

Abstract
Introduction
We investigated in a prospective, observational trial the feasibility of using the Eustachian tube function test (ETFT) to measure the effect of repetitive pressure exposure during open seawater dives on Eustachian tube function.
Methods
The study included 28 adult divers during six consecutive days of diving in the Red Sea. Participants underwent otoscopy and ETFT before the first dive, between each dive and after the last dive. ETFT included regular tympanometry (R-tymp), tympanometry after Valsalva (V-tymp) and after swallowing (S-tymp). The R-tymp was obtained as 'baseline' peak pressure. After a Valsalva, the peak pressure should shift (positively), revealing a positive shift of the tympanic membrane. This pressure shift is defined here as R-VdP. The changes in compliance and peak pressure were recorded and correlated with otoscopic findings and diving experience. Middle ear barotrauma was scored using the Edmonds modified TEED scale.
Results
The 28 participants performed 437 dives. Positive shift of pressure in the middle ear was evident with significant changes from day one to day three (P < 0.0001). Divers with barotrauma showed significantly lower values of R-tymp peak pressure and significantly higher negative R-VdP, compared to divers with normal otoscopic findings (P < 0.05). Diving experience significantly correlated with R-tymp peak pressure and prevalence of middle ear barotrauma.
Conclusions
Significant changes in middle ear pressure and pressure equalization from repeated pressure exposure in saltwater were seen using ETFT. Repetitive, multi-day diving led to significantly decreased compliance and increased R-tymp peak pressure (overpressure) in the middle ear. Most profound changes were observed in less and intermediate experienced divers.
Keywords: Tympanometry, Middle ear, Ear barotrauma, Recreational diving
Introduction
Recreational scuba diving requires reliable and adequate pressure equalization in the middle ear. Rapidly increasing and decreasing the surrounding pressure during diving induces stress on the tympanic membrane (TM) and middle ear. The Eustachian tube (ET) is essential for drainage, protection and pressure equalization of the middle ear.[ 1 - 3] Pressure equalization occurs in both directions;[ 4 - 6] active pressure equalization is usually required during descent, whilst equalization is passive on ascent. Active equalization is supported by well-known musculature-involving manoeuvres such as swallowing, Valsalva or Toynbee.[ 4 - 6] Inadequate pressure equalization leads to consequent trauma of the middle ear mucosa, and TM and may impair ET function.[ 7 , 8] Corresponding pathological otoscopic findings such as hyperaemia, oedema, haemotympanum or even TM rupture characterize painful middle ear barotrauma (MEBt).[ 9 , 10]
Despite the rising popularity of recreational scuba diving,[ 7] the influence of repeated pressure changes on the middle ear and ET during scuba diving remains unclear. Challenging study conditions and the lack of reliable diagnostic methods might partly explain the low number of prospective, open-water studies. Whilst tympanometry remains one of the most commonly used diagnostic tools for assessing middle ear function in clinical otology and in basic research,[ 11] the Eustachian tube function test (ETFT) (based on the Williams inflation/deflation procedure[ 12 - 14] takes this a step further, using a series of three tympanometric measurements.
The primary objective of this trial was to evaluate changes in ET function and pressure equalization of the middle ear after repetitive saltwater dives. The secondary objective was to confirm the feasibility of using the ETFT prospectively in recreational scuba diving to study these changes.
Methods
ETHICAL CONSIDERATIONS AND INCLUSION CRITERIA
The Ethics Committee of the University Hospital of Cologne, Germany approved this observational, prospective cohort study. The trial was registered by the German Clinical Trial Register (No. DRKS00008968). Written informed consent was obtained from each participant before their inclusion. The study-related examinations took place during their vacation. All participants were certified divers over 18 years old, with a valid medical certificate and who had not been diving for 24 hours prior to the study. The divers were classified as 'inexperienced' (< 50 dives), 'intermediate' (50–200 dives), 'experienced' (201–499 dives) and 'professional' (≥ 500 dives). The experience levels were set according to recommendations of the diving instructors who participated in the study.
DIVING
Diving was conducted in the Sharm el Sheikh region of Egypt over six consecutive days. Water temperature in the Red Sea was stable at 23–24°C, and the salinity was 4.2%.[ 15] On the first day of diving, all participants performed shore dives; from days two to six the majority of dives were boat dives. Participants were allocated to two boats for the whole week. Start time, duration and depth of every dive were assessed for each participant.
