

Abstract
Background
Studies in high-income countries have reported associations between oral health and diabetes. There is however a lack of evidence on this association from low and middle-income countries, especially India. The current study aimed to assess the prevalence of common oral diseases and their association with diabetes.
Methods
This cross-sectional study was nested within the second Cardiometabolic Risk Reduction in South Asia Surveillance Study. A subset of study participants residing in Delhi were administered the World Health Organization’s Oral Health Assessment Questionnaire and underwent oral examination for caries experience and periodontal health assessment using standard indices. Diabetes status was ascertained by fasting blood glucose, glycosylated hemoglobin values or self-reported medication use. Information was captured on co-variates of interest. The association between oral health and diabetes was investigated using Multivariable Zero-Inflated Poisson (ZIP) regression analysis.
Results
Out of 2045 participants, 47% were women and the mean age of study participants was 42.17 (12.8) years. The age-standardised prevalence (95% confidence interval) estimates were 78.9% (75.6–81.7) for dental caries, 35.9% (32.3–39.6) for periodontitis. Nearly 85% participants suffered from at least one oral disease. Compared to diabetes-free counterparts, participants with diabetes had more severe caries experience [Mean Count Ratio (MCR) = 1.07 (1.03–1.12)] and attachment loss [MCR = 1.10 (1.04–1.17)]. Also, the adjusted prevalence of periodontitis was significantly higher among participants with diabetes [42.3%(40.0–45.0)] compared to those without diabetes [31.3%(30.3–32.2)].
Conclusion
We found that eight out of ten participants in urban Delhi suffered from some form of oral disease and participants with diabetes had worse oral health. This highlights the need for public health strategies to integrate oral health within the existing Non-Communicable Disease control programs.
Electronic supplementary material
The online version of this article (10.1186/s12903-019-0884-4) contains supplementary material, which is available to authorized users.
Keywords: Dental caries, Periodontitis, Diabetes, Non-communicable diseases, Low- and middle-income countries
Background
Oral conditions are known to affect almost half of the world’s population. Dental decay alone affects nearly 2.5 billion people, making it the most prevalent condition worldwide [1]. More than 7% of the world population suffers from severe chronic periodontitis [1]. More Indians suffer from caries and periodontitis than their South Asian counterparts [2]. A recent survey reports prevalence of caries and periodontitis among rural Indian adults was nearly 65% for both conditions [3]. It has been estimated that the total health loss associated with oral conditions is comparable to that for hypertensive heart disease, schizophrenia, and all maternal conditions combined [1]. Besides, India has the maximum number of adults with diabetes in the South-East Asian Region (72.9 million) with the numbers expected to rise to 134 million in 2045 [4].
Epidemiological studies indicate that there are several oral manifestations of diabetes such as periodontitis, dry mouth, root caries, candidiasis [5]. There are pathways linking diabetes with oral diseases, especially periodontitis, which is often referred to as the sixth complication of diabetes [6]. One of the first studies to conclude an association between periodontitis and diabetes was conducted among Pima Indians [7]. The risk of periodontitis was threefold among those with diabetes when compared to those without.
Oral health problems are associated with pain, compromised mastication, xerostomia that profoundly affect overall quality of life, loss of work hours and are often expensive to treat [8, 9]. Despite this, oral health remains an under-recognized and neglected global health issue. Given the burden of oral diseases and their association with diabetes, there is a strong pathophysiological basis for addressing oral health problems within general healthcare practice [10, 11]. Such a comprehensive approach may be particularly useful in Low and Middle-Income Countries (LMICs) for judicious use of resources and reducing the associated expenditure. Despite these considerations, the national Non-Communicable Disease (NCD) programs in most LMICs do not encompass oral health, and data on the co-occurrence of oral diseases with NCDs are scant. To address this knowledge gap, we planned to assess the prevalence of oral diseases and their association with diabetes in a subset of participants enrolled in a population-based cohort in India.
Methods
Study participants
The Cardio-metabolic Risk Reduction in South Asia (CARRS) Study Cohort 2 is a population-based study conducted in Chennai and New Delhi, India and in Karachi, Pakistan. The CARRS Oral Health sub-study was nested within the baseline assessment of the Delhi site (2014). A representative sample of adults ≥20 years of age was identified using multistage cluster sampling. This scheme follows the protocol of an earlier study (CARRS − 1), described elsewhere [12]. The primary sampling unit in Delhi were the municipal wards, from which, census enumeration blocks (five per ward) and households (n = 25 per block) were randomly selected in that order. Two participants were approached from each household to participate. A subset of CARRS participants was randomly selected for this sub-study and written informed consent was obtained.
The minimum sample size (n = 1965) required for the sub-study was calculated using prevalence estimates of periodontitis from a previous community based study with 5% absolute error [13]. However, more participants were recruited to account for any possible missing information on diabetes status. Figure 1 outlines the recruitment flowchart for this study.
Fig. 1.

Participant recruitment flowchart
Ethical approval was obtained from the Institutional Review Board of Public Health Foundation of India, New Delhi.
Study procedures
Oral health assessment
Oral health was assessed through a combination of interviewer-administered questionnaire and clinical examination performed by qualified dentists assisted by trained field personnel at neighborhood locations accessible to the participants. Five dentists attended a three-day training in study methods. Calibration sessions included interpretation of scores from Decayed, Missing, Filled Tooth (DMFT) and Loss of Attachment (LOA) Indices, the average intraclass correlation and kappa statistic were 0.97 (0.94–0.99) and 0.71 (0.58–0.83) respectively. Data was collected using a tablet and took 25–30 min per participant. The application was developed using an open-source software, open data kit, with appropriate logic and range checks that enabled real time transfer [14].
World Health Organization’s Oral Health Assessment Questionnaire was used to capture information on oral hygiene practices, self-reported oral health problems, and service utilisation [15].
The examination began with evaluation and palpation of extraoral features for ulcers, erosion or fissures on face, neck, commissures and vermilion border or enlarged lymph nodes.
