

Abstract
The literature on rural-urban health disparities have mostly focused on de facto rural/urban differences, and its intersections with de jure rural-urban divide are less understood. This research provides a comprehensive investigation of how the intersection of rural\urban residence and rural\urban household registration (hukou) status is associated with a range of health outcomes in later life. We investigate major mechanisms in accounting for these health disparities across the life span. Results show that rural hukouers in rural areas were exposed to highest level of hardships and adversities throughout life and are disadvantaged in a variety of health measures. In urban areas, those who have obtained urban hukou are better off than rural hukouers in psychological well-being but have higher risks of diabetes. These differences are mainly explained by disparities in socioeconomic status between the two groups. We discuss these results in a life course perspective and in the context of China’s unique social, economic, and political settings.
Keywords: rural-urban health disparities, health outcomes, life course, hukou system, China
1. Introduction
Current literature on rural-urban disparities of health has mostly focused on inequalities created by geographical differences, such as differences in ecological environments, population densities, lifestyles, and socioeconomic status (SES) (Arcury, 2005, Hartley, 2004; Khan et al., 2012). However, there is not sufficient understanding of how social institutions, especially institutional discrimination may create health inequalities across the rural-urban line. This paper examines a type of institutional constraint – household registration system, or hukou system, in context of China, which for more than half a century of its implementation, has created a de jure rural-urban divide on top of the de facto rural-urban divide, and profoundly impacted life chances and experiences of every Chinese individual. Despite some weakening of the system in recent years, China is still struggling with legacy of the system today (Whyte, 2010).
Established in 1955 and promulgated in 1958, hukou system was first established as a form of social control to exclude rural population from access to state-allocated goods, welfare and entitlements (Chan, 2010). Once born, each person is assigned a hukou type (either agricultural (rural) hukou or non-agricultural(urban) hukou) based on place of birth and lineage (i.e. mother’s hukou type). A de jure rural-urban divide has been created as hukou system strictly bound individuals to land they were born for a few decades. The system differentiates opportunity structures for all Chinese by giving priority to urban hukou holders in almost every sphere, including education (L. Li, S. Li, & Chen, 2010), job opportunities (X. Wu & Treiman, 2004, 2007), housing (X. Wu & Treiman, 2004), health insurance (Liu, 2005), and other social services and provisions. With large rural-urban labor migration transpiring in recent decades, the rigid hukou system creates a distinct “floating population” in urban areas, which describes migrants who resided outside their household registration place for an extended period of time. The majority of them are rural-urban migrants who are ineligible for social entitlements associated with a local urban hukou, and face institutional discrimination, social stigma and marginalization in urban areas (J. Li & Rose, 2017; Logan, Fang, & Zhang, 2010). Thus, implications of rural-urban hukou divide well transcend spatial hierarchies of rurality and urbanity: it creates a citizenship stratification with a rural caste and an urban caste, with rural caste facing institutional and social discriminations (Cheng & Sheldon, 1994; Whyte, 2010).
Despite its role in creating an important dimension of social division and stratifying experiences of individuals throughout their life course, there is still limited knowledge on how hukou types create inequalities in various aspects of physical and psychological health, and how such inequalities unfold as individuals experience opportunities and circumstances delineated by their hukou types across life course. The hukou “footprint” on health is especially important for mid-aged and older Chinese, as their childhood experiences, identity, and life chances have been profoundly shaped by the hukou they were affiliated with, which have been an integral social structure that prescribed their institutional and geographical rights for most of their life. This study comprehensively examines life-course impact of hukou types on individual health.
To disentangle complex role of hukou system in creating health disparities in rural and urban China in later life, we focus on two comparisons. Due to decades of rural-urban segregation, urban and rural economic and social structure has been deeply entrenched into life of people who have always lived in rural or urban areas with same type of hukou. First, we focus on comparisons of two perpetual groups – “perpetual rural group” (rural hukouers in rural areas, thereafter) with “perpetual urban group”, those born in urban areas with urban hukou and remained so (urban-urban born, thereafter). Second, we examine and compare two urban resident groups in “mixed population” – those born with rural hukou but who later obtained urban hukou (urban-rural born, thereafter) and those who still had rural hukou (rural-urban migrants, thereafter). This comparison allows us to directly assess the role of hukou types in creating differentials in life chances and health disparities in urban space.
