

Abstract
The source of bleeding in postoperative spinal epidural hematoma (pSEH) is often unclear. We describe a surgical case of pSEH in which the source of bleeding was thought to be the deep cervical artery (DCA). A 67-year-old man underwent C3 laminectomy, C4–6 unilateral open door laminoplasty, and C7 partial laminotomy for cervical spondylotic myelopathy. Intraoperatively, arterial hemorrhage from a distal branch of the right DCA was observed while drilling the lateral end of the C3 lamina, so electrocoagulation hemostasis was performed. A suction drain was used to obliterate the epidural space, and it was removed 22 h postoperatively. The patient suddenly felt posterior cervical pain 26 h postoperatively. Computed tomography demonstrated a huge epidural hematoma at the C3–6 level. The hematoma was evacuated 4 h after the onset of symptoms. Active bleeding was not seen intraoperatively. The patient was discharged on postoperative day 13, and no symptoms caused by the epidural hematoma remained. Considering the findings of the first operation, we concluded that a branch of the DCA might have been the source of bleeding in pSEH, and the site of the drain and removal procedure might have been one of the causes of bleeding. It is important to be aware of the DCA as a blood vessel because it requires careful attention when dissecting the semispinalis cervicis or performing operations for hemostasis before wound closure.
Keywords: postoperative spinal epidural hematoma, deep cervical artery
Introduction
Postoperative spinal epidural hematoma (pSEH) is a serious complication of spinal surgery. There are several reports about the risk factors for pSEH,1–3) but much about the source of bleeding remains unclear. Of 400 cases of cervical laminoplasty, we describe our experience with only one surgical case of pSEH (approximately 0.25%) for which the source of bleeding was thought to be the deep cervical artery (DCA), and the site of the drain and removal procedure were considered to have possibly caused the bleeding.
Case Report
The patient was a 67-year-old man with no noteworthy medical or drug history. He was admitted for surgical treatment of cervical spondylotic myelopathy that was diagnosed based on pain around the right shoulder and right C5 paralysis. Preoperative magnetic resonance imaging showed cervical kyphosis and dural sac compression centered at the C4–6 level (Fig. 1A).
Fig. 1.
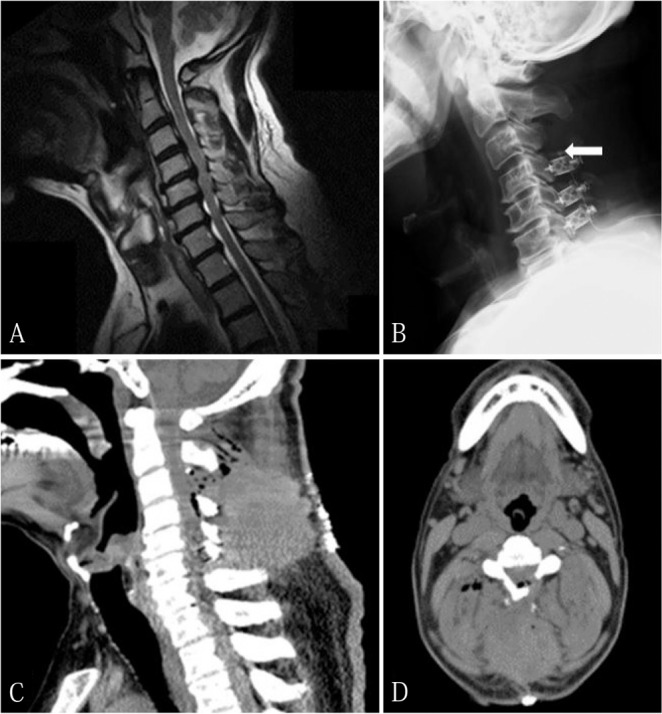
Perioperative imaging study. (A) Preoperative sagittal T1-weighted magnetic resonance imaging scan shows cervical kyphosis and dural sac compression centered at the C4–6 level. (B) Plain radiograph on postoperative day 1. The tip of the drain is placed at the C3–4 level (arrow). (C and D) Computed tomography image on postoperative day 1. Sagittal image shows the spinal epidural hematoma at the C3–6 level (C). Axial image shows the C3/4 level (D).
Laminoplasty was performed using a posterior approach. While drilling the lateral end of the C3 lamina, the anterior portion of the right semispinalis cervicis was damaged, and arterial hemorrhage from a distal branch of the right DCA was observed (Figs. 2A and 2B). Electrocoagulation hemostasis was performed at both the distal branch of the right DCA and semispinalis cervicis. Ultimately, C3 laminectomy, C4–6 unilateral open door laminoplasty, and C7 partial laminotomy were performed. One epidural drain was inserted, and the tip was placed at the C3/4 level (Fig. 1B). The drain was connected to a suction system, and the wound was closed after confirming that injection and suction of physiological saline at the wound site were performed effectively.