For intraoral examination, both hard and soft tissues were examined, measures outlined in Table 1. The oral cavity was divided into four quadrants; maxillary (upper) right-left and mandibular (lower) left-right, examined in that order from anterior to posterior direction. The overall caries experience was recorded using the standardised DMFT index and prevalence of dental caries was assessed using the Decayed component of the index. Gingival and periodontal health was assessed using Community Periodontal Index (CPI) Loss of Attachment (LOA) index. Unlike DMFT, periodontal examination was done by assessment of six index teeth (representative teeth from each sextant: right-left maxillary/mandibular posterior and maxillary/mandibular anterior). Both, CPI and LOA were used for assessment of gingival and periodontal health. Prevalence of periodontitis was measured according to the U.S. Centres for Disease Control and Prevention and the American Academy of Periodontology [16].
Table 1.
Clinical assessment measures of oral health status
| Examination | Purpose and Index | Instrument Used |
|---|---|---|
| EXTRAORAL ASSESSMENT | Assessment of extraoral abnormalities | Visual examination and palpation |
| INTRAORAL ASSESSMENT | Assessment of both, hard and soft tissues | |
| Dentition | Assessment of teeth | |
| Caries experience |
Tooth decay, loss and restoration DMFT Index |
Mouth mirror, curved double ended probe |
| Fluorosis |
Fluorosis Dean’s index |
|
| Traumatic dental injuries | Trauma | |
| Soft tissue | Assessment of tooth supporting structure and oral mucosa | |
| Gingivitis |
Status of gingiva CPI Index |
Mouth mirror, WHO CPI Probe |
| Periodontitis |
Status of periodontium and attachment loss LOA Index |
|
| Oral mucosal lesions | Pre-malignant, malignant and other conditions of the mucosa | Visual examination and palpation |
DMFT Decayed Missing Filled Teeth
LOA Loss of attachment Index
WHO World Health Organisation
Socio-demographic factors
The covariates considered were based on evidence of their role in the association between diabetes and oral health outcomes. Data for these were obtained from CARRS-2 cohort [12]. Age was categorized as 20–39, 40–59 and ≥ 60 years. With respect to monthly household income [in Indian Rupee (INR)], the study population was divided into four groups; < 10,000, 10,001–20,000, 20,001–30,000, and ≥ 30,001. Education status was classified as primary school or less, high school, secondary to intermediary school, or graduate degree and above. The summary household asset index variable was developed based on the principal component analysis, took into consideration type of kitchen, drinking water source, type of toilet facility, and ownership of a refrigerator, washing machine, microwave, grinder, digital video disc player, computer, car, motorcycle and bicycle. For the purposes of the current analysis, the distribution of the household asset index was divided into tertiles (low, medium, high).
Diabetes and modifiable risk factors
Diabetes was defined as: measured fasting plasma glucose ≥126 mg/dl and/or HbA1c ≥6.5% or receipt of anti-diabetes medications [17]. Participants were interviewed about ‘ever-use’ of tobacco (both smoking and smokeless forms) and alcohol. Dietary habits were ascertained using a food frequency questionnaire, adapted from the INTERHEART study, administered to obtain information on usual intake of fruits, desserts and sugary beverages (each expressed as daily/weekly, monthly, never/less than once a month) [12, 18]. Body Mass Index (BMI) was calculated from the measured values of weight and height and classified as underweight (< 18.5 kg/m2), normal (18.5 to 24.9 kg/m2), overweight (25.0 to 29.9 kg/m2) or obese (≥30.0 kg/m2).
Statistical methods
Participant characteristics were presented as means and standard deviations (SD) for continuous variables and as percentages for categorical variables. The two main outcome variables for measuring oral health status were DMFT for caries experience and LOA scores for attachment loss (both count variables). Many participants had zero observations for these scores therefore Zero-Inflated Poisson (ZIP) regression was used. ZIP regression generates two separate models. The first is a logit model that estimates the likelihood of having a DMFT/LOA score of zero (vs. any other value) and generates the corresponding odds ratio (OR) along with the 95% confidence interval (CI). The second is a Poisson model that predicts severity of the oral condition among those who had scores of > 0; the results of this second model are expressed as mean count ratios (MCR) and 95% CIs [19]. The final model has been adjusted for the following variables: age, gender, educational status, income, asset index, frequency of cleaning, service utilisation, consumption of fruits, deserts, sugary drinks, tobacco and alcohol consumption and BMI. Population attributable fraction (PAF) of diabetes and common modifiable risk factors were also estimated (Additional file 1: Appendix, Box 1).
As the CARRS-Oral Health study included only a subset of the CARRS-2 cohort participants, key background characteristics of all participants were included in a separate regression model to calculate the probabilities of selection into the sub-study. Inverse values of these probabilities were used as weights in the sensitivity analyses to account for potential selection bias (Additional file 1: Appendix, Table S1).
To ensure that the sub-study sample remained representative of the Delhi target population, final analysis weight was computed by multiplying the sub-study selection weight by the overall CARRS-2 survey weight. Analysis was performed using Stata v14.2 (StataCorp, College Station, Texas, USA).
Results
Out of 2045 participants, 47% were women. Mean (SD) age of the participants was 42.17 (12.8) years. Around 27% participants reported ever-use of tobacco (men 46%, women 7%) and 26% had ever-consumed alcohol (men 48%, women 1%). Average (SD) BMI was 25.91 (5.1) kg/m2, fasting plasma glucose was 107.69 (40.4) mg/dl, HbA1c was 5.90 (1.2) % and 16.9 participants had diabetes. Table 2 shows the background characteristics of study population.
Table 2.
