

Abstract
This case series demonstrates that classical homeopathy may have a solution to psoriasis and its complications which goes beyond skin clearance and achieves general well‐being. The variety in clinical phenotypes and their response to treatment may be explained on the basis of the theory of “Levels of Health."
Keywords: case report, erythroderma, homeopathy, personalized medicine, psoriasis
1. INTRODUCTION
Six cases of varying severity of psoriasis are presented here. Two cases had erythroderma one of which developed septicemia. They were all treated exclusively with individualized homeopathy showing improvement in PASI scores and the general condition. The varied results are explored in the background of the concept of “Levels of Health.
Psoriasis a chronic inflammatory disease affecting over 125 million people globally1 besides being psychologically stressful due to its appearance, can cause serious morbidity and mortality due to systemic inflammation.2 Erythroderma is a fulminant, potentially life‐threatening change in psoriasis which may lead to sepsis, organ failure, and death, making its treatment extremely challenging.3 Treatment options are mostly in the form of blockage of inflammatory factors4 and the latest biologics which again come with limitations and complications of their own.5 While they successfully relieve the gross signs of inflammation they give rise to severe immune suppression and their prolonged use is not desirable. A natural alternative if present it would be welcome.6
A combination of genetic and epigenetic phenomenon has been suggested as etiology of psoriasis—an epigenetic trigger over genetic predisposition. It is agreed upon by clinicians and researchers alike that the ideal therapy for this multifactorial disease must act beyond skin clearance and lead to a better quality of life, addressing the comorbidities and systemic inflammation.7
While conventional medicine focuses on the inhibition of inflammation in the skin and therefore generalizes the medication to the diagnosis, classical homeopathy investigates the genetic and epigenetic influences that a person has been subjected to and the individualistic response to them. This, taken into consideration with the presenting symptomatology forms the data on which remedy selection is made, tailoring the therapy to every individual,8, 9 yielding results that are encouraging, despite the severity of the pathology.10, 11, 12, 13 The homeopathic remedies are prepared through a special process called “potentization” which involves dilution and subjecting to calculated friction of the material to be prepared.8
Many studies exist involving homeopathy and psoriasis. The prospective observational study by Witt et al showed that psoriasis may be significant as a therapeutic alternative in practice14; this series however involves cases that were of much greater severity and complication. It also shows different levels of health in the same diagnosis, giving an insight into the probable reason for varied responses to treatment.15
2. CASE SERIES
2.1. Case 1
2.1.1. Case history
43‐year‐old Indian male with psoriasis since 2009 used conventional topical steroids initially but stopped after a while. He also had hypertension but did not take any medication (Table 1, Figure 1). He sought homeopathic therapy in February 2014 with a baseline PASI score (Psoriasis Area and Severity Index) of 2.8. He was under emotional and professional stress which apparently had triggered the condition and responded well with homeopathic medication till the beginning of 2017. In March 2017, severe stress at work and humiliation at the hands of his superiors caused the lesions to flare up—turning cracked and erythrodermic. It got infected from showering, leading to septic condition with fever and inflammation (blood test results in Table 1). His PASI score at this point was 57.6. An abscess the size of a palm developed on the side of his abdomen and he developed high fever (103°F) with severe dullness of sensorium.
Table 1.
