

ABSTRACT
Introduction
A third of all children spend at least 60 min·d−1 in moderate to vigorous physical activity (MVPA) as recommended by the World Health Organization. We investigated the distribution of objectively measured physical activity (PA) intensities achieved by schoolchildren during physical education (PE) and organized youth sports (OYS) and the contribution of PE and OYS to the achievement of the PA recommendations.
Methods
In two surveys, PA of 396 children was measured using accelerometry during typical school weeks. Proportions (%) of sedentary behavior, light PA, and MVPA per day and particularly during sports were assessed in children 6–17 yr old. Adjusted odds ratios (AOR) were calculated to analyze the association between frequency (d·wk−1) and duration (min·wk−1) of PE and OYS and meeting the PA recommendations.
Results
Average proportions of MVPA during PE and OYS ranged between 15% and 31%. Between 68% and 74% of children (6–10 yr) and between 27% and 37% of adolescents (11–17 yr) met the PA recommendations. In both age-groups, PE and OYS on at least 2 d·wk−1 were both significantly associated with meeting the PA recommendations (AOR for PE = 3.60, 95% confidence interval [CI] = 2.05–6.31; AOR for OYS = 3.83, 95% CI = 2.09–6.99), compared with no PE or no OYS in that week. Likewise, significant AOR values were found for >90 min of PE per week (AOR = 3.48, 95% CI = 2.03–5.98) and >120 min of OYS per week (AOR = 3.72, 95% CI = 2.01–6.89), compared with no PE or no OYS in that week, respectively.
Conclusion
Schoolchildren spent less than one-third of PE and OYS in MVPA. PE and OYS were found to support children and adolescents to engage sufficiently in MVPA as recommended by the World Health Organization.
Key Words: ACTIVITY BEHAVIOR, ACCELEROMETRY, ACTIVITY GUIDELINES, CLUB SPORTS, SCHOOL SPORTS, PREVENTION
Physical activity (PA) is known to have beneficial effects on several health indicators such as cardiometabolic parameters or bone health in children and adolescents (1,2). Although many intervention studies in school-age children have been conducted to increase young people’s PA (3–5), only one-third of young people actually achieve at least 60 min of moderate to vigorous PA (MVPA) per day as recommended by the World Health Organization (WHO) (1). To assess PA levels in epidemiological studies, accelerometers have become the most frequently used objective technology worldwide. These lightweight devices assess accurately the frequency, duration, and different intensities of PA (6–10). However, some limitations have to be considered when accelerometry is used to assess sedentary behavior (SB), light PA (LPA), and MVPA. Accelerometers are unable to measure certain high-intensity activities such as swimming, cycling, and strength training (10,11). Another important limitation is that established devices were not previously able to assess the context of PA, which has only been available by the simultaneous application of questionnaires or diaries (7,8,10). The latter may record the timing of sports activities on an individual level during accelerometer wearing periods. Merging information from activity diaries with objective PA data facilitates investigation of PA intensities during sports activities such as physical education (PE) or organized youth sports (OYS). Because the extent to which sports activities contribute to total PA is yet inconclusive (12–15), this approach is needed to enable researchers to reliably estimate the association between the objectively measured volume of sports activities and their contribution to the overall volume of PA. Further, it is used to evaluate if the specific guidelines of at least 50% MVPA during PE classes are achieved by schoolchildren as recommended by the Centers for Disease Control and Prevention (CDC) (16).
Recent studies investigating the proportion of different PA intensities such as SB, LPA, and MVPA during sports activities in children and adolescents have reported large discrepancies of MVPA ranging from 10% to 74% (12–15,17–20). Two reviews are available from Fairclough and Stratton (17) as well as Hollis and colleagues (19) showing that the proportion of MVPA during PE classes in young schoolchildren (<12 yr) ranges between 37% and 45%. Thus, proportions of MVPA are below the abovementioned guidelines during PE (19,21). Currently, no guidelines for the proportion of MVPA during OYS exist, but a reasonable argument not to apply the PE guidelines for OYS was not found. Further, the evidence on the proportion of MVPA during OYS in school-age children is scarce because of the low number of studies conducted in this field (12,13,15,18,22). The present study evaluated the proportion of different PA levels during PE and OYS in 396 German children and adolescents as well as the contribution of PE or OYS to the achievement of the PA recommendations given by the WHO. First, durations and proportions of SB, LPA, and MVPA during PE and OYS in children 6–10 yr old and adolescents 11–17 yr old were measured. Second, we analyzed the association between different frequencies and durations of PE or OYS and the achievement of the PA recommendations of at least 60 min MVPA per day.
