

Abstract
Introduction
We investigated the effect of repetitive pressure exposure during freshwater dives on Eustachian tube function and the middle ear, assessed by the Eustachian tube function test (ETFT).
Methods
This prospective observational cohort study included 23 divers over three consecutive days of diving in freshwater lakes in Nordhausen, Germany. Participants underwent otoscopy and ETFT before the first dive, between each dive and after the last dive. ETFT included regular tympanometry (R-tymp), tympanometry after Valsalva (V-tymp) and after swallowing (S-tymp). The peak pressure difference between the R-tymp and the V-tymp (R-VdP) defined effectiveness of pressure equalization after Valsalva manoeuvres. We evaluated the change in compliance and peak pressure and correlated the results to the otoscopic findings and diving experience.
Results
Twenty-three divers performed 144 dives. Middle ear barotrauma was assessed using the Edmonds modification of the TEED scoring system. In the ETFT, the R-tymp peak pressure displayed a negative shift from day one to three (P = 0.001) and differed significantly between the experience groups (P = 0.01). R-VdP did not change significantly on any of the three days of diving (all P > 0.05). Participants without MEBt showed significantly lower R-tymp values than did those with barotrauma (P = 0.019).
Conclusion
Repetitive pressure exposure during three consecutive days of freshwater diving led to a negative shift of the peak pressure in the middle ear. Less experienced divers showed significantly higher middle ear peak pressure and higher pressure differences after equalization manoeuvres. Higher middle ear peak pressure was also associated with a higher prevalence of barotrauma.
Keywords: Tympanometry, Middle ear, Ear barotrauma, Recreational diving
Introduction
Our knowledge about the effect of rapid pressure changes during diving on middle ear and Eustachian tube (ET) function is mostly based on research on professional divers, navy divers or on case reports and retrospective questionnaires.[ 1 - 4] None of these studies were conducted in freshwater. However, diving in freshwater differs from diving in the sea. Besides the characteristics of the water itself, e.g., density, temperature, salinity, etc., diving conditions in a freshwater lake, such as visibility, temperature and depth, may influence the ability to effectively equalize pressure in the middle ear. Using the Eustachian tube function test (ETFT),[ 5 , 6] we prospectively evaluated the changes in middle ear pressures and evidence of middle ear barotrauma (MEBt) after repetitive freshwater dives. The findings were also compared to those in the accompanying study on a cohort of divers in the Red Sea.[ 7]
Methods
The Ethics Committee of the University Hospital of Cologne, Germany, approved this observational prospective cohort study. The trial was registered prior to all study-related interventions by the German Clinical Trials Register (No. DRKS00008968; URL: http://apps.who.int/trialsearch/). Written informed consent was obtained from each participant before their inclusion. All participants presented a valid medical certificate prior to all study-related interventions. Three participants were under age (all 16-years-old) and, therefore, presented with written consent from a parent or legal guardian before their inclusion. None of the divers had been diving for 24 hours prior to the study.
The study was conducted in two freshwater lakes in Nordhausen, Thuringia, Germany in August 2015 over three consecutive days. The lakes are a maximum depth of 31 metres. Surface water temperature was 22–23°C, 18–19°C below the first thermocline at a depth of 8–10 metres and 7–8°C below the second thermocline at 14–15 metres. Dive time, maximum depth of each dive and surface intervals were recorded for each diver.
