

Abstract
Pyogenic granuloma is a non-neoplastic reactive lesion that commonly occurs in gingiva. It is rarely found in other locations such as the lips, tongue, palate and buccal mucosa. Lesions affecting the upper lip are even rarer and very few cases have been reported in the literature. In such situations, the lesion may mimic other conditions such as minor salivary gland tumours, mesenchymal tumours, and infectious lesions, which may create diagnostic difficulty. This case report describes an uncommon location of pyogenic granuloma occurring on the upper lip in a 49-year-old male patient.
Keywords: Gingival lesions, Granuloma, Pyogenic, Upper lip
Introduction
Pyogenic granuloma is a non-neoplastic reactive lesion commonly occurring in the oral cavity as a response to chronic local irritation, trauma and hormonal changes.1 Despite its name, the condition is neither associated with pus nor there is granuloma formation; hence, the term ‘pyogenic granuloma’ is a misnomer.2, 3 Several other terms have been used to describe this lesion such as telangiectatic granuloma, haemangiomatous granuloma, vascular epulis and vascular tumour. The term pregnancy tumour is also used when it occurs in pregnant women.5
Several concepts have been proposed to explain the pathogenesis of pyogenic granuloma. According to Regezi et al.,6 it is a reactive or reparative process in which a certain stimulus causes exuberant proliferation of connective tissue. Another hypothesis suggests that there is an imbalance between promoters and inhibitors of angiogenesis, and this explains why there is excessive vascular proliferation in these lesions.7
Clinically, pyogenic granuloma presents as a pedunculated or sessile growth with a smooth or lobulated surface.8 The lesion may vary from red to pink in colour depending upon the maturity of the lesion, and the surface may be ulcerated.9 The most common intra-oral site of occurrence is the gingiva, especially the maxillary anterior region. Extra-gingivally, the lesion may be found on the lower lip, tongue, palate and buccal mucosa.9 Pyogenic granuloma of the upper lip is a rare occurrence.10, 11
This article reports a case of pyogenic granuloma occurring on the upper lip, which created a diagnostic dilemma because of its unusual location.
Case report
A 49-year-old male patient presented with a chief complaint of swelling on the front upper lip region for the past 3 months. Initially the swelling was small in size, but it had gradually increased to the present size. The swelling was not associated with pain and showed occasional spontaneous bleeding. There was no history of similar lesions.
On clinical examination, a swollen area of about 0.6 × 0.8 cm was noted on the midline of the upper lip. The lesion was solitary, sessile, reddish-pink in colour with ulceration of the superficial mucosa (Figure 1). On palpation, the lesion was firm in consistency, non-tender and was not fixed to the underlying tissue. Lymph nodes were non-palpable and non-tender. Based on clinical examination, differential diagnosis of fibroma and keratoacanthoma were given. The lesion was then excised and sent for histopathological evaluation.
Figure 1.

Solitary, sessile swelling of the upper lip with ulceration of the superficial mucosa.
The histopathologic examination revealed orthokeratinized stratified squamous epithelium with areas of ulceration (Figure 2). A fibrinopurulent membrane consisting of neutrophils and extravasated RBCs was noted in the ulcerated areas. Numerous endothelium-lined blood vessels engorged with RBCs and budding capillaries were noted in the underlying stroma (Figure 3, Figure 4). Dense chronic inflammatory cell infiltration consisting chiefly of lymphocytes and plasma cells was also noted. Based on these histopathological findings, the diagnosis of pyogenic granuloma was confirmed.
Figure 2.

Low-power view showing orthokeratinized stratified squamous epithelium with highly vascular stroma (haematoxylin and eosin (H&E), 100 ×).
Figure 3.