Background characteristics of study participants and oral health scores (N = 2045)
| Characteristics | Total N (%) | DMFT score Mean (SD) |
LOA scorea Mean (SD) |
|---|---|---|---|
| SOCIO-DEMOGRAPHIC FACTORS | |||
| Age group, in years | |||
| 20–39 | 814 (46.0) | 4.61 (3.6) | 0.11 (0.3) |
| 40–59 | 929 (41.5) | 6.00 (5.4) | 0.23 (0.2) |
| ≥ 60 | 302 (12.6) | 13.07 (10.7) | 0.50 (0.6) |
| Gender | |||
| Men | 929 (52.8) | 5.76 (5.8) | 0.23 (0.4) |
| Women | 1116 (47.2) | 6.78 (6.4) | 0.17 (0.3) |
| Education status | |||
| Graduate and above | 531 (27.9) | 5.36 (5.8) | 0.99 (0.3) |
| Higher secondary | 573 (26.5) | 6.25 (6.4) | 0.18 (0.3) |
| High school | 530 (26.5) | 6.37 (5.8) | 0.25 (0.4) |
| Primary or below | 411 (19.1) | 7.38 (6.4) | 0.32 (0.5) |
| Monthly household income, in INR | |||
| ≤ 10,000 | 738 (33.8) | 6.19 (6.1) | 0.26 (0.4) |
| 10,001–20,000 | 567 (28.6) | 6.32 (5.6) | 0.20 (0.3) |
| 20,001–30,000 | 289 (14.2) | 5.84 (6.7) | 0.21 (0.4) |
| ≥ 30,001 | 406 (23.3) | 6.22 (6.0) | 0.11 (0.3) |
| Household asset index | |||
| Low | 725 (34.0) | 6.27 (5.7) | 0.26 (0.4) |
| Middle | 692 (34.8) | 6.13 (5.9) | 0.22 (0.4) |
| High | 628 (31.2) | 6.35 (6.8) | 0.12 (0.3) |
| ORAL HEALTH PRACTICES | |||
| Frequency of cleaning | |||
| Irregular | 46 (2.6) | 13.35 (11.7) | 0.31 (0.4) |
| Once a day | 1458 (72.3) | 5.86 (5.6) | 0.21 (0.4) |
| Twice a day | 541 (25.1) | 6.62 (6.2) | 0.18 (0.3) |
| Dental service utilization | |||
| Never | 642 (32.4) | 4.04 (4.4) | 0.15 (0.3) |
| < 6 months | 299 (13.6) | 7.38 (6.9) | 0.17 (0.4) |
| 6–24 months | 460 (23.6) | 7.29 (6.1) | 0.25 (0.4) |
| > 24 months | 644 (30.4) | 7.27 (6.9) | 0.23 (0.4) |
| MODIFIABLE RISK FACTORS AND DIABETES | |||
| Frequency of fruits intake | |||
| Daily/weekly | 1336 (66.3) | 6.08 (6.0) | 0.17 (0.4) |
| Monthly | 215 (10.5) | 6.90 (6.4) | 0.26 (0.4) |
| Never | 494 (23.2) | 6.41 (6.3) | 0.24 (0.4) |
| Frequency of sugary drinks consumption | |||
| Daily/weekly | 588 (31.1) | 5.42 (5.4) | 0.14 (0.3) |
| Monthly | 336 (16.1) | 6.92 (5.9) | 0.21 (0.4) |
| Never | 1121 (52.8) | 6.53 (6.5) | 0.24 (0.4) |
| Frequency of desserts consumption | |||
| Daily/weekly | 682 (36.0) | 5.75 (5.5) | 0.17 (0.4) |
| Monthly | 767 (37.2) | 6.29 (5.9) | 0.16 (0.3) |
| Never | 595 (26.8) | 6.84 (7.1) | 0.29 (0.4) |
| Tobacco consumptionb | |||
| Yes | 466 (27.5) | 5.99 (6.3) | 0.32 (0.4) |
| No | 1579 (72.6) | 6.34 (5.7) | 0.16 (0.3) |
| Alcohol consumptionb | |||
| Yes | 409 (25.7) | 5.75 (5.0) | 0.23 (0.3) |
| No | 1636 (74.3) | 6.42 (6.5) | 0.19 (0.4) |
| BMI groups | |||
| Underweight | 98 (5.4) | 3.88 (4.3) | 0.19 (0.3) |
| Normal | 804 (41.5) | 6.46 (6.0) | 0.22 (0.4) |
| Overweight | 695 (32.4) | 6.11 (5.9) | 0.20 (0.4) |
| Obese | 437 (20.6) | 6.58 (6.8) | 0.16 (0.3) |
| Diabetes Status | |||
| Diabetes | 406 (16.9) | 7.85 (8.6) | 0.28 (0.5) |
| No diabetes | 1639 (83.1) | 5.92 (5.5) | 0.18 (0.4) |
DMFT Decayed, Missing, Filled Tooth
LOA Loss of Attachment
SD Standard Deviation
INR Indian Rupee
BMI Body Mass Index
aMean of mean LOA scores
bEver-used
The age-standardised prevalence (95% CI) estimates were 78.9% (75.6–81.7) for dental caries, 35.9% (32.3–39.6) for periodontitis, 14.9% (10.8–20.1) for fluorosis and 3.1% (2.2–4.3) for dental trauma. Only 15% participants had healthy gingiva, bleeding on probing and calculus deposits were observed in 57 and 24% participants respectively. The mean number of sound teeth present in study participants were 25.75 (6.1). Oral pre-malignant lesions; leucoplakia and lichen planus were provisionally diagnosed in 1.6% of participants. Nearly 85% participants suffered from at least one form of oral disease. With respect to oral hygiene practices, only 26% participants reported cleaning their teeth twice-daily and 31% participants had never visited a dental care facility.
The mean (SD) values for DMFT and LOA indices were 5.71 (5.0) and 0.20 (0.4) respectively. Details of score distributions are presented in Table 2.
Estimates from the logit model of ZIP regression showed that the odds of having zero score for caries experience and attachment loss were significantly higher among younger participants, those with higher education, higher household income and had never visited a dental facility. The likelihood of having zero LOA score was significantly lower among those who had ‘ever-used’ tobacco.
The Poisson component showed that among those with score > 0, participants in older age and low household income groups had significantly greater severity of caries experience and attachment loss when compared to their reference groups (Table 3). Women had higher DMFT, but lower LOA counts relative to men. MCRs were significantly higher among those who did not clean their teeth regularly. Participants with diabetes presented with more severe caries experience and attachment loss compared to diabetes-free participants. The MCR (95% CI) estimates for DMFT was 1.07 (1.03–1.12) and LOA was 1.10 (1.04–1.17) after adjusting for co-variates.
