Abstract
Objective To analyze whether a reduction in the waiting time for orthopedic surgery in elderly patients with fracture of the proximal end of the femur leads to a reduction in in-hospital mortality, 6-month mortality, and duration of hospitalization.
Methods This was a retrospective cohort study including 81 patients with intertrochanteric and subtrochanteric fractures who underwent surgical repair between 2015 and 2016 in a referral hospital, before and after a protocol for early surgical fixation (< 48 hours) was implemented.
Results The mean length of hospital stay decreased from 17 to 11 days. Regarding the in-hospital mortality rate, five patients died before, and another five died after the protocol was implemented. The 6-month postoperative mortality decreased from 26.7% to 19.4%. The results showed no statistical significance.
Conclusion The present study demonstrated that there is a tendency to reduce the length of hospital stay and 6-month mortality when the surgery for the treatment of proximal femoral fractures in the elderly is performed within 48 hours of hospitalization.
Keywords: hip fractures, mortality, elderly, orthopedics
Introduction
The progressive increase in life expectancy observed over the last decades resulted in a significant increase in the prevalence of trauma in elderly individuals. Proximal femur fractures are among the most common fractures in the elderly, and present high morbidity and mortality rates, constituting a public health issue. Epidemiological data indicate that the 1-year mortality of elderly patients with proximal femoral fractures ranges from 14 to 36%, 1 2 3 4 5 6 and only 50 to 65% of these patients completely recover their previous functional activity. 1 7 8
More than 98% of the cases are surgically treated, and evidence indicates that surgery performed within 48 hours reduces the risk of complications secondary to femoral fractures in the elderly. On the other hand, surgeries performed after 48 hours or more increase the risk of mortality in 30 days and up to 1 year. 9 10 11 12 13 Considering the importance of this issue, the present study was developed to analyze whether the reduction in the waiting time for orthopedic surgery in elderly patients with proximal femoral fractures has an impact on the reduction of in-hospital and 6-month mortalities, as well as on the length of hospital stay.
Material and Methods
This was a retrospective cohort study including male and female patients > 60 years old with closed isolated femoral transtrochanteric or subtrochanteric fractures. The anatomical classification of the fractures was made by an orthopedist with a specialist degree at the emergency room, and was confirmed by the orthopedic surgeon at the referral hospital.
The present study was submitted and approved by the Ethics in Research Committee of our institution under the number 1.890.165. Data regarding hospitalization (length of hospital stay, diagnosis, treatment and clinical outcome) were obtained through a review of electronic medical records. The verification of death and its date were obtained from the electronic medical records, by contact by telephone, or from the obituary.
A specific protocol was developed in 2016 for the care of elderly patients with proximal femoral fractures in the urgency and emergency network of our hospital to reduce the waiting time for orthopedic surgery in this type of fracture and, thus, to reduce mortality and length of hospital stay. The primary objective of this protocol is to operate elderly patients with transtrochanteric and/or subtrochanteric fractures within 48 hours of hospital admission.
Every patient in the study was admitted and underwent surgical treatment at a referral hospital in trauma care starting in 2015. The patients were divided into 2 groups: those who underwent surgery under the femoral fracture in the elderly protocol (after the first quarter of 2016) and those who underwent surgery outside the protocol (throughout 2015 and during the first quarter of 2016).
Patients with incomplete and/or insufficient data at the review of the medical records, patients who had undergone nonsurgical treatments, and those who could not be reached by telephone, deemed lost at follow-up, were excluded from the study.
The following variables were studied: length of hospital stay (before and after the implementation of the protocol), and general, in-hospital and 6-month mortalities. The data were analyzed through tables and parametrical analysis of variance (ANOVA) and equality of two proportions statistical tests using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, US), Minitab 16 (Minitab, LLC., State College, PA, US), and Excel (Microsoft Corporation, Redmond, WA, US). A maximum significance level of 5% ( p ≤ 0.05) was defined.
