

Abstract
The British Heart Rhythm Society’s Clinical Practice Guidelines on the Management of Patients Developing QT Prolongation on Antipsychotic Medication are written for heart rhythm consultants, primary care physicians, specialist registrars, nurses and physiologists who may be requested to review ECGs or advise on cases where antipsychotic-induced QT prolongation is suspected or proven. The guidance is adapted from the latest Maudsley Prescribing Guidelines in Psychiatry, published in 2018.
Keywords: Antipsychotic medication, schizophrenia, QT prolongation, guidelines, psychiatry
Heart rhythm consultants, primary care physicians, specialist registrars, nurses and physiologists may be requested to review ECGs or advise on cases where antipsychotic-induced QT prolongation is suspected or evident. The British Heart Rhythm Society has issued the Clinical Practice Guidelines on the Management of Patients Developing QT Prolongation on Antipsychotic Medication to support them. The guidance is adapted from the most recent Maudsley Prescribing Guidelines in Psychiatry, issued in 2018.[1]
When considering the risk of death with schizophrenia, it is important to recognise that this condition carries a mortality from its psychiatric effects. Nearly one-third of the excess mortality in schizophrenia is attributable to a significantly higher risk of suicide – 5% risk over the patient’s lifetime – with an additional 12% due to accidental death. Antipsychotics reduce adverse outcomes on mortality in the schizophrenia population.[2–5]
The overall and cardiovascular mortality distributions follow a U-shaped curve in relation to antipsychotic dose with patients taking no medication and those taking the highest doses having the greatest mortality.
This indicates that antipsychotics can protect patients against the consequences of schizophrenia, including suicide, at low and medium cumulative doses; compliance is critical and high doses should be avoided.[6] Indeed, mortality is 40% lower in patients with schizophrenia who use antipsychotics than those who do not.
Long-acting injection (LAI) use is associated with an approximately 30% lower risk of death than oral use of the same medication, most probably because this ensures adherence and sustained drug action. Second-generation LAI antipsychotics and oral aripiprazole have the lowest mortality.[7]
The mortality data also indicate that people with schizophrenia have higher fatality rates due to natural causes than the general population in the US. Cardiovascular, respiratory and metabolic disorders are 2–3 times more prevalent in people with schizophrenia.[3,4] Some antipsychotics cause increased appetite and weight gain, and can also directly cause metabolic syndrome, dyslipidaemia, hypertension and insulin resistance, which probably leads to greater cardiac mortality rates. Unhealthy lifestyles, polypharmacy and suboptimal healthcare are all regarded as contributing factors to the risk of higher mortality.
Case-control studies have suggested that the use of most antipsychotics is associated with rate of sudden cardiac death that is two- to three-times higher than in the general population –15 per 10,000 years of drug exposure.[8–12] This is substantially lower than the mortality associated with uncontrolled psychosis.
Most antipsychotics (which are prescribed for schizophrenia and other psychoses, agitation, severe anxiety, mania and violent or dangerously impulsive behaviour) prolong the QT interval primarily through K channel blocking effects. QT prolongation increases the risk of torsades de pointes and sudden cardiac death, although the evidence base to suggest this is exponential is limited; there are exceptions in that some drugs prolong the QT interval but do not increase dispersion of repolarisation. However, more robust data indicate that, once the QTc interval is >500 ms, the risk of torsades de pointes in significantly increased.[11]
Accurate QT measurement may be challenging because the presence of U waves makes it difficult to determine the end of the T wave, but the QT interval can be easily measured using the ‘tangent method’ if automated measurement is not available or appears incorrect. Correct QT measurement is key to minimise the risks of over- or under-estimating the QT interval and wrongly stratifying patient risk.
To minimise inconsistencies, it is best to measure the tangent of the descending T wave to baseline in leads II or V5.[13,14] This technique has been found to be the most reproducible among experts and non-experts alike (Figure 1).
Figure 1. Tangent Method of QTc Measurement.