METHODS
Study sample
For this study, two surveys were carried out between September 2012 and June 2013, including two primary and two secondary schools in the city of Bremen (Germany). Children (6–10 yr) from 14 classes and adolescents (11–17 yr) from 10 classes were invited to participate in the study (see Fig. 1), and their parents were asked for written informed consent. Adolescents were asked for written consent, whereas primary schoolchildren were also asked for oral consent. Further information on recruitment and measurements can be found elsewhere (23). The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the institutional review board of the University of Bremen (23). For the baseline measurement (September 2012 to February 2013), 376 participants (51% boys) provided accelerometer data of at least 1 d up to 7 d and completed activity diaries, resulting in 2207 objectively measured days. In the follow-up measurement (March to June 2013), 280 participants from baseline took part, and an additional 20 participants were newly recruited. After exclusion of invalid measurements, a total of N = 396 participants (51% boys) were available for the daily sample (Fig. 1).
FIGURE 1.
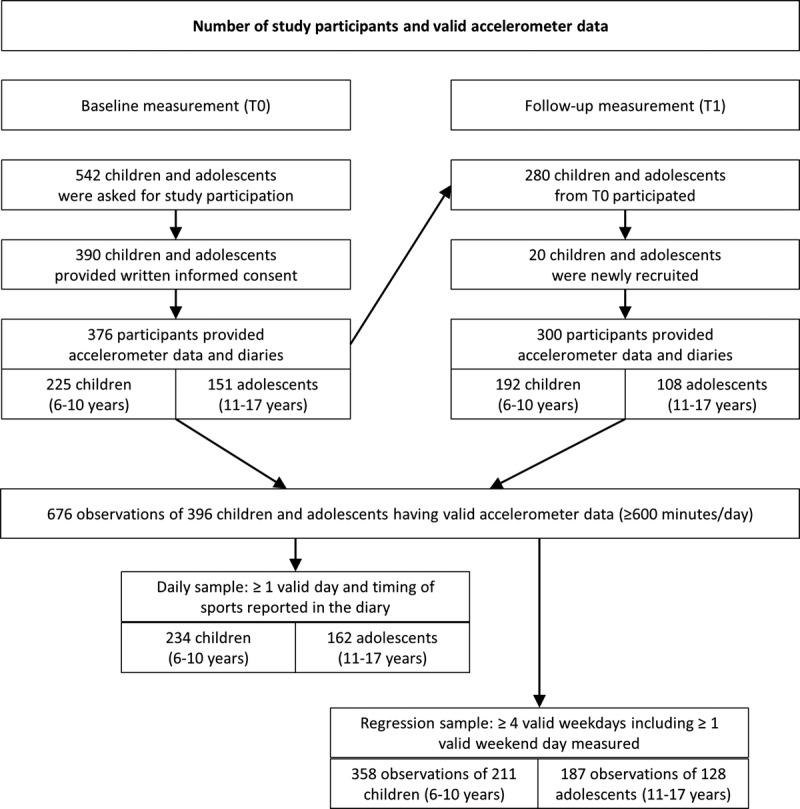
Number of study participants and valid accelerometer data.
Accelerometry
In each survey, PA was measured at 3-s epochs using ActiGraph accelerometers (ActiGraph Corp., Pensacola, FL) and computed with the ActiLife 6 software. In both surveys, about one-third of the children wore GT3X+ (33%), whereas 25% wore the GT1M and 42% the ActiTrainer, respectively. The abovementioned ActiGraph accelerometer models (GT1M, GT3X, and ActiTrainer) have been widely used to assess PA in children and adolescents in previous studies (24–28). For each survey, study participants were instructed to wear the devices for seven consecutive days, including weekdays and weekend days. The accelerometers were attached with an elastic belt and worn on the right hip during waking hours, except when showering, bathing, and swimming. One week later, accelerometers and diaries were collected by the survey personnel and without reminder. Periods with consecutive zero counts of 90 min and more were excluded from the analysis (29). Accelerometer counts were categorized according to the cutoff points proposed by Evenson and colleagues (30) (SB, ≤25 counts/15 s; LPA, 26–573 counts/15 s; MVPA ≥574 counts/15 s). Evenson cutoff points were divided to match the 3-s epoch setting used in our study. Most accelerometer studies in school-age children included accelerometer data of 3–4 weekdays with a minimum daily wear time of 10 h as representative for PA during a typical week, but less than half of them required a weekend day (31). The daily sample describes average SB, LPA, and MVPA expressed as minutes and proportions (%) per day as well as proportions of PA intensities, i.e., SB, LPA, and MVPA during total time of PE and OYS. For the regression analyses (regression sample), only participants were included who provided at least four weekdays including at least one weekend day in any survey as recommended (31), resulting in N = 545 observations for N = 339 children and adolescents. We averaged daily information over valid days for each survey per child to calculate the average PA intensities and the number of days with PE and/or OYS. To classify whether children and adolescents achieve the PA recommendations of the WHO or not, daily MVPA was summed up and divided by the number of valid days for each survey. This way, most participants provided observations for both surveys, including overall PA levels for baseline and follow-up. For each survey, participants that showed average daily MVPA of at least 60 min were categorized as sufficiently active according to the recommendations.