Table 3.
Multivariable results of Zero Inflated Poisson regression by determinants of oral health (N = 1988)
| DMFT | LOA | |||
|---|---|---|---|---|
| Logit model | Poisson model | Logit model | Poisson model | |
| OR (95% CI) n = 1988 | MCR (95% CI) n = 1750 | OR (95% CI) n = 1988 | MCR (95% CI) n = 710 | |
| SOCIO-DEMOGRAPHIC FACTORS | ||||
| Age group, in years | ||||
| 20–39 | 1 | 1 | 1 | 1 |
| 40–59 | 0.93 (0.67–1.30) | 1.20d (1.15–1.26) | 0.32d (0.24–0.41) | 1.35d (1.22–1.48) |
| ≥ 60 | 0.35c (0.17–0.69) | 2.43d (2.30–2.62) | 0.05d (0.03–0.08) | 2.65d (2.40–2.93) |
| Gender | ||||
| Men | 1 | 1 | 1 | 1 |
| Women | 0.70 (0.48–1.03) | 1.09d (1.04–1.14) | 1.06 (0.80–1.40) | 0.89d (0.84–0.95) |
| Education status | ||||
| Graduate and above | 1 | 1 | 1 | 1 |
| Higher Secondary | 0.80 (0.53–1.21) | 1.08c (1.03–1.14) | 0.73 (0.53–1.01) | 1.07 (0.99–1.16) |
| High school | 0.70 (0.44–1.13) | 1.04 (0.98–1.10) | 0.51d (0.36–0.72) | 1.03 (0.95–1.12) |
| Primary or below | 0.64 (0.36–1.14) | 1.02 (0.95–1.08) | 0.58c (0.39–0.87) | 1.06 (0.97–1.17) |
| Monthly Household income, in INR | ||||
| ≥ 30,001 | 1 | 1 | 1 | 1 |
| ≤ 10,000 | 0.73 (0.42–1.27) | 1.17d (1.10–1.25) | 0.55d (0.37–0.83) | 1.13b (1.03–1.25) |
| 10,001–20,000 | 0.68 (0.41–1.14) | 1.07b (1.01–1.13) | 0.63b (0.44–0.91) | 0.96 (0.88–1.04) |
| 20,001–30,000 | 0.84 (0.50–1.39) | 1.07b (1.01–1.13) | 0.69 (0.47–1.01) | 1.09 (1.00–1.19) |
| Household asset index | ||||
| High | 1 | 1 | 1 | 1 |
| Low | 0.79 (0.42–1.38) | 0.98 (0.92–1.05) | 0.75 (0.50–1.12) | 0.93 (0.84–1.02) |
| Middle | 0.92 (0.59–1.42) | 0.95 (0.91–1.00) | 1.03 (0.75–1.42) | 0.97 (0.91–1.05) |
| ORAL HEALTH PRACTICES | ||||
| Frequency of cleaning | ||||
| Twice a day | 1 | 1 | 1 | 1 |
| Irregular | 0.27 (0.06–1.22) | 1.68d (1.53–1.83) | 0.73 (0.35–1.52) | 1.94d (1.74–2.16) |
| Once a day | 0.89 (0.63–1.25) | 0.98 (0.95–1.02) | 1.24 (0.97–1.58) | 1.08c (1.02–1.14) |
| Dental service utilization | ||||
| < 6 months | 1 | 1 | 1 | 1 |
| 6–24 months | 1.11 (0.59–2.09) | 0.97 (0.97–1.07) | 0.93 (0.66–1.31) | 0.89d (0.82–0.97) |
| > 24 months | 1.31d (0.73–2.37) | 1.02 (0.97–1.07) | 1.15 (0.83–1.59) | 0.99 (0.92–1.06) |
| Never | 4.71d (2.70–8.18) | 0.72d (0.67–0.76) | 2.14d (1.51–3.04) | 0.74d (0.67–0.81) |
| MODIFIABLE RISK FACTORS AND DIABETES | ||||
| Frequency of fruits intake | ||||
| Daily/weekly | 1 | 1 | 1 | 1 |
| Monthly | 0.71 (0.41–1.21) | 1.10c (1.04–1.16) | 0.69b (0.48–0.99) | 1.09b (1.01–1.18) |
| Never | 0.81 (0.55–1.18) | 1.06c (1.02–1.11) | 0.86 (0.65–1.12) | 1.07b (1.01–1.14) |
| Frequency of sugary drinks consumption | ||||
| Never | 1 | 1 | 1 | 1 |
| Daily/weekly | 0.91 (0.64–1.29) | 1.00 (0.96–1.04) | 1.10 (0.85–1.42) | 1.03 (0.96–1.10) |
| Monthly | 0.89 (0.58–1.38) | 1.11d (1.06–1.16) | 0.89 (0.65–1.20) | 1.00 (0.93–1.08) |
| Frequency of desserts consumption | ||||
| Never | 1 | 1 | 1 | 1 |
| Daily/weekly | 0.79 (0.53–1.18) | 1.02 (0.97–1.07) | 1.30 (0.98–1.74) | 1.09b (1.02–1.17) |
| Monthly | 0.82 (0.56–1.20) | 1.02 (0.97–1.06) | 1.39b (1.06–1.83) | 0.97 (0.91–1.03) |
| Tobacco consumptiona | ||||
| No | 1 | 1 | 1 | 1 |
| Yes | 1.35 (0.89–2.03) | 1.05 (1.00–1.10) | 0.69b (0.51–0.94) | 0.95 (0.88–1.02) |
| Alcohol consumptiona | ||||
| No | 1 | 1 | 1 | 1 |
| Yes | 0.84 (0.55–1.28) | 0.97 (0.91–1.02) | 1.00 (0.72–1.38) | 0.83d (0.77–0.90) |
| BMI groups | ||||
| Normal | 1 | 1 | 1 | 1 |
| Underweight | 1.24 (0.68–2.27) | 0.91b (0.82–0.99) | 1.14 (0.67–1.94) | 0.92 (0.79–1.08) |
| Overweight | 0.73 (0.50–1.04) | 0.92d (0.89–0.97) | 0.97 (0.75–1.26) | 1.03 (0.96–1.09) |
| Obese | 0.82 (0.52–1.27) | 0.99 (0.94–1.05) | 1.21 (0.88–1.67) | 1.24d (1.15–1.34) |
| Diabetes Status | ||||
| No Diabetes | 1 | 1 | 1 | 1 |
| Diabetes | 0.95 (0.62–1.45) | 1.07c (1.03–1.12) | 0.90 (0.68–1.19) | 1.10c (1.04–1.17) |
DMFT Decayed, Missing, Filled Tooth Score
LOA Loss of Attachment Score
OR Odds Ratio
CI Confidence Intervals
MCR Mean Count Ratio
INR Indian Rupee
BMI Body Mass Index
aEver used
bp < 0.05
cp < 0.01
dp < 0.001
Figure 2 shows that the adjusted prevalence of periodontitis was significantly higher among participants with diabetes 42.3 (95%CI: 40.0–45.0) compared to their disease-free counterparts 31.3 (30.3–32.2) but prevalence of caries was higher among those without diabetes [80.1 (79.7–80.4) vs. 73.2 (72.3–74.1)]. Mean number of sound teeth present among those with diabetes was significantly lower than those without diabetes (24.14 vs. 26.07; p < 0.001). Collectively, diabetes and common risk factors (diet, tobacco use, frequency of cleaning) accounted for 12% & 15% of the PAF of DMFT and LOA scores respectively (Additional file 1: Appendix, Table S2).