STUDY-RELATED INTERVENTIONS AND THE ETFT
Before the first dive, all participants were questioned about their diving and ENT-related medical history and diving experience. In addition, otoscopy and endoscopy of the nose and epipharynx were performed to exclude any pathology. No topical anesthetic or lubricant was used for nasal endoscopy. Otoscopic changes of the tympanic membrane (TM) were evaluated according to the TEED classification for middle ear barotrauma (MEBt) as modified by Edmonds.[ 8 , 9] A Valsalva manoeuvre was assessed by otoscopy in all participants. Tympanometry was performed at 226 Hz before the first dive and immediately after every dive according to the ETFT using a mobile tympanometer (Titan®, Interacoustics A/S, Denmark) as previously described.[ 7] R-tymp measurement represented the peak pressure in the middle ear at rest, V-tymp the peak pressure after a Valsalva manoeuvre and S-tymp after swallowing. R-VdP represented the difference in peak pressure between the R-tymp and V-tymp and V-SdP the difference between the V-tymp and the S-tymp. A more detailed description of the tympanometry methodology is provided in the accompanying paper.[ 7]
PARTICIPANTS
We included 23 participants (46 ears), seven female and 16 male, with a mean age of 34.5 ± 11.5 years. The median number of dives completed before the study was 40 (range 1–1,100). The last dive was performed a median of 1.9 months (range 0.9–11.9 months) prior to the study. We defined 13 divers as 'inexperienced' (< 50 dives), five divers as ‘intermediate’ (50–200 dives) and five divers as 'professional' (≥ 500 dives). The categorization of diving experience was developed during our saltwater study and was applied in the present trial to allow comparison of the results.[ 7] No one matched the criteria of an 'experienced' diver (201–499 dives) as defined in that study.
STATISTICAL EVALUATION
All data were de-identified. The findings of the left and right ears were evaluated separately, but analyzed together using SPSS (version 23.0.0.0, IBM Corporation, USA). Quantitative data are presented as mean ± standard deviation (SD), or 95% confidence interval (95% CI), or as median and range, or interquartile range (IQR) and qualitative variables as absolute number and percentage. We applied mixed model analysis of variance with repeated measures for analysis of quantitative data for the ETFT values. To correct for multiple testing, P-values were adjusted using the Bonferroni method. The mixed model analysis allows for inclusion of multiple time points per subject, while accounting for unbalanced data structure of irregular time intervals between ETFT measurements and unequal numbers of ETFT analyses per subject. The respective ETFT parameters − R-tymp peak pressure, R-VdP, V-SdP and R-tymp compliance − were included as dependent variable; and the dive number, diving day, TEED and diving experience groups as covariates. The univariate analysis (F-test) was based on analysis of linear independent pairwise comparisons. Chi-square test was applied for analysis of TEED distribution per diving day. Kruskall-Wallis test was applied to test the influence of diving depth on TEED distribution. Spearman’s correlation was applied to test an association of diving depth and R-tymp peak pressure. A corrected P-value of < 0.05 was considered to be significant for all tests. All reported P-values are two-sided.
Results
DIVING
During the three days, the participants completed 144 dives. Seven participants used a drysuit and 16 a wetsuit. The average number of dives during the three days was six (median 5, range 4–10). The average depth and duration of the dives were 13 ± 4.1 metres' freshwater and 35 ± 10.6 min, respectively. There was a significant difference in the diving depths between the different experience groups ((Figure 1; Kruskal-Wallis test, P < 0.0001). The mean duration of the surface intervals between the dives was 127 ± 67 min.
Figure 1.