Accelerometer diary and time-stamping of accelerometer data
All participants were asked to complete a short paper-based diary to record time points of putting on the device in the morning and removing it in the evening as well as non–wear time during the day, including the reasons for removing the accelerometer. Participants were instructed verbally and in writing on how to use the accelerometer and the diary. To evaluate objectively measured PA during PE and OYS, the particular timing of sports activities (PE and OYS) was recorded in the diaries. After merging all objectively measured counts during sports-related time intervals, durations (min·wk−1) and proportions (%) of SB, LPA, and MVPA during PE and OYS were calculated.
Statistical analyses
The durations and proportions spent in different PA levels were calculated for each measurement day. Furthermore, proportions of SB, LPA, and MVPA during the time intervals of PE and OYS were calculated. We investigated the association between different frequencies and durations of weekly PE and OYS (independent variables) and the achievement of the PA recommendations of at least 60 min MVPA per day on average (dependent variables) in N = 545 observations of N = 339 children and adolescents by conducting logistic mixed models. Mixed models are capable of handling unbalanced longitudinal data, i.e., unbalanced number of observations in participants, and can account for possible clustering in the data. We considered residual-side random effects to account for repeated measurements in participants that provided two aggregated measures of PA in both surveys. In addition, we modeled a random intercept to account for different measures induced by the use of different ActiGraph models. Participants were categorized according to the frequency of participating in sports activities per week: one day with PE or OYS, two or more days with PE or OYS, and no PE or OYS (reference) (model 1). To estimate the duration of sports activities per week in the analysis, the total time of PE and OYS was categorized. For PE, one unit was considered as 45 min because this is the typical duration of PE classes in Germany, whereas we considered 60 min of OYS as one unit (model 2). Models were calculated and stratified by age-groups and adjusted by sex. To account for possible selection effects in the sample by the number of provided measurements in days and seasonal effects, respectively, we conducted sensitivity analyses by estimating regression models based on observations of children, who provided at least five or six valid weekdays for the respective observation in any survey and by adjusting regression models for season. Statistical analyses were conducted with SAS (9.3 SAS Institute Inc., Cary, NC) using the GLIMMIX procedure.
RESULTS
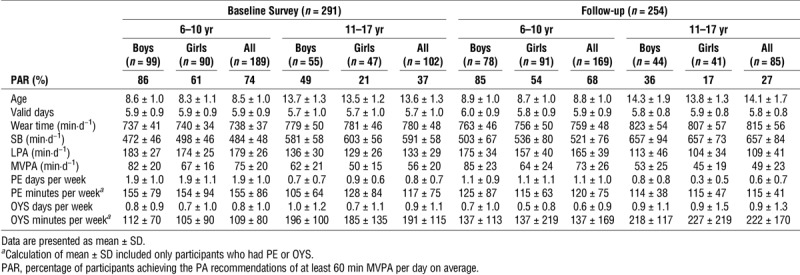
Table 1 describes PA levels in participants. At the baseline measurement, the mean age was 8.5 yr for primary schoolchildren and 13.6 yr for adolescents (Table 1). In both measurement periods, the mean valid wear time per day was longer than 12 h in both age-groups, and the number of measurement days were similar in boys and girls. Primary schoolchildren spent approximately 2 h less SB per day and almost about 50 and 20 min·d−1 more LPA and MVPA, respectively, compared with adolescents. At baseline, 74% of children (6–10 yr) and 37% of adolescents (11–17 yr) met the recommendation of at least 60 min MVPA per day. In particular, adolescent girls spent the least time in MVPA at baseline and follow-up measurement. In both, baseline and follow-up, younger children engaged more frequently (1.1–1.9 d) and longer (120–155 min) in PE per week, compared with adolescents who engaged an average of 0.6 and 0.8 d and 115 and 117 min in PE per week. Although the number of OYS days per week was similar in both age-groups, the weekly duration of OYS was about 80 min longer among adolescents compared with children.
TABLE 1.
Age, wear time, and PA values (mean and SD) in children and adolescents (N = 339).
