccination like tetanus toxoid (TT), and typhoid were important findings after each observation. Hand hygiene was also gradually improved. There was gradual reduction in the numbers of food handlers who were sick, who had long nails, and who had long hairs. The number of staff clinic card holders also increased, i.e., accessibility of health checkup in that hospital was increased [Figures 1–5].
Figure 1.
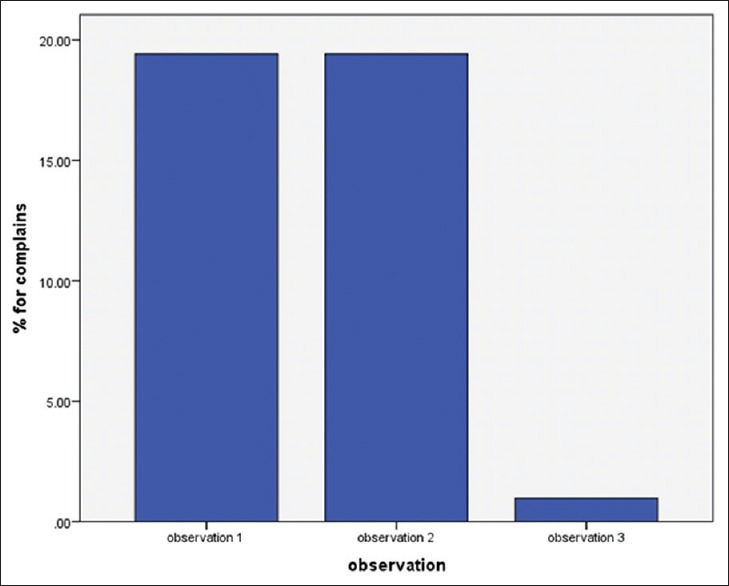
Decrease in health complaints after each intervention
Figure 5.
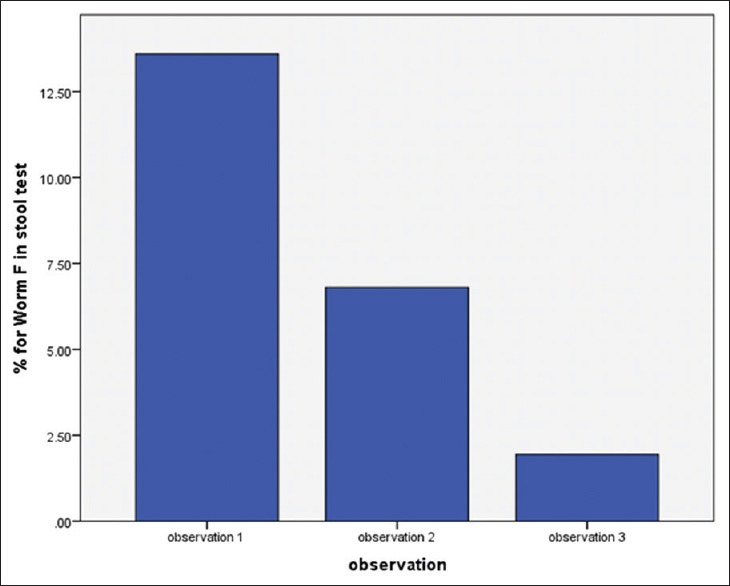
Decrease in worm load in stools after each intervention
Figure 2.