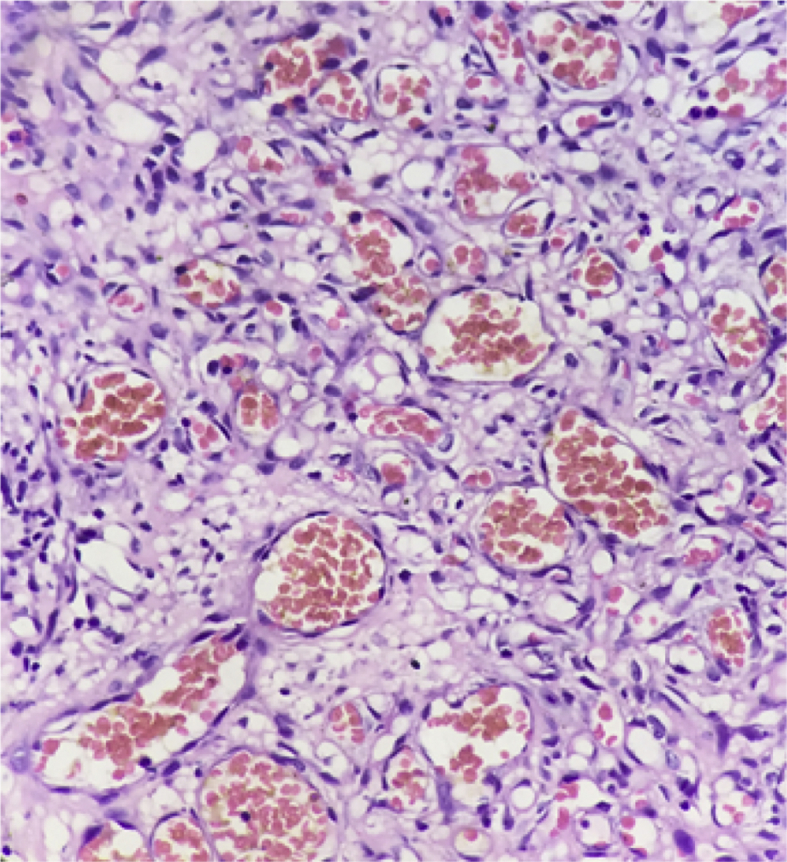
High-power view showing endothelial cell lined blood vessels engorged with red blood cells (H&E, 400 ×)
Figure 4.
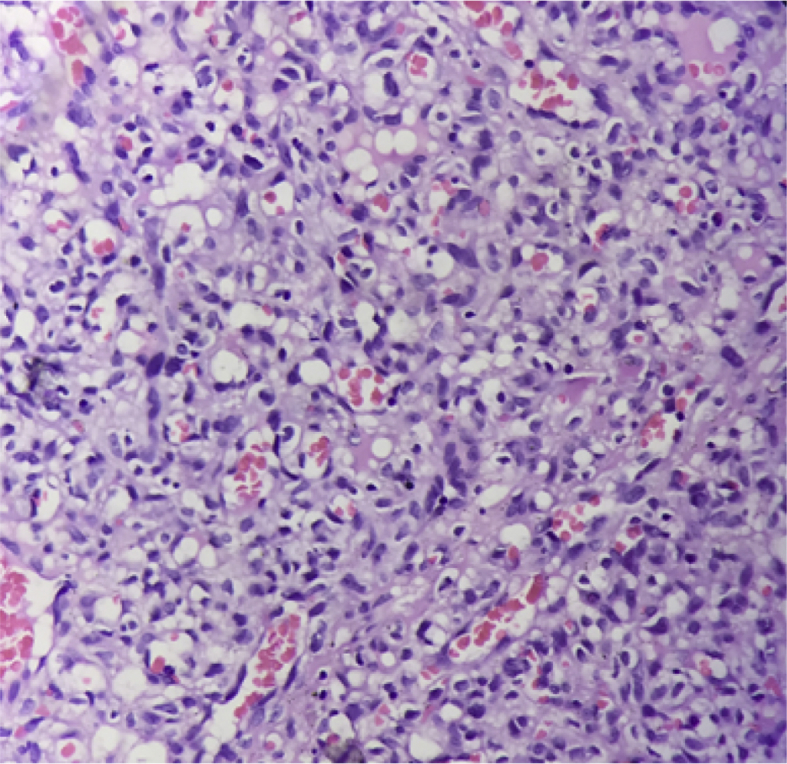
High-power view showing numerous budding capillaries (H&E, 400 ×).
