

Abstract
Background:
During the surgery for intrinsic brain lesions, it is important to plan the proper site of the craniotomy and to identify the relations with the gyri and superficial veins. This might be a challenge, especially in small subcortical lesions and when there is a distortion of the cortical anatomy.
Materials and Methods:
Using the free computer software Osirix, we have created a 3-dimensional reconstruction of the head and cerebral showing the gyri and superficial veins. With the aid of some tools, it is possible to create a colored image of the lesion and also to calculate the distance between the areas of interest and some easily identifiable structure, making it easier to plan the site of the craniotomy identify the topography of the lesion.
Results:
The reconstructions were compared to the intraoperative view. We found this technique to be useful to help identify the gyri and cortical veins and use them to find the lesions. The use of a region of interest to show better the lesion under the cortical surface and in the three-dimensional reconstruction of the head was also helpful.
Conclusions:
This is a low-cost and easy technique that can be quickly learned and performed before every surgery. It helps the surgeon to plan a safe craniotomy and lesionectomy.
Keywords: Gyrus, medical topography, neuroanatomy, sulcus, surgical procedure
Introduction
The correct position of the craniotomy and the study of the anatomic relations of the lesion with the neural structures around it are of great importance for modern neurosurgery.[1] Many craniometric references have been correlated with different underlying gyri and sulci, and accurate knowledge of these references is helpful in assessing the extracranial projection of intracranial lesions.[2]
One option is the use of neuronavigation, idealized in 1987,[3] is a very important tool in the surgical planning for brain tumors,[4,5] the method is very useful and accurate, the main problem is the brain shift during the surgery;[6,7,8] unfortunately, it is not widely available worldwide.
The use of three-dimensional (3D) reconstruction has been previously reported for surgical planning but using techniques that are not widely available and cannot be performed by the surgeon, but showing that it could be helpful to identify key structures and perform a safer procedure.[9] Recently, there have been reports of the use of Osirix for surgical planning in traumatic brain injury,[1] the study of cranial and central nervous system relations.[10]
Harput et al. published in 2014, the use of Osirix for surgical planning for neocortical supratentorial lesions comparing the results with surgical view, with good accuracy.[11]
In this article, we use the previous technique adding two more steps. The first one is using the region of interests (ROIs) to make a color reconstruction of the lesion to make it easier to visualize in the head while planning the approach and also in the cortical surface to make it possible to see small subcortical lesions. The second is the use of measuring tools to plan the site of the craniotomy in the 3D head.
Materials and Methods
Patients signed an informed consent and underwent scans with 1.5T magnetic resonance scanner, the sequences used for the reconstruction were volumetric T1 both nonenhanced and enhanced with gadolinium. All images in Digital Imaging and Communications in Medicine (DICOM) files were transferred to a MacBook Pro 2.9 GHz Intel Core i7. We then used the Osirix Medical Image Software Lite v 7.5, a free version available for download on their website.
The sequence without gadolinium is used for the brain surface reconstruction showing the sulci and gyri, and the gadolinium-enhanced sequences were used to appreciate the anatomic relationship between the cortical vessels and the underlying cerebral cortex.[11]
After selecting the DICOM files of the desired patient, the reconstruction begins double-clicking the desired sequence and it will be shown in 2D, for small subcortical lesions that are sometimes impossible to show in the normal reconstruction, select the pencil tool and draw the borders of the lesion on every slice of the sequence. Then click on the ROI menu and select the ROI rename, click on the option “all ROIs in this series” and name it [Figure 1]. Now, using that same menu, it is possible to use the option ROI volume to compute the volume of the lesion if desired [Figure 1].
Figure 1.

(a) Use the pencil tool to draw the lesion in every slice of the sequence, click on the region of interest menu, and select region of interest rename, (b) select all region of interests in this series and chose the name, (c) after the three-dimensional reconstruction open the region of interest menu and click on region of interest manager, then select the preciously named region of interest, (d) using the adjust brightness and contrast to show both the superficial layers and the reconstruction of the lesion. The arrow shows a small cavernous hemangioma
Using the 2D/3D-reconstruction tools, select the 3D-volume rendering option. Then, a 3D reconstruction of the whole cranial space will appear on the main screen, adjust brightness, and contrast to achieve the desired color and tissue density. To plan the site of the craniotomy open the ROI, click on the ROI manager and chose the name of the region chosen before, this will make a colored reconstruction of the lesion inside the 3D head, and adjusting again the contrast, it can be easily seen. Now, it is possible to use the tool to measure distances from the lesion to easily identifiable structures on the surface of the head, for example, the tragus [Figure 2].
Figure 2.