Case 1 details of treatment (during erythrodermic precipitation and septic state)
| Date | Symptoms | Remarkable Laboratory findings | Prescription |
|---|---|---|---|
| 31/05/2017 | Severely painful abscess over erythrodermic psoriasis; Fever—discordant with pulse (temperature 103.5°F, but pulse 72/min); very low energy; decreased appetite; weight loss; generally very dull | RBC count: 4.3 × 106 /cmm; Hb: 11 g%; Hematocrit: 36; Total leukocyte count: 16 800/cmm; N: 71; L: 20; Platelet count: 380 × 103/µL; ESR: 76 mm/h | Pyrogenium 200C three times a day for 3 d |
| 05/06/2017 | Fever reduced, but low grade continues—100°F; general state and energy improved. Abscess is large and persisting; psoriasis still exhibiting erythrodermic change. | RBC count: 4.0 × 106/cmm; Hb: 10.7 g%; Hematocrit: 31.5; Total leukocyte count: 19 700/cmm; Platelet count: 380 × 103/µL; N: 81; L: 12; ESR: 90 mm/h | Sulfur 200C one dose—abscess opened and started draining in 2 h after the medication. |
| 27/06/2017 | Profuse pus drainage from the abscess for days after administration of sulfur 200C; healing up well; psoriatic lesions are reduced remarkably—no more erythrodermic in nature; patient is very sensitive to cold | RBC count: 4.0 × 106/cmm; Hb: 9.5 g%; Hematocrit: 30.5; Total leukocyte count: 10 600/cmm; Platelet count: 490 × 103/µL; N: 76; L: 18; ESR: 130 mm/h | Calcarea carbonica 200C one dose |
| 15/07/2017 | General improvement; severe pain in abscess region; another abscess formed and drained below the old one; Possible anti‐doting of remedy by herbal toothpaste | Calcarea carbonica 200C three times a day for three days | |
| 09/08/2017 | Patient was well; Psoriasis remarkably reduced; Relapse of fever when faced with the prospect of returning to work | RBC count: 4.0 × 106/cmm; Hb: 10.4 g%; Hematocrit: 33.5; Total leukocyte count: 15 900/cmm; Platelet count: 590 × 103/µL; N: 78; L: 16; ESR: 48 mm/h | Lycopodium 200C one dose |
| 18/09/2017 | Psoriasis clearing well; now changed completely to plaque type but still quite extensive | Hepar sulfuricum 200C one dose | |
| 20/11/2017 | Psoriatic lesions improved, and much less inflammation; Patient feels well and energetic | RBC count: 4.9 × 106/cmm; Hb: 12.8 g%; Hematocrit: 42; Total leukocyte count: 7500/cmm; Platelet count: 360 × 103/µL; N: 50; L: 43; ESR: 10 mm/h | Wait |
| 03/09/2017 | Psoriasis is clearing up well but appears to be static in progress for a few months. Patient is generally very energetic and feels well. |
Bryonia 200C Patient continues to be under treatment |
|
| 01/10/2018 | Skin lesions are much thinner and erythema is reduced. Scaling is greatly decreased. | Wait |
Figure 1.

Case 1 before and after treatment of erythrodermic psoriasis
2.1.2. Homeopathic intervention
Five months of homeopathic treatment was given from this point till he recovered completely from the septicemia and the erythrodermic condition. The inflammatory state was monitored through blood tests and showed steady improvement (Table1). The septic state responded to Pyrogenium, a medicine that has time and again proven its benefit high infectious and toxemic states.16, 17, 18 There was no culture of the abscess or blood performed as in homeopathic approach the individualized clinical semiology of the septic state is the indicator of the remedy rather than the microorganism involved. The specific keynote of pulse and temperature being out of sync accompanied by offensive odor of bodily discharges along with other pathological features of sepsis direct the homeopathic physician toward this remedy. However, expertise of the homeopathy is a big limitation in this case and such cases must not be handled without prior experience. Once the sepsis improved however the psoriatic lesions still continued to be extensive and required a series of remedies to see the changes depicted in the Figure 1.
2.1.3. Outcome
At the time of reporting, his PASI score is 11.3. He continues to be treated and is on an upward trend skin clearance wise. He had quit his work after the humiliation and was unable to take up another job because of his condition but now is working at a very good company in a very good position and is able to handle the challenges without trouble.
2.2. Case 2
2.2.1. Case history
A 53‐year‐old lady developed psoriasis of the scalp in December 2014 (basic PASI score—2) (Table 2, Figure 2). She also had diabetes mellitus since mid‐2014 and was on antihyperglycemic drugs.
Table 2.