Discussion
Pyogenic granuloma is a relatively common lesion of the oral mucosa, first described by Poncet and Dor as “human botryomycosis”. Later, it was proposed that the lesion is caused by pyogenic bacteria such as streptococci and staphylococci; hence, the lesion was given the name ‘pyogenic granuloma’. Currently, this terminology is considered to be a misnomer.2 These are in fact, non-neoplastic reactive lesions occurring in response to chronic local irritation or trauma.4 In the present case, there was a negative history of trauma. However, the oral hygiene status was poor and the lips were dry, which could be causative factors for the lesion.
Pyogenic granuloma is commonly found in keratinized mucosa such as the gingiva, a site which is frequently subjected to trauma and chronic irritation.4 Occurrence of this lesion on the upper lip as seen in our case is very rare in contrast to the lower lip, where this lesion is relatively common. In a 15-year retrospective study of benign lip lesions conducted by Arslan et al., only 10% of lesions were located on the upper lip. This highlights the fact that the upper lip is a relatively uncommon location for benign lesions, including pyogenic granuloma.12 Thus, we aimed to report this case of pyogenic granuloma of the upper lip, an common lesion in an uncommon location.
Lesions of the upper lip usually present a diagnostic challenge as there is a propensity for minor salivary gland tumours in that location, such as pleomorphic adenoma, canalicular adenoma and mucoepidermoid carcinoma. Other differential diagnoses include mesenchymal tumour (such as lipoma, leiomyoma, nerve tumours, benign fibrous histiocytoma, oral focal mucinosis and granular cell tumour) and infectious lesions (such as periapical abscess, tuberculosis, syphilitic gumma and deep fungal infections).13 Parajuli and Maharjan described a case of pyogenic granuloma of the upper lip which posed a diagnostic challenge; final diagnosis was established only after biopsy.5
In the current case, the presentation was indicative of keratoacanthoma because of its location, crusted appearance and occasional tendency to bleed. However, it is always beneficial to evaluate a lesion histopathologically to determine the prognosis of the patient.
Microscopically, pyogenic granuloma shows an atrophic or hyperplastic epithelium that may be ulcerated in places. The underlying connective tissue stroma consists of numerous endothelium-lined vascular spaces, proliferation of fibroblasts and budding endothelial cells.14 In addition to these features, the presence of mixed inflammatory cell infiltration may also be noted.3 The histopathological features seen in our case were in accordance with these features; hence, a final diagnosis of pyogenic granuloma was given.
The treatment of choice for pyogenic granuloma is usually surgical excision. Other treatment modalities that have been used include cryosurgery, sclerotherapy, electrocautery, and radiosurgery among others.15 Some studies report using intralesional corticosteroid injection for treatment of recurrent cases.9 The recurrence rate of pyogenic granuloma is 15%, which is attributed to incomplete excision of the lesion and failure to remove the etiologic factors.16 Frumkin et al. suggested a conservative non-surgical protocol to prevent recurrence, which includes removal of irritating factors with debridement under local anaesthesia along with adjunctive measures, such as chlorhexidine mouthwash and strict oral hygiene instructions. Those authors also suggested a follow-up protocol which includes repeated visits to the clinic every 2 weeks for the first 2 months followed by maintenance visits once every 2 months.3 However recurrence is uncommon in extra-gingival locations following surgical excision.16
Conclusion
Pyogenic granuloma is a common lesion occurring in the oral cavity. Our article highlights a rare location of pyogenic granuloma. Although these lesions can be diagnosed clinically, unusual locations may sometimes create difficulty in diagnosis. Thus, through this case report, we wish to emphasize the fact that the diagnosis of oral lesions is intricate. Detailed clinical examination followed by histopathological evaluation is always the gold standard.
Conflict of interest
The authors have no conflict of interest to declare.
Ethical approval
Not applicable.
Consent
Informed consent was obtained from the above-described patient regarding use of any clinical, radiographical and other diagnostic and histopathological data or photographs for academic or publication purposes.