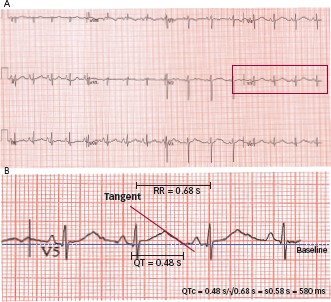
Leads II or V5 may be measured. The tangent of the downslope of the T wave is taken to the baseline of the ECG and the QT interval measured in seconds between the Q wave and point where the tangent hits the baseline. It is important to use seconds as the measurement rather than milliseconds in the calculation if using a calculator or the QTc value will be incorrect. An average of 3–5 beats should be measured. A number of online or mobile apps can be employed to simplify the calculation of QTc, including https://www.mdcalc.com/corrected-qt-interval-qtc and https://www.omnicalculator.com/health/qtc.
Many patients will have a resting tachycardia (>100/min) on medication so a correction for heart rate using the Fredericia formula (which uses the cube root of the RR interval) is recommended rather than Bazett’s as the latter will overestimate the QTc at higher heart rates. A simple online calculator to work out the QTc can be found at https://www.mdcalc.com/corrected-qt-interval-qtc. Regardless of which of these forumulae is used, detection of QTc >500 ms should prompt review.
Quantifying Risk
Drugs are categorised here according to data available on their effects on QTc (Table 1).
Table 1. The Effect of Psychotropics on QTc.
| No effect |
| Brexpiprazole (not available in UK) Cariprazine Lurasidone |
| Low effect (only in overdose or <10 ms increases in QTc) |
| Aripiprazole, amisulpride, asenapine, clozapine, flupentixol, fluphenazine perphenazine, prochlorperazine, olanzapine*, risperidone, sulpiride, loxapine, paliperidone, sulpiride |
| Moderate effect (>10 ms QT prolongation at clinical doses) |
| Amisulpride, chlorpromazine, levomepromazine, iloperidone, melperone, quetiapine, ziprasidone |
| High effect (>20 ms QTc prolongation at average clinical doses) |
| Pimozide, sertindole Any drug or combination of drugs used in doses exceeding recommended maximum |
*Isolated cases of QTc prolongation demonstrated effect on IKr,other data suggest no effect on QT.[19,22–24,34,40–42] Data on paliperidone are confusing (some suggest no effect) and recent data suggest aripiprazole prolongs QT to a small extent and is probably torsadogenic. Source: The Maudsley Prescribing Guidelines in Psychiatry.[1] Reproduced with permission from Wiley Blackwell.
In summary, currently the only antipsychotics not associated with QT prolongation are:
lurasidone;
cariprazine; and
brexpiprazole.
As a general rule, if the QTc is significantly prolonged (>500 ms) with no other reversible causes (see below) or any another antipsychotic, the patient should be switched to one of the three drugs above, but clinicians should be aware that the risk of relapse is increased to a small extent. The sole exception is clozapine – do not switch the patient from clozapine – the patient will relapse dramatically and quickly. Changing antipsychotic medications should be undertaken in consultation with the patient’s psychiatrist.
Action to be Taken According to QTc
A summary of management according to QTc is shown in Figure 2.
Figure 2. Summary of Management According to QTc.
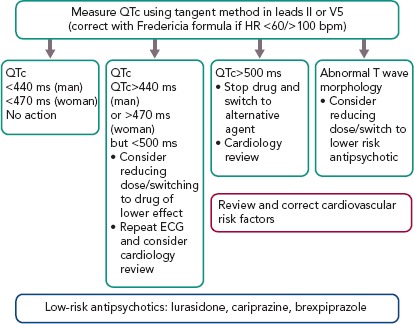
QTc <440 ms (Men) or <470 ms (Women)
No action required unless abnormal T-wave morphology – consider cardiac review if in doubt.
QTc >440 ms (Men) or >470 ms (Women), but <500 ms
Consider reducing dose or switching to drug of lower effect; repeat ECG and consider cardiology review.
QTc >500 ms
Stop suspected causative drug(s) and switch to drug with a lower effect: immediate cardiology review is needed. If the patient has syncope or pre-syncope, immediate ECG monitoring for ventricular arrhythmias should be performed.
Abnormal T-wave Morphology
Review treatment. Consider reducing dose or switching the patient to a lower risk antipsychotic, i.e. lurasidone, cariprazine or brexpiprazole.
Clozapine has a small effect on QTc. An implantable loop or closer 24-hour Holter recording may need to be considered if the QTc is persistently prolonged over 500 ms to check that the patient is not developing ventricular arrhythmias.