Fig. 2.
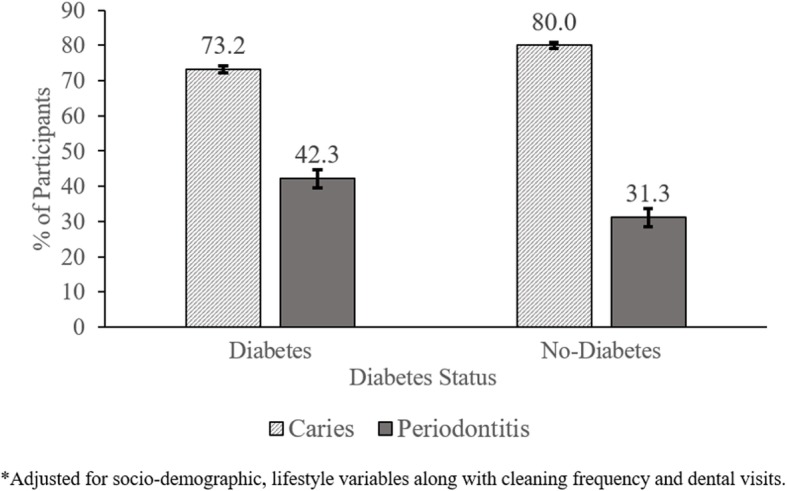
Adjusted* prevalence of dental caries and periodontitis by diabetes status
Discussion
We found a high prevalence of dental caries and periodontitis among Delhi CARRS-cohort members. These results are consistent with other studies reporting prevalence estimates from India [20]. Previous studies also confirm a similar service utilization pattern, with 77% participants ‘ever-visiting’ a dental facility [21]. Study participants who had ‘never-visited’ a dental facility had greater likelihood of having zero scores. Good oral health could be the reason for their non-visits as oral health is often perceived unimportant and visits are associated with symptoms such as pain or discomfort [22].
Most of the participants practiced inadequate oral hygiene. This results in improper removal of dental plaque and debris which adheres to the tooth surface and gingiva leading to caries and gingival inflammation. A similar inflammatory response is observed in tobacco users resulting in gingival damage [23]. This could be the reason for lower odds of zero score among tobacco users in the study. Though sugar-rich diet is an important risk factor for caries but our data did not confirm this association [24]. Several others factors, that include: nature and adhesiveness of diet, salivary characteristics, masticatory functions, and nutritional inadequacy of micronutrients are also accountable [24]. These details were not captured in our study.
Our finding, that participants with diabetes had poor periodontal health than those without diabetes, corresponds with studies from high income countries [7, 25–27]. The National Health and Nutrition Examination Survey III found that adults with HbA1c > 9% had a significantly higher prevalence of severe periodontitis than those without diabetes [OR = 2.90 (1.40–6.03)] after controlling for confounders [27]. Studies also report participants with diabetes had greater tooth loss and gingival bleeding on probing [26]. Individuals with uncontrolled diabetes also have a higher risk of infection, as well as prolonged healing time [28]. We found lower prevalence of caries in participants with diabetes but higher cumulative DMFT score compared to those without diabetes. This could be attributed to greater missing-tooth component [29].
Studies on the cooccurrence of dental caries and diabetes have yielded non-conclusive results [30, 31]. Diet modification is often advised for patients with diabetes. The restricted consumption of carbohydrates may have a non-cariogenic effect on the participants with diabetes in the study additionally the anti-microbial defense capacity of saliva is not weakened in diabetes [32]. On the contrary, increased salivary glucose concentration could be the reason for increased caries among patients with diabetes.
Mechanistic links suggest Hyperglycaemia often results in altered cellular immunity, proliferation of bacteria, and formation of advanced glycation end-products (AGEs) [5]. Altered cellular immunity results in dysfunction of cells, inflammation and degradation of supporting connective tissue [6]. Bacterial proliferation also exacerbates the inflammatory response contributing to periodontal destruction [4]. Excess glucose forms AGEs on coming in contact with structural proteins [33, 34]. These end-products stimulate endothelial receptors and perpetuate a series of inflammatory events by attracting monocytes and ultimately leading to degradation of the attachment apparatus. Furthermore, hyperglycaemic environment impairs the function of fibroblasts and predisposes collagen to degradation by matrix metalloproteinase enzymes, thereby preventing tissue repair and regeneration [35]. Reduced salivary flow, pH, dryness of mouth and gingival recession is also commonly observed in diabetes, predisposing to dental decay and tooth loss [36]. Previous studies have concluded that diabetes has many adverse effects on periodontal tissue, and conversely, periodontitis may aggravate the hyperglyceamia. Combined results from 13 meta-analyses indicate a significant but small effect of periodontal treatment on improved HbA1c in diabetes patients [28]. However, it warrants additional high-quality studies to obtain a conclusive evidence.