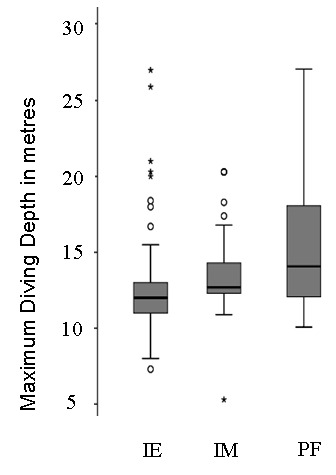
Maximum diving depth in different experience groups; (median test, P = 0.002; Kruskal-Wallis test, P < 0.0001); 13 divers were defined as 'inexperienced' (< 50 dives) (IE), five divers as 'intermediate' (50-200 dives) (IM) and five divers as 'professional' (≥ 500 dives) (PF)
CLINICAL EXAMINATION
Before the first dive, endoscopy of the nose and the epipharynx was normal in all divers as were the otoscopy findings in 45 ears. One diver had a hyperaemic TM (TEED 1). However, all divers were able to perform a Valsalva manoeuvre successfully before diving. Tympanometry showed a normal type A pattern in all 46 ears.[ 10]
During the three days' diving, MEBt (TEED 1−3) was observed in 105 ears (26%). TEED 1 was present in 86 (21%), TEED 2 in 14 (3%) and TEED 3 in five (1%). No TM perforations (TEED 4) occurred. Increasing number of dives per day was associated with a significant increase of pathologic otoscopic findings (TEED > 0; Chi-squared test, P < 0.0001). Furthermore, the maximum diving depth significantly influenced the MEBt prevalence (Kruskal-Wallis test, P = 0.035), shallower dives being associated with more signs of MEBt. The number of ears with signs of MEBt (TEED > 0) was equally distributed between the three experience groups (Fisher's test, P = 0.623); however, higher TEED levels (TEED ≥ 2) were present only in the inexperienced and intermediate divers.
COMPLIANCE
The mean values of the R-tymp compliance on days one to three did not differ significantly: mean 1.2 ml (IQR 0.7−1.7 ml); mean 1.3 ml (IQR 0.7−1.8 ml) and mean 1.2 ml (IQR 0.5−1.8), for days one, two and three respectively (F-test, P = 0.947). However, a significant increase in compliance was evident after the first dive (F-test, P = 0.041; Table 1. Professional divers had higher compliance values compared to the intermediate or inexperienced divers (F-test, P = 0.004; Table 2). Professional and intermediate divers also showed significantly higher change in compliance after the first dive compared to the inexperienced divers (pair-by-pair comparison, all P < 0.05, data not shown ∗).
Table 1. R-tymp peak pressure (dPa) during six consecutive days of diving in 28 divers (P < 0.001); ∗ Day 1 value is significantly different to values on days 2–6 (pair-by-pair comparison, all P < 0.05) .
| Dive number | Mean | 95% confidence interval |
| 1 | 1 | 0.7 to 1.3 |
| 2 | 1.4 | 1.1 to 1.7 |
| 3 | 1.3 | 1 to 1.5 |
| 4 | 1.2 | 0.8 to 1.6 |
| 5 | 1.1 | 0.6 to 1.5 |
| 6 | 1.3 | 0.3 to 2.0 |
Table 2. R-tymp compliance (ml), R-tymp peak pressure (dPa) and peak pressure difference after Valsalva manoeuvre (R-VdP) (dPa) in different experience groups of divers; 'professional' divers had higher compliance values (P = 0.004) and lower peak pressures (P = 0.01) compared to divers with lower experience; R-VdP was greatest in inexperienced divers (P = 0.02); 95% CI – 95% confidence interval .
| R-tymp compliance (ml) | R-tymp peak pressure (dPa) | R-VdP (dPa) | ||||
| Diving experience | Mean | (95%CI) | Mean | (95%CI) | Mean | (95%CI) |
| Inexperienced (n = 13) | 0.9 | (0.5 to 1.4) | 9.5 | (-17 to 36) | 39.3 | (-3.7 to 82.2) |
| Intermediate (n = 5) | 0.7 | (0.1 to 1.3) | -13.8 | (-42.3 to 14.7) | 13.4 | (-33 to 59.8) |
| Professional (n = 5) | 1 | (0.3 to 2.6) | -23.1 | (-53 to 6.7) | -6.9 | (-55.7 to 41.9) |
PEAK PRESSURE
The mean values of the R-tymp peak pressure differed significantly from day one to day three and revealed a negative pressure shift (F-test for diving day, P = 0.001; Table 3). The peak pressure in the middle ear varied significantly in different experience groups (F-test, P = 0.01; Table 2). Pair-by-pair comparison revealed significantly decreased R-tymp peak pressure during the three days of diving especially in groups of intermediate and professional divers, compared to inexperienced divers (data not shown∗).