Cardiology review is necessary to specifically assess if the QTc measurement is accurate and there are no other factors leading to QT prolongation, including the cardiovascular risk factors or structural heart disease highlighted in Table 2.
Table 2. Physiological Risk Factors for QTc Prolongation and Arrhythmia.
| Cardiac |
| Long QT syndrome |
| Bradycardia |
| Ischaemic heart disease |
| Myocarditis |
| MI |
| Left ventricular hypertrophy |
| Metabolic |
| Hypokalemia |
| Hypomagnesaemia |
| Hypocalcaemia |
| Others |
| Extreme physical exertion |
| Extreme physical exertion |
| Anorexia nervosa |
| Extremes of age – children and elderly may be more susceptible to QT changes |
| Stress or shock |
| Female sex |
Note: Hypokalemia-related QTc prolongation is more commonly observed in acute psychotic admissions. Also, there are a number of physical and genetic factors which may not be discovered on routine examination, but which probably predispose patients to arrhythmia. Source: The Maudsley Prescribing Guidelines in Psychiatry.[1] Reproduced with permission from Wiley Blackwell.
Recommended Cardiology Assessment
A cardiology/electrophysiology expert review should consist of an ECG, echocardiography, 24-hour Holter and electrolyte monitoring, and liver function tests. If there are features in the history or investigations suggestive of coronary artery disease, it is prudent to undertake a CT coronary angiogram, as per National Institute for Health and Care Excellence guidance.[15]
Reversible causes of QT prolongation independent of the psychotropic drug effect should be assessed. These include other QT-prolonging drugs, agents that alter the metabolism of the antipsychotics to prolong half-life and electrolyte abnormalities (Table 3). If no reversible cause is identified apart form the antipsychotic drug, an alternative agent should be employed.
Table 3. Non-psychotropics Associated with QT Prolongation.
| Antibiotics |
| Erythromycin |
| Clarithromycin |
| Ampicillin |
| Co-trimoxazole |
| Pentamidine |
| Some 4-quinolones affect QTc – see manufacturers’ literature |
| Antimalarials |
| Chloroquine |
| Mefloquine |
| Quinine |
| Antiarrhythmics |
| Quinidine |
| Disopyramide |
| Procainamide |
| Sotalol |
| Amiodarone |
| Bretylium |
| Other Medication |
| Amantadine |
| Cyclosporin |
| Diphenhydramine |
| Hydroxyzine |
| Nicardipine |
| Tamoxifen |
| Note: Beta 2 agonists and sympathomimetics may provoke torsades de pointes in patients with prolonged QTc. |
| ECG Monitoring |
Measure QTc in all patients prescribed antipsychotics:
|
| Metabolic Inhibition |
| The effect of drugs on the QTc interval is usually plasma level-dependent. Drug interactions are therefore important, especially when metabolic inhibition results in increased plasma levels of the drug affecting QTc. Commonly used metabolic inhibitors include fluvoxamine, fluoxetine, paroxetine and valproate. |
Source: Adapted from the Maudsley Prescribing Guidelines in Psychiatry.1Used with permission from Wiley Blackwell.
Consideration should be given to inherited causes of QT prolongation; a significant proportion of drug-induced cases with a large degree of QT prolongation are associated with ion channel mutations.[16] This can be evaluated by assessing persistent features of repolarisation abnormalities after stopping the drug for five half lives and examining the family history to see if there are any indications to suggest an inherited channelopathy, e.g. family history of sudden death at a young age, cot death, epilepsy, congenital deafness as well as ion channel mutation testing when clinically indicated (see the section in the Heart Rhythm Society guidelines on gene testing for inherited arrhythmias).[17]
Other cardiovascular risk factors such as smoking, obesity and impaired glucose tolerance should be considered, because they may present a much greater risk to patient morbidity and mortality than the uncertain outcome of QT changes. These should be managed accordingly, e.g. with statin treatment as per current guidelines.
ICD Implantation
There are no systematic data on the use of prophylactic pacing or ICDs in this population and therefore it is not addressed in the current Heart Rhythm Society and European Society of Cardiology guidelines, which focus on minimising QT prolongation.
