

Abstract
Hemorrhage associated with meningiomas is extremely rare and most commonly occurs in convexity meningiomas of higher grade or the angioblastic variety. Moreover, bleeding associated with a meningioma usually occurs in the form of a subdural hematoma or subarachnoid hemorrhage. We report a case of giant left medial sphenoid wing meningioma with histopathological diagnosis of a meningothelial type with apoplexy. A 54-year-old female presented with clinical features suggestive of apoplexy. Her neuroimaging demonstrated a large left medial sphenoid wing meningioma with features suggestive of an intratumoral bleed with mass effect. Gross total excision of the tumor was done with the good postoperative outcome. The biopsy came out to be Grade I meningothelial meningioma. Apoplexy in meningiomas is extremely rare with a reported incidence of 0.5%–2.4%, especially in a nonconvexity meningioma with histopathological diagnosis of meningothelial variety. Early diagnosis and prompt surgical intervention are critical as meningiomas associated with apoplexy are associated with high morbidity.
Keywords: Intratumoral hemorrhage, meningioma, meningothelial, nonconvexity, sphenoid wing
Introduction
While spontaneous intratumoral hemorrhage is commonly associated with intracranial malignant lesions such as parenchymal metastasis and glioblastoma, it remains rare in benign intracranial tumors.[1] Hemorrhage associated with meningiomas is extremely rare with an estimated incidence of around 2.4% and most commonly takes the form of a subdural or a subarachnoid hemorrhage.[2] Spontaneous intratumoral hemorrhage (ITH) in meningiomas remains an extremely rare but a potentially fatal complication.[1,2,3,4] Spontaneous intratumoral bleed in meningiomas, hitherto, had been described in convexity meningiomas of usually angioblastic type or high grade. Herein, we describe a case of giant left medial sphenoid wing meningioma with ITH and its successful management with a brief review of the literature.
Case Report
A 54-year-old female presented with the complaints of sudden onset severe headache associated with recurrent episodes of vomiting 3 months back followed by a complete recovery. The patient subsequently experienced two episodes of right faciobrachial motor seizures with secondary generalization after 1 month and progressive right hemiparesis since then, leading to admission under our care. On examination, there was a motor weakness of upper motor neuron type on the right side (Medical Research Council Grade 3/5) with right-sided extensor plantar reflex. Besides, fundoscopy revealed bilateral papilledema.
On computed tomogram done at a local center, a hyperdense ovoid mass lesion was seen in the medial temporal lobe area [Figure 1a]. On magnetic resonance imaging (MRI), the lesion suggestive of a left medial sphenoid wing meningioma with bleed was found. The lesion showed a small area of peripheral T1 hyperintensity, while on T2 imaging, the lateral periphery of the tumor showed T2 hypointense cap which showed strong blooming artifact on susceptibility image [Figure 1b–d]. The tumor showed a mass effect on the surrounding structures and enhanced homogenously with nonenhancing cores in between [Figure 1e–g]. Coronal and sagittal images pointed toward a possible basal attachment on the temporal dura and the dura over the sphenoid wing [Figure 1f and g]. Computed tomographic angiogram ruled out an aneurysm as a likely pathology.
Figure 1.

Computed tomography scan of the head performed after the acute episode of a headache showing an ovoid left medial temporal mass lesion. The hyperdensity is not uniform, and there is a pocket of hypodense area posteriorly (a). The lesion on magnetic resonance imaging appears bigger and is hypointense on T1 except for a small hyperdensity posteriorly, whereas it is isointense on T2 image and capped by a hypointense area toward the cerebral convexity, the latter showing blooming on susceptibility-weighted image (b-d). The lesion shows strong but inhomogeneous enhancement (e-g). The center and the posterolateral periphery of the lesion does not enhance at all. Moreover, the nonenhancing portions are capped by another layer of nonenhancing tissue, possibly blood clot (e-g)
The patient was taken up for surgery through a left frontotemporal craniotomy. The lesion appeared extra-axial, encapsulated, dusky brown, based on the sphenoid wing and the temporal base. There was xanthochromic staining around the tumor and the tumor–brain interface. The tumor was removed entirely after carefully dissecting the underlying middle cerebral artery. The dural base was generously coagulated to ensure Grade 2 Simpson's excision [Figure 2a].