STUDY-RELATED INTERVENTIONS
Certification level, diving experience, number of dives and date of the last dive were recorded. The otoscopic appearances of the TM, the external ear canal and the ability to perform a Valsalva manoeuvre were evaluated (Heine, Herrsching, Germany). Presence of TM movement during a Valsalva manoeuvre was documented as 'present' or 'absent'. Nasopharyngeal pathologies were excluded using a rigid 0° endoscope (Storz, Tuttlingen, Germany). All parameters were documented separately for the left and right ears. During the week of diving, participants underwent otoscopy and the ETFT before the first dive, between each dive and after the last dive. ETFT was performed an average of 43 ± 22 min after the dive (range: 1–116 min). Two consecutive dives within 12 h of each other were defined as repetitive dives. TM changes were evaluated using the TEED classification for MEBt as modified by Edmonds.[ 16 , 17] Final examination took place at least 12 hours after the last dive.
EUSTACHIAN TUBE FUNCTION TEST
ETFT was carried out according to the guidelines of the manufacturers in the sitting position for each ear separately after an otoscopic examination.[ 12 - 14] Two mobile tympanometers were used (Titan, Interacoustics A/S, Denmark and EasyTymp, Meico Diagnostics GmbH, Germany). The tympanometers were allocated to the particular boats and consequently to the same participants throughout the week. The frequency setting for tympanometry was 226 Hz. In contrast to Williams' original procedure, the participants were asked to perform a Valsalva manoeuvre after the first tympanogram and to swallow after the second tympanogram (OtoAcess Software, Interacoustics A/S, Denmark).[ 14] Thereby, the possibility and the effectiveness of both passive and active pressure equalization could be assessed.[ 14] Regular tympanometry was performed first (R-tymp), a second measurement was made after the Valsalva manoeuvre (V-tymp) and a third after swallowing (S-tymp) (Figure 1).[ 12 - 14] The Williams procedure kept the pressure inbetween the first and second tympanogram at 'stop pressure' and between the second and third tympanogram at 'start pressure'.[ 14]
Figure 1.
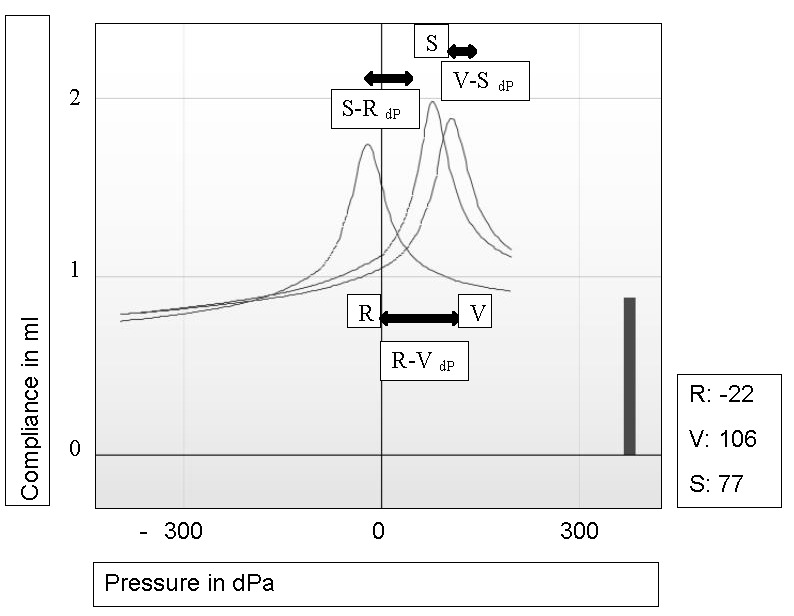
Eustachian tube function test; regular tympanometry (R = R-tymp) was performed first, the second measurement (V = V-tymp) was carried out after a Valsalva manoeuvre and the third after swallowing (S = S-tymp); compliance (y-axis, ml), peak pressure of R-tymp, V-tymp and S-tymp (x-axis, dPa); the pressure differences between R-tymp and V-tymp (R-VdP), V-tymp and S-tymp (V-SdP) and S-tymp and R-tymp (S-RdP) are shown
ETFT Interpretation
Tympanometry primarily provides information about the pressure (peak pressure, in dPa, R-tymp) in the middle ear and the static compliance (in ml) of the middle ear system. In addition, the gradient and/or the tympanometric width describe the steepness of the curve (Figure 1). Determination of the middle ear pressure is based on the observation that compliance reaches a maximum when ear canal pressure is equal to the middle ear pressure, at which point the sound energy is maximized (peak pressure in dPa).[ 11]
A positive shift of the R-tymp peak pressure mirrors the increasing middle ear pressure ('overpressure' or positive pressure). Accordingly, a negative shift of the peak pressure occurs due to negative middle ear pressure. The R-tymp was obtained as ‘baseline’ peak pressure. After a Valsalva, the peak pressure should shift (positively), revealing a positive shift of the TM. This pressure shift is defined in this paper as R-VdP. The extent of the peak pressure shifts (i.e., R-VdP, V-SdP and S-RdP) provides information about the effectiveness of pressure equalization during the Valsalva manoeuvre and swallowing, respectively. Higher R-VdP might indicate better ET function. Figure 1 gives an example of normal ETFT data.