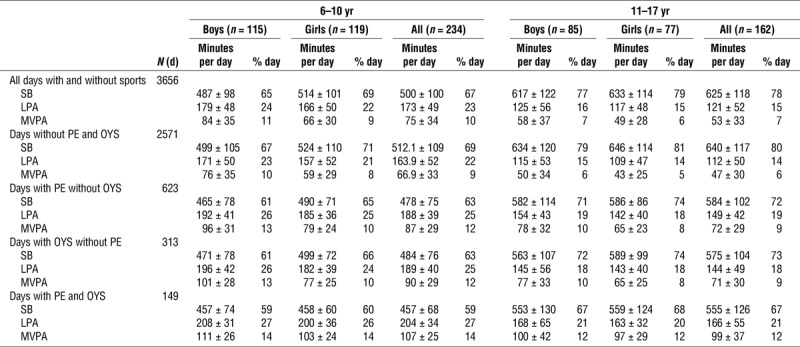
Of all 3656 measured days, no sports activities were reported for 67% and 76% of the days in primary schoolchildren and adolescents, respectively. PE was reported on 17% of all days across both age-groups. The lowest proportion of active time (sum of LPA and MVPA) as well as the highest proportion of average daily SB occurred on days without any sports activities with the average daily SB proportion ranging from 67% in primary school boys to 81% in adolescent girls (Table 2). By contrast, proportions of SB were lower (59%–68%) on days with PE and OYS in boys and girls of both age-groups. Compared with days without sports activities, PE and OYS increased daily MVPA values to similar extents for boys and girls in both age-groups.
TABLE 2.
Minutes per day (mean ± SD) and proportions (%) of SB, LPA, and MVPA on days either with or without sports (N = 396).
About 60 min MVPA were accumulated on days without sports activities in children, with slightly lower MVPA levels on weekend days, compared with weekdays (Fig. 2). However, additional sports activities (PE or OYS) facilitated increasing daily MVPA values up to 70–90 min on any day of the week.
FIGURE 2.
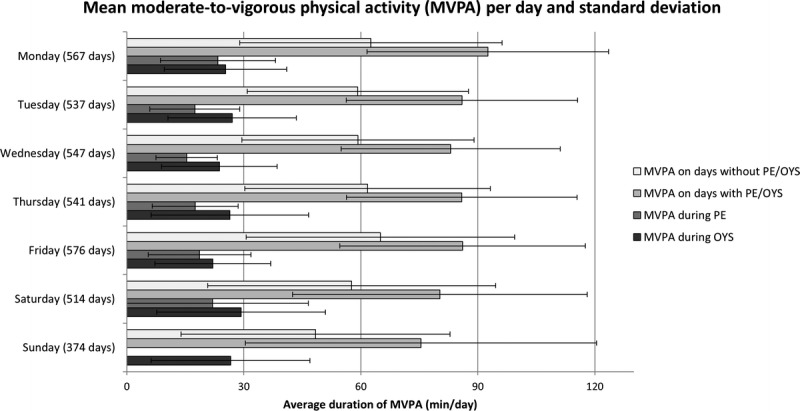
Mean MVPA per day, and SD.
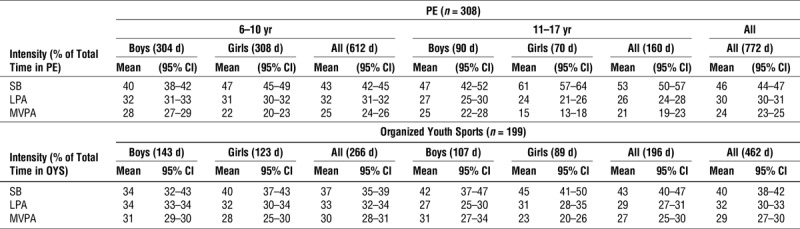
Primary schoolchildren spent more than half of the total time of PE (57%) in either LPA or MVPA (Table 3), whereas adolescents spent only 47% in LPA and MVPA. In particular, adolescent girls achieved the lowest activity levels, spending only 15% of total time of PE in MVPA. Independent of age and sex, higher proportions of SB and lower proportions of MVPA were observed during time of PE compared with time of OYS. Similar to PE, the average duration of OYS was shorter in primary schoolchildren compared with adolescents, but higher proportions of LPA and MVPA were observed in the younger age-group. The proportion of SB in total time of OYS was indeed below 50% in both age-groups and in both sexes, with the lowest proportion observed in primary schoolchildren, compared with adolescents.
TABLE 3.
Proportion (%) of SB, LPA, and MVPA during total time of PE and OYS in children and adolescents.