From a life course approach, we ask two major questions. First, how differences exist in mechanisms across their life span that may account for their current health inequalities compared to the other comparison group? These mechanisms range from childhood experiences and histories of healthcare access and behaviors, to current SES, family support, and local context. Second, how the groups in each comparison differ in current health in terms of a wide range of health conditions (self-rated health, physical impairment, psychological well-being, and chronic diseases), and how these mechanisms account for such health differences.
2. Background
The implementation of hukou system has undergone several stages. In socialist era (before late 1970s), through “food rationing system” in urban areas (which ended in 1992), urban hukou holders were eligible for food rations that were stable across the years, greater in quantity, and more various than rural hukou holders (Cheng & Sheldon, 1994). Rural residents were tied to the land to produce an agricultural surplus, and were left to deal with volatility of agricultural production, and with usually poorly resourced self-reliant villages for any resource allocation (Chan, 2010). Only people with urban hukou were entitled to have access to state employment assignment and key social resources and services, such as “housing, food, water, sewage disposal, transportation, medical facilities, police protection, schools, and other essentials and amenities of life” (Banister, 1987: 328). Urban hukou granted entitlements such as quality healthcare, insurance, and childcare, while rural hukouers usually did not have access to health insurance and mainly relied on “barefoot doctors,” peasants who received a short-term medical training for healthcare (Zhang & Unschuld, 2008). Upward (rural-urban) hukou mobility was highly selective, with education being most important (X. Wu & Treiman, 2007).
Since late 1970s, hukou system was relaxed and allowed for free movement of people. This has brought about decades of greater rural-urban migration. However, reforms on hukou mobility have taken much smaller and slower steps. Since 1990s, hukou reform was decentralized to local governments, who have the autonomy to secure resources and experiment on hukou reforms (L. Wu, 2013). This has strengthened capacity of some major wealthy cities, such as Beijing, Shanghai, or Guangzhou, which are largest migrant receiving cities, in providing resources, social welfare and public services to their local urban hukou-holders. However, as traditional destinations of rural-urban migrants, these cities also have the strictest hukou policy and most draconian social policy towards migrants.
This reform has also left a sizable migrant population in these highly urbanized cities still holding a rural hukou. By 2010, the floating population, most of whom are rural-urban migrants, comprised 17% (221 million) of total Chinese population (China Statistics Press, 2012). Rural-urban migrants are particularly vulnerable to potential downfalls in the city as they are largely excluded from social security programs, such as social assistance programs (e.g., minimum living guarantee), social welfare (e.g., disability benefits), and social insurance1 (Xu, Guan, & Yao, 2011). Rural migrants face occupation segregations with urban hukou holders, with rural migrants highly concentrated in occupations that are physically demanding, difficult, and dangerous (3D jobs), and usually face hiring discrimination, wage discrimination, and have a much higher probability to face wage arrears (Meng & Zhang, 2001). In large metro areas with high housing prices, migrant workers usually have high level of residential segregation from local hukouers, with most of them reside in work-unit dormitories and construction camps in urban fringe (Logan, Fang, & Zhang, 2010). Moreover, migrant workers experienced various forms of stigmatization, such as labelling, stereotyping, social isolation, status loss, and discrimination, and are considered as a “second class” of urban citizens (Roberts, 1997; X. Li et al., 2006).
3. The Four Principles of Life Course Framework
The four principles of life course framework (Elder, 1998) provide as the theoretical guidance to inform the mechanisms and pathways connecting hukou types and health outcomes. The principle of “historical time and place” (Principle 1) emphasizes the historical and geographical contexts in shaping individual experience over their life-time. Urban-urban born and rural hukouers in rural areas have experienced disparate trajectories throughout their lives. While growing up, rural hukouers in rural areas would have less accessibility to medical care and resources and experienced lower nutrition, which might lead to lower childhood health than urban-urban born. They would also have high exposure of natural and political upheavals, such as Great Famine (1958-1962). The “timing of lives” (Principle 2) states that the impacts of events are contingent on their timing. This is important in that rural hukouers in rural areas, if at all, may start healthcare access and adopt good health behaviors (or forsak bad ones) at a later stage in life, contributing to worse health outcomes than urban-urban born.