Results
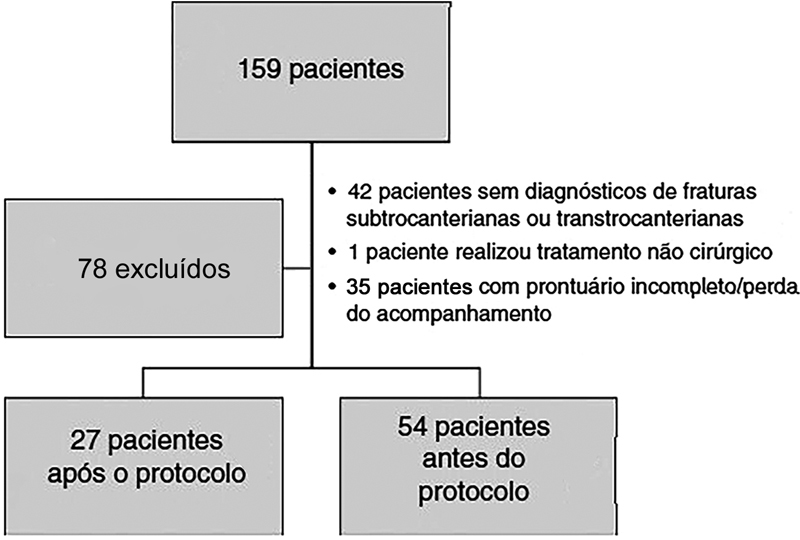
A total of 159 patients were selected in 2015 and 2016 under ICD10 S72. Of the total, 78 patients were excluded because they did not meet the study criteria, resulting in a final sample of 81 patients ( Fig. 1 ). All of the patients had their electronic medical records reviewed and/or were contacted by telephone.
Fig. 1.
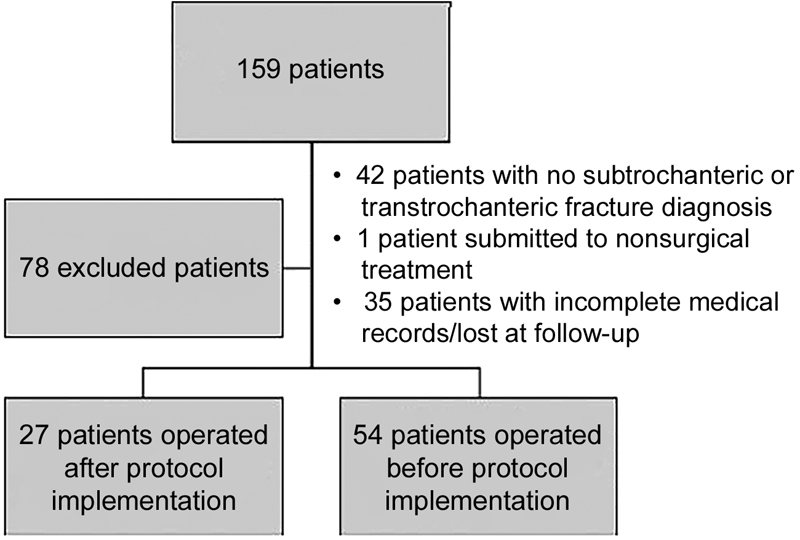
Flow chart of patient inclusion.
The mean hospital stay was of ∼ 17 days for the group evaluated prior to the implementation of the protocol and of 11 days for patients hospitalized after the implementation of the protocol ( Table 1 ). There was no statistically significant difference ( p = 0.095).
Table 1. Comparison of in-hospital length of stay.
| Length of hospital stay (days) | Before protocol implementation | After protocol implementation |
|---|---|---|
| Average | 16.6 | 11.3 |
| Median | 13 | 8 |
| Standard deviation | 14.8 | 9.3 |
| Coefficient of variation | 89% | 82% |
| Minimum value | 6 | 2 |
| Maximum value | 108 | 35 |
| N | 54 | 27 |
| Confidence interval | 4 | 3.5 |
| p-value | 0.095 | |
Of the total sample, 19 patients died during the investigation period, corresponding to 26.7% of the preprotocol implementation group and 19.4% of the postprotocol implementation group, respectively ( p = 0.446) ( Table 2 ).