Case 2 Details of Treatment (during erythrodermic precipitation)
| Date | Symptoms | Prescription |
|---|---|---|
| 20/08/2015 | Patient on treatment for diabetes mellitus for 15 mo and psoriasis of scalp for 8 mo suddenly suffered severe increase in the psoriatic lesions and spreading all over the body with erythrodermic change; Fever for one day—100°F | Phosphorous 30C twice a day for 2 d, increased to four times a day when no change was observed |
| 25/08/2015 | Temperature 101.8°F Psoriasis extensive with burning in lesions; Weakness increased; edematous swelling in legs with burning pain | Lac caninum 200C three times a day for 1 wk |
| 31/08/2015 | Temperature 99°F; edema in legs improved; Weakness improved; Skin lesions still spreading | Medorrhinum 30C 4 to 5 times a day for 15 d as required |
| 01/10/2015 | Psoriasis improving—thickness improved; Itching improved; two episodes of fever in the last 2 d—temperature up to 99.2°F | Elaps corallinus 30C three times a day—continued for 50 d |
| 04/09/2018 | Psoriasis—one lesion with mild itching and very mild scaling on the left elbow. Otherwise, no psoriatic lesions. No flare ups or significant lesions for the past 3 y | Patient is still on treatment for her diabetes, but psoriasis does not bother her anymore. There are occasional itching lesions which disappear on their own. |
Figure 2.

Case 2 before and after treatment of erythrodermic psoriasis
2.2.2. Homeopathic Intervention
She sought homeopathic treatment for psoriasis and was responding very slowly for over three months, when she had a flare up after some emotional stress and the lesions turned erythrodermic, spreading all over the body. Her PASI score was 48 at this time and she also developed mild fever of 100°F. The treatment was then tailored to the new situation.
2.2.3. Outcome
Within a month of starting homeopathic treatment for her erythrodermic state, she improved considerably and in 3 months the psoriasis had reduced to PASI score 0.5 (Table 2). She continues to be treated for her diabetes with occasional mild relapse of the psoriasis in the 3 years of follow‐up.
2.3. Case 3
2.3.1. Case history and homeopathic intervention
A 40‐year‐old Indian woman developed psoriasis of the forearms in early 2009. She was from a remote rural background and was seen by the homeopathyhomeopath once a month during a medical camp (Table 3 and Figure 3.1). At the beginning of treatment, the PASI score was 10 with very thick indurated lesions.
Table 3.
Case 3 details of treatment
| Date | Symptoms | Prescription |
|---|---|---|
| 14/09/2006 | Psoriasis of forearms | Phos 30C twice a day for 1 wk |
| 11/01/2007 | Skin smooth | Stopped treatment |
Figure 3.

(1) Case 3 before and after treatment of psoriasis. (2) Case 4 before and after treatment of psoriasis
2.3.2. Outcome
In 3 months, the lesions became simple and less erythematous with PASI score of 0.6. At this point, however she stopped treatment by herself.
2.4. Case 4
2.4.1. Case history
58‐year‐old Indian man developed psoriasis on the sole of his left foot in 2010 and sought homeopathic treatment in 2012 (Table 4 and Figure 3.2). He complained of intense itching.
Table 4.
Case 4 details of treatment
| Date | Symptoms | Prescription |
|---|---|---|
| 22/04/2012 | Psoriasis of soles of feet for 2 y, intense itching aggravated by milk and milk products | Magnesium sulfuricum 10 M one dose |
| 08/05/2012 | Itching reduced | Placebo |
| 23/08/2012 | Itching reduced further | Placebo |
| 24/12/2012 | Psoriatic lesion began decreasing | Placebo |
| 25/02/2013 | Psoriatic lesion improved by 50% | Placebo |
| 22/05/2013 | Psoriasis completely cleared | Stop treatment |
| 10/09/2017 | Patient has stayed clear of psoriasis for over 4 y |
2.4.2. Homeopathic intervention
Along with the psoriatic symptoms, he also complained of confusion of the mind on waking in the morning which got better after passing stools. Such peculiar associations of symptoms are valuable to a homeopath and point to a particular remedy.8
2.4.3. Outcome
His baseline PASI score was 1.2 and he achieved a complete remission in a year.
2.5. Case 5
2.5.1. Case history
A 41‐year‐old Indian male developed psoriasis of the whole body since early 2016, triggered after overuse of antibiotics for recurrent fevers that he suffered for a year before onset of psoriasis (Table 5, Figure 4). Once the psoriasis began, however, the fevers stopped. He was put on topical steroids initially but had graduated to methotrexate, without avail.
Table 5.