The “linked lives” (Principle 3) principle accentuates the interdependency of families. This is especially important for older rural hukouers in rural areas, whose adult children, their major elder support, migrated to urban areas. Being left behind in rural areas would contribute to more depressive symptoms and lower self-rated health for older rural adults (Silverstein, Cong, & Li, 2006; Song, 2017). The “human agency principle” (Principle 4) emphasizes actions individuals take within constraints and opportunities prescribed by social circumstances. Urban-urban born are exposed to opportunities of greater range of occupations, which are usually higher in SES than those of rural hukouers in rural areas. Finally, the cumulative dis/advantage theory (CAD) may shed light on the relationships between these pathways. CAD argues that effects of risk factors accumulate over life course, and inequalities exist in early life experiences, abilities, and resources are intrinsically linked to different trajectories in late life outcomes, including health (Elder, 1994). Consistent with CAD, these disadvantages associated with rural residence and hukou may accumulate throughout the lives of rural hukouers in rural areas, contributing to worse health outcomes than urban-urban born in middle and later life.
Similarly, the four principles of life course approach can also inform health disparities and their mechanisms between hukou converters and non-converters in urban areas. Being denied of urban citizenship and suffering from insecurities of work and life, rural-urban migrants may not have access to healthcare until much later in life, if at all, and to cope with stress, more likely to adopt unhealthy behaviors, such as smoking, than urban hukou converters (Cui et al., 2012) (Principle 2). The contingency status associated with a rural hukou may render migrants leave their families behind in rural areas, reducing their family support (Principle 3). Rural hukou status further constrained rural-urban migrants life opportunities in urban areas, creating occupational segregation with urban hukouers (Logan, Fang, & Zhang, 2010) (Principle 4). Decentralization of hukou reform since the 1990s provides each city/county a “historical place” (Principle 1) where localized hukou policies have created various meso environments, such as physical and social environments and general living conditions for migrants, shaping disparate migrant experience across counties. For example, rural-urban migrants historically tend to concentrate in large metro areas with more draconian hukou policies, which exposed them to poor working and living conditions (Logan, Fang, & Zhang, 2010). But recently developed and smaller cities may offer more generous social policies and provide better living conditions for migrants. These variations in localized hukou policies may cause repercussions in the health of rural-urban migrants.
4. Data and Methods
4.1. Data
We combine China Health and Retirement Longitudinal Study (CHARLS) 2015 with CHARLS 2014 life history data. CHARLS is a high-quality nationally representative sample of Chinese residents age 45 and older living in continental China. In national baseline survey, 150 county-level units from 28 provinces were randomly chosen, adopting multi-stage stratified Probability Proportional to Size (PPS) sampling. The sampling frame contains all county-level units (with exception of Tibet), and is stratified by region and urban districts, rural counties and per capita statistics. Within each county-level unit, 3 primary sampling units (PSUs), either villages in rural areas or neighborhoods in urban areas, were chosen. Individuals and their spouses were sampled with condition that such individual is aged 45 or older (their spouses can be less than age 45). The baseline yielded 17,708 individual participants from 10,257 households (Zhao et al., 2012). Among participants, 78.9% provided anthropometric and physical performance measures, and 67.0% provided samples of fasting blood. Biomarkers from blood were collected and analyzed at China CDC. CHARLS also contain socio-economic factors, health behaviors, childhood circumstances, community environment, social and family support, and health care and insurance.
In 2014, a special life history survey was conducted. The life history survey samples all living respondents in first two waves, and includes modules of residence, demographic backgrounds, family information, education history, health history and health care history, wealth history, and work history. This includes individual’s each migration trip, work experiences, and history in hukou conversion. Follow-up rate is high across waves. By Wave 3 (2015), panel response rate is 87.15%. The large sample size provided by this dataset allows for incorporating an extensive range of control variables. Our final sample varies slightly (16,437-17,817 respondents) by specific health measures due to missing values2.