Compared with children and adolescents without any PE or OYS, both children and adolescents had a significantly higher chance to meet the PA recommendations if they had either PE (adjusted odds ratio [AOR] in children = 3.28, AOR in adolescents = 5.52) or OYS (AOR in children = 9.38, AOR in adolescents = 2.57) for at least two times per week (Table 4). The chance of meeting the PA recommendations was significantly higher for children and adolescents who participated in more than 90 min·wk−1 in PE (AOR = 3.48, 95% confidence interval [CI] = 2.03–5. 98) or in more than 120 min·wk−1 in OYS (AOR = 3.72, 95% CI = 2.01–6.89), compared with those who did not participate in PE or OYS, respectively. In particular, children 6–10 yr old having more than 120 min OYS per week were 13 times more likely to meet the PA recommendations (AOR = 13.15, 95% CI = 3.08–56.17) than children having no OYS. The number of observations was relatively small in the highest categories of frequency and duration of sports activities (≥2 d·wk−1, >90/120 min PE/OYS per week) compared with the other categories, particularly regarding the PE frequency of ≥2 d·wk−1 in adolescents (n = 23), which led to less accurate estimates. Indeed, about one-third (both measurement periods combined) of adolescents 11–17 yr old were sufficiently active, and the AOR values in models 1 and 2 showed higher chances of meeting the PA recommendations in both age-groups. Sensitivity analyses regarding average information over different numbers of valid weekdays and seasonal effects revealed slightly higher AOR values but lower precision, i.e., wider confidence limits, compared with the presented results, particularly due to the smaller sample size (data not shown).
TABLE 4.
Association between frequency and duration of PE and OYS and the achievement of PA recommendations in terms of AOR and 95% CI against the reference category (ref.) estimated in logistic mixed regression models stratified by age-groups.

DISCUSSION
In our study, objectively measured PA data were merged with information from activity diaries to investigate the proportions of SB, LPA, and MVPA during PE and OYS in children between 6 and 17 yr under free-living conditions. Further, we analyzed the association between different frequencies and durations of sports activities and the achievement of the PA recommendations. To the best of our knowledge, this is the first study investigating proportions of different PA intensities during PE and OYS and the contribution of PE or OYS to the achievement to the WHO recommendations in primary and secondary school boys and girls. We observed proportions around 30% of time spent in MVPA during sports activities. Their proportions are substantially lower than the recommended level of 50% during PE as recommended by the CDC (21). We observed that MVPA was higher in boys than that in girls as well as lower in adolescents 11–17 yr old, compared with children 6–10 yr old, which is in line with recent studies (32,33).
Proportions of PA intensities during PE and OYS
The previously observed proportions of MVPA during PE differing between 11% and 85% (19) may be explained by the application of different methods (accelerometry, direct observation, and heart rate monitoring) for PA measurement (17,19,34). The review by Fairclough and Stratton (17) reported proportions of MVPA during PE of 37% for accelerometry, 40% for heart rate monitoring, and 33% based on direct observation (17). Similarly, the observed proportions of MVPA during PE of 25% in children and 21% in adolescents in the current study were well below the CDC guidelines of at least 50%. By contrast, higher proportions of MVPA during PE were reported by a more recent review by Hollis and colleagues (19), with proportions of MVPA varying between 33% for accelerometry and 58% for direct observation. Indeed, in 8 of the included 13 studies, trained PE teachers were involved, who are known to better motivate children to engage more intensively during sports compared with ordinary classroom teachers (19,34). One recent study from Germany (18) investigated the contribution of different domains to total PA in 1403 adolescents 15 yr old on average and reported proportions of SB, LPA, and MVPA during PE of 23%, 43%, and 29% among adolescent boys, respectively, and of 27%, 53%, and 16% among adolescent girls (18). The proportions of MVPA are very similar to our findings (boys 25%; girls, 16%), whereas the differences regarding SB and LPA may be due to the differing epoch settings (60 s) and the use of cutoff points proposed by Freedson and colleagues (26). The latter are known to underestimate MVPA in children (28). Finally, the results of our study indicate that the sex-specific differences of MVPA levels observed in adolescents 11–17 yr old during PE were smaller in younger children.
Compared with PE, there exist no international guidelines with recommended MVPA levels that should be achieved during OYS. The two existing reviews considering proportions of PA intensities during sports activities (17,19) were limited to PA in the school context, supporting the statement of Smith and colleagues (15) that MVPA levels during PE have been well studied in contrast to MVPA during OYS (15). Moreover, only a few studies investigating PA intensities reported proportions across the entire PA intensity continuum (including SB and LPA) (12,13,18,35). Most studies investigating MVPA during OYS reported between 22% and 46% MVPA (12,13,18,20,22). For example, Leek and colleagues (12) observed 46% MVPA during OYS in children 7–14 yr old (n = 200) (12). A general explanation for low proportions of MVPA (~30%) during OYS observed by recent studies (13,18,22) and our study is that sports activities are always accompanied by other activities before and after the sports activities such as changing clothes or showering that could be regarded as part of sports activities by participants who complete activity diaries. Sports activities may further be interrupted by resting breaks, waiting queues, and instructions by coaches. Moreover, balance training and isometric muscular exercises that are frequently included during PE and OYS are very likely to be at least moderate PA (34) but may be categorized as sedentary or LPA by accelerometry because no/low acceleration on the hip is measured during such activities. Finally, the proportions of SB, LPA, and MVPA did not differ substantially between the baseline measurement and the follow-up measurement, neither for PE nor for OYS.