Compliance depends on the state of the TM and the pressure in the middle ear. The condition of the middle ear mucosa, fluid in the middle ear, chronic and acute structural TM changes influence the compliance variables.
STATISTICAL ANALYSIS
All data were de-identified. The findings of the left and right ears were evaluated separately, but analysed together using SPSS software (version 23.0.0.0, IBM Corporation, USA). Quantitative variables are presented as mean ± standard deviation, or 95% confidence intervals (95% CI), or median and range, or interquartile range (IQR) and qualitative variables as absolute number and percentage. We applied mixed model analysis of variance with repeated measures for analysis of quantitative data and Chi-square test for analysis of qualitative data. The mixed model analysis allows for inclusion of multiple time points per subject, while accounting for unbalanced data structure of irregular time intervals between ETFT measurements and unequal numbers of ETFT analyses per subject. The respective ETFT parameters (R-tymp, R-VdP, V-SdP, and R-tymp compliance) were included as dependent variable and the dive number, diving day, TEED grade and diving experience groups as covariates. Univariate analysis (F-test) was based on analysis of linear independent pairwise comparisons. A P-value < 0.05 was considered statistical significant. All reported P-values are two-sided. To correct for multiple testing, P-values were adjusted using the Bonferroni correction. A corrected P-value of < 0.05 was considered to be significant for all tests.
Results
PARTICIPANTS
Of the 28 participants, 19 were male and nine female, mean age 38 ± 10.0 years. Median number of dives before the study was 53 (range: 4−2,550). The last dive was performed a median of 2.5 months (range: 27 days to 186 months) prior to the study. The participants performed an average of 15 dives (range: 9−19) during the six days; on average three per day (range: 1−4). Average diving duration was 51 ± 7 minutes; average depth was 25 ± 7 metres' seawater. We defined 13 divers as inexperienced, seven as intermediate, three as experienced and five as professional.
CLINICAL EXAMINATIONS BEFORE THE FIRST DIVE
Endoscopy of the ear, nose and epipharynx was normal in 26 participants. No local anaesthetic or lubricant was used for the endoscopic evaluation. Two participants (both experienced divers) showed exostoses of the external ear canal in both ears. The appearances of the TMs were normal bilaterally in all the divers and they were able to perform a Valsalva manoeuvre successfully, with a type-A tympanogram.[ 18]
OTOSCOPY DURING THE DIVING
Valsalva manoeuvres were effective in 99.7% (n = 437) of dives. No cases of external ear canal inflammation were seen. As reported elsewhere, MEBt (TEED 1−3) was observed in 42.2% (n = 490) of the 1,161 otoscopic examinations.[ 19] In total, TEED 0 was observed in 57.8% (n = 671), TEED 1 in 34.1% (n = 396), TEED 2 in 7.5% (n = 87) and TEED 3 in 0.6% (n = 7). No TM perforations (TEED 4) occurred.[ 19]
COMPLIANCE
No significant differences in compliance were seen between the right and left ears (F-test for left/right ear, P = 0.717). Mean compliance values also did not differ significantly between the R-, V- and S-tymp measurements: 1.4 ± 1.3 ml for all measurements; median 1.0 ml (IQR 0.7−1.5 ml), 1.0 ml (IQR 0.7−1.5 ml) and 1.1 ml (IQR 0.7−1.6 ml), respectively. For this reason, we performed the following analyses using only the R-tymp compliance. There was a significant increase in compliance after the first dive (F-test for dive number, P < 0.0001). During the six diving days, the mean values for compliance slightly decreased after day 1 (1.9 ml on day 1, 1.5 ml on day 2) but thereafter remained stable (F-test for diving day, all P > 0.474). Professional divers had higher compliance values compared to divers with less experience (F-test for experience groups, P < 0.0001; data not shown∗). Furthermore, professional divers also showed a significantly greater difference in compliance after the first, second and third dive in a day compared to less experienced divers (pair-by-pair comparison, all P < 0.05; data not shown∗).