Table 2. General mortality in 6 months.
| Before protocol implementation | After protocol implementation | p-value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Non-death | 33 | 73.30% | 29 | 80.60% | 0.446 |
| Death | 12 | 26.70% | 7 | 19.40% | |
During the hospital stay, 5 patients from the preprotocol implementation group and 5 from the postprotocol implementation group died, but there was no statistical difference in the mortality rate between the groups ( p = 0.210) ( Table 3 ).
Table 3. Analysis of deaths.
| Before protocol implementation | After protocol implementation | p-value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| In-hospital | 5 | 41.70% | 5 | 71.40% | 0.21 |
| After discharge | 7 | 53.80% | 2 | 28.60% | |
Discussion
The present study evaluated the length of hospitalization and in-hospital and 6-month mortalities in elderly patients with proximal femoral fractures before and after the implementation of a protocol for early definitive surgical treatment (within 48 hours of admission). We observed a decrease in the length of hospitalization and in the mortality rate at 6 months postsurgery, but with no statistical significance.
Our results showed a reduction in general mortality in 6 months from 26.7% to 19.4% after the implementation of the protocol (a high value compared to other studies, which can be explained by the small number of patients analyzed).
Although it is recommended that the optimal time for surgical treatment of proximal femoral fractures is 24 to 48 hours after the occurrence, some studies have not demonstrated a reduction in mortality or an increase in functional recovery with early surgery. 2 14 15 16 17 18
Orosz et al 2 studied 1,206 patients aged > 50 years old and observed a general mortality rate in 2 months of 8.3%; their analysis showed that surgery within 24 hours does not reduce mortality in 2 and 6 months.
Siegmeth et al, 16 after analyzing 3,628 (clinically compensated) patients aged > 60 years old, concluded that the mortality of previously healthy patients increased when the surgical procedure was performed after 48 hours.
Regarding the length of hospital stay, we noticed a reduction from 17 to 11 days, which, although with no significant association, is consistent with literature findings. Lefaivre et al 19 evaluated 607 patients and concluded that the delay in performing the surgical treatment increased the length of hospital stay, which was related to medical comorbidities, age, gender and type of fracture.
We also identified a percentage increase in in-hospital deaths when comparing the two study groups, which is possibly associated with the medical conditions of the patients and with the lower number of patients operated after the implementation of the protocol.
As limitations of the present study, we emphasize that this is a retrospective analysis, with a small sample when compared with large multicenter studies.
Future studies will be performed with an increased sample population operated under the implemented protocol.
Conclusion
The ideal timing for surgical treatment of proximal femoral fractures in elderly patients is still controversial. Several factors may influence this decision, such as clinical comorbidities and the availability of equipment, a trained staff and a postoperative intensive care unit. The present study demonstrated that the length of hospital stay and the 6-month mortality rate in elderly patients tend to be reduced when the surgical treatment of proximal femoral fractures is performed within 48 hours of admission.
Conflitos de Interesses Os autores declaram não haver conflitos de interesses.
Trabalho desenvolvido no Departamento de Ortopedia e Traumatologia, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, SP, Brasil. Publicado originalmente por Elsevier Editora Ltda.
Study performed at the Orthopedics and Traumatology Department, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, SP, Brazil. Originally Published by Elsevier Editora Ltda.