PA levels on days with and without sports activities
Our results align with recent studies that found the duration of MVPA to be significantly longer on days with sports activities such as PE or OYS, compared with days without sports activities (13–15,35–37). In one study by Wickel and Eisenmann (13), 119 children 6–12 yr old wore accelerometers during days they participated in OYS. They achieved 110 min of MVPA on average and a proportion of 23% MVPA per day. Such long durations of MVPA were not even reached on days children engaged in both PE and OYS in our study. Two other studies (14,37) reported increases of MVPA by 50%–60% on days when school-age children attended PE classes, a result we could only confirm when comparing days without any sports activities to days with both PE and OYS. Regarding proportions of SB, we were able to confirm the results of Sigmund and colleagues (35) who observed a smaller proportion of total daily SB in children 9–11 yr old on days with PE compared with days without PE. A German study reported that adolescents 15 yr old on average spent almost two-thirds of their daytime sedentary, nearly one-third in LPA, and under 5% in MVPA (18). In our study, such low activity levels were only observed on days without any sports activities in the least active subgroup of adolescent girls (5% MVPA).
Association between PE or OYS and the achievement of the PA recommendations
Recent studies investigating the contribution of sports to total daily MVPA concluded that sports activities may significantly increase MVPA levels on days with PE or OYS, but these effects were not sustained over the entire week (12–15). By contrast, we observed that engaging more frequently and longer in PE or OYS significantly increased the chance of meeting the PA recommendations of at least 60 min MVPA per day during a typical school week. Although the proportion of participants meeting the PA recommendations was much higher in younger children (6–10 yr) compared with adolescents (11–17 yr), the chance of achieving an average of 60 min MVPA per day was significantly increased in both age-groups. However, on a daily basis, children and adolescents who engaged in OYS showed similar MVPA levels on days without any sport activities compared with children who did not engage in OYS. Further, both groups showed increased level of MVPA for about 20 min·d−1 when engaging in PE (data not shown). Hence, higher MVPA levels in children and adolescents with more PE or OYS may solely be explained by the MVPA that was accumulated during sports activities, and a general more active lifestyle may not be assumed in children and adolescents who regularly participate in OYS. Because PE is mandatory in schools, increasing the number of PE classes may be an effective strategy to promote a more active daily life in school-age children. In contrast to PE, factors such as membership fees or the availability of sports equipment need to be considered as potential barriers to engage in OYS for some children who would need additional support to maintain an active lifestyle.
Strengths and limitations
An important strength of this study is the combination of objectively measured PA with activity diary information for two different contexts of sports activities under free-living conditions. Hence, we were able to analyze the association between the frequency and the duration of PE or OYS and the achievement of the PA recommendations among boys and girls in two different age-groups. Another strength is that the large longitudinal sample of schoolchildren that included repeated observations of two PA measurements could be handled using linear mixed models and increased our statistical power for this analysis. Moreover, we used short sample intervals of 3 s as recommended (35,38) because sampling intervals of 15 s or longer have shown to provide significantly lower MVPA values than shorter epoch settings (38,39). When using different ActiGraph accelerometers, care should be taken because of inconclusive findings in validation studies. Although some studies showed that the GT1M and the GT3X provide comparable counts across all PA intensities (26,27,40), one of these studies highlighted significantly lower counts measured by the ActiTrainer, when comparing to counts measured by the GT1M and the GT3X (40). Another study comparing three ActiGraph models only pointed out that differences occur particularly for counts at lower PA intensities such as LPA and SB (41). To avoid potential over- or underestimations of results, future studies should consider accounting for different ActiGraph models in the analyses similar to our approach using random effects models to account for within model variation by means of a random intercept. Another important limitation is that we had to rely on the accuracy of time intervals reported in the accelerometer diaries, and we were not able to distinguish between the actual sports activities and the activities such as changing clothes, showering, and instructions by the coach/teacher. This is indeed an issue to be considered when assessing sports activities under free-living conditions. Furthermore, we must acknowledge that the younger children in this study might be a selective sample, with 68%–74% of all children 6–10 yr old achieving the PA recommendations of 60 min·d−1. Another important limitation of accelerometers is their inability to assess water-based activities such as swimming. As a result, the total MVPA may be underestimated because no direct observation was applied in our study. Finally, we must acknowledge that our study sample does not claim to be representative for German schoolchildren. Future research needs to investigate determinants that explain and support children and adolescents to create and maintain an overall active lifestyle.