∗Footnote:
Additional summary data tables not shown here are available from the authors at moritz.meyer@uk-koeln.de
PEAK PRESSURE
All participants were able to equalize pressure in the middle ear before diving. Analysing the R-tymp values during the six consecutive days of diving, significant positive shift of pressure in the middle ear was evident (Table 1; F-test for diving day, P < 0.0001). R-tymp values changed significantly after the first three diving days (F-test, all P < 0.05) and remained stable on days four through seven (a non-diving day). Day 1 values were significantly different to values on days two through six (pair-by-pair comparison, all P < 0.05).
Table 1. R-tymp peak pressure (dPa) during six consecutive days of diving in 28 divers (P < 0.001); ∗ Day 1 value is significantly different to values on days 2–6 (pair-by-pair comparison, all P < 0.05) .
| Day | Mean | 95% confidence interval |
| 1∗ | -9.6 | -22 to 2.8 |
| 2 | 13.9 | 1.8 to 26 |
| 3 | 21.3 | 9.4 to 33.2 |
| 4 | 17.9 | 7 to 28.9 |
| 5 | 18.8 | 6.8 to 30.7 |
| 6 | 17 | 4.9 to 29.2 |
| 7 | 10.8 | -9.3 to 31 |
Positive pressure shift in R-tymp was also evident over a single diving day (F-test for dives 0 to 4, P = 0.344). However, R-tymp values differed significantly between different experience groups (F-test for experience groups; P < 0.0001, Table 2). During the six diving days, R-tymp values in intermediate divers showed a significant positive shift (pair-by-pair comparison for days one to six for intermediate divers; all P < 0.05). During a single diving day, a significant positive shift of R-tymp peak pressure was only evident in inexperienced divers for the fourth dive of a day (pair-by-pair comparison for dives 0 to 4, all P < 0.05).
Table 2. R-tymp peak pressure (dPa) in different experience groups of divers; values are statistically significant in pair-by-pair comparison to the inexperienced group ∗, intermediate group ∗∗, experienced divers group †; F-test for experience groups, P < 0.0001 .
| Diving experience | Mean | 95% confidence interval |
| Inexperienced∗, † | 10.4 | 1.9 to 18.9 |
| Intermediate∗∗, † | 4.9 | -2.6 to 12.4 |
| Experienced∗, ∗∗∗, † | -15.3 | -25.6 to -5 |
| Professional∗, ∗∗∗, † | 33.8 | 16.1 to 51.5 |
PEAK PRESSURE DIFFERENCE R-VdP
The changes in R-VdP during the diving week are shown in Table 3. Only that for inexperienced divers was statistically significant (F-test for diving day, P = 0.013) (Table 4). The R-VdP was significantly lower in experienced and professional divers compared to the inexperienced and intermediate divers (F-test for experience groups, P < 0.0001) (Table 4). There were no statistically significant changes in R-VdP during a diving day (Table 5).
Table 3. R-VdP (dPa) changes during single day of diving (A; F-test for dives 0−4, P = 0.099) and over the diving week (B; F-test for days 1−7, P = 0.659) .
| A. | ||
| Dive no. | Mean | 95% confidence interval |
| 0 | -5.9 | -15.6 to 3.9 |
| 1 | -19 | -30.1 to -7.9 |
| 2 | -19.8 | -31.3 to -8.3 |
| 3 | -27.9 | -42.6 to -13.3 |
| 4 | -28 | -80.8 to 24.8 |
| B. | ||
| Day | ||
| 1 | -8.3 | -25.3 to 8.7 |
| 2 | -12.3 | -28.5 to 3.9 |
| 3 | -20.2 | -36.1 to -4.3 |
| 4 | -21.2 | -35.8 to -6.5 |
| 5 | -20.9 | -36.9 to -5 |
| 6 | -16.9 | -33.6 to -0.2 |
| 7 | -32.7 | -59.5 to -6 |
Table 4. Day-by-day change in R-VdP (dPa) in different experience groups during the diving week; ∗ pair-by-pair comparison for diving days 1 to 6; day 7 was a non-diving day; 95%CI – 95% confidence interval .