Table 3. R-tymp peak pressure (dPa) during three consecutive days of diving in all participants; mean values differed significantly from days one through three (P = 0.001) .
| Day | Mean | 95% confidence interval |
| 1 | -10.4 | -39.2 to 18.5 |
| 2 | 15.2 | -10.6 to 40.9 |
| 3 | -33.8 | -65 to -2.5 |
PEAK PRESSURE DIFFERENCE (R-VdP)
R-VdP did not change significantly on any of the three days of diving: mean 19.2 dPa (95%CI -27 to 65.4); mean 18.2 dPa (95%CI 24.5 to 60.9) and mean 8.3 dPa (95%CI -40.9 to 57.5) for days one, two and three respectively; F-test, P = 0.818). In addition there were no statistically significant changes in R-VdP during a diving day (F-test, P = 0.522). However, when comparing the experience groups, a significantly higher R-VdP was evident in the inexperienced group (F-test, P = 0.02; Table 2). Similarly changes in V-S dP and S-R dP were not statistically significant (F-test for diving day and dive number, P > 0.05 respectively; data not shown∗).
∗Footnote:
Summary tables for data not shown here are available from the authors at moritz.meyer@uk-koeln.de
CORRELATION OF PEAK PRESSURE AND MEBt
Altogether, an increase of cumulative pathologic otoscopic findings (TEED > 0) was evident over the three days (Pearson's Chi-squared test, P < 0.0001). Participants without barotrauma showed significantly lower values of the R-tymp peak pressure (mean -21.2 dPa, 95%CI -47.5 to 5.1) than did those with barotrauma (mean 2.9 dPa, 95%CI -23.8 to 29.5; F-test 1 through 3, P = 0.019). This difference was evident on each diving day (data not shown*). Diving depth also significantly influenced the distribution of MEBt (Kruskal-Wallis test, P = 0.035); however, only a small association between diving depth and R-tymp peak pressure was evident (Spearman's Rho -0.185, -0.093 and +0.239 on days one, two and three respectively).
Discussion
INTERPRETATION OF THE RESULTS
Summarizing all the changes in the ETFT measurements, the negative shift in pressures was likely the result of ET dysfunction and/or increasing tissue damage because of slowly failing equalization. Because of the short (three-day) evaluation period, we were unable to analyze these pressure changes further. The more experienced divers had significantly lower peak pressures, including following a Valsalva and higher compliance values and a greater difference in compliance after the first dive, compared to less experienced divers. The higher compliance may be the result of chronic elasticity loss due to cumulative pressure exposure during diving. However, the increasing compliance did not seem to influence TM stability and implies efficient equalization techniques. Although the distribution of TEED classification between the groups did not show significant alterations, otoscopic findings with TEED 2 and 3 occurred only in the less experienced divers.
A variety of factors influence middle ear and ET function. Besides divers' pre-existing medical history and diving experience, the depth profile, number of repetitive dives per day, water and air temperature, salinity and density may influence the stress on the ET and the middle ear. The dives performed in this freshwater study were shorter and shallower than those in our saltwater (Red Sea) study.[ 7] Shallower dives require more frequent active and passive pressure equalization (Boyle’s Law) and are probably associated with an increased risk of barotrauma.[ 11 , 12] This could be exacerbated by divers experiencing more buoyancy problems in waters with poor visibility, resulting in inadequate and/or delayed pressure equalization and consequent MEBt.
We observed a significant inverse correlation between the prevalence of barotrauma and diving depth, but this may be because less experienced divers performed shallower dives than those with more experience. The short evaluation time does not allow us to draw reliable conclusions regarding this correlation. However, peak pressure alteration in the ETFT may reflect more sensitively the immediate effect of the previous dive, while longer pressure exposure may be needed for manifestation of otoscopic evidence of barotrauma.
RESULTS IN CONTEXT TO PREVIOUS RESEARCH
It is assumed that active pressure equalization during descent and passive pressure equalization during ascent does not differ between saltwater and freshwater. There is a possible decongestant effect of saltwater that might improve ET function and make pressure equalization easier. However, this effect would have to occur very rapidly to have any impact on equalization during the initial descent.