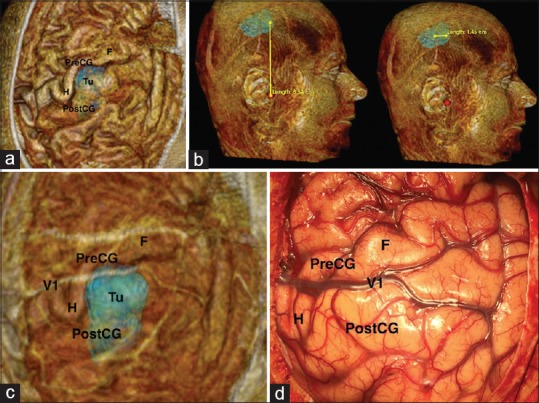
(a) Non-enhanced reconstruction showing the cortical surface, (b) use of length measurement tool to program the approach, (c) superposition of the reconstruction simulating intraoperative findings, (d) surgical picture. V1 – cortical vein; Pre-CG – precentral gyrus; Post-CG – postcentral gyrus; H – motor area of the hand; F – motor area of the face; Tu – Tumor
The next step consists of removing the skin, fat, bone, and dura. That can be achieved cropping the contralateral side of the head and then using simple tools including move, rotate and sculpt, identify the layers, and peel them away. The previously described technique of ROI reconstruction can also be used to show the site of a subcortical lesion under the brain surface [Figure 3].
Figure 3.

After selecting the desired sequence for the reconstruction (a) using the two-dimensional/three-dimensional reconstruction tool select the three-dimensional volume rendering option, (b) adjust brightness and contrast to achieve the desired color and tissue density, (c) crop the side of the head contralateral to the lesion, (d) use the tools to rotate, move and sculpt and remove the layers
The last step is to position this 3D-reconstruction simulating the surgical position, and then, it can be saved by adding it as the fly-through point and exporting and saving it in the desired folder. The same procedure is then performed in the gadolinium-enhanced sequences and after the superficial layers are removed this file can be reimported as the fly-through point. This will match the new reconstruction in the exact position and size of the nonenhanced previously saved.
When these two images are exported as jpg files, the gadolinium-enhanced image can be placed over the non-enhanced image with any image-processing software, such as Photoshop or any presentation software such as Keynote or PowerPoint. Then, by decreasing and increasing the opacity of the upper image, the dense vascular cortical net becomes the surgical landmark for realizing the sulcal and gyral anatomy surrounding the tumor, and for the small subcortical lesions, the colored reconstruction using ROIs also show them by transparency and its relations with the cerebral sulci and superficial veins.
Results and Illustrative Cases
Case 1
A 38-year-old woman with partial seizures on the right side, the magnetic resonance imaging (MRI) shows a small cavernous hemangioma underneath the precentral gyrus of the left side. The patient was admitted for surgical resection. The reconstruction showed the lesion under the precentral gyrus just behind the middle frontal gyrus, two cortical veins near the lesions were used to navigate during the surgery. A small craniotomy was performed and the intraoperative findings were compared to the reconstructions [Figure 4]. The lesion was successfully removed, and the patient had an improvement on seizure control [Figure 5].
Figure 4.
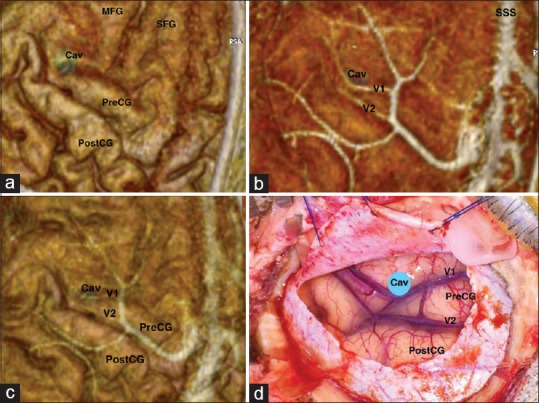
(a) Non-enhanced reconstruction showing the cortical surface, (b) gadolinium-enhanced reconstruction showing the cortical veins, (c) superposition of the reconstruction simulating intraoperative findings, (d) surgical picture. MFG – middle frontal gyrus; SFG – superior frontal gyrus; Cav – cavernous hemangioma; Pre-CG – precentral gyrus; Post-CG – postcentral gyrus; V1 – cortical vein one; V2 – cortical vein 2
Figure 5.