| Diving experience | Day | Mean | 95%CI | P-value |
| Inexperienced | ||||
| 1 | -11.3 | -35.6 to 13.1 | 0.01∗ | |
| 2 | -54.5 | -77.3 to -31.7 | ||
| 3 | -53.2 | -75.4 to -31 | ||
| 4 | -53.7 | -74.2 to -33.2 | ||
| 5 | -49.8 | -72.5 to -27.1 | ||
| 6 | -52.6 | -74.4 to -30.7 | ||
| 7 | -72.8 | -110.2 to -35.3 | ||
| Intermediate | ||||
| 1 | -44.9 | -75.1 to -14.7 | > 0.7 | |
| 2 | -16.5 | -45.2 to 12.1 | ||
| 3 | -22.8 | -51.6 to 6 | ||
| 4 | -40 | -67.5 to -12.4 | ||
| 5 | -41.8 | -69 to -14.6 | ||
| 6 | -27.1 | -62.3 to 8.1 | ||
| 7 | -39.9 | -86.5 to 6.7 | ||
| Experienced | ||||
| 1 | -3.9 | -50.1 to 42.3 | > 0.9 | |
| 2 | 8.8 | -29.9 to 47.5 | ||
| 3 | -7.3 | -48.4 to 33.8 | ||
| 4 | 0.1 | -39.4 to 39.6 | ||
| 5 | -18.6 | -58.1 to 20.9 | ||
| 6 | -9.4 | -50.6 to 31.7 | ||
| 7 | -7.2 | -76.7 to 62.2 | ||
| Professional | ||||
| 1 | -20.4 | -58.5 to 17.6 | > 0.5 | |
| 2 | 27.1 | -16.1 to 70.3 | ||
| 3 | -8 | -46 to 29.8 | ||
| 4 | 12.8 | -22.8 to 48.5 | ||
| 5 | 20.6 | -20.8 to 61.9 | ||
| 6 | 22.2 | -17.3 to 61.7 | ||
| 7 | 0.9 | -68.6 to 70.3 |
Table 5. Dive-by-dive change in R-VdP (dPa) in different experience groups of divers over a day's diving; pair-by-pair comparison for dives 0 to 4 not significant; 95%CI – 95% confidence interval .
| Diving experience | Dive # | Mean | 95%CI | P-value |
| Inexperienced | 0 | -39.7 | -52.9 to -26.5 | > 0.6 |
| 1 | -42.7 | -57.8 to -27.6 | ||
| 2 | -48.3 | -63.8 to -32.9 | ||
| 3 | -55.4 | -75.4 to -35.3 | ||
| 4 | -67.4 | -125.4 to -9.4 | ||
| Intermediate | 0 | -11.9 | -29.5 to 5.6 | > 0.5 |
| 1 | -37 | -56.5 to -17.6 | ||
| 2 | -34.9 | -55.1 to -14.8 | ||
| 3 | -54.3 | -83.8 to -24.7 | ||
| 4 | - | - | ||
| Experienced | 0 | 12.2 | -14.2 to 38.6 | > 0.4 |
| 1 | -16.2 | -44.1 to 11.8 | ||
| 2 | -2.1 | -33.2 to 29 | ||
| 3 | -9.1 | -43.8 to 25.7 | ||
| 4 | - | - | ||
| Professional | 0 | 17.9 | -6.8 to 42.5 | > 0.9 |
| 1 | 9.9 | -18 to 37.8 | ||
| 2 | 2.1 | -26.2 to 30.5 | ||
| 3 | 2.5 | -34.9 to 39.9 | ||
| 4 | 33.7 | -83.5 to -83.5 |
Similarly changes in V-S dP and S-R dP were not statistically significant (F-test for diving day and dive number, P > 0.05 respectively; data not shown∗). However, inexperienced divers showed significantly higher V-S dP compared to other experience groups (F-test for experience groups, P < 0.0001; data not shown∗).
CORRELATION OF PEAK PRESSURE AND MEBt
The clinical findings of MEBt have been described elsewhere.[ 19] Divers with signs of barotrauma (TEED > 0) showed lower values of R-tymp peak pressure (mean 5.8 dPa, 95% CI -1.7 to 13.3) than divers with regular otoscopic findings (mean 13.8 dPa, 95% CI 6.8 to 20.9; F-test for TEED 0 vs. > 0, P = 0.029). Furthermore, the R-V dP displayed significantly higher negative pressure values in divers with barotrauma (mean -31.9, 95% CI -43.5 to -20.3) compared to those without barotrauma (mean 9.3, 95% CI -20.2 to 1.6; F-test for TEED 0 vs. > 0, P < 0.0001). R-V dP increased from TEED 0 to TEED 1 (pair-by-pair comparison, P = 0.002) and then increased further for TEED 2 and 3 (P = 0.012 and P = 0.52 respectively; data not shown*). Divers with the greatest level of barotrauma (TEED 3) displayed high negative R-tymp peak pressure in the middle ear (mean -55.8 daPa, 95% CI -96.4 to -15.2).