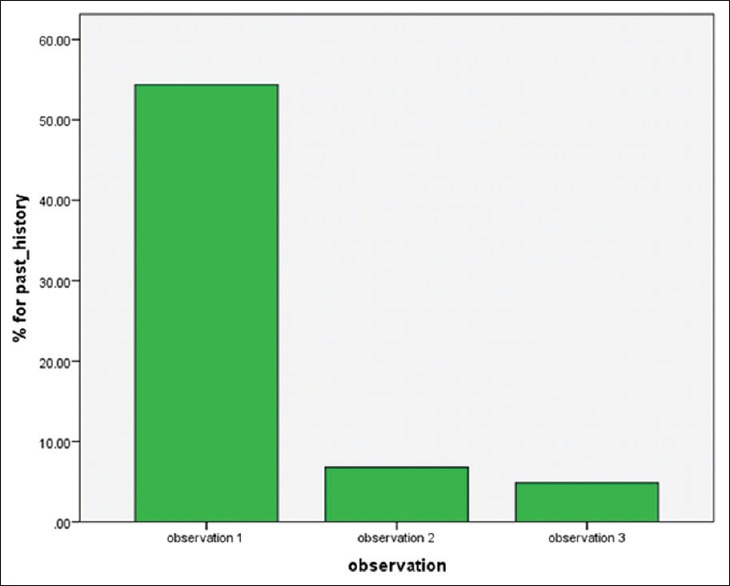
Decrease in past history of illness after each intervention
Figure 3.
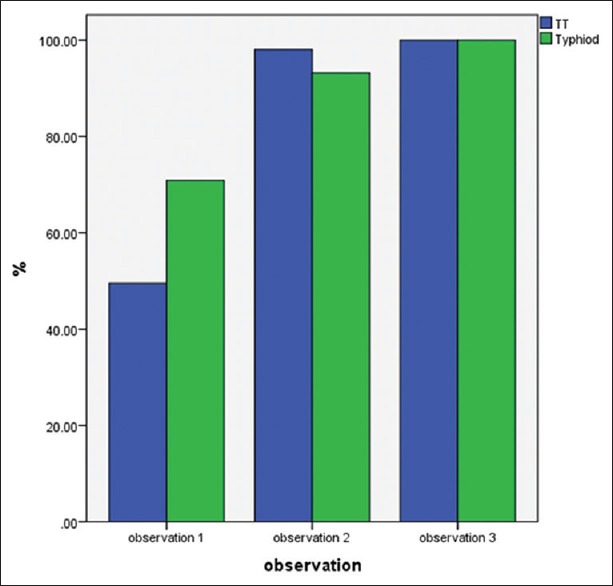
Increase in tetanus toxoid and typhoid vaccination coverage after each intervention
Figure 4.
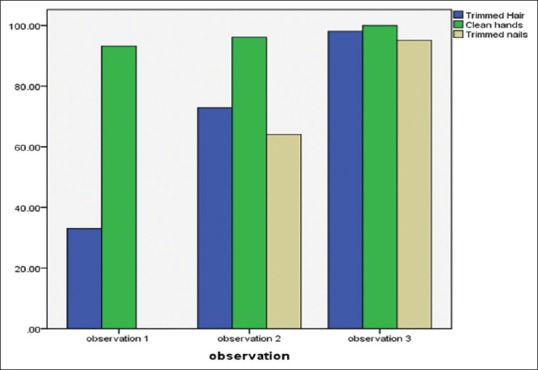
Gradual improvement in hand and hair hygiene after each intervention
Discussion
Poor and faulty food handling practices have been identified as the leading cause of the majority of foodborne diseases. Our baseline study identified some poor hygiene practices among food handlers exhibited at work place. These include keeping long dirty nails, fungi-infected nails, long beards, and worm in the stools. An opposite finding was observed in a cross-sectional study conducted by Adane et al. It was found that almost three-quarter (72%; 84/116) of food handlers in food establishments had a good level of food hygiene and safety practices.[15]
In our study, we found that our food handlers had health problems such as low back pain, short sightedness, and uncontrolled hypertension. Most of them had suffered from viral fever in the last month, followed by typhoid, dengue, and UTI. These health-related ailments (infectious) may be directly or indirectly related with their poor hygiene.
Although, health checkup and hygiene training for the food handlers has been conducted regularly (6 monthly) to improve their personal hygiene. According to the food handlers, there was no shortage of uniform or supplies in logistics. In spite of that, our baseline data were found unsatisfactory. Their cooking practices are not up to the mark, and their mean hygiene score was poor (Score-1 = 23.76).