As reported in the accompanying saltwater paper, we observed that pressure equalization became easier during repetitive diving.[ 7] Alternatively divers might have performed a Valsalva manoeuvre more often on a dive as the week progressed. In the present study, such an effect could be observed only on the first day, remaining unchanged thereafter, which might suggest less efficient pressure equalization in the middle ear during repetitive freshwater dives compared to saltwater.
The same procedures and the same tympanometer were used during the ETFT in both trials. Repetitive saltwater dives resulted in a steady increase in R-tymp peak pressure, whereas in the present study, the middle ear peak pressure did the opposite, moving to ‘underpressure’ over the three days. These conflicting observations might be caused by the two diving cohorts utilizing different equalization techniques. Nevertheless, in both conditions, inexperienced divers had, on average, the highest peak pressures and higher R-VdP. In this trial, divers with barotrauma also showed significantly higher R-tymp peak pressure. Consequently, increasing R-VdP probably mirrors higher equalization pressure in the inexperienced divers. We previously hypothesized that increasing underpressure in the middle ear might lead to acute tissue damage and to MEBt.[ 7] Comparing the results of the salt- and fresh-water investigations, the pressure difference during pressure equalization appears to be crucial for development of barotrauma.
Ear problems are the commonest issue that forces a diver to stop a dive.[ 11 , 12] There has not been a good screening test available to evaluate MEBt and ET dysfunction on an on-going basis during diving activities. The poor reliability of the Valsalva manoeuvre and the poor correlation of subjective complaints to the degree of barotrauma has been of concern for many.[ 1 - 4] In the seawater study, over 70% of the divers with otoscopic evidence of MEBt remained asymptomatic.[ 13] Furthermore, all participants in both studies were able to perform the Valsalva manoeuvre effectively. The use of the ETFT has shown that changes in middle ear pressure occur before MEBt is otoscopically or clinically obvious. The ETFT has proven to be a useful investigative tool during diving activities.
LIMITATIONS OF THE STUDY
The analysis of ET function outside of a clinical facility poses a challenge. The ETFT offers the advantages of being easy to operate and provides a series of measurements during pressure equalization manoeuvres. However, no standardized values exist for this test. The lack of a control group, such as subjects undergoing dry dives in a pressure chamber, only allowed us to compare the data between the measurements. Furthermore, the possibility of intra-individual variation of intensity and length of a pressure equalization manoeuvre[ 14] cannot be excluded and might also bias the results. An extended evaluation time is needed to verify our findings. Furthermore, additional influencing factors like water temperature and the exact diving depth profile could not be considered in this analysis.
Conclusions
Using the ETFT, we were able to detect early changes in ET function in divers after repetitive dives in freshwater. Repetitive pressure exposure led to negative shift of the peak pressure in the middle ear. Less experienced divers showed significantly higher middle ear peak pressure and higher pressure differences after equalization manoeuvres. Higher middle ear peak pressure was also associated with higher barotrauma prevalence. The ETFT has proven to be a useful investigative tool during diving activities.
Footnotes
Acknowledgments
We thank the team at Actionsport Würzbung, especially Georg Seufert and Bernd Blümmert, and the OASIS Dive Centre (Nordhausen, Germany) for their support and the enthusiastic volunteer divers in this trial.
Conflict of interest: nil
Funding
Interacoustics A/S kindly loaned the Titan® tympanometer for the study.
Contributor Information
Stefanie Jansen, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Medical Faculty, Germany.
Manuela Boor, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Medical Faculty, Germany.
Moritz F Meyer, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Medical Faculty, Germany.
Eberhard D Pracht, German Center for Neurodegenerative Diseases (DZNE), Bonn, Germany.
Ruth Volland, Department of Paediatric Oncology and Haematology, University Children's Hospital of Cologne, Cologne, Germany.