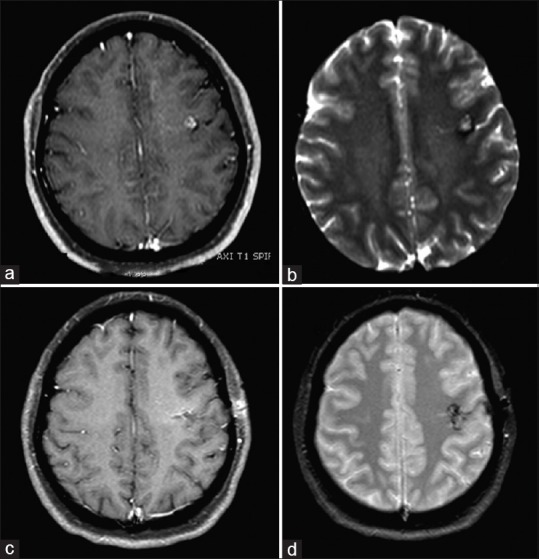
(a) preoperative contrast-enhanced T1-weighted magnetic resonance imaging, (b) preoperative T2-weighted magnetic resonance imaging, (c) postoperative contrast-enhanced T1-weighted magnetic resonance imaging, (d) postoperative T2-weighted magnetic resonance imaging
Case 2
A 60-year-old woman with a history of ovarian cancer presented with motor deficit on the left side. MRI showed a tumor near the postcentral gyrus on the right side. The reconstruction showed the tumor under the postcentral gyrus and superficial veins that were helpful to localize the lesion. Furthermore, the site of the motor gyrus knows as omega that corresponds to the area responsible for hand movement was easily identified and confirmed through cortical stimulation. The patient was operated with an awake craniotomy using neurostimulation for brain mapping, thus the need of a big craniotomy for this case, and the site of the tumor was confirmed using intraoperative ultrasound [Figure 2]. The tumor was removed successfully, and the patient had no additional deficits [Figure 6].
Figure 6.
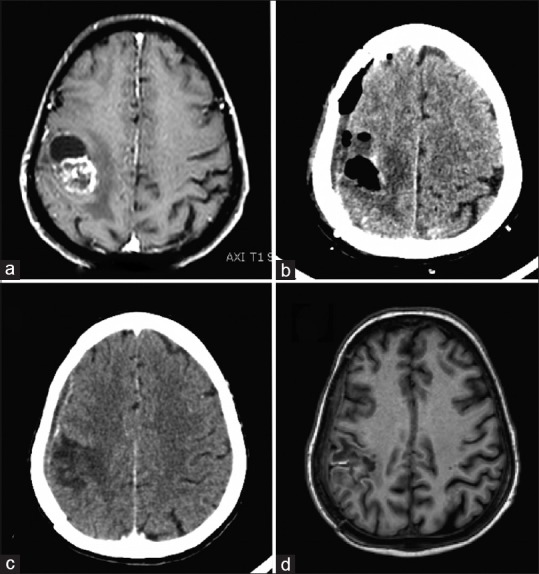
(a) Preoperative contrast-enhanced T1-weighted magnetic resonance imaging, (b) immediate postoperative computed tomography scan, (c) late postoperative computed tomography scan, (d) late postoperative T1-weighted magnetic resonance imaging
Discussion
The appropriate presurgical planning using a deep anatomical knowledge as well as craniometric points is important to perform a safe surgery. It is important to mentally correlate the preoperative cortical morphology and topography with the intraoperative findings; this is usually done studying multiplanar MRI images.[11,12]
Since the end of 1980s, the use of neuronavigation is an option, allowing the delineation of the tumors and identification of surrounding structures.[3] One problem is the cost of this system, making it not widely available in developing countries.
The use of a 3D reconstruction showing identifiable structures that can be used even to locate the lesion even after brain shift using the free version of the Osirix software is a low-cost option for planning a safer surgery. The method shows precise images of the gyral, sulcal, and cortical vascular patterns, and only takes a few minutes to be performed.[11] We added two steps to this reconstruction, one is using ROIs to make a colored reconstruction of the lesion, making it easier to visualize subcortical tumors, especially for small lesions. The other step is to use this same ROIs and measuring tools in the 3D reconstruction of the head to plan the site of the craniotomy using easily identifiable points in the head.
Another aim of the use of the Osirix's device is the possibility to estimating the exact location of the lesion, marking the lesion with the use of ROI dots, simulating the craniotomy in virtual space, simulating the skin incision, and the position of the tumor including in axial section. The planning of the surgery is based on the borders of the tumor and the size of the craniotomy after measuring the location of the tumor using the known in craniometric points. Therefore, the surgeon can project the borders of the tumor into the skin and mark these borders.[13]
Rotariu et al. have published a paper that proposes the use of the Osirix in endoscopic surgery. The images obtained using this method are high quality and have a good resemblance with the intraoperative images. The main advantage brought by the use of virtual endoscopic is the possibility to known the endoscopic anatomy, offers a prospective information about the anatomic variations and mainly define the position of the carotid artery and your relations with the sphenoid septum.[14]
We emphasize this is a low-cost option, and the surgeon only needs his own computer and a free software.[11] The process takes about 10 min and this time also helps to understand better the lesion the anatomy of the surrounding structures.