Case 5 details of treatment
| Date | Symptoms | Prescription |
|---|---|---|
| 21/01/2017 | Psoriasis for one year—all over the body, intense burning and itching; Insomnia—crowding of thoughts preventing sleep, wakes up with a headache because of this | Natrum muriaticum 1 M one dose |
| 02/02/2017 | Severe aggravation of itching followed by cold, throat pain and fever—102°F | Placebo |
| 18/02/2017 | Psoriatic lesion improved remarkably; sleeping very well | Placebo |
| 21/03/2017 | Skin is smooth—no psoriatic lesions; sleeping very well, no headaches | Placebo |
| 03/11/2017 | Skin still smooth, no lesions; no acute infections; Sleeping very well; Blood markers are normal for inflammatory signs | Stop treatment |
Figure 4.

Case 5 before and after treatment of psoriasis
2.5.2. Homeopathic intervention
At this point, he stopped them and sought homeopathic treatment in 2017. He also had insomnia from stress at work.
2.5.3. Outcome
His baseline PASI score was 22.8 and he achieved a 100% skin clearance indicator (PASI100; indicating complete skin clearance) in 3 months of Classical homeopathic therapy. His blood tests showed no inflammatory signs at the end of treatment and for over 2 years the patient has been monitored without any relapse.
2.6. Case 6
2.6.1. Case history
An 18‐year‐old man developed psoriasis 2 months after being emotionally stressed from failing university examinations in November 2016 (Table 6, Figure 5). The lesions started in the scalp and spread to around and inside the ears.
Table 6.
Details of treatment
| Date | Symptoms | Prescription |
|---|---|---|
| 17/03/2018 | Psoriatic lesions on scalp, elbows, left knee, and calf for one year. Started after failing examinations. Great sadness and feeling of being insulted | Aurum metallicum 1 M one dose |
| 08/05/2018 | Sadness improved. Able to communicate easily with people now. However, psoriatic lesions are increasing with new patches appearing. | Phosphorous 200C one dose |
| 14/08/2018 | Generally, all the lesions are increasing, and new lesions are appearing | Ambra grisea 10 M one dose |
| 30/09/2018 |
After the last medication, the lesions gradually cleared up within a month. Presently completely clear ESR: 2 mm/h; hsCRP: <1.0 mg/L both are normal values |
Wait and watch |
Figure 5.

Case 6 before and after treatment of psoriasis
2.6.2. Homeopathic intervention
He was treated from March 2018 with classical homeopathy. There was a flare up phase in between which reduced with continued treatment and resolved completely.
2.6.3. Outcome
The initial PASI score was 12.8 and a PASI100 was achieved in 5 months time. The erythrocyte sedimentation rate (ESR) and high‐sensitivity C‐reactive protein (hsCRP) at the end of treatment were normal.
3. DISCUSSION
The Levels of Health Theory and The Continuum Theory15, 19 state that people with a low energy complex in their organism (energy available for vital functions including that of immune system—determined by genetic factors and influences on health by previous treatments and stresses) will show tardy response to treatments, require a longer period of treatment and many homeopathic remedies in the right sequence in order to obtain good results; most of these patients cannot be cured and one can only hope to maintain them in a good state. Whereas people with a higher energy complex will respond quicker and will require lesser number of remedies to achieve good results; most of these patients are completely curable. An understanding of the level of health of a patient at presentation helps a physician to assess the prognosis and plan accordingly. In the above cases, one may see different depths of the pathology though the diagnosis remains the same. Patients who had a low state, with comorbid conditions (Cases 1 and 2) showed severe flare ups and took much longer to achieve a state of remission. Even then, they continue to be treated either due to relapses or persistence of the lesions. The others, (Cases 3, 4, 5 and 6) however, presented uncomplicated situations and they achieved skin clearance within a short time and stayed clear even on long follow‐ups.
The question of whether homeopathy may treat critical illnesses such as sepsis and be useful in emergency conditions has been dealt with before now.20, 21, 22 However, a word of caution must be added here. In India, all homeopathic physicians are medically trained doctors and therefore handling a septicemic case may be considered under their care. Even so without expertise and constant vigilance through monitoring of the vital stats and the blood picture (taken every 12 or 24 hours as necessary) as was done in this case, it is not recommended to treat such precarious states. Even in Case 2, extreme caution was taken as erythroderma can easily cause fulminant septicemia and organ failure. The patients in both these cases were aware of their predicament and chose to take homeopathy and without such cooperation on the patient's side and experience and expertise on the physician's part, this treatment is not recommended. The physician in question had experience with severe infections before now18 and therefore endeavored to take up the serious states with utmost precaution.