Heinz D Kluenter, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Medical Faculty, Germany.
Karl-Bernd Hüttenbrink, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Medical Faculty, Germany.
Dirk Beutner, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Medical Faculty, Germany.
Maria Grosheva, Department of Otorhinolaryngology, Head and Neck Surgery, University of Cologne, Medical Faculty, Germany.
References
- Klingmann C, Praetorius M, Baumann I, Plinkert PK. Otorhinolaryngologic disorders and diving accidents: an analysis of 306 divers . Eur Arch Otorhinolaryngol. 2007;264:1243–51. doi: 10.1007/s00405-007-0353-6. [DOI] [PubMed] [Google Scholar]
- Kitajima N, Kitajima S. Altered Eustachian tube function in SCUBA divers with alternobaric vertigo . Otol Neurotol. 2014;35:850–6. doi: 10.1097/MAO.0000000000000329. [DOI] [PubMed] [Google Scholar]
- Uzun C. Evaluation of predive parameters related to Eustachian tube dysfunction for symptomatic middle ear barotrauma in divers . Otol Neurotol. 2005;26:59–64. doi: 10.1097/00129492-200501000-00010. [DOI] [PubMed] [Google Scholar]
- Ramos CC, Rapoport PB, Brito Neto RV. Clinical and tympanometric findings in repeated recreational scuba diving . Travel Med Infect Dis. 2005;3:19–25. doi: 10.1016/j.tmaid.2004.06.002. [DOI] [PubMed] [Google Scholar]
- Williams PS. A tympanometric pressure swallow test for assessment of Eustachian tube function . Ann Otol Rhinol Laryngol. 1975;84(3 Pt):339–43. doi: 10.1177/000348947508400309. [DOI] [PubMed] [Google Scholar]
- Spreitzer JB, Newman CW. Reliability of a measure of Eustachian tube function in normal subjects . Ann Otol Rhinol Laryngol. 1984;93:48–51. doi: 10.1177/000348948409300112. [DOI] [PubMed] [Google Scholar]
- Meyer MF, Boor M, Jansen S, Pracht ED, Felsch M, Klünter HD, et al. Influence of repetitive diving in saltwater on pressure equalization and Eustachian tube function in recreational scuba divers . Diving Hyperb Med. 2017;47:215–21. doi: 10.28920/dhm47.4.216-222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teed RW. Factors producing obstruction of the auditory tube in submarine personnel . United States Naval Medical Bulletin. 1944;42:293–306. [Google Scholar]
- Edmonds C. Otological aspects of diving. Sydney: Australasian Medical Publishing Company; 1973. [Google Scholar]
- Jerger J. Clinical experience with impedance audiometry . Arch Otolaryngol. 1970;92:311–24. doi: 10.1001/archotol.1970.04310040005002. [DOI] [PubMed] [Google Scholar]
- Azizi MH. Ear disorders in scuba divers . Int J Occup Environ Med. 2011;2:20–2. [PubMed] [Google Scholar]
- Molvaer OI, Natrud E. Ear damage due to diving . Acta Otolaryngol. 1979;360(Suppl):187–9. doi: 10.3109/00016487809123512. [DOI] [PubMed] [Google Scholar]
- Jansen S, Meyer MF, Boor M, Felsch M, Klünter HD, Pracht ED, et al. Prevalence and risk factors of barotrauma in recreational scuba divers after repetitive dives in salt water . Otol Neurotol. 2016;37:1325–31. doi: 10.1097/MAO.0000000000001158. [DOI] [PubMed] [Google Scholar]
- Mikolajczak S, Meyer MF, Hahn M, Korthäuer C, Jumah MD, Hüttenbrink KB, et al. Characterizing the active opening of the Eustachian tube in a hypobaric/hyperbaric pressure chamber . Otol Neurotol. 2015;36:70–5. doi: 10.1097/MAO.0000000000000575. [DOI] [PubMed] [Google Scholar]