4.2. Construction of key variables
We define “rural hukouers” as respondents who reported they currently have agricultural hukou, and “urban hukouers” as those who reported to have nonagricultural hukou or unified residence hukou. Types of place of residents are based on administrative records where living in village indicates rural areas, and living in community or both village and community as urban areas. We interact these variables taking account of hukou conversion history, and develop a comprehensive categorization of middle and older aged Chinese: rural hukouers in rural areas, urban hukouers born in urban areas and living in urban areas (i.e., urban-urban born), urban hukouers in rural areas, and finally, two urban residential groups with rural origins, one of which has obtained urban hukou (i.e., urban-rural born), and one still having rural hukou (i.e., rural-urban migrants). We focus on two pairs of comparisons – two “perpetual” groups: rural hukouers in rural areas and urban-urban born, and two “mixed” groups: urban-rural born and rural-urban migrants.
4.3. Analytical strategy
In the first step of analysis, we predict the possible pathways through which hukou and residential types intersect to contribute to health of individuals in later life, using basic demographic characteristics and educational attainment. Next, we examine health disparities between comparison groups on a wide range of health measures. We first show models controlling for demographic attributes and educational attainments. To examine how mechanisms account for health disparities, we show models incorporating childhood health and experiences, and models further incorporating histories of healthcare access and health behaviors and SES. Finally, we use fixed effects models at county level to investigate the role of various social environments created by localized hukou policies. The cluster option is used in STATA to adjust for within-household correlation. Survey weights are used in descriptive analysis.
4.4. Demographic characteristics, family contexts and experiences across the life course
Demographic characteristics include gender, age, and educational levels. Age is grouped into five categories: younger than 50, 50-59, 60-69, 70-79, 80 and older. Educational levels are measured with highest degrees obtained, including no education, primary school, middle school, high school, and college or higher. Childhood health includes self-rated health in childhood and two other questions (ever confined to bed in childhood, ever hospitalized for a month or more before age 16). Self-rated childhood health ranges from 0 to 4, indicating “much less healthy” to “much healthier” as compared to other children of same age. Childhood experiences include healthcare resources in childhood (accessibility to a usual source of care before age 15), and whether respondent and their family experienced starvation during Great Famine period (1958-1962).
Histories of healthcare access include three aspects. Time of getting first health insurance is categorized by age groups and current status (had health insurance at or before age 41 (reference), had insurance after age 41, never had insurance). The last time getting physical exam is constructed to show last physical exam happened more than two years ago (reference), in the past two years, and never had physical exams. Inadequate hospitalization indicates that in past year, whether respondent was told by a doctor should be hospitalized but did not, or released from hospital earlier than should be.
Health behaviors over the life course include smoking and drinking histories and a measure for improving health behaviors starting in mid-life. These measures include whether or not respondent ever smoked, is currently smoking, ever consumed alcohol, consumed alcohol in last year, and whether or not the respondent adopted healthier lifestyles after age 41 (coded 1 if reported “yes” to any of following: after age 41, increased physical activity, changed into a healthier diet, stopped smoking, reduced alcohol consumption).
Family context is captured by living arrangements (living alone vs. living with others). SES includes annual household expenditure per capita, Communist Party membership, and current or last job categories. Two principal measures of household economic resources are available in CHARLS—income and consumption expenditures. Household expenditure is collected in CHARLS since the literature has shown that expenditure is a much better welfare measure than income in developing countries, such as China (Strauss & Thomas, 2008). Consumption expenditure is believed to suffer much less from measurement error than income measures in survey data for these countries. The main reason for this is that in developing countries, such as China, many people have zero incomes since they do not work for money but work in kind in the agricultural sector or in family own business. These people, who are a significant part of the population, have zero incomes but positive consumption expenditures. Communist Party membership is associated with social, political and occupation mobility (X. Wu & Treiman, 2007), and is closely correlated with an urban hukou. Job categories include the occupations of current work or in the case of retirement, the most recent work. We regrouped the categories to indicate agricultural work (reference), government or public institutions, private firms, self-employed, and others, most of which are never working status or engaging in sideline work. Ordered logit regression is used to predict self-rated childhood health, OLS regression is used to predict annual household expenses, and multinomial regressions are used to predict categories of health insurance, physical exam, and occupation. Logit regressions are used to predict other variables.