The PASI score assessment (Figure 6) of these cases shows that considerable skin clearance was achieved in all these cases. The effect of classical homeopathic therapy, however, was even more pronounced on the overall well‐being of the patient. The general well‐being is one of the most important factors for the homeopathic physician to assess the progress of a case. Patients complained of no adverse effects or deterioration in their well‐being while on therapy. On the contrary, the comorbidities eased up and the general state improved. In three cases (Cases 1, 5, and 6), the inflammatory state was assessed by blood tests and proven to be stable. While the absence of control and selection bias make it difficult to categorically take this case series as proof of homeopathic efficacy in psoriasis, it gives enough evidence to plan larger controlled studies to confirm the clinical benefits observed here. The concept of levels of health merits a deeper investigation to understand the varied treatment response in patients with the same pathology.
Figure 6.
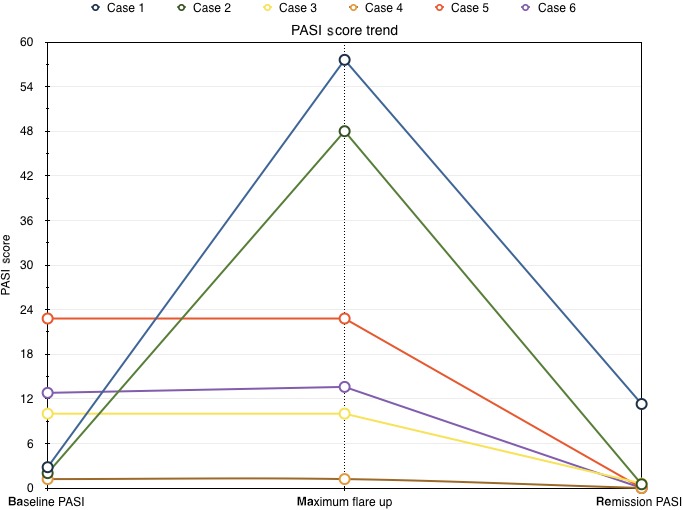
Changes in PASI score
4. CONCLUSIONS
This case series illustrates the considerable improvement in the PASI score of patients with psoriasis treated with individualized homeopathy. The patients also experienced betterment of their general well‐being. Larger controlled studies are necessary to ascertain the clinical benefits observed here.
CONFLICT OF INTEREST
None declared.
AUTHORS' CONTRIBUTIONS
Author 1: collected and analyzed the data, wrote the manuscript, and contributed to referencing. Author 2: collected and analyzed the data. Author 3: collected and analyzed the data. Author 4: analyzed the data, wrote the manuscript, and provided guidance.
Mahesh S, Shah V, Mallappa M, Vithoulkas G. Psoriasis cases of same diagnosis but different phenotypes—Management through individualized homeopathic therapy. Clin Case Rep. 2019;7:1499–1507. 10.1002/ccr3.2197
REFERENCES
- 1. World Psoriasis Day 2016 General Summary [Internet]. Bromma, Sweden: International Federation of Psoriasis Associations; 2016. https://ifpa-pso.com/wp-content/uploads/2017/03/WPD-2016-Report-General-Summary.pdf. Accessed October 3, 2018. [Google Scholar]
- 2. Reich K. The concept of psoriasis as a systemic inflammation: implications for disease management. J Eur Acad Dermatol Venereol. 2012;26:3‐11. [DOI] [PubMed] [Google Scholar]
- 3. Prystowsky J, Cohen P. Pustular and erythrodermic psoriasis. Dermatol Clin. 1995;13(4):757‐770. [PubMed] [Google Scholar]
- 4. Fernandes A, Martins‐Gomes C, Santini A, Silva A, Souto E. Psoriasis vulgaris—pathophysiology of the disease and its classical treatment versus new drug delivery systems. Design of Nanostructures for Versatile Therapeutic Applications. 2018;379‐406.