Device implantation in such patients may be difficult because their mental state may affect their ability to tolerate an ICD, which may exacerbate their psychiatric condition. The decision to implant an ICD therefore requires careful consideration. Prophylactic ICD implantation may be considered if the patient is developing non-sustained torsades de pointes or the QTcs are consistently very prolonged (e.g. >550 ms), or if a reversible cause such as stopping the antipsychotic is contraindicated due to the severity of the psychiatric condition.
Secondary prevention for out-of-hospital cardiac arrest or sustained haemodynamically compromising ventricular arrhythmias is appropriate if a reversible cause cannot be corrected and the patient is able to accept an ICD and comply with follow-up, which may be easier in the current era of home monitoring.
A dual chamber device to enable atrial pacing at 70–80 BPM and minimise QT prolongation or short-long-short pauses to trigger to torsades de pointes is advisable, although emerging data describe subcutaneous ICDs being employed in people with long QT syndrome.
In cases where symptoms of pre-syncope or syncope are suspected due to ventricular arrhythmias, an implantable loop recorder may be considered (if the patient is amenable) to correlate symptoms with arrhythmia and hence guide management.
General Principles
Assume all antipsychotics carry an increased risk of sudden cardiac death.
Prescribe the lowest antipsychotic dose possible and avoid polypharmacy/metabolic interactions.
Perform ECG on admission, before discharge and at yearly check-up.
Consider measuring QTc within a week of reaching therapeutic doses of moderate-/high-risk antipsychotics.
References
- 1.Taylor DM, Barnes TRE, Young AH. Maudsley Prescribing Guidelines in Psychiatry. 13th edition. Chichester: Wiley Blackwell 2018
- 2.Brown S. Excess mortality of schizophrenia. A meta-analysis. Brit J Psychiatry. 1997;171:502–8. doi: 10.1192/bjp.171.6.502. [DOI] [PubMed] [Google Scholar]
- 3.Casey DE. Metabolic issues and cardiovascular disease in patients with psychiatric disorders. Am J Med. 2005;118 (Suppl 2):12S–22S. doi: 10.1016/j.amjmed.2005.01.046. [DOI] [PubMed] [Google Scholar]
- 4.Enger C, Weatherby L, Reynolds RF et al. Serious cardiovascular events and mortality among patients with schizophrenia. J Nerv Ment Dis. 2004;192:19–27. doi: 10.1097/01.nmd.0000105996.62105.07. [DOI] [PubMed] [Google Scholar]
- 5.Torniainen M, Mittendorfer-Rutz E, Tanskanen A et al. Antipsychotic treatment and mortality in schizophrenia. Schizophr Bull. 2015;41:656–63. doi: 10.1093/schbul/sbu164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Taipale H, Mittendorfer-Rutz E, Alexanderson K et al. Antipsychotics and mortality in a nationwide cohort of 29,823 patients with schizophrenia. Schizophr Res. 2018;197:274–80. doi: 10.1016/j.schres.2017.12.010. [DOI] [PubMed] [Google Scholar]
- 7.Reilly JG, Ayis SA, Ferrier IN et al. Thioridazine and sudden unexplained death in psychiatric in-patients. Br J Psychiatry. 2002;180:515–22. doi: 10.1192/bjp.180.6.515. [DOI] [PubMed] [Google Scholar]
- 8.Hennessy S, Bilker WB, Knauss JS et al. Cardiac arrest and ventricular arrhythmia in patients taking antipsychotic drugs: cohort study using administrative data. BMJ. 2002;325:1070. doi: 10.1136/bmj.325.7372.1070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Straus SM, Bleumink GS, Dieleman JP et al. Antipsychotics and the risk of sudden cardiac death. Arch Intern Med. 2004;164:1293–7. doi: 10.1001/archinte.164.12.1293. [DOI] [PubMed] [Google Scholar]