To conclude, the proportion of MVPA during PE and OYS in schoolchildren was on average below 30%, with particular low MVPA proportions of 15% and 23% observed in adolescent girls during PE and OYS, respectively. However, participation in PE or OYS on at least 2 d·wk−1 or engaging for more than 90 min in PE or 120 min in OYS per week significantly increased the chance to meet the PA recommendations of at least 60 min MVPA per day in children and adolescents. More frequent and longer mandatory PE classes and the participation in OYS can substantially increase MVPA particularly in adolescents.
Acknowledgments
The authors declare no conflict of interest. The sponsors did not influence the design of the study; the collection, analysis, or interpretation of data; the writing of the manuscript; or the decision to publish the results. The results of the current study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The authors thank all participating children, parents, schools, and teachers for supporting the present study. The authors also thank everyone who helped with the data collection.
The present study was carried in the framework of the Competence Network of Obesity and funded by the Federal Ministry of Education and Research (BMBF). The Leibniz Institute for Prevention Research and Epidemiology (BIPS) has received funding from the Federal Ministry of Education and Research (grant no. DLR 01GI1129). The authors received no funds for covering costs to publish in open access. The results of the present study do not constitute an endorsement by the American College of Sports Medicine.
Antje Hebestreit and Wolfgang Ahrens conceived and designed the study; Ole Sprengeler conducted the data collection; Ole Sprengeler, Christoph Buck, and Norman Wirsik analyzed the data; Ole Sprengeler drafted the manuscript; and all authors revised the paper and approved the final version submitted.
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the institutional review board of the University of Bremen (06-3, approved on the November 18, 2011).
The authors declare that they have no competing interests.
REFERENCES
- 1.Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7:40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Poitras VJ, Gray CE, Borghese MM, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6 Suppl 3):S197–239. [DOI] [PubMed] [Google Scholar]
- 3.Harris KC, Kuramoto LK, Schulzer M, et al. Effect of school-based physical activity interventions on body mass index in children: a meta-analysis. CMAJ. 2009;180(7):S719–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ. 2012;345:e5888. [DOI] [PubMed] [Google Scholar]
- 5.Heath GW, Parra DC, Sarmiento OL, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet. 2012;380(9838):272–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Trost SG. State of the art reviews: measurement of physical activity in children and adolescents. Am J Lifestyle Med. 2007;1(4):299–314. [Google Scholar]
- 7.Reilly JJ, Penpraze V, Hislop J, et al. Objective measurement of physical activity and sedentary behaviour: review with new data. Arch Dis Child. 2008;93(7):614–9. [DOI] [PubMed] [Google Scholar]
- 8.Westerterp KR. Assessment of physical activity: a critical appraisal. Eur J Appl Physiol. 2009;105:823–8. [DOI] [PubMed] [Google Scholar]
- 9.Ekelund U, Tomkinson G, Armstrong N. What proportion of youth are physically active? Measurement issues, levels and recent time trends. Br J Sports Med. 2011;45(11):859–65. [DOI] [PubMed] [Google Scholar]
- 10.Helmerhorst HJ, Brage S, Warren J, Besson H, Ekelund U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int J Behav Nutr Phys Act. 2012;103(9):1–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rowlands AV, Eston RG. The measurement and interpretation of children’s physical activity. J Sports Sci Med. 2007;6:270–6. [PMC free article] [PubMed] [Google Scholar]
- 12.Leek D, Carlson JA, Cain KL, et al. Physical activity during youth sports practices. Arch Pediatr Adolesc Med. 2011;165(4):294–9. [DOI] [PubMed] [Google Scholar]
- 13.Wickel EE, Eisenmann JC. Contribution of youth sport to total daily physical activity among 6- to 12-yr-old boys. Med Sci Sports Exerc. 2007;39(9):1493–500. [DOI] [PubMed] [Google Scholar]
- 14.Castillo JC, Clark BR, Butler CE, et al. Support for physical education as a core subject in urban elementary schools. Am J Prev Med. 2015;49(5):753–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Smith M, Berdel D, Nowak D, et al. Sport engagement by accelerometry under field conditions in german adolescents: results from GINIPlus. PloS One. 2015;10(8):e0135630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Centers for Disease Control and Prevention. School Health Guidelines to Promote Healthy Eating and Physical Activity. 2011;60(5):1–80. [PubMed] [Google Scholar]
- 17.Fairclough SJ, Stratton G. A review of physical activity levels during elementary school physical education. J Teach Phys Educ. 2006;25(2):240–58. [Google Scholar]