Figure 2.
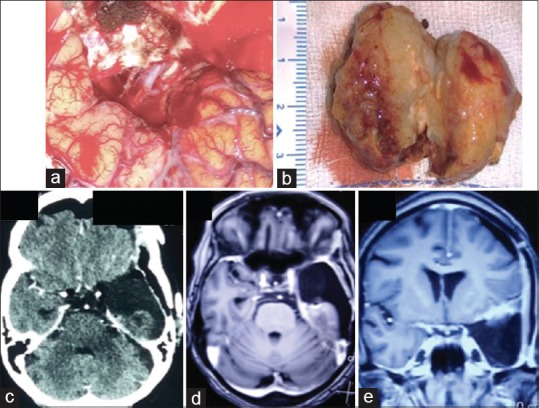
Postexcision surgical cavity with an internal carotid artery with its bifurcation, optic nerve, and oculomotor nerves visualized at the free edge of the tentorium (a). The specimen showing hemorrhage peripherally with an otherwise fleshy, nonnecrotic interior (b). Postoperative computed tomography (done within 24 h of surgery) as well magnetic resonance imaging (done after two months) showing evidence of gross total tumor excision (c-e)
The specimen was rounded and encapsulated, and the cut section showed a fleshy interior with evidence of bleed in the subcapsular peripheral region [Figure 2b]. Histopathological findings were consistent with the diagnosis of a meningothelial meningioma with the areas of hemorrhagic degeneration and coagulative necrosis. There were no mitotic figures, cellular atypia, or microscopic brain invasion.
Postoperatively, the patient developed transient oculomotor nerve paresis, but the hemiparesis gradually improved by one grade at the time of discharge. Postoperative computed tomogram scan showed a complete tumor excision and a well-formed surgical cavity [Figure 2c].
At 2-month follow-up, the patient can self-ambulate (power improved to 4+/5) with partial oculomotor paresis persisting. Contrast MRI showed a complete tumor excision [Figure 2d and e].
Discussion
Meningiomas usually present with a long-standing history of headache and seizures and less commonly with neurological deficits. Acute symptomatology, particularly heralding the presence of an intracranial meningioma, is very rare in clinical practice. Such a presentation generally points toward an underlying vascular pathology which may range from an aneurysm rupture to hypertensive intracranial hemorrhage.[5,6]
Hemorrhage or apoplexy inside intracranial tumors is observed explicitly in malignant lesions such as metastases and glioblastomas.[1] Certain benign tumors such as oligodendrogliomas and pituitary adenomas may also show ITH. Apoplexy in meningiomas is extremely rare with a reported incidence of 0.5%–2.4%.[2] Most hemorrhages reported with intracranial meningiomas are subdural (SDH), subarachnoid (SAH), or intraventricular hemorrhages. Massive hemorrhages inside the tumor, the so-called ITH, in meningioma are exceptionally uncommon.[1,3,4] SDH is usually associated with convexity location, whereas SAH is commonly seen with parasagittal and falcine meningioma.[2]
Bosnjak et al.[2] reported on 145 patients of intracranial meningiomas associated with hemorrhage and found that meningiomas in patients aged either more than 70 years or <30 years had a higher risk. They noted a higher propensity for fibrous, transitional, and angiomatous meningiomas to show this complication. Various postulations are available for this rare phenomenon: compensatory vascular dilatation, neovascular formation, vascular erosion, intratumoral necrosis, trauma, etc.[1,2,7,8] The exact etiopathogenesis of bleed in our case is difficult to explain as the lesion proved to be a Grade 1 meningothelial meningioma on histopathology, and such presentation is very rare in the pathology mentioned above. The most likely cause for the ITH in our case may be attributed to the ill-formed new blood vessels which bled or the vascular erosion caused by the tumor.