Referências
- 1.Zuckerman J D. Hip fracture. N Engl J Med. 1996;334(23):1519–1525. doi: 10.1056/NEJM199606063342307. [DOI] [PubMed] [Google Scholar]
- 2.Orosz G M, Magaziner J, Hannan E L et al. Association of timing of surgery for hip fracture and patient outcomes. JAMA. 2004;291(14):1738–1743. doi: 10.1001/jama.291.14.1738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Simunovic N, Devereaux P J, Sprague S et al. Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. CMAJ. 2010;182(15):1609–1616. doi: 10.1503/cmaj.092220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Panula J, Pihlajamäki H, Mattila V M et al. Mortality and cause of death in hip fracture patients aged 65 or older: a population-based study. BMC Musculoskelet Disord. 2011;12:105. doi: 10.1186/1471-2474-12-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schnell S, Friedman S M, Mendelson D A, Bingham K W, Kates S L. The 1-year mortality of patients treated in a hip fracture program for elders. Geriatr Orthop Surg Rehabil. 2010;1(01):6–14. doi: 10.1177/2151458510378105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Parker M, Johansen A.Hip fracture BMJ 2006333(7557):27–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Koval K J, Skovron M L, Aharonoff G B, Meadows S E, Zuckerman J D. Ambulatory ability after hip fracture. A prospective study in geriatric patients. Clin Orthop Relat Res. 1995;(310):150–159. [PubMed] [Google Scholar]
- 8.Koval K J, Zuckerman J D. Functional recovery after fracture of the hip. J Bone Joint Surg Am. 1994;76(05):751–758. doi: 10.2106/00004623-199405000-00018. [DOI] [PubMed] [Google Scholar]
- 9.Bottle A, Aylin P.Mortality associated with delay in operation after hip fracture: observational study BMJ 2006332(7547):947–951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gdalevich M, Cohen D, Yosef D, Tauber C. Morbidity and mortality after hip fracture: the impact of operative delay. Arch Orthop Trauma Surg. 2004;124(05):334–340. doi: 10.1007/s00402-004-0662-9. [DOI] [PubMed] [Google Scholar]
- 11.Perez J V, Warwick D J, Case C P, Bannister G C. Death after proximal femoral fracture--an autopsy study. Injury. 1995;26(04):237–240. doi: 10.1016/0020-1383(95)90008-l. [DOI] [PubMed] [Google Scholar]
- 12.Novack V, Jotkowitz A, Etzion O, Porath A. Does delay in surgery after hip fracture lead to worse outcomes? A multicenter survey. Int J Qual Health Care. 2007;19(03):170–176. doi: 10.1093/intqhc/mzm003. [DOI] [PubMed] [Google Scholar]
- 13.Rogers F B, Shackford S R, Keller M S. Early fixation reduces morbidity and mortality in elderly patients with hip fractures from low-impact falls. J Trauma. 1995;39(02):261–265. doi: 10.1097/00005373-199508000-00012. [DOI] [PubMed] [Google Scholar]
- 14.Majumdar S R, Beaupre L A, Johnston D W, Dick D A, Cinats J G, Jiang H X. Lack of association between mortality and timing of surgical fixation in elderly patients with hip fracture: results of a retrospective population-based cohort study. Med Care. 2006;44(06):552–559. doi: 10.1097/01.mlr.0000215812.13720.2e. [DOI] [PubMed] [Google Scholar]
- 15.Grimes J P, Gregory P M, Noveck H, Butler M S, Carson J L. The effects of time-to-surgery on mortality and morbidity in patients following hip fracture. Am J Med. 2002;112(09):702–709. doi: 10.1016/s0002-9343(02)01119-1. [DOI] [PubMed] [Google Scholar]
- 16.Siegmeth A W, Gurusamy K, Parker M J. Delay to surgery prolongs hospital stay in patients with fractures of the proximal femur. J Bone Joint Surg Br. 2005;87(08):1123–1126. doi: 10.1302/0301-620X.87B8.16357. [DOI] [PubMed] [Google Scholar]
- 17.Franzo A, Simon G, Francescutti C.Mortality associated with delay in operation after hip fracture: ... but Italian data seem to contradict study findings BMJ 2006332(7549):1093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Khan S K, Kalra S, Khanna A, Thiruvengada M M, Parker M J. Timing of surgery for hip fractures: a systematic review of 52 published studies involving 291,413 patients. Injury. 2009;40(07):692–697. doi: 10.1016/j.injury.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 19.Lefaivre K A, Macadam S A, Davidson D J, Gandhi R, Chan H, Broekhuyse H M. Length of stay, mortality, morbidity and delay to surgery in hip fractures. J Bone Joint Surg Br. 2009;91(07):922–927. doi: 10.1302/0301-620X.91B7.22446. [DOI] [PubMed] [Google Scholar]