Oral health care is conventionally disease-oriented, curative in nature and serves limited people due to high costs. Given the burden of unmet dental care needs and their association with systemic conditions, it is imperative to bridge the disconnect and re-orient oral-health services to be integrated and prevention-based at community level. It is propagated that these services should primarily be based on education to increase awareness and influence attitude of the people in seeking oral health care [37]. Pilot projects have demonstrated positive outcomes where health-facility staff was trained to deliver oral health education messages by integrating within their primary health care tasks [37]. Better collaboration by minimal training and expanding the role of other health professionals can be useful in providing basic oral health education and early recognition of oral conditions for further referral. Integration of oral health with the national chronic disease programs require serious consideration given the high burden of oral diseases, NCDs and shared set of risk factors [10]. The Government of India’s National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Disease and Stroke (NPCDCS) launched in 2010 lacks any oral health goals within it [38]. However, its recent expansion includes screening, early detection, management and referral of cases of three common cancers, oral cancer being one of them [39]. Therefore, an integrated approach inclusive of oral health may have greater benefits for health of the community and facilitate judicious use of resources.
Our study is among the few studies in India to have followed a comprehensive approach by integrating oral health with NCDs [40–43]. To our knowledge, this is the first study with the above strategy using a representative sample from community. We have used standard survey methods that will enable comparison of findings from other studies. Although index teeth examination may underestimate the prevalence of periodontal disease, this method is efficient in estimating the mean periodontal scores. Adoption of this method prevented examiner fatigue and excessive participant time. Other limitations include the fact that clinical examination was not supported by radiographic or saliva sample investigations, cross-sectional nature limits conclusion of causal relations and duration and severity of diabetes was not used in present analysis.
Conclusion
In summary, we found that eight out of ten participants in urban Delhi suffered from some form of oral disease and participants with diabetes had worse oral health. The high burden of oral diseases and diabetes among Indians, evidence of their association and role of shared risk factors provides an opportunity to expand the scope of existing national NCD program by integrating oral health interventions.
Additional file
Appendix. The file contains Box 1: formulae for calculating population attributable fraction (PAF), Table S1. Sample distribution of participants in oral health sub-study and CARRS-2 Delhi cohort and Table S2. Population attributable fraction associated with common risk factors. (DOCX 26 kb)
Acknowledgements
The authors would like to acknowledge the dental surgeons for conducting clinical examination and the CARRS Study field team for their support.
Abbreviations
- AGEs
Advanced glycation end-products
- BMI
Body Mass Index
- CARRS
Cardio-metabolic Risk Reduction in South Asia
- CI
Confidence interval
- CPI
Community Periodontal Index
- DMFT
Decayed, Missing, Filled Tooth
- INR
Indian Rupee
- LMIC
Low and Middle-Income Countries
- LOA
Loss of Attachment
- MCR
Mean Count Ratio
- NCD
Non-Communicable Disease
- PAF
Population attributable fraction
- SD
Standard Deviation
- ZIP
Zero-Inflated Poisson
Authors’ contributions
IR and SSH were responsible for the concept, design and implementation of the work. SG analysed the participant data. SAP, MG helped in interpretation of data and were major contributors in writing the manuscript along with IR. RSA, VSA, MKA, KMV, NT and DP also drafted the work and substantively revised it. All authors read and approved the final manuscript.
Funding
This sub-study was coordinated by Center of Excellence-CARRS based at Public Health Foundation of India (PHFI), New Delhi, India in collaboration with Centre for Chronic Disease Control (CCDC), New Delhi, Emory University, Atlanta, U.S.A., All India Institute of Medical Sciences (AIIMS), New Delhi. This project is funded in part by the National Heart, Lung, and Blood Institute (NHLBI), National Institutes of Health (NIH), Department of Health and Human Services, under Contract No. HHSN268200900026C, and the United Health Group, Minneapolis, MN, USA. Several members of the research team were/are supported by the Fogarty International Center (FIC) and the Eunice Kennedy Shriver National Institute of Child Health & Human Development at the National Institutes of Health through Grant Number 1 D43 HD065249, Fogarty International Center of the National Institutes of Health under Award Number D43TW009135 and NIH, National Cancer Institute grant number P20CA210298–01. RS was supported by a Wellcome Trust Capacity Strengthening Strategic Award Extension phase to the Public Health Foundation of India and a consortium of UK universities (WT084754/Z/08/A). However, the contents of this paper are solely the responsibility of the writing group and do not necessarily represent the official views of the funding agency. The funding agency had no role in design, data collection, analysis, and interpretation and in writing the manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Ethical approval was obtained from the Institutional Review Board of Public Health Foundation of India. The IEC No. of the study was TRC-IEC-34/09.1 All study participants were approached and written informed consent was obtained to participate in the study.
Consent for publication
NA.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Ishita Rawal, Phone: 011-41618456, Email: ishita@ccdcindia.org.
Shreeparna Ghosh, Email: smilyshri@gmail.com.
Safraj Shahul Hameed, Email: safraj.s@phfi.org.
Roopa Shivashankar, Email: roopa@ccdcindia.org.
Vamadevan S. Ajay, Email: ajay@ccdcindia.org
Shivani Anil Patel, Email: s.a.patel@emory.edu.
Michael Goodman, Email: mgoodm2@emory.edu.
Mohammed K. Ali, Email: mkali@emory.edu
K. M. Venkat Narayan, Email: knaraya@emory.edu.
Nikhil Tandon, Email: nikhil_tandon@hotmail.com.
Dorairaj Prabhakaran, Email: dprabhakaran@ccdcindia.org.