Fig. 2.
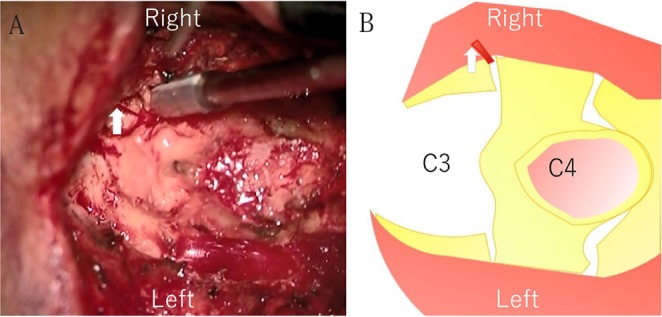
Intraoperative microscopic view. (A) Active bleeding is shown from the right deep cervical artery (arrow). (B) Schema of A. The red line shows spouting bleeding.
Systolic blood pressure was about 120 mmHg when the patient was extubated postoperatively. Pain management was good with patient-controlled analgesia, but systolic and diastolic blood pressures gradually increased; thus, the blood pressures were lowered using a continuous intravenous injection of nitroglycerin (2 mg/h). Discharge from the drain gradually decreased and became serious. There were no signs of surgical site bleeding or subcutaneous bleeding, so the drain was removed 22 h postoperatively.
The patient felt sudden posterior cervical pain upon rising from bed 26 h postoperatively. Although the nervous system symptoms did not worsen, exudative hemorrhage from the wound and subcutaneous bleeding around the surgical site were observed. Computed tomography (CT) showed an epidural hematoma posterior to the C3–6 level (Figs. 1C and 1D). Spouting hemorrhage from the surgical site was observed when the staples were removed in the patient’s hospital room. Subsequently, the patient was transported to the operating theater for hematoma evacuation and bleeding control. The hematoma was evacuated 4 h after the onset of symptoms. Active bleeding was not seen intraoperatively, and the site of bleeding could not be identified. One epidural drain was inserted, and the surgical procedure was completed. Systolic blood pressure was decreased within the target of 140 mmHg or below. The epidural drain was removed on postoperative day 3 without applying negative pressure to it.
The patient progressed without a recurrent increase in hematoma size or worsening of neurological symptoms. Pain around the right shoulder and right C5 paralysis gradually improved, and there were no wound issues. He was discharged on postoperative day 13.
Discussion
Wang et al.’s4) meta-analysis showed that the incidence of pSEH after cervical surgery was 1.1%. To date, several reports suggested that the source of bleeding in pSEH is the split muscle wall,5) epidural venous plexus,6) or radicular artery.7) However, much about the source of bleeding in pSEH remains unclear, and only one report suggested that the source of bleeding in pSEH is outside of spinal canal.5) There are no reports about the DCA being the source of bleeding in pSEH after posterior cervical surgery5–13) (Table 1).
Table 1.
Review of previously reported cases of postoperative spinal epidural hematoma after posterior cervical surgery
| Author | Number of cases | Active bleeding intraoperatively | Operative level |
|---|---|---|---|
| Neo et al.5) | 1 | Artery (Split muscle wall) (Not described about the name of artery) | C3-T1 |
| Ohba et al.7) | 1 | Artery (Radicular artery) | C3–6 |
| Goldstein et al.6) | 8 | Unknown (Hypothesized that epidural venous plexus) | C4–6 C3–6 C3–7 C2–4 C3–6 C2–4 C2–5 C3–5 |
| Lee et al.8) | 1 | Unknown | C3–7 |
| Yi et al.9) | 1 | Unknown | C5/6 |
| Yin et al.10) | 1 | Unknown | C4–7 |
| Ohba et al.7) | 2 | 1. Unknown | C2–7 |
| 2. Unknown | C3–7 | ||
| Anno et al.11) | 4 | 1–4. Unknown | Not described |
| Rasekhi et al.12) | 1 | Unknown | C4–7 |
| Tomii et al.13) | 1 | Unknown | C3–7 |
This case suggests the following two points. First, the DCA can be a possible source of bleeding in pSEH. Second, the site of the drain and removal procedure may inadvertently cause pSEH.