As a part of our intervention, video-based interactive training, booklet distribution, ensuring continuous supply of logistics (soap, nail cutter, tray), displaying Do's and Don’ts in the whiteboard and practising “Zero Level Tolerance, and checklist-based scoring was done.
Significant improvement was observed after intervention-1. At that point of time, the Score-2 was 34.04. Same interventions were repeated and Score-3 (42.57) was obtained, which was quite high. The score difference (Score1-Score2, Score2-Score3, and Score3-Score1) came statistically significant (P < 0.05) by using repeated measures ANOVA test.
Statistically significant (P < 0.05) differences in hygiene score were observed for some variables such as state of residence, education level, and working experiences (inside or outside the hospital). Similar findings were observed in a cross-sectional study conducted by Akabanda et al.[16]
It was observed that the higher the education level and more the working experiences, the more they were practicing good hygiene in the kitchen. Similar finding was observed in a cross-sectional study conducted by Thakur et al. where it was observed that basic education plays a definite role in the hygiene level of food handlers.[17]
It was quite relevant to note here that food handlers came from different state had different cultural practices regarding hygiene. The difference in level of education was also responsible for variation in their hygiene status. It is expected that with increase in awareness level regarding health hygiene, more people will practice good hygiene. Our study also revealed that previous work experiences of the food handlers had played a important role in their current hygiene practices, as food handlers become more experienced, they used to learn more about improved hygiene practices. Similar finding (more experienced food handlers maintained better hygiene than others) was observed in a cross-sectional study conducted by Akabanda et al.[16]
After administrative interventions, it was also observed that the health complaints were decreased among the food handlers. The coverage of TT and hepatitis-B vaccination was increased. Coverage under the staff clinic was also improved. An increase in hygiene score was observed. There was a reduction in the number of participants who had long hair, long beard, dirty hands, and positive stool test for hookworm [Figures 1–5].
As we mentioned previously that annual health checkup and bi annual training were in place, still, their hygiene score was poor. This can be explained by the reinforcement theory of Skinner.[18] Our study also emphasizes the importance of reinforcement of learned positive behavior for the improvement of health and hygiene.
Significant improvement in overall score was observed in our study; this was may be due to the inclusion of innovative training techniques we have used, coupled by administrative measures. Most of the studies conducted previously among food handlers were cross-sectional studies which had no scope for changing behavior. Our intervention study showed favorable response to the training of food handlers.[19]
Conclusion
Our interventional study demonstrated that with using existing inputs if we improve our process (innovative training and administrative measures), our output (improvement in hygiene) will improve with no extra or minimal cost. This is the hallmark of our study.
Recommendations
It is evident from our study that “piggyback training approach” (i.e., video-based interactive training coupled with administrative measures) can cause drastic improvement in the hygiene of the food handlers; this approach should be percolated down in every kitchen of the health care setup. We also recommend that the frequency of health checkups, supportive supervision, and training should be increased so that food handlers can maintain optimal health not only in workplace but also in the society.
Limitations of our study
We cannot ignore the role of Hawthorne effect in our study. Our sample size was only 103; the study would have better with larger sample size.
Financial support and sponsorship
This study was financially supported by IAPSM-Ford Foundation.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We do acknowledge Mr Manish Goyel, Research Scholar, Punjab University, India, for his valuable statistical inputs. We also acknowledge the food handlers who supported us during the study.
References
- 1.Home. [Last accessed on 2018 Dec 19]. Available from: https://www.fssai.gov.in/home .