4.5. Health measures
We examine a wide range of physical and mental health. Self-rated health (SRH) is reverse coded so that a higher score indicates better health (0-4 indicating very poor to very good). Physical impairment is measured by instrumental activities of daily living (IADLs), which is measured by summing up levels of difficulty in performing certain daily tasks (0 indicates do not have any difficulty, 4 indicates cannot do it at all). Depressive symptoms in CHARLS adopt CES-D 10, with 10 questions asking how often respondents experience these symptoms3. Answers range from “rarely or none of the time” to “most or all of the time.” We recoded some of the answers and took means such that larger values indicate more depressive symptoms. Chronic conditions include hypertension and diabetes. We combine diagnosed conditions with anthropometric measures and biomarkers collected in the field in CHARLS to measure these illnesses4. Details on all variable constructions are in Appendix A.
5. Descriptive results
Figure 2 shows distribution of all individuals in our sample (45+ years old) according to their hukou and residential types, weighted by sampling and nonresponses. The majority of population are rural hukouers in rural areas (63.6%), followed by urban residents born with urban hukou (11.7%). Rural residents with urban hukou constitute a small percentage (3.7%). In urban areas (Figure 3), hukou converters comprise 11.4%, and 9.6% are those who still hold rural hukou. The urban-urban born is a minority of current urban population – nearly 30% of current urban residents hold rural hukou, and 35% are hukou type converters, with merely 36% being “perpetual” urban residents. Among urban groups with rural origins, nearly half (46%) still have rural hukou. Such a high departmentation suggests China’s rapid urbanization and a high heterogeneity in early life experiences and opportunity structures among current middle-aged and older urban population.
Figure 2.
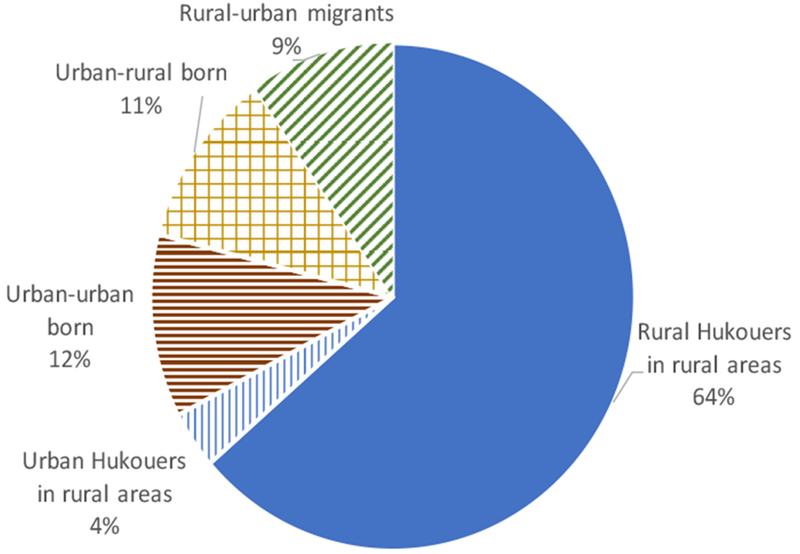
Distribution of All Individuals based on Place of Residence and Hukou, 45+, CHARLS 2014, 2015
Figure 3.