Authors' contributions
PP prepared the manuscript, NC performed the surgery and VM and RS critically reviewed the manuscript. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Footnotes
Peer review under responsibility of Taibah University.
References
- 1.Pandey R., Gupta R., Rawat S. Pyogenic granuloma of buccal mucosa mimicking as traumatic fibroma in pregnancy. Indian J Dent Adv. 2016;8(3):172–175. [Google Scholar]
- 2.Asha V., Dhanya M., Patil B.A., Revanna G. An unusual presentation of pyogenic granuloma of the lower lip. Contemp Clin Dent. 2014;5(4):524–526. doi: 10.4103/0976-237X.142823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Frumkin N., Nashef R., Shapira L., Wilensky A. Nonsurgical treatment of recurrent gingival pyogenic granuloma : a case report. Quintessence Int. 2015;46(6):539–544. doi: 10.3290/j.qi.a33992. [DOI] [PubMed] [Google Scholar]
- 4.Nalin A.S., George S., Kunjumon R.M., Raj P.R., George G.B. Extra gingival pyogenic Granuloma : unusual location for the usual lesion. IJSS case reports Rev. 2015;2(4):19–21. [Google Scholar]
- 5.Parajuli R., Maharjan S. Unusual presentation of oral pyogenic granulomas: a review of two cases. Clin Case Reports. 2018;6(4):690–693. doi: 10.1002/ccr3.1435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mastammanavar D., Hu asgi S., Koneru A., Vanishree M., Surekha R., Vardendra M. Aggressive pyogenic granuloma: a case report. Int J Oral Maxillofac Pathol. 2014;5(2):29–32. [Google Scholar]
- 7.Gowda D., Owens C. Pyogenic granuloma in an unusual site. Glob Pediatr Heal. 2017;4 doi: 10.1177/2333794X17704607. 2333794X17704607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brunet-llobet L., Miranda-rius J., Lahor-soler E., Mrina O. A gray-purple mass on the floor of the Mouth : gigantic mucogingival pyogenic granuloma in a teenage patient. Open Dent J. 2014;8:125–128. doi: 10.2174/1874210601408010125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sachdeva S.K. Extragingival pyogenic granuloma: an unusual clinical presentation. J Dent Shiraz Univ Med Sci. 2015;16(3 Suppl):282–285. [PMC free article] [PubMed] [Google Scholar]
- 10.Mulinari-Santos G., Garcia B.T., de Assis Taveira L.A. Pyogenic granuloma on the upper Lip : a rare location. J Craniofac Surg. 2017;28(2):577–578. doi: 10.1097/SCS.0000000000003249. [DOI] [PubMed] [Google Scholar]
- 11.Al-shiaty R.A., Ottoman B.A.E. Recurrent pyogenic granuloma : an update. Int J Sci Reports. 2015;1(1):22–31. [Google Scholar]
- 12.Ural A. A 15-year retrospective study of 160 cases of benign lip lesions. J Laryngol Otol. 2015;129:1224–1227. doi: 10.1017/S0022215115002923. [DOI] [PubMed] [Google Scholar]
- 13.Bhandarkar G.P., Shetty K.V. Differential diagnoses of elevated lesions of the upper lip: an overview. J Canc Res Therapeut. 2017;13(2):170–174. doi: 10.4103/0973-1482.204890. [DOI] [PubMed] [Google Scholar]
- 14.Nagarajappa A., Chandrashekar K., Jain N., Pandya D., Kaushal T. Extragingival pyogenic granuloma: report of an unusual case with review of literature. Int J Med Appl Sci. 2016;5(2):46–52. [Google Scholar]
- 15.Wollina U., Langner D., França K., Gianfaldoni S., Lotti T., Tchernev G. Pyogenic granuloma – a common benign vascular tumor with variable clinical Presentation : new findings and treatment options. Macedonian J Med Sci. 2017;5(4):423–426. doi: 10.3889/oamjms.2017.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ghalayani P., Hajisadeghi S., Babadi F. Extragingival pyogenic granuloma associated with medication: report of an unusual case. Dent Res J. 2014;11(3):400–404. [PMC free article] [PubMed] [Google Scholar]