Herein, it was found that the DCA can be a source of bleeding in pSEH. The joint capsules of the zygapophyseal joints, the synovial membranes with their villi and folds receive their blood supply from branches of the DCA, the vertebral artery, the ascending pharyngeal artery, and the uppermost intercostal artery.14) The DCA diverges at the costocervical trunk and is located lateral to the C3–6 lamina.15) Vascular supply at the C3/4 level is shown in Fig. 3 modified from Lang.14) The DCA anastomoses with branches of the vertebral artery and the occipital artery at the lateral end of lamina. In this case, arterial hemorrhage from a distal branch of the right DCA was observed during the initial surgery. An evident source of hemorrhage could not be confirmed during hematoma evacuation. However, it was clear from CT image on postoperative day 1 that the responsible blood vessel was outside of the spinal canal. Thus, considering the anatomy of the DCA, arterial hemorrhage from the right DCA, which was observed during the initial surgery, and the location of the hematoma, the DCA can be a source of bleeding in pSEH. Therefore, operators should be aware of the DCA as one blood vessel that is vulnerable to damage caused by posterior cervical surgery.
Fig. 3.
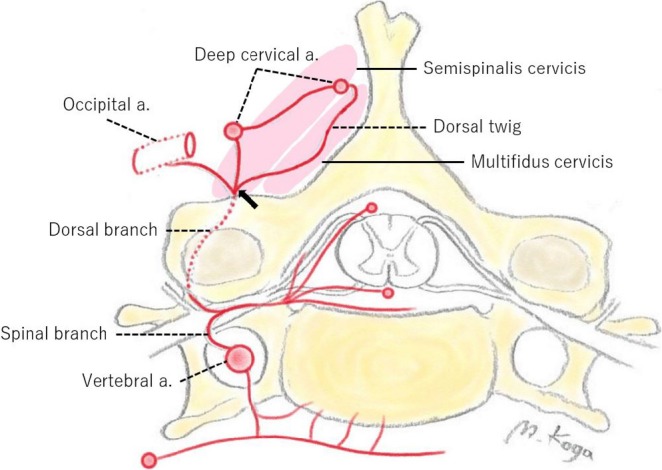
Vascular supply at the Cl level (modified from Lang14)). The deep cervical artery anastomoses with branches of the vertebral artery and the occipital artery at the lateral end of lamina. The damaged point is shown on semispinalis cervicis (arrow).
We also found that the site of the drain and removal procedure may inadvertently cause pSEH. A previous study suggested the possibility of hemorrhage from the drain placement site.16) When the erector spinae muscles are damaged while drilling the lamina, the bleeding point of the damaged artery is buried in the muscle. Therefore, it is difficult to perform complete hemostasis at the damaged artery. As the tip of the drain was placed near the damaged DCA during the initial surgery, it is possible that friction between the tip of the drain and the DCA during the removal of the drain caused recurrent hemorrhage from the DCA. Operators must perform complete hemostasis at the bleeding artery such as the DCA during the procedure of muscle dissection, and it is necessary to consider the location of drain placement and placement period based on each individual case. It has also been reported that connecting the drain to a suction system as quickly as possible during the operation reduces the occurrence rate of pSEH because coagulation of extravascular blood inadvertently causes pSEH.17) In our case, the drain was connected to the suction system before wound closure, and there were no problems in the drain’s function.
Old age (≥60 years), preoperative nonsteroidal anti-inflammatory drug use, large intraoperative blood loss (≥1 L), intraoperative hemoglobin level ≤10 g/dl, Rh+ blood type, prothrombin time-international normalized ratio ≥2.0, multilevel procedures, previous spinal surgery, and alcohol intake have been reported as risk factors for pSEH.1–3) Old age and multilevel procedure were applicable to this case. There are also various reports regarding blood pressure management during the perioperative period. Excluding Kao et al.’s18) study, most studies found that preoperative hypertension is not a risk factor for pSEH.1,2,19) However, an increased blood pressure of 50 mmHg or above during extubation is reported as a risk factor for pSEH.20) Regarding postoperative care, a study reported the possibility that postoperative diastolic hypertension increases blood viscosity, causing blood clots and drain dysfunction, which in turn causes pSEH.18) In Ohba et al.’s7) study, postoperative diastolic hypertension was observed in all four cases of late-onset pSEH (48 or 72 h postoperatively). Although there were no problems in blood pressure management during extubation after the initial surgery in our case, systolic and diastolic blood pressures were abnormally high after the patient returned to the hospital room, which may be related to the occurrence of pSEH.
Conclusion
The DCA should be considered as a possible source of bleeding in pSEH. It is important to be aware of the DCA as a blood vessel because it requires careful attention when dissecting the semispinalis cervicis or performing operations for hemostasis before wound closure. We also found that the site of the drain and removal procedure may inadvertently cause pSEH. Although drainage methods should be modified according to each individual case, there are no clear indexes for the location of drainage placement, application of negative pressure, or duration of drain placement; hence, further investigation of these issues is necessary.
Footnotes
Conflicts of Interest Disclosure
All authors declare no conflicts of interest.