Conclusions
This freeware method using ROIs and surface reconstruction is a helpful tool to help programming the site of the craniotomy as well as to delineate the cortical projection of supratentorial lesions, even small subcortical ones. It can be an alternative in places where the neuronavigation is not available or in situations where there is no time for it. This method demands a profound knowledge of neuroanatomy and the relations between the skull and the central nervous system.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Mandel M, Amorim R, Paiva W, Prudente M, Teixeira MJ, Andrade AF. 3D preoperative planning in the ER with osiriX®: When there is no time for neuronavigation. Sensors (Basel) 2013;13:6477–91. doi: 10.3390/s130506477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ribas GC, Yasuda A, Ribas EC, Nishikuni K, Rodrigues AJ., Jr Surgical anatomy of microneurosurgical sulcal key points. Neurosurgery. 2006;59:ONS177–210. doi: 10.1227/01.NEU.0000240682.28616.b2. [DOI] [PubMed] [Google Scholar]
- 3.Watanabe E, Watanabe T, Manaka S, Mayanagi Y, Takakura K. Three-dimensional digitizer (neuronavigator): New equipment for computed tomography-guided stereotaxic surgery. Surg Neurol. 1987;27:543–7. doi: 10.1016/0090-3019(87)90152-2. [DOI] [PubMed] [Google Scholar]
- 4.Cho JM, Kim EH, Kim J, Lee SK, Kim SH, Lee KS, et al. Clinical use of diffusion tensor image-merged functional neuronavigation for brain tumor surgeries: Review of preoperative, intraoperative, and postoperative data for 123 cases. Yonsei Med J. 2014;55:1303–9. doi: 10.3349/ymj.2014.55.5.1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Orringer DA, Golby A, Jolesz F. Neuronavigation in the surgical management of brain tumors: Current and future trends. Expert Rev Med Devices. 2012;9:491–500. doi: 10.1586/erd.12.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nabavi A, Black PM, Gering DT, Westin CF, Mehta V, Pergolizzi RS, Jr, et al. Serial intraoperative magnetic resonance imaging of brain shift. Neurosurgery. 2001;48:787–97. doi: 10.1097/00006123-200104000-00019. [DOI] [PubMed] [Google Scholar]
- 7.Nimsky C, Ganslandt O, Cerny S, Hastreiter P, Greiner G, Fahlbusch R. Quantification of, visualization of, and compensation for brain shift using intraoperative magnetic resonance imaging. Neurosurgery. 2000;47:1070–9. doi: 10.1097/00006123-200011000-00008. [DOI] [PubMed] [Google Scholar]
- 8.Roberts DW, Hartov A, Kennedy FE, Miga MI, Paulsen KD. Intraoperative brain shift and deformation: A quantitative analysis of cortical displacement in 28 cases. Neurosurgery. 1998;43:749–58. doi: 10.1097/00006123-199810000-00010. [DOI] [PubMed] [Google Scholar]
- 9.Casey SO, Rubinstein D, Lillehei KO, Alberico RA, Ozsvath RR, Cajade-Law AG, et al. Integral and shell-MIP display algorithms in MR and CT three-dimensional models of the brain surface. AJNR Am J Neuroradiol. 1998;19:1513–21. [PMC free article] [PubMed] [Google Scholar]
- 10.Rahmah NN, Murata T, Yako T, Horiuchi T, Hongo K. Correlation between squamous suture and sylvian fissure: OSIRIX DICOM viewer study. PLoS One. 2011;6:e18199. doi: 10.1371/journal.pone.0018199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Harput MV, Gonzalez-Lopez P, Türe U. Three-dimensional reconstruction of the topographical cerebral surface anatomy for presurgical planning with free osiriX software. Neurosurgery. 2014;10(Suppl 3):426–35. doi: 10.1227/NEU.0000000000000355. [DOI] [PubMed] [Google Scholar]
- 12.Ono M, Kubik S, Abernathey CD. 1st ed. Stuttgart: George Thieme; 1990. Atlas of the Cerebral Sulci. [Google Scholar]
- 13.Spiriev T, Nakov V, Laleva L, Tzekov C. OsiriX software as a preoperative planning tool in cranial neurosurgery: A step-by-step guide for neurosurgical residents. Surg Neurol Int. 2017;8:241. doi: 10.4103/sni.sni_419_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rotariu DI, Ziyad F, Budu A, Poeata I. The role of osiriX based virtual endoscopy in planning endoscopic transsphenoidal surgery for pituitary adenoma. Turk Neurosurg. 2017;27:339–45. doi: 10.5137/1019-5149.JTN.16311-15.2. [DOI] [PubMed] [Google Scholar]