

Abstract
Patient: Female, 64
Final Diagnosis: Coronary artery disease
Symptoms: Chest discomfort • dyspnea
Medication: —
Clinical Procedure: Percutaneous coronary intervention
Specialty: Cardiology
Objective:
Rare disease
Background:
Despite improvements in percutaneous coronary intervention (PCI) devices and operator expertise, coronary chronic total occlusion (CTO) poses a management dilemma for interventional cardiologists. Occasionally, in CTO lesions and in bifurcation lesions with severe curvature and stenosis, wires cannot be introduced into the main artery, although wiring into the side branch is possible. We herein report a case of stumpless ostial left anterior descending artery (LAD) CTO that was successfully treated with a novel strategy.
Case Report:
A 64-year-old female with symptoms of heart failure was admitted to our hospital. Coronary angiography showed CTO of the stumpless ostial LAD. The patient had invisible and continuous collaterals; therefore, we used the antegrade approach for CTO access. However, the wire could be guided only in the direction of the diagonal branch due to a severe angulation at the CTO exit site, despite successful wire crossing into the CTO lesion. We attempted intravascular ultrasound-guided direct wire entry technique to obtain additional information about the occlusion cap location and to assist in negotiating the wire into the true lumen. The guide-wire (Conquest pro) could cross the lesion after several approaches and successfully advance the device over the wire through the occluded segment after the modified See-saw wiring technique was employed.
Conclusions:
This method appears to be a promising novel strategy for difficult and complex lesions when performing CTO revascularization.
MeSH Keywords: Case Reports, Coronary Artery Disease, Percutaneous Coronary Intervention
Background
Despite considerable advances in percutaneous coronary intervention (PCI) devices and operator expertise, coronary chronic total occlusion (CTO) is difficult to manage and poses problems for interventional cardiologists. Compared to all the other CTOs, stumpless ostial left anterior descending artery (LAD) CTO rarely allows antegrade embarking of a procedure, even with microcatheter support and the stiffest guidewire. In such cases, ordinary techniques are initially used to introduce a wire into the main artery with a multifunctional catheter. However, those techniques may be ineffective depending on the bifurcation angle and CTO lesions type.
We herein report a case of stumpless ostial LAD CTO that was successfully treated with the modified See-saw wiring technique antegradely.
Case Report
In March 2018, a 64-year-old female with a history of hyper-tension, type 2 diabetes mellitus, chronic kidney disease, coronary artery disease, ischemic heart disease, and acute coronary syndrome presented with heart failure since several months. On arrival, she had class IV congestive heart failure according to the New York Heart Association criteria. A surface electrocardiogram showed normal sinus rhythm with left atrial enlargement, left ventricular hypertrophy, and secondary repolarization abnormality. A subsequent plain chest radiograph showed a tortuous thoracic aorta and pulmonary congestion. Initial laboratory data such as biochemistry, electrolytes, and blood cell count revealed no significant findings except pro-BNP of 15 000 pg/mL, C-reactive protein of 1.25 mg/dL, creatinine of 10.99 mg/dL, estimated glomerular filtration rate of 3.51 mL/min/1.73 m2, and troponin I of 0.197 ng/mL. A 2-dimensional transthoracic echocardiogram demonstrated impaired left ventricle contractility with regional wall motion abnormality.
After the heart failure improved with treatment, cardiac catheterization was performed to identify the cause of heart failure. The target lesion was the CTO in the ostium left anterior descending artery (Figure 1). The patient had ambiguous and continuous collaterals (Video 1); therefore, we adopted the ante-grade approach for CTO access. A retrograde diagnostic catheter, transradial approach, of the AL1.0 SH, 5Fr, (Cordis Corporation) was used for dual injection. Via the patient’s right femoral artery with an 8F introducer sheath (Cordis Corporation), a 7F EBU SH (Cordis Corporation) was smoothly engaged to the left coronary artery. Several types of guidewires are usually employed to recanalize the occluded vessel during this procedure: Sion blue, Fielder XT-R, Ultimate bros 3, Gaia series, and Conquest pro (Asahi Intecc).
Figure 1.
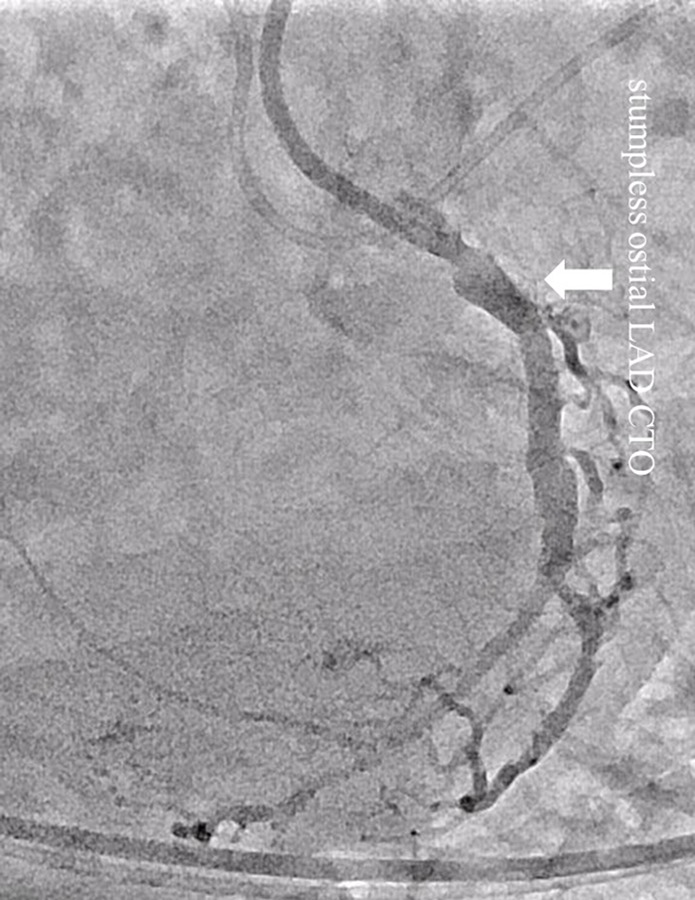
Spider view showing the stumpless ostial left anterior descending artery chronic total occlusion.
Video 1.

