

Setting and Problem
There is growing interest in international rotations and a need for American surgeons to be prepared to provide humanitarian care in low- and middle-income countries. The Loma Linda University Health (LLUH) global surgery rotation at Malamulo Adventist Hospital (MAH) in Malawi is a novel, sustainable, and collaborative program that benefits both the host nation and LLUH. In 2011, the Accreditation Council for Graduate Medical Education (ACGME), the Review Committee for Surgery, and the American Board of Surgery approved ACGME-accredited surgery residencies to offer a global surgery rotation (GSR).1 In June 2012, the LLUH surgery residency received approval for an 8-week GSR during postgraduate year 4, with MAH serving as a participating nonintegrated site.
Intervention
LLUH and MAH leadership created a comprehensive manual for the GSR, including pre-trip orientation, checklists, logistics, code of conduct, dress code, language basics, and cultural expectations. To limit the use of local resources, LLUH residents bring their own surgical gloves, caps, and masks. Residents participate in pre- and post-rotation interviews with a point person based at LLUH and the international rotation director.
Since 2014, MAH has hosted an accredited Pan African Academy of Christian Surgeons (PAACS) residency that trains African physicians as surgeons, and the LLUH residents scrub in with these trainees. This allows LLUH residents to teach-assist junior PAACS residents for cases such as inguinal herniorrhaphy and endoscopy, and enables senior PAACS residents to teach-assist LLUH residents through more complex cases such as cesarean section and open prostatectomy. The LLUH residents also have helped improve residency structure, lectures, rounds, and skills transfer for the African surgery program.
Program costs include residents' travel and travel insurance, visas, room and board, and medical licenses for Malawi, supported from LLUH institutional funds and donations. Important to the success of any GSR is having an engaged rotation director at the international site, who is a champion of the GSR with the authority to initiate changes, and a consistent point person at the US site.
Outcomes to Date
Since 2012, LLUH residents have filled 74% of the available slots, and 88% of residents agreed or strongly agreed the GSR was one of their favorite rotations.2 For the past 6 years, nearly all medical student applicants have asked about the GSR, and we believe students applying to LLUH for surgery and the program's ranking in students' lists have improved since we initiated the GSR.
The consistent presence of LLUH residents allows MAH to rely on their clinical contributions, and the residents are integrated into the PAACS resident call schedule and didactic sessions. The MAH surgical team and hospital staff have become accustomed to the LLUH residents, and they understand their capabilities and how to relate to them.
LLUH's GSR was designed to ensure residents are prepared for the international rotation, which immerses them in a low-resource surgical department where surgeons perform obstetric, gynecologic, urologic, and other surgical specialty procedures. Through this broad case experience, the GSR has exposed the LLUH residents to the demands of global humanitarian practice, and has better prepared them for common global surgery cases.3 With an average of 90 major cases in the 2-month rotation, the GSR has improved LLUH residents' surgical training. The Figure shows the growth in surgical volume at MAH. The positive experience with the LLUH residents influenced the institution to establish the PAACS residency, and the added training mission has transformed this rural mission hospital.4 The GSR also changed the function of the MAH surgical department and improved the hospital's financial position. The lives and perspectives of the LLUH residents also have been positively influenced through their experience at MAH, and the LLUH and PAACS residents have developed close and lasting friendships. This link between the surgeons from 2 continents will further the growth of global surgery for a generation.
Figure.
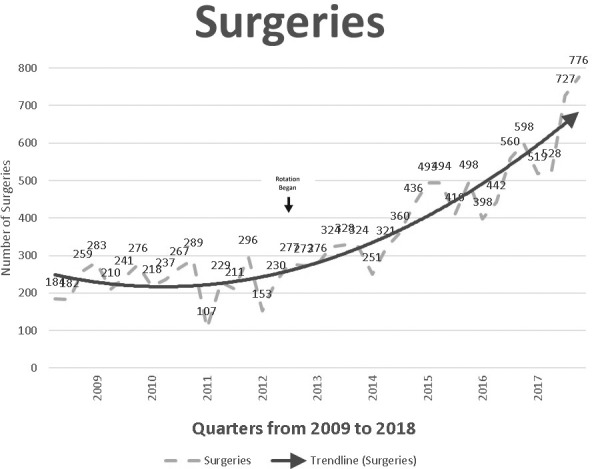
Quarterly Number of Surgical Cases at Malamulo Adventist Hospital From Medical Statistics and Data (2009–2018)
Our 6-year experience shows a well-designed global rotation is feasible and sustainable. Our innovative GSR could be replicated in other programs, with benefits for US residency programs and the international site.
References
- 1.Mitchell KB, Tarpley MJ, Tarpley JL, Casey KM. Elective global surgery rotations for residents: a call for cooperation and consortium. World J Surg. 2011;35(12):2617–2624. doi: 10.1007/s00268-011-1311-4. [DOI] [PubMed] [Google Scholar]
- 2.Teferi AN, Hayton RA, Fekadu A, Graybill CK, Donley DK, O'Neill LR, et al. Global surgery training: a prototype for a core international surgery residency rotation. JACS. 2018;227(4S2):151. [Google Scholar]
- 3.Donley DK, Graybill CK, Fekadu A, Hayton RA. Loma Linda global surgery elective: first 1000 cases. J Surg Educ. 2017;74(6):934–938. doi: 10.1016/j.jsurg.2017.04.005. [DOI] [PubMed] [Google Scholar]
- 4.Hayton RA, Kamwiyo M, Mabuku S, Reeves ME, Steffes BC. Starting a general surgery residency transformed a rural mission hospital. Int J Surg. In press.