- 2.Zain MM, Naing NN. Sociodemographic characteristics of food handlers and their knowledge, attitude and practice towards food sanitation: A preliminary report. Southeast Asian J Trop Med Public Health. 2002;33:410–7. [PubMed] [Google Scholar]
- 3.World Health Organization. Food Safety: What you should Know. SEARO. [Last accessed on 2018 Dec 19]. Available from: http://www.searo.who.int/world_health_day/2015/whd-what-you-should-know/en/
- 4.Annor GA, Baiden EA. Evaluation of food hygiene knowledge attitudes and practices of food handlers in food businesses in Accra, Ghana. Food Nutr Sci. 2011;2:830–6. [Google Scholar]
- 5.Djéni TN, Kouamé AK, Traoré Y, Nevry RK, Dje MK. Assessment of knowledge, attitudes and practices of food handlers in Attieke production units in relation to food hygiene and safety in Côte d’Ivoire in 2012. Food Nutr Sci. 2014;5:896–904. [Google Scholar]
- 6.Iwu AC, Uwakwe KA, Duru CB, Diwe KC, Chineke HN, Merenu IA, et al. Knowledge, attitude and practices of food hygiene among food vendors in Owerri, Imo state, Nigeria. Occup Dis Environ Med. 2017;5:11–25. [Google Scholar]
- 7.Sharif L, Obaidat MM, Al-Dalalah MR. Food hygiene knowledge, attitudes and practices of the food handlers in the military hospitals. Food Nutr Sci. 2013;4:245–51. [Google Scholar]
- 8.Vaz ML, Novo NF, Sigulem DM, Morais TB. A training course on food hygiene for butchers: Measuring its effectiveness through microbiological analysis and the use of an inspection checklist. J Food Prot. 2005;68:2439–42. doi: 10.4315/0362-028x-68.11.2439. [DOI] [PubMed] [Google Scholar]
- 9.WHO's First Ever Global Estimates of Foodborne Diseases Find Children Under 5 Account for Almost One Third of Deaths. [Last accessed on 2018 Dec 19]. Available from: https://www.who.int/news-room/detail/03-12-2015-who-s- first-ever-global-estimates-of-foodborne-diseasesfind-children-under-5-account-for-almost-one-third-of-deaths .
- 10.About FSSAI>Introduction. [Last accessed on 2018 Dec 19]. Available from: http://www.old.fssai.gov.in/AboutFSSAI/introduction.aspx .
- 11.Dudeja P, Gupta RK, Minhas AS. Food Safety in the 21st Century: Public Health Perspective. New Delhi: Academic Press; 2016. p. 628. [Google Scholar]
- 12.World Health Organization. World Health Day 2015: from Farm to Plate, Make Food Safe. SEARO. [Last accessed on 2018 Dec 19]. Available from: http://www.searo.who.int/world_health_day/2015/world-health-day-2015-from-farm-to-plate-make-food-safe/en/
- 13.Revelas A. Healthcare-associated infections: A public health problem. Niger Med J. 2012;53:59–64. doi: 10.4103/0300-1652.103543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bortolussi R. Listeriosis: A primer. CMAJ. 2008;179:795–7. doi: 10.1503/cmaj.081377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Adane M, Teka B, Gismu Y, Halefom G, Ademe M. Food hygiene and safety measures among food handlers in street food shops and food establishments of Dessie town, Ethiopia: A community-based cross-sectional study. PLoS One. 2018;13:e0196919. doi: 10.1371/journal.pone.0196919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Akabanda F, Hlortsi EH, Owusu-Kwarteng J. Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health. 2017;17:40. doi: 10.1186/s12889-016-3986-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Thakur CP, Mehra R, Narula C, Mahapatra S, Kalita Food Safety and Hygiene Practices Among Street Food Vendors in Delhi, India. Int J Current Res. 2013;5:3531–4. [Google Scholar]
- 18.Omomia OA, Omomia TA. Relevance of skinner's theory of reinforcement on effective school evaluation and management. Eur J Psychol Stud. 2014;4:174–80. [Google Scholar]
- 19.Bhattacharya S, Talati S, Gupta AK, Malhotra S, Singh A. New Era, Chandigarh: 2018. Hastpataalon Ke Rashoi Karmiyon ki Vyaktigat Swachta Mein Sudhar Sambandhi Kaushal Vikas (Hindi) Paperback. [Google Scholar]