- 10.Liperoti R, Gambassi G, Lapane KL et al. Conventional and atypical antipsychotics and the risk of hospitalization for ventricular arrhythmias or cardiac arrest. Arch Intern Med. 2005;165:696–701. doi: 10.1001/archinte.165.6.696. [DOI] [PubMed] [Google Scholar]
- 11.Ray WA, Chung CP, Murray KT et al. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med. 2009;360:225–35. doi: 10.1056/NEJMoa0806994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Malik M, Camm AJ. Evaluation of drug-induced QT interval prolongation: implications for drug approval and labelling. Drug Saf. 2001;24:323–51. doi: 10.2165/00002018-200124050-00001. [DOI] [PubMed] [Google Scholar]
- 13.Botstein P. Is QT interval prolongation harmful? A regulatory perspective. Am J Cardiol. 1993;72:B50–2. doi: 10.1016/0002-9149(93)90041-A. [DOI] [PubMed] [Google Scholar]
- 14.Postema PG, De Jong JS, Van der Bilt IA, Wilde AA. Accurate electrocardiographic assessment of the QT interval: teach the tangent. Heart Rhythm. 2008;5:1015–8. doi: 10.1016/j.hrthm.2008.03.037. [DOI] [PubMed] [Google Scholar]
- 15.London: NICE: 2010. National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis.www.nice.org.uk/cg95 Available at. (accessed 12 June 2019) [PubMed] [Google Scholar]
- 16.Itoh H, Sakaguchi T, Ding WG et al. Latent genetic backgrounds and molecular pathogenesis in drug-induced long-QT syndrome. Circ Arrhythm Electrophysiol. 2009;2:511–23. doi: 10.1161/CIRCEP.109.862649. [DOI] [PubMed] [Google Scholar]
- 17.Priori SG, Wilde AA, Horie M et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013. Heart Rhythm. 2013;10:1932–63. doi: 10.1016/j.hrthm.2013.05.014. [DOI] [PubMed] [Google Scholar]
- 18.Haddad PM, Anderson IM. Antipsychotic-related QTc prolongation, torsade de pointes and sudden death. Drugs. 2002;62:1649–71. doi: 10.2165/00003495-200262110-00006. [DOI] [PubMed] [Google Scholar]
- 19.Taylor DM. Antipsychotics and QT prolongation. Acta Psychiatr Scand. 2003;107:85–95. doi: 10.1034/j.1600-0447.2003.02078.x. [DOI] [PubMed] [Google Scholar]
- 20.Glassman AH, Bigger JT Jr. Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death. Am J Psychiatry. 2001;158:1774–82. doi: 10.1176/appi.ajp.158.11.1774. [DOI] [PubMed] [Google Scholar]
- 21.Warner B, Hoffmann P. Investigation of the potential of clozapine to cause torsade de pointes. Adverse Drug React Toxicol Rev. 2002;21:189–203. doi: 10.1007/BF03256196. [DOI] [PubMed] [Google Scholar]
- 22.Harrigan EP, Miceli JJ, Anziano R et al. A randomized evaluation of the effects of six antipsychotic agents on QTc, in the absence and presence of metabolic inhibition. J Clin Psychopharmacol. 2004;24:62–9. doi: 10.1109/MM.2004.1269000. [DOI] [PubMed] [Google Scholar]
- 23.Lindborg SR, Beasley CM, Alaka K, Taylor CC. Effects of intramuscular olanzapine vs haloperidol and placebo on QTc intervals in acutely agitated patients. Psychiatry Res. 2003;119:113–23. doi: 10.1016/S0165-1781(03)00107-0. [DOI] [PubMed] [Google Scholar]
- 24.Dineen S, Withrow K, Voronovitch L et al. QTc prolongation and high-dose olanzapine. Psychosomatics. 2003;44:174–5. doi: 10.1176/appi.psy.44.2.174. [DOI] [PubMed] [Google Scholar]
- 25.Gupta S, Nienhaus K, Shah SA. Quetiapine and QTc issues: a case report. J Clin Psychiatry. 2003;64:612–3. doi: 10.4088/JCP.v64n0518e. [DOI] [PubMed] [Google Scholar]
- 26.Su KP, Shen WW, Chuang CL et al. A pilot cross-over design study on QTc interval prolongation associated with sulpiride and haloperidol. Schizophr Res. 2003;59:93–4. doi: 10.1016/S0920-9964(01)00336-X. [DOI] [PubMed] [Google Scholar]
- 27.Lin CH, Chen MC, Wang SY, Lin CY. Predictive factors for QTc prolongation in schizophrenic patients taking antipsychotics. J Formos Med Assoc. 2004;103:437–41. [PubMed] [Google Scholar]