Bilateral concurrent contrast injection with ambiguous and continuous collaterals.
Just before the CTO, a Sion blue wire was inserted into the left circumflex and wiring using a Fielder XT-R wire was started with support of a Crusade (Kaneka Corporation). We carefully inserted the wire into the CTO and gradually advanced it through the lesion. However, due to a severe angulation at the CTO exit site, we could guide the wire only in the direction of the diagonal branch. This occurred despite successful wire crossing of the CTO lesion. We also attempted using the intravascular ultrasound-guided (Eagle Eye Platinum) direct wire entry technique to provide added information regarding the occlusion cap location and assist in negotiating the wire into the true lumen (Figure 2, Video 2).
Figure 2.

Intravascular ultrasound guiding the guidewire to enter the chronic total occlusion entry point.
Video 2.

Surveying of the true lumen with intravascular ultrasound.
Finally, after several attempts, the guidewire Conquest pro engaged and crossed the lesion (Figure 3A–3D, Videos 3, 4). We could successfully advance the device over the wire through the occluded segment (Figure 4) after using a novel strategy, the modified See-saw wiring technique and landmark technique, which involved the use of a single-lumen microcatheter (Finecross 130 cm), a dual-lumen microcatheter (Crusade), and triple wires. Predilatation was performed with 1.0-mm, 1.25-mm, 1.5-mm, and 2.5-mm balloons, after which the stents (Desyne 4.0×18 mm, Desyne 3.5×23 mm, and Orsiro 2.75×22 mm) were deployed at the lesion site to fully cover the lesion. After the absence of flow disturbance or other complications associated with this advanced procedure were confirmed, the strategies and management were deemed successful (Figure 5, Video 5).
Figure 3.

Several attempts using the guidewire (A, B). Conducting the modified See-saw wiring technique and landmark technique using a single-lumen microcatheter Finecross 130 cm, dual-lumen microcatheter Crusade, and triple wires (C, D).
Video 3.