- 5. Singh J, Wells G, Christensen R, et al. Adverse effects of biologics: a network meta‐analysis and Cochrane overview. Cochrane Database Syst Rev. 2011;2:CD008794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Serhan C. Treating inflammation and infection in the 21st century: new hints from decoding resolution mediators and mechanisms. FASEB J. 2017;31(4):1273‐1288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Chandra A, Ray A, Senapati S, Chatterjee R. Genetic and epigenetic basis of psoriasis pathogenesis. Mol Immunol. 2015;64(2):313‐323. [DOI] [PubMed] [Google Scholar]
- 8. Hahnemann S. Organon of Medicine. New Delhi, India: B Jain Publishers; 2009. [Google Scholar]
- 9. Vithoulkas G, Tiller W. The Science of Homeopathy. Athens, Greece: International Academy of Classical Homeopathy; 2009. [Google Scholar]
- 10. Mahesh S, Mallappa M, Vithoulkas G. Gangrene: five case studies of gangrene, preventing amputation through homoeopathic therapy. Indian J Res Homoeopathy. 2015;9(2):114. [Google Scholar]
- 11. Mahesh S, Mallappa M, Tsintzas D, Vithoulkas G. Homeopathic treatment of vitiligo: a report of fourteen cases. Am J Case Rep. 2017;18:1276‐1283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Mahesh S, Mallappa M, Vithoulkas G. Embryonal carcinoma with immature teratoma: a homeopathic case report. Complemen Med Res. 2017;25(2):117‐121. [DOI] [PubMed] [Google Scholar]
- 13. Tenzera L, Djindjic B, Mihajlovic‐Elez O, Pulparampil B, Mahesh S, Vithoulkas G. Improvements in long standing cardiac pathologies by individualized homeopathic remedies: a case series. SAGE Open Med Case Rep. 2018;6:75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Witt C, Lüdtke R, Willich S. Homeopathic treatment of patients with psoriasis – a prospective observational study with 2 years follow‐up. J Eur Acad Dermatol Venereol. 2009;23(5):538‐543. [DOI] [PubMed] [Google Scholar]
- 15. Vithoulkas G. Levels of Health. Alonissos, Greece: International Academy of Classical Homeopathy; 2017. [Google Scholar]
- 16. Ahmad S, Abbasi W, Rehman T. Evaluation of antipyretic activity of Belladonna and Pyrogenium ultrahigh dilutions in induced fever model. J Complement Integr Med. 2018;16(1): https://www.degruyter.com/view/j/jcim.2019.16.issue-1/jcim-2018-0127/jcim-2018-0127.xml. [DOI] [PubMed] [Google Scholar]
- 17. Frass M, Zagorchev P, Yurukova V, et al. Two cases of fulminant hepatic failure from amanita phalloides poisoning treated additively by homeopathy. Ochsner J. 2014;14(2):252‐258. [PMC free article] [PubMed] [Google Scholar]
- 18. Mahesh S, Mallappa M, Vithoulkas G. Could homeopathy become an alternative therapy in dengue fever? An example of 10 case studies. J Med Life. 2018;11(1):75‐82. [PMC free article] [PubMed] [Google Scholar]
- 19. Vithoulkas G, Carlino S. The “continuum” of a unified theory of diseases. Med Sci Monit. 2010;16(2):SR7‐15. [PubMed] [Google Scholar]
- 20. Frass M, Linkesch M, Banyai S, et al. Adjunctive homeopathic treatment in patients with severe sepsis: a randomized, double‐blind, placebo‐controlled trial in an intensive care unit. Homeopathy. 2005;94(2):75‐80. [DOI] [PubMed] [Google Scholar]
- 21. Oberbaum M, Schreiber R, Rosenthal C, Itzchaki M. Homeopathic treatment in emergency medicine: a case series. Homeopathy. 2003;92(1):44‐47. [DOI] [PubMed] [Google Scholar]
- 22. Teixeira M, Leal S, Ceschin V. Homeopathic practice in Intensive Care Units: objective semiology, symptom selection and a series of sepsis cases. Homeopathy. 2008;97(4):206‐213. [DOI] [PubMed] [Google Scholar]