- 28.Chong SA, Mythily Lum A et al. Prolonged QTc intervals in medicated patients with schizophrenia. Hum Psychopharmacol. 2003;18:647–9. doi: 10.1002/hup.540. [DOI] [PubMed] [Google Scholar]
- 29.Krantz MJ, Kutinsky IB, Robertson AD, Mehler PS. Dose-related effects of methadone on QT prolongation in a series of patients with torsade de pointes. Pharmacotherapy. 2003;23:802–5. doi: 10.1592/phco.23.6.802.32186. [DOI] [PubMed] [Google Scholar]
- 30.Gil M, Sala M, Anguera I et al. QT prolongation and torsades de pointes in patients infected with human immunodeficiency virus and treated with methadone. Am J Cardiol. 2003;92:995–7. doi: 10.1016/S0002-9149(03)00906-8. [DOI] [PubMed] [Google Scholar]
- 31.Piguet V, Desmeules J, Ehret G et al. QT interval prolongation in patients on methadone with concomitant drugs. J Clin Psychopharmacol. 2004;24:446–8. doi: 10.1097/01.jcp.0000132347.81455.57. [DOI] [PubMed] [Google Scholar]
- 32.Stollberger C, Huber JO, Finsterer J. Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005;20:243–51. doi: 10.1097/01.yic.0000166405.49473.70. [DOI] [PubMed] [Google Scholar]
- 33.Isbister GK, Murray L, John S et al. Amisulpride deliberate self-poisoning causing severe cardiac toxicity including QT prolongation and torsades de pointes. Med J Aust. 2006;184:354–6. doi: 10.5694/j.1326-5377.2006.tb00272.x. [DOI] [PubMed] [Google Scholar]
- 34.Ward DI. Two cases of amisulpride overdose: a cause for prolonged QT syndrome. Emerg Med Australas. 2005;17:274–6. doi: 10.1111/j.1742-6723.2005.00734.x. [DOI] [PubMed] [Google Scholar]
- 35.Vieweg WV, Schneider RK, Wood MA. Torsade de pointes in a patient with complex medical and psychiatric conditions receiving low-dose quetiapine. Acta Psychiatr Scand. 2005;112:318–22. doi: 10.1111/j.1600-0447.2005.00592.x. [DOI] [PubMed] [Google Scholar]
- 36.Huang BH, Hsia CP, Chen CY. Sulpiride induced torsade de pointes. Int J Cardiol. 2007;18:e100–2. doi: 10.1016/j.ijcard.2007.01.060. [DOI] [PubMed] [Google Scholar]
- 37.Kane JM, Lauriello J, Laska E et al. Long-term efficacy and safety of iloperidone: results from 3 clinical trials for the treatment of schizophrenia. J Clin Psychopharmacol. 2008;28 (Suppl 1):S29–35. doi: 10.1097/JCP.0b013e318169cca7. [DOI] [PubMed] [Google Scholar]
- 38.Kim MD, Eun SY, Jo SH. Blockade of HERG human K+ channel and IKr of guinea pig cardiomyocytes by prochlorperazine. Eur J Pharmacol. 2006;544:82–90. doi: 10.1016/j.ejphar.2006.06.009. [DOI] [PubMed] [Google Scholar]
- 39.Meltzer H, Bobo WV, Nuamah IF et al. Efficacy and tolerability of oral paliperidone extended-release tablets in the treatment of acute schizophrenia: pooled data from three 6-week placebo-controlled studies. J Clin Psychiatry. 2006;69:817–29. doi: 10.4088/jcp.v69n0515. [DOI] [PubMed] [Google Scholar]
- 40.Su KP, Lane HY, Chuang CL et al. Olanzapine-induced QTc prolongation in a patient with Wolff-Parkinson-White syndrome. Schizophr Res. 2004;66:191–2. doi: 10.1016/S0920-9964(03)00182-8. [DOI] [PubMed] [Google Scholar]
- 41.Morissette P, Hreiche R, Mallet L et al. Olanzapine prolongs cardiac repolarization by blocking the rapid component of the delayed rectifier potassium current. J Psychopharmacol. 2007;21:735–41. doi: 10.1080/02680930600969308. [DOI] [PubMed] [Google Scholar]
- 42.Bär KJ1, Koschke M, Berger S et al. Influence of olanzapine on QT variability and complexity measures of heart rate in patients with schizophrenia. J Clin Psychopharmacol. 2008;28:694–8. doi: 10.1097/JCP.0b013e31818a6d25. [DOI] [PubMed] [Google Scholar]