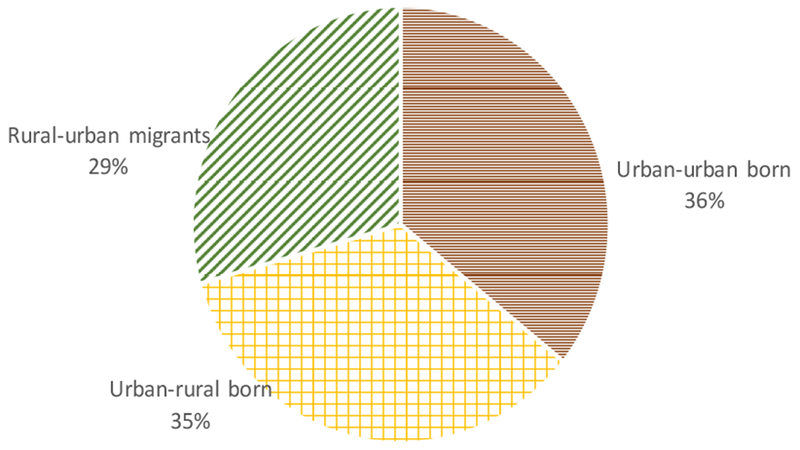
Distribution of Urban Residence based on Hukou Histories, 45+, CHARLS 2014, 2015
Table 1 describes distribution of respondents in sample according to their demographic characteristics, educational attainment, and mechanisms for health outcomes. Slightly more women (52.5%) than men are in sample, with slightly less than half (46.2%) of respondents aged 60 or older. The largest category of educational attainment is primary school (39.5%), followed by middle school (25.8%) and no schooling (20.7%). Approximately 81.7% of respondents and their families experienced starvation during Great Famine during 1958-1962. The majority (78.7%) obtained first insurance after 41 years old in life, probably attributed to New Rural Cooperative Medical Scheme that was introduced in 2003 and extended to most rural residents by 2010. The percentage of those who never had physical exams remains to be relatively large (17.9%). In the past year, approximately 10.9% of them did not receive adequate hospitalization.
Table 1.
Description of Sample
| % or mean | |
|---|---|
| Demographic Characteristics | |
| Male | 47.5 |
| Age Categories | |
| <50 years old | 22.6 |
| 50-59 years old | 31.2 |
| 60-69 years old | 28.8 |
| 70-79 years old | 13.2 |
| 80+ years old | 4.2 |
| Education Attainment | |
| No education | 20.7 |
| Primary school | 39.5 |
| Middle school | 25.8 |
| High school | 11.1 |
| College or higher | 2.9 |
| Childhood Health and Resources | |
| Self-rated health in childhood | |
| Much less healthy | 5.1 |
| Somewhat less healthy | 8.0 |
| About average | 51.8 |
| Somewhat healthier | 18.5 |
| Much healthier | 16.7 |
| Ever confined to bed in childhood | 5.6 |
| Ever hospitalized for a month or more | 2.3 |
| Experienced starvation during the Great Famine (1958-1962) | 81.7 |
| Had access to a usual source of care before 16y | 9.3 |
| Healthcare Utilization | % or mean |
| Time of getting first health insurance | |
| Had insurance before or at 41 y | 17.9 |
| Had insurance after 41 y | 78.7 |
| Never had insurance | 3.4 |
| Last time taking a physical exam | |
| In the past two years | 41.7 |
| More than two years ago | 40.4 |
| Never had physical exam | 17.9 |
| Inadequate hospitalization in the last year | 10.9 |
| Health Behaviors | |
| Ever smoked | 37.5 |
| Currently smoke | 28.1 |
| Ever drunk alcohol | 45.9 |
| Currently drink alcohol | 31.7 |
| Adopted healthier lifestyle after 41 y | 30.5 |
| Family Contexts and SES | |
| Living alone | 9.1 |
| Household per capita expenditure(yuan) | 1611.0 |
| Party Membership | 18.6 |
| Current or Last Job Categories | |
| Agriculture | 54.9 |
| Government or public institution | 7.8 |
| Private firms | 15.7 |
| Self-employed | 18.8 |
| Never worked or done sideline work | 3.3 |
Table 2 reports five health measures of individuals by their hukou and residential types. Panel A shows comparisons between rural hukouers in rural areas and all other groups. Panel B shows the comparison between hukou converters and nonconverters in urban areas. T-tests are carried out for self-rated health, IADLs, and depression symptoms; proportion tests are carried out for hypertension and diabetes. First, we observe that urban-urban born have advantages over rural hukouers in rural areas in terms of SRH, IADLs, and psychological well-being, but are more likely to have measured and diagnosed hypertension and diabetes. In fact, all other groups also have better SRH and psychological well-being, but more likely to have hypertension than rural hukouers in rural areas. Second, when two urban groups with rural origins are compared, both groups have similar levels of SRH and IADLs, but rural-urban