References
- 1.Kassebaum NJ, Smith AGC, Bernabé E, Fleming TD, Reynolds AE, Vos T, et al. Global, regional, and National Prevalence, incidence, and disability-adjusted life years for Oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017;96(4):380–387. doi: 10.1177/0022034517693566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Balaji S. Burden of dental diseases in India as compared to South Asia: An insight. Indian J Dent Res. 2018;29(3):374. doi: 10.4103/ijdr.IJDR_333_18. [DOI] [PubMed] [Google Scholar]
- 3.Shah N, Mathur VP, Kant S, Gupta A, Kathuria V, Haldar P, et al. Prevalence of dental caries and periodontal disease in a rural area of Faridabad District, Haryana, India. Indian J Dent Res. 2017;28(3):242–247. doi: 10.4103/ijdr.IJDR_370_16. [DOI] [PubMed] [Google Scholar]
- 4.IDF. IDF Diabetes Atlas. 8th ed; 2017. idf.org. Available from: http://www.diabetesatlas.org/. Accessed 3 Mar 2018.
- 5.Novotna M, Podzimek S, Broukal Z, Lencova E, Duskova J. Periodontal Diseases and Dental Caries in Children with Type 1 Diabetes Mellitus. Mediators Inflamm. 2015;2015:379626. doi: 10.1155/2015/379626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mealey BL. Periodontal disease and diabetes. A two-way street. J Am Dent Assoc. 2006;137(Suppl (October)):26S–31S. doi: 10.14219/jada.archive.2006.0404. [DOI] [PubMed] [Google Scholar]
- 7.Nelson RG, Shlossman M, Budding LM, Pettitt DJ, Saad MF, Genco RJ, et al. Periodontal disease and NIDDM in Pima Indians. Diabetes Care. 1990;13(8):836–840. doi: 10.2337/diacare.13.8.836. [DOI] [PubMed] [Google Scholar]
- 8.Petersen PE, Bourgeois D, Ogawa H, Estupinan-day S, Ndiaye C. Policy and practice the global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(05):661–669. [PMC free article] [PubMed] [Google Scholar]
- 9.Newton JT, Prabhu N, Robinson PG. The impact of dental appearance on the appraisal of personal characteristics. Int J Prosthodont. 2003;16(4):429–434. [PubMed] [Google Scholar]
- 10.Sheiham A, Watt RG. The common risk factor approach: a rational basis for promoting oral health. Community Dent Oral Epidemiol. 2000;28(6):399–406. doi: 10.1034/j.1600-0528.2000.028006399.x. [DOI] [PubMed] [Google Scholar]
- 11.Petersen PE, Bourgeois D, Bratthall D, Ogawa H. Oral health information systems--towards measuring progress in oral health promotion and disease prevention. Bull World Health Organ. 2005;83(9):686–693. [PMC free article] [PubMed] [Google Scholar]
- 12.Nair M, Ali MK, Ajay VS, Shivashankar R, Mohan V, Pradeepa R, et al. CARRS Surveillance study: design and methods to assess burdens from multiple perspectives. BMC Public Health. 2012;12(1):701. doi: 10.1186/1471-2458-12-701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Doifode VV, Ambadekar NN, Lanewar AG. Assessment of oral health status and its association with some epidemiological factors in population of Nagpur, India. Indian J Med Sci. 2000;54(7):261–269. [PubMed] [Google Scholar]
- 14.Anokwa Y, Hartung C, Brunette W. Open source data collection in the developing world. Computer (Long Beach Calif) 2009;42(10):97–99. [Google Scholar]
- 15.Who Oral Health Surveys - Basic Methods. World Health Organ. 2013;1:137. [Google Scholar]
- 16.Page RC, Eke PI. Case definitions for use in population-based surveillance of periodontitis. J Periodontol. 2007;78(7 Suppl):1387–1399. doi: 10.1902/jop.2007.060264. [DOI] [PubMed] [Google Scholar]
- 17.Riddle MC, Bakris G, Blonde L, AJM B, D ‘alessio D, De Groot M, et al. Introduction: Standards of Medical Care in Diabetes—2018. Diabetes Care. 2018;41(Supplement 1):S1–S2. doi: 10.2337/dc18-Sint01. [DOI] [PubMed] [Google Scholar]
- 18.Iqbal R, Anand S, Ounpuu S, Islam S, Zhang X, Rangarajan S, et al. Dietary patterns and the risk of acute myocardial infarction in 52 countries: results of the INTERHEART study. Circulation. 2008;118(19):1929–1937. doi: 10.1161/CIRCULATIONAHA.107.738716. [DOI] [PubMed] [Google Scholar]
- 19.Preisser JS, Stamm JW, Long DL, Kincade ME. Review and recommendations for zero-inflated count regression modeling of dental caries indices in epidemiological studies. Vol. 46, Caries Research. 2012. pp. 413–423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shah N, Pandey R, Duggal R, Mathur V, Rajan K. Oral health in India: a report of the multi centric study, directorate general of health services, Ministry of Health and Family Welfare, government of India and World Health Organisation collaborative program. New Delhi; 2007. Available from: https://www.scienceopen.com/document?vid=29e38796-6867-4d5d-88a8-f70608f3c86e. Accessed 25 Apr 2016.