Modified see-saw wiring technique and and landmark technique.
Video 4.

Conquest pro engaged and crossed the lesion.
Figure 4.

Using a Conquest pro wire supported by a Finecross catheter to cross the left anterior descending artery chronic total occlusion predilatation with 1.0-mm, 1.25-mm, 1.5-mm, and 2.5-mm balloon.
Figure 5.

Post stenting of the proximal left anterior descending artery.
Video 5.

Successful recanalization of LAD CTO.
Discussion
The treatment of CTO has been a limitation of percutaneous revascularization compared to treatment for less severe stenosis, and is associated with unpredictable success and excessive restenosis rates. Over the past decade, enormous improvement in PCI facilities and techniques such as the retrograde approach, as well as development of new strategies have enabled us to treat with success even complex CTO [1]. However, due to the differences in plaque accumulation and the position of the oscillatory shearing forces at the left main bifurcation, stumpless ostial LAD CTO is an extremely specific location; interventional cardiologists therefore tend to avoid it if possible [2].
The advantageous anatomic features of the CTO will increase the possibility of PCI success and reduce the risk of complications. One of the important factors that increases the likelihood of CTO PCI success is the use of a dual coronary injection approach [3,4]. Bilateral catheterization with concurrent contrast injection will allow visualization of occluded distal segment of target vessel via collateral flow. The overall aim is to connect antegrade and retrograde channels to allow successful CTO PCI. However, the retrograde technique was unavailable, while the basic technique of the antegrade approach played an important role in PCI for CTO lesions in this case.
It is important to assess lesion factors and patient-related factors before deciding to perform a CTO PCI. The J-CTO registry reported that using J-CTO scores enabled physicians to predict the successful guidewire crossing in CTO antegradely within 30 minutes [5]. According to the J-CTO score, the factors that decrease the likelihood of successful PCI in such cases are 1) blunt stump, making it difficult for the guidewire to find an entry point through the proximal cap; 2) calcification, with a lesion that is hard and not easily penetrable; 3) severe curvature within the lesion, often >45°: and 4) length of occluded lesion greater than 20 mm long lesions. The JCTO score only contains the 5 most important factors (calcification, lesion length, stump morphology, bending angle, and re-do), which cannot entirely represent the lesion-related difficulty, especially in specific coronary artery sites. Preferential entry of the guidewire into a side branch where the occlusion is flush with the origin of the side branch and long-standing occlusion can also count as a specific characteristic and obstacle to ostial LAD CTO [6].
Without accessible retrograde collaterals, successful antegrade recanalization rate of stumpless ostial LAD CTO lesion is extremely low. Intravascular ultrasound may be effective to guide the guidewire into the CTO entry point. We introduced the intravascular ultrasound catheter into the LCX lumen to identify the true entry point of the LAD ostium, and guided stiff wire to enter the true lumen with the adjacent side-branch wire as markers. Nevertheless, we could not conduct this strategy successfully due to severe curvature and stenosis. Aside from surveying of the true lumen, intravascular ultrasound guidance in DES (Data Encryption Standard) implantation is associated with a significant reduction in MACE (major adverse cardiac event) risk in patients with complex lesions, particularly those with CTO lesions [7–9].
Parallel-wire technique, the cornerstone technique in CTO PCI, was first described by Reifart in 1995 and was further developed by Katoh [10]. See-saw wiring technique is a variation of the parallel wire technique. Here, both wires are supported by angioplasty catheters and are alternatively used to probe the occlusion to find the true lumen. Sometimes, three or more wires are used to identify the true lumen.