Our patient developed pure ITH, as evident by the intact tumor capsule all around tumor radiologically as well as intraoperatively. The hemorrhage was located at the periphery, contained by the capsule. This type of hemorrhage has been described to be dangerous as capsular rupture can lead to intracerebral/subarachnoid extension as compared to hemorrhages located at the center. Kuzeyli et al.[1] noted that microcystic and micronecrotic changes are the primary underlying pathological weaklings predisposing to ITH in meningiomas. It is worthwhile to note that the incidence of microscopic hemorrhages inside the tumor is very high and only a tiny subset of these patients present with radiologically evident bleed.[1]
Hemorrhage associated with meningioma is associated with nearly 41% mortality.[1,2] The extent of hemorrhage and the status of consciousness before surgery are considered significant predictors of outcome. Bosnjak et al.[2] noted that a very high percentage of these patients develop major morbidity even if they survive. Our patient was perhaps lucky in that the hemorrhage was contained inside the tumor by its capsule and she did not have a repeat hemorrhage before surgery. The key to success in these patients is early diagnosis and prompt surgical excision of the tumor and the hematoma.[1,2,9]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kuzeyli K, Cakir E, Usul H, Karaarslan G, Yazar U, Baykal S, et al. Intratumoral haemorrhage: A clinical study. J Clin Neurosci. 2004;11:490–2. doi: 10.1016/j.jocn.2003.10.012. [DOI] [PubMed] [Google Scholar]
- 2.Bosnjak R, Derham C, Popović M, Ravnik J. Spontaneous intracranial meningioma bleeding: Clinicopathological features and outcome. J Neurosurg. 2005;103:473–84. doi: 10.3171/jns.2005.103.3.0473. [DOI] [PubMed] [Google Scholar]
- 3.Lin RH, Shen CC. Meningioma with purely intratumoral hemorrhage mimicked intracerebral hemorrhage: Case report and literature review. J Med Sci. 2016;36:158–61. [Google Scholar]
- 4.Mangubat EZ, Byrne RW. Major intratumoral hemorrhage of a petroclival atypical meningioma: Case report and review of literature. Skull Base. 2010;20:469–74. doi: 10.1055/s-0030-1261266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nguyen HS, Doan N, Eckardt G, Gelsomino M, Shabani S, Brown WD, et al. A completely thrombosed, nongiant middle cerebral artery aneurysm mimicking an intra-axial neoplasm. Surg Neurol Int. 2015;6:146. doi: 10.4103/2152-7806.164696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kim YJ, Jeun SS, Park JH. Thrombosed large middle cerebral artery aneurysm mimicking an intra-axial brain tumor: Case report and review of literature. Brain Tumor Res Treat. 2015;3:39–43. doi: 10.14791/btrt.2015.3.1.39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang HC, Wang BD, Chen MS, Li SW, Chen H, Xu W, et al. An underlying pathological mechanism of meningiomas with intratumoral hemorrhage: Undifferentiated microvessels. World Neurosurg. 2016;94:319–27. doi: 10.1016/j.wneu.2016.07.042. [DOI] [PubMed] [Google Scholar]
- 8.Niiro M, Ishimaru K, Hirano H, Yunoue S, Kuratsu J. Clinico-pathological study of meningiomas with haemorrhagic onset. Acta Neurochir (Wien) 2003;145:767–72. doi: 10.1007/s00701-003-0089-z. [DOI] [PubMed] [Google Scholar]
- 9.Vij M, Jaiswal S, Jaiswal AK, Kumar S, Behari S. Meningioma with hemorrhagic onset: Two case reports. J Cancer Res Ther. 2012;8:145–7. doi: 10.4103/0973-1482.95198. [DOI] [PubMed] [Google Scholar]