- 21.Kadaluru UG, Kempraj VM, Muddaiah P. Utilization of oral health care services among adults attending community outreach programs. Indian J Dent Res. 2012;23(6):841–842. doi: 10.4103/0970-9290.111290. [DOI] [PubMed] [Google Scholar]
- 22.Gambhir RS, Brar P, Singh G, Sofat A, Kakar H. Utilization of dental care: an Indian outlook. J Nat Sci Biol Med. 2013;4(2):292–297. doi: 10.4103/0976-9668.116972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bergström J. Tobacco smoking and chronic destructive periodontal disease. Odontology. 2004;92(1):1–8. doi: 10.1007/s10266-004-0043-4. [DOI] [PubMed] [Google Scholar]
- 24.Chapple ILC, Bouchard P, Cagetti MG, Campus G, Carra MC, Cocco F, et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol. 2017;44:S39–S51. doi: 10.1111/jcpe.12685. [DOI] [PubMed] [Google Scholar]
- 25.Taylor GW, Burt BA, Becker MP, Genco RJ, Shlossman M, Knowler WC, et al. Severe periodontitis and risk for poor glycemic control in patients with non-insulin-dependent diabetes mellitus. J Periodontol. 1996;67(10 Suppl):1085–1093. doi: 10.1902/jop.1996.67.10s.1085. [DOI] [PubMed] [Google Scholar]
- 26.Lamster IB, Cheng B, Burkett S, Lalla E. Periodontal findings in individuals with newly identified pre-diabetes or diabetes mellitus. J Clin Periodontol. 2014;41(11):1055–1060. doi: 10.1111/jcpe.12307. [DOI] [PubMed] [Google Scholar]
- 27.Tsai C, Hayes C, Taylor GW. Glycemic control of type 2 diabetes and severe periodontal disease in the US adult population. Community Dent Oral Epidemiol. 2002;30(3):182–192. doi: 10.1034/j.1600-0528.2002.300304.x. [DOI] [PubMed] [Google Scholar]
- 28.Hasuike A, Iguchi S, Suzuki D, Kawano E, Sato S. Systematic review and assessment of systematic reviews examining the effect of periodontal treatment on glycemic control in patients with diabetes. Med Oral Patol Oral Cir Bucal. 2017;22(2):e167–e176. doi: 10.4317/medoral.21555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lin Brent P.-J., Taylor George W., Allen Doris J., Ship Jonathan A. Dental caries in older adults with diabetes mellitus. Special Care in Dentistry. 1999;19(1):8–14. doi: 10.1111/j.1754-4505.1999.tb01361.x. [DOI] [PubMed] [Google Scholar]
- 30.Collin HL, Uusitupa M, Niskanen L, Koivisto AM, Markkanen H, Meurman JH. Caries in patients with non-insulin-dependent diabetes mellitus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(6):680–685. doi: 10.1016/S1079-2104(98)90035-X. [DOI] [PubMed] [Google Scholar]
- 31.Tavares M, Depaola P, Soparkar P, Joshipura K. The prevalence of root caries in a diabetic population. J Dent Res. 1991;70(6):979–983. doi: 10.1177/00220345910700061401. [DOI] [PubMed] [Google Scholar]
- 32.Tenovuo J, Lehtonen OP, Viikari J, Larjava H, Vilja P, Tuohimaa P. Immunoglobulins and innate antimicrobial factors in whole saliva of patients with insulin-dependent diabetes mellitus. J Dent Res. 1986;65(1):62–66. doi: 10.1177/00220345860650011101. [DOI] [PubMed] [Google Scholar]
- 33.Seppälä B, Sorsa T, Ainamo J. Morphometric analysis of cellular and vascular changes in gingival connective tissue in Long-term insulin-dependent diabetes. J Periodontol. 1997;68(12):1237–1245. doi: 10.1902/jop.1997.68.12.1237. [DOI] [PubMed] [Google Scholar]
- 34.Preshaw PM, Alba AL, Herrera D, Jepsen S, Konstantinidis A, Makrilakis K, et al. Periodontitis and diabetes: a two-way relationship. Diabetologia. 2012;55(1):21–31. doi: 10.1007/s00125-011-2342-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Willershausen-Zönnchen B, Lemmen C, Hamm G. Influence of high glucose concentrations on glycosaminoglycan and collagen synthesis in cultured human gingival fibroblasts. J Clin Periodontol. 1991;18(3):190–195. doi: 10.1111/j.1600-051X.1991.tb01132.x. [DOI] [PubMed] [Google Scholar]
- 36.Kudiyirickal MG, Pappachan JM. Diabetes mellitus and oral health. Endocrine. 2015;49(1):27–34. doi: 10.1007/s12020-014-0496-3. [DOI] [PubMed] [Google Scholar]
- 37.Helderman Wim van Palenstein, Mikx Frans, Begum Aziza, Adyatmaka Andreas, Bajracharya Manik, Kikwilu Emil, Rugarabamu Paschalis. Integrating oral health into primary health care - experiences in Bangladesh, Indonesia, Nepal and Tanzania. International Dental Journal. 1999;49(4):240–248. doi: 10.1111/j.1875-595X.1999.tb00528.x. [DOI] [PubMed] [Google Scholar]
- 38.Ministry of Health and Family Welfare. National Programme For Prevention and Control of Cancer, Diabetes, Cardiovascular Disease and Stroke (NPCDCS) [Internet]. Available from: https://mohfw.gov.in/about-us/departments/departments-health-and-family-welfare/national-programme-prevention-and-control-cancer-diabetes-cardiovascular-disease-and. Accessed 18 June 2018.
- 39.Ministry of Health and Family Welfare . Prevention screening and control of common Non-Communicable Diseases: Hypertension, Diabetes and Common Cancers (Oral, Breast and Cervix) 2016. [Google Scholar]
- 40.Bajaj S, Prasad S, Gupta A, Singh VB. Oral manifestations in type-2 diabetes and related complications. Indian J Endocrinol Metab [Internet] 2012;16(5):777–779. doi: 10.4103/2230-8210.100673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Singh A, Gupta A, Peres MA, Watt RG, Tsakos G, Mathur MR. Association between tooth loss and hypertension among a primarily rural middle aged and older Indian adult population. J Public Health Dent. 2016;76(3):198–205. doi: 10.1111/jphd.12136. [DOI] [PubMed] [Google Scholar]
- 42.Singh Iqbal, Singh Paramjeet, Singh Amarpreet, Singh Tara, Kour Robindera. Diabetes an inducing factor for dental caries: A case control analysis in Jammu. Journal of International Society of Preventive and Community Dentistry. 2016;6(2):125. doi: 10.4103/2231-0762.178748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Shetty D, Dua M, Kumar K, Dhanapal R, Astekar M, Shetty DC. Oral hygiene status of individuals with cardiovascular diseases and associated risk factors. Clin Pract. 2012;2(4):e86. doi: 10.4081/cp.2012.e86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix. The file contains Box 1: formulae for calculating population attributable fraction (PAF), Table S1. Sample distribution of participants in oral health sub-study and CARRS-2 Delhi cohort and Table S2. Population attributable fraction associated with common risk factors. (DOCX 26 kb)
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.