Discussion
Despite the enormous popularity of recreational scuba diving, only few aspects are known about ET and middle ear function after repetitive diving. The feasibility of test procedures, small study groups and different diving environments are some of the parameters which limit scientific understanding.
INTERPRETATION OF RESULTS
We included 28 participants in this prospective cohort study. Continuous supervision of the participants during the week's diving allowed for accurate clinical follow-up. Overall, we observed on-going changes in middle ear pressures from day to day, which could be correlated to the repeated pressure exposure. Cumulative pressure exposure resulted in significantly decreasing compliance, which was obvious from the first dive, mostly affecting less experienced divers. The 'professional' divers showed significantly higher initial compliance before diving than inexperienced divers and significantly higher differences in compliance between the dives. They also had less barotrauma. Thus, the decreasing compliance in inexperienced divers may be owing to more pronounced MEBt arising from inadequate pressure equalization techniques. Hence, repeated exposure to pressure alterations over a long time period may influence TM mobility and ET function in a positive manner, resulting in increased compliance without decreasing TM stability. However, a long-term follow-up of professional divers is required to confirm this assumption.
We defined R-VdP as the main indicator for successful pressure equalization in the middle ear. The R-VdP measurements suggest that inexperienced divers who were unused to repetitive pressure exposure seemed to apply more pressure during a Valsalva manoeuvre than did more experienced divers. However, the steadily increasing R-VdP in this group after repetitive dives might also indicate easier equalization as the week progressed.
Divers with signs of barotrauma (TEED > 0) had lower values of R-tymp peak pressure ('underpressure'), as well as a greater negative R-VdP. These results correlated with peak pressure changes in the inexperienced and intermediate divers. Thus, increasing negative pressure in the middle ear during diving seems to be a crucial factor for the development of barotrauma.
RESULTS IN CONTEXT OF PREVIOUS PUBLICATIONS
Previous studies have described visible alterations of the TM from exposure to varying pressure levels.[ 16 , 17 , 20] The TEED-classification nowadays is applied worldwide for the classification of MEBt.[ 16] However, the influence of repetitive pressure changes on ET function is insufficiently investigated by simple otoscopy, whilst other diagnostic techniques, such as pure tone tympanometry etc., allow drawing only indirect conclusions about ET function.[ 11]
The Valsalva manoeuvre during tympanometry is the most widely-used diagnostic test for evaluating middle ear ventilation and ET function.[ 11] Whereas the Valsalva manoeuvre only allows categorical differentiation of pressure equalization, pure tone tympanometry displays compliance, impedance and peak pressure objectively and thus provides information about TM mobility and pressure conditions in the middle ear.[ 11] Because repeatedly performed tympanometry only shows minor fluctuations of middle ear pressure,[ 11] tests based on repeated measurement of tympanic impedance were developed (e.g., Williams inflation/deflation test and the nine-step inflation/deflation test).[ 12 , 13 , 21 - 23] However, the reliable dynamic evaluation of ET function is only possible in a pressure chamber;[ 4 - 6] its application in routine clinical practice has been limited by time and cost.[ 4]
There are several studies evaluating ET function in scuba divers.[ 19 - 21 , 24 , 25] In 62 healthy participants in a Navy diving programme, the original Williams inflation/deflation test correlated with subjective performance and otoscopic findings after a single dive in a pressure chamber and after a single 12 m deep dive in water. There was no relationship between ET test results, otoscopy or subjective complaints by the participants. Consequently, the authors concluded that this test was of little value for screening divers.[ 24]
In contrast, a high predictive value for the nine-step inflation/deflation test for symptomatic MEBt was reported in 31 divers after repeated pressure exposure during 774 dives.[ 20] Our results confirm these findings. Decreasing compliance, lower values of R-tymp peak pressure and negative R-VdP in our study correlated significantly with a higher prevalence of barotrauma. Previous analysis of the MEBt prevalence in the same participants revealed that four of the 28 divers missed at least one dive because of problems during pressure equalization.[ 19] However, the question whether a diver omitted a dive was not asked until the last day of the trial and could not be correlated retrospectively to a specific ETFT measurement. If our results can be reproduced in further prospective trials, ETFT may serve as a valuable monitoring test for adequate pressure equalization in divers to prevent further MEBt development. The study has shown clearly the feasibility of using the ETFT during diving activities.