- 18.Smith MP, Berdel D, Nowak D, et al. Physical activity levels and domains assessed by accelerometry in German adolescents from GINIplus and LISA plus. PloS One. 2016;11(3):e0152217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hollis JL, Williams AJ, Sutherland R, et al. A systematic review and meta-analysis of moderate-to-vigorous physical activity levels in elementary school physical education lessons. Prev Med. 2016;86:34–54. [DOI] [PubMed] [Google Scholar]
- 20.Schlechter CR, Guagliano JM, Rosenkranz RR, et al. Physical activity patterns across time-segmented youth sport flag football practice. BMC Public Health. 2018;18(1):226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Centers for Disease Control and Prevention. Guidelines for school and community programs to promote lifelong physical activity among young people. MMWR Morb Mortal Wkly Rep. 1997;46(RR-6):1–46. [PubMed] [Google Scholar]
- 22.Guagliano JM, Rosenkranz RR, Kolt GS. Girls’ physical activity levels during organized sports in Australia. Med Sci Sports Exerc. 2013;45(1):116–22. [DOI] [PubMed] [Google Scholar]
- 23.Sprengeler O, Wirsik N, Hebestreit A, et al. Domain-specific self-reported and objectively measured physical activity in children. Int J Environ Res Public Health. 2017;14(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hänggi JM, Phillips LR, Rowlands AV. Validation of the GT3X ActiGraph in children and comparison with the GT1M ActiGraph. J Sci Med Sport. 2013;16(1):40–4. [DOI] [PubMed] [Google Scholar]
- 25.Robusto KM, Trost SG. Comparison of three generations of ActiGraph activity monitors in children and adolescents. J Sports Sci. 2012;30(13):1429–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sasaki JE, John D, Freedson PS. Validation and comparison of ActiGraph activity monitors. J Sci Med Sport. 2011;14(5):411–6. [DOI] [PubMed] [Google Scholar]
- 27.Vanhelst J, Mikulovic J, Bui-Xuan G, et al. Comparison of two ActiGraph accelerometer generations in the assessment of physical activity in free living conditions. BMC Res Notes. 2012;5:187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Guinhouya BC, Samouda H, de Beaufort C. Level of physical activity among children and adolescents in Europe: a review of physical activity assessed objectively by accelerometry. Public Health. 2013;127(4):301–11. [DOI] [PubMed] [Google Scholar]
- 29.Choi L, Liu Z, Matthews CE, et al. Validation of accelerometer wear and nonwear time classification algorithm. Med Sci Sports Exerc. 2011;43(2):357–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Evenson KR, Catellier DJ, Gill K, et al. Calibration of two objective measures of physical activity for children. J Sports Sci. 2008;26(14):1557–65. [DOI] [PubMed] [Google Scholar]
- 31.Cain KL, Sallis JF, Conway TL, Van Dyck D, Calhoon L. Using accelerometers in youth physical activity studies: a review of methods. J Phys Act Health. 2013;437–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hallal PC, Andersen LB, Bull FC, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247–57. [DOI] [PubMed] [Google Scholar]
- 33.Konstabel K, Veidebaum T, Verbestel V, et al. Objectively measured physical activity in European children: the IDEFICS study. Int J Obes (Lond). 2014;38(2 Suppl):S135–43. [DOI] [PubMed] [Google Scholar]
- 34.Telford RM, Telford RD, Cochrane T, et al. The influence of sport club participation on physical activity, fitness and body fat during childhood and adolescence: the LOOK Longitudinal Study. J Sci Med Sport. 2016;19(5):400–6. [DOI] [PubMed] [Google Scholar]
- 35.Sigmund E, Sigmundova D, Hamrik Z, et al. Does participation in physical education reduce sedentary behaviour in school and throughout the day among normal-weight and overweight-to-obese Czech children aged 9–11 years? Int J Environ Res Public Health. 2014;11(1):1076–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Carlson JA, Sallis JF, Norman GJ, et al. Elementary school practices and children’s objectively measured physical activity during school. Prev Med. 2013;57(5):591–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Racette SB, Dill TC, White ML, et al. Influence of physical education on moderate-to-vigorous physical activity of urban public school children in St. Louis, Missouri, 2011–2014. Prev Chronic Dis. 2015;12:E31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Banda JA, Haydel KF, Davila T, et al. Effects of varying epoch lengths, wear time algorithms, and activity cut-points on estimates of child sedentary behavior and physical activity from accelerometer data. PloS One. 2016;11(3):e0150534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kettner S, Kobel S, Fischbach N, et al. Objectively determined physical activity levels of primary school children in south-west Germany. BMC Public Health. 2013;13:895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Santos-Lozano A, Santin-Medeiros F, Cristi-Montero C, et al. GT1M, GT3X and ActiTrainer counts comparison during standardized activities in young, adults and older adults. Nutr Hosp. 2016;33(3):280. [DOI] [PubMed] [Google Scholar]
- 41.Lee KY, Macfarlane DJ, Cerin E. Comparison of three models of ActiGraph accelerometers during free living and controlled laboratory conditions. Eur J Sport Sci. 2013;13(3):332–9. [DOI] [PubMed] [Google Scholar]