Multifunctional dual-lumen microcatheters, such as the Crusade catheter (Kaneka Corporation), contain both a monorail and an OTW port and are preferably suited to parallel wiring by allowing the introduction of multiple wires without removal of the catheter from an optimal position. Using initial wires serves as a marker occludes the wrong pathway and can potentially modify the anatomy by changing vessel geometry and smoothening sharp curves. A stiffer third guidewire, for instance Conquest Pro, is manipulated along with another single-lumen microcatheter support, an attempt to enter the true lumen of stumpless ostial LAD CTO by puncturing the proximal cap [11–13]. This novel strategy, called the modified Seesaw wiring technique, could be used effectively and safely in CTO PCI, especially for a CTO with the morphology of a calcified and unknown ostium.
Conclusions
When approaching stumpless ostial LAD CTO lesion, cardiovascular interventionists must realize that the maximum difficulty in performing PCI is in the antegrade entry of the guidewire. Combined application of multiple antegrade techniques and the latest devices may provide an effective and safe approach for complex CTO PCI cases, where a retrograde approach is not feasible. Experience with the techniques and equipment of PCI CTO are essential for high success rates.
Acknowledgments
I would like to thank Dr. Lin Shen-Chang, the corresponding author, for his invaluable editorial assistance. I appreciate the expert comments by the reviewers and editors and the contacts they shared.
Footnotes
Conflict of interest
None.
References:
- 1.Touma G, Ramsay D, Weaver J. Chronic total occlusions: Current techniques and future directions. Int J Cardiol Heart Vasc. 2015;7:28–39. doi: 10.1016/j.ijcha.2015.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kimura BJ, Russo RJ, Bhargava V, et al. Atheroma morphology and distribution in proximal left anterior descending coronary artery: In vivo observations. J Am Coll Cardiol. 1996;27:825–31. doi: 10.1016/0735-1097(95)00551-x. [DOI] [PubMed] [Google Scholar]
- 3.Ramanath VS, Thompson CA. Coronary chronic total occlusion recanalisation – current techniques and approaches. Interv Cardiol. 2013;8:41–45. doi: 10.15420/icr.2013.8.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Galassi A, Grantham A, Kandzari D, et al. Percutaneous treatment of coronary chronic total occlusion part 2: Technical approach. Interv Cardiol. 2014;9:201–7. doi: 10.15420/icr.2014.9.3.201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4:213–21. doi: 10.1016/j.jcin.2010.09.024. [DOI] [PubMed] [Google Scholar]
- 6.Rinfret S, Joyal D, Spratt JC, Buller CE. Chronic total occlusion percutaneous coronary intervention case selection and techniques for the antegrade-only operator. Catheter Cardiovasc Interv. 2015;85:408–15. doi: 10.1002/ccd.25611. [DOI] [PubMed] [Google Scholar]
- 7.Huang WC, Teng HI, Hsueh CH, et al. Intravascular ultrasound guided wiring re-entry technique for complex chronic total occlusions. J Interv Cardiol. 2018;31:572–79. doi: 10.1111/joic.12518. [DOI] [PubMed] [Google Scholar]
- 8.Moriuchi M, Saito S, Honye J, et al. [Role of intravascular ultrasound imaging for assessing pathophysiology of coronary artery disease] J Cardiol. 2000;35(Suppl. 1):51–55. [in Japanese] [PubMed] [Google Scholar]
- 9.Kadohira T, Kobayashi Y. Intravascular ultrasound-guided drug-eluting stent implantation. Cardiovasc Interv Ther. 2017;32:1–11. doi: 10.1007/s12928-016-0438-5. [DOI] [PubMed] [Google Scholar]
- 10.Sianos G, Werner GS, Galassi AR, et al. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention. 2012;8:139–45. doi: 10.4244/EIJV8I1A21. [DOI] [PubMed] [Google Scholar]
- 11.Cuneo A, Tebbe U. The management of chronic total coronary occlusions. Minerva Cardioangiol. 2008;56:527–41. [PubMed] [Google Scholar]
- 12.Mitsudo K, Yamashita T, Asakura Y, et al. Recanalization strategy for chronic total occlusions with tapered and stiff-tip guidewire. The results of CTO new techniQUE for STandard procedure (CONQUEST) trial. J Invasive Cardiol. 2008;20:571–77. [PubMed] [Google Scholar]
- 13.Xue J, Li J, Wang H, et al. “Seesaw balloon-wire cutting” technique is superior to Tornus catheter in balloon uncrossable chronic total occlusions. Int J Cardiol. 2017;228:523–27. doi: 10.1016/j.ijcard.2016.10.107. [DOI] [PubMed] [Google Scholar]