In the only long-term follow-up, tympanometry, otoscopic findings and subjective symptoms were studied over a 31-day study period. Despite the limited sample size (two divers) and asymptomatic participants throughout the study period, tympanometry revealed a strong association of decreased middle ear pressure with repetitive pressure exposure (more than two dives daily).[ 25] Furthermore, using the Valsalva manoeuvre led to restoration of middle ear pressure in both participants. These observations confirm other reports describing a significant recovery of the middle ear after a surface interval of more than 11 h.[ 21] We detected neither complete recovery of middle ear pressure, nor of the otoscopic findings in the present trial.[ 19] However, higher numbers of less experienced divers might explain this discrepancy.
LIMITATIONS OF THE STUDY
There is no standardized procedure for quantitative measurement of successful pressure equalization in the middle ear during diving or flying. Furthermore, routine tympanometry only provides categorical classification of middle ear and ET function.[ 11] In this trial, we assumed that active equalization methods (especially the Valsalva manoeuvre) could differentiate within individuals based on the length and intensity of the action.[ 6] This aspect may have biased the measurements. In addition, since our analysis does not contain normal non-diving participants, who underwent sham-dives (i.e., in a pressure chamber), the present results should be seen as a reference point for further controlled studies.
Conclusions
Using ETFT, we observed significant changes in middle ear pressure and pressure equalization in divers due to repeated pressure exposure in saltwater. Repetitive diving over six consecutive days led to significantly decreased compliance and increased R-tymp peak pressure ('overpressure') in the middle ear. The most profound changes were observed in less experienced divers. Besides greater stiffness of the TM, significantly negative values of R-tymp peak pressure, as well as significantly higher negative R-VdP were associated with a higher prevalence of MEBt in this cohort of divers. An accompanying paper investigates these changes in another cohort of divers in colder freshwater.[ 26]
Footnotes
Acknowledgments
The authors would like to thank the team of Actionsport Würzbung, especially Georg Seufert, the team of Sinai Divers (Naama Bay) and the enthusiastic, voluntary contribution of all the divers who participated in this trial.
Conflict of interest: nil
Funding
Interaucoustics A/S kindly loaned the tympanometry equipment.
Contributor Information
Moritz F Meyer, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Germany.
Manuela Boor, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Germany.
Stefanie Jansen, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Germany.
Eberhard D Pracht, German Centre for Neurodegenerative Diseases (DZNE), Bonn, Germany.
Moritz Felsch, Institute of Medical Statistics, Informatics and Epidemiology, University of Cologne, Germany.
Moritz Klünter, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Germany.
Karl-Bernd Hüttenbrink, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Germany.
Dirk Beutner, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Germany.
Maria Grosheva, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Germany.
References
- Bluestone CD. Impact of evolution on the Eustachian tube . Laryngoscope. 2008;118:522–7. doi: 10.1097/MLG.0b013e31815ddaa0. [DOI] [PubMed] [Google Scholar]
- Feldmann H. [Physiology and physiopathology of middle ear ventilation. I. Middle ear volume and its gas content. Physiology of the Eustachian tube.] . Z Laryngol Rhinol Otol. 1973;52:471–85. (Ger). [PubMed] [Google Scholar]
- Feldmann H. [Physiology and pathophysiology of the ventilation of the middle ear. 2. Methods of examination of the Eustachian tube. Pathophysiology of typical ventilation disorders of the middle ear] . Z Laryngol Rhinol Otol. 1973;52:555–72. (Ger). [PubMed] [Google Scholar]
- Meyer MF, Mikolajczak S, Korthäuer C, Jumah MD, Hahn M, Grosheva M, et al. Impact of xylomethazoline on Eustachian tube function in healthy participants . Otol Neurotol. 2015;36:769–75. doi: 10.1097/MAO.0000000000000709. [DOI] [PubMed] [Google Scholar]