References
- 1).Amiri AR, Fouyas IP, Cro S, Casey AT: Postoperative spinal epidural hematoma (SEH): incidence, risk factors, onset, and management. Spine J 13: 134–140, 2013 [DOI] [PubMed] [Google Scholar]
- 2).Awad JN, Kebaish KM, Donigan J, Cohen DB, Kostuik JP: Analysis of the risk factors for the development of post-operative spinal epidural haematoma. J Bone Joint Surg Br 87: 1248–1252, 2005 [DOI] [PubMed] [Google Scholar]
- 3).Kou J, Fischgrund J, Biddinger A, Herkowitz H: Risk factors for spinal epidural hematoma after spinal surgery. Spine (Phila Pa 1976) 27: 1670–1673, 2002 [DOI] [PubMed] [Google Scholar]
- 4).Wang T, Tian XM, Liu SK, Wang H, Zhang YZ, Ding WY: Prevalence of complications after surgery in treatment for cervical compressive myelopathy: a meta-analysis for last decade. Medicine (Baltimore) 96: e6421, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5).Neo M, Sakamoto T, Fujibayashi S, Nakamura T: Delayed postoperative spinal epidural hematoma causing tetraplegia. Case report. J Neurosurg Spine 5: 251–253, 2006 [DOI] [PubMed] [Google Scholar]
- 6).Goldstein CL, Bains I, Hurlbert RJ: Symptomatic spinal epidural hematoma after posterior cervical surgery: incidence and risk factors. Spine J 15: 1179–1187, 2015 [DOI] [PubMed] [Google Scholar]
- 7).Ohba T, Ebata S, Haro H: Influence of postoperative hypertension on the development of spinal epidural hematoma. Orthop Surg 9: 386–390, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8).Lee SC, Lee ST, Lui TN: Epidural hematoma of the cervical spine after cervical laminectomy in a patient with ventriculo-peritoneal shunt. J Clin Neurosci 11: 302–304, 2004 [DOI] [PubMed] [Google Scholar]
- 9).Yi S, Yoon DH, Kim KN, Kim SH, Shin HC: Postoperative spinal epidural hematoma: risk factor and clinical outcome. Yonsei Med J 47: 326–332, 2006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10).Yin G, Ni B: Acute postoperative cervical spinal epidural hematoma. Acta Orthop Traumatol Turc 48: 437–442, 2014 [DOI] [PubMed] [Google Scholar]
- 11).Anno M, Yamazaki T, Hara N, Ito Y: The incidence, clinical features, and a comparison between early and delayed onset of postoperative spinal epidural hematoma. Spine (Phila Pa 1976) 44: 420–423, 2019 [DOI] [PubMed] [Google Scholar]
- 12).Rasekhi R, Viswanath O, Fu E, Cordova C: Iatrogenic spinal epidural hematoma in the acute postoperative period. Ochsner J 18: 268–270, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13).Tomii M, Mizuno J, Kazama K, Matsushima T, Watanabe K: Delayed postoperative spinal epidural hematoma after cervical laminoplasty. NMC Case Rep J 5: 35–38, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14).Lang J: Clinical Anatomy of the Cervical Spine. New York, Thieme Medical Publishers Inc, 1993, p. 69. [Google Scholar]
- 15).Yue BY, le Roux CM, Corlett R, De La Harpe D, Richardson M, Ashton M: The arterial supply of the cervical and thoracic spinal muscles and overlying skin: anatomical study with implications for surgical wound complications. Clin Anat 26: 584–591, 2013 [DOI] [PubMed] [Google Scholar]
- 16).Aono H, Ohwada T, Hosono N, et al. : Incidence of postoperative symptomatic epidural hematoma in spinal decompression surgery. J Neurosurg Spine 15: 202–205, 2011 [DOI] [PubMed] [Google Scholar]
- 17).Ahn DK, Shin WS, Kim JW, Yi SM: Why cannot suction drains prevent postoperative spinal epidural hematoma? Clin Orthop Surg 8: 407–411, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18).Kao FC, Tsai TT, Chen LH, et al. : Symptomatic epidural hematoma after lumbar decompression surgery. Eur Spine J 24: 348–357, 2015 [DOI] [PubMed] [Google Scholar]
- 19).Modi HN, Lee DY, Lee SH: Postoperative spinal epidural hematoma after microscopic lumbar decompression: a prospective magnetic resonance imaging study in 89 patients. J Spinal Disord Tech 24: 146–150, 2011 [DOI] [PubMed] [Google Scholar]
- 20).Yamada K, Abe Y, Satoh S, Yanagibashi Y, Hyakumachi T, Masuda T: Large increase in blood pressure after extubation and high body mass index elevate the risk of spinal epidural hematoma after spinal surgery. Spine (Phila Pa 1976) 40: 1046–1052, 2015 [DOI] [PubMed] [Google Scholar]