- Meyer MF, Mikolajczak S, Luers JC, Lotfipour S, Beutner D, Jumah MD. [Characterizing the passive opening of the Eustachian tube in a hypo-/hyperbaric pressure chamber] . Laryngorhinootologie. 2013;92:600–6. doi: 10.1055/s-0033-1347175. (Ger). [DOI] [PubMed] [Google Scholar]
- Mikolajczak S, Meyer MF, Hahn M, Korthäuer C, Jumah MD, Hüttenbrink MD, et al. Characterizing the active opening of the Eustachian tube in a hypobaric/hyperbaric pressure chamber . Otol Neurotol. 2015;36:70–5. doi: 10.1097/MAO.0000000000000575. [DOI] [PubMed] [Google Scholar]
- Klingmann C, Praetorius M, Baumann I, Plinkert PK. Otorhinolaryngologic disorders and diving accidents: an analysis of 306 divers . Eur Arch Otorhinolaryngol. 2007;264:1243–51. doi: 10.1007/s00405-007-0353-6. [DOI] [PubMed] [Google Scholar]
- Azizi MH. Ear disorders in scuba divers . Int J Occup Environ Med. 2011;2:20–6. [PubMed] [Google Scholar]
- Molvaer OI, Natrud E. Ear damage due to diving . Acta Otolaryngol Suppl. 1979;360:187–9. doi: 10.3109/00016487809123512. [DOI] [PubMed] [Google Scholar]
- Shupak A, Doweck I, Greenberg E, Gordon CR, Spitzer O, Melamed Y, et al. Diving-related inner ear injuries . Laryngoscope. 1991;101:173–9. doi: 10.1288/00005537-199102000-00013. [DOI] [PubMed] [Google Scholar]
- Therkildsen AG, Gaihede M. Accuracy of tympanometric middle ear pressure determination. The role of direction and rate of pressure change with a fast modern tympanometer . Otol Neurotol. 2005;26:252–6. doi: 10.1097/00129492-200503000-00021. [DOI] [PubMed] [Google Scholar]
- Williams PS. A tympanometric pressure swallow test for assessment of Eustachian tube function . Ann Otol Rhinol Laryngol. 1975;84:339–43. doi: 10.1177/000348947508400309. [DOI] [PubMed] [Google Scholar]
- Spreitzer JB, Newman CW. Reliability of a measure of Eustachian tube function in normal subjects . Ann Otol Rhinol Laryngol. 1984;93:48–51. doi: 10.1177/000348948409300112. [DOI] [PubMed] [Google Scholar]
- Interacoustics . Titan tympanometers manual . Interacoustics A/S. Audiometer Allé; 5500 Middelfart: http://www.interacoustics.com . [Google Scholar]
- Turekian K. Oceans. Englewood Cliffs, NJ: Prentice Hall; 1968. [Google Scholar]
- Teed RW. Factors producing obstruction of the auditory tube in submarine personnel . United States Naval Medical Bulletin. 1944;42:293–306. [Google Scholar]
- Edmonds C. Otological aspects of diving. Sydney: Australasian Medical Publishing Company; 1973. [Google Scholar]
- Jerger J. Clinical experience with impedance audiometry . Arch Otolaryngol. 1970;92:311–24. doi: 10.1001/archotol.1970.04310040005002. [DOI] [PubMed] [Google Scholar]
- Jansen S, Meyer MF, Boor M, Felsch M, Klünter HD, Pracht ED, et al. Prevalence and risk factors of barotrauma in recreational scuba divers after repetitive dives in salt water . Otol Neurotol. 2016;37:1325–31. doi: 10.1097/MAO.0000000000001158. [DOI] [PubMed] [Google Scholar]
- Ramos CC, Rapoport PB, Brito Neto RV. Clinical and tympanometric findings in repeated recreational scuba diving . Travel Med Infect Dis. 2005;3:19–25. doi: 10.1016/j.tmaid.2004.06.002. [DOI] [PubMed] [Google Scholar]
- Uzun C. Evaluation of predive parameters related to Eustachian tube dysfunction for symptomatic middle ear barotrauma in divers . Otol Neurotol. 2005;26:59–64. doi: 10.1097/00129492-200501000-00010. [DOI] [PubMed] [Google Scholar]
- Bluestone CD. Assessment of Eustachian tube function. Jerger J, editor. . New York: American Electromedics; 1975. p. 127- 48. [Google Scholar]
- Hussein A, Abousetta A. Use of the nine-step inflation/deflation test and resting middle-ear pressure range as predictors of middle-ear barotrauma in aircrew members . J Laryngol Otol. 2014;128:612–7. doi: 10.1017/S0022215114001467. [DOI] [PubMed] [Google Scholar]
- Schuchman G, Joachims HZ. Tympanometric assessment of Eustachian tube functions of divers . Ear and Hearing. 1985;6:325–8. doi: 10.1097/00003446-198511000-00009. [DOI] [PubMed] [Google Scholar]
- Green SM, Rothrock SG, Green EA. Tympanometric evaluation of middle ear barotrauma during recreational scuba diving . Int J Sports Med. 1993;14:411–5. doi: 10.1055/s-2007-1021201. [DOI] [PubMed] [Google Scholar]
- Jansen S, Boor M, Meyer MF, Pracht ED, Volland R, Kluenter HD, et al. Repetitive diving in freshwater alters Eustachian tube function measured by Eustachian tube function test in recreational scuba divers . Diving Hyperb Med. 2017;47:222–6. doi: 10.28920/dhm47.4.223-227. [DOI] [PMC free article] [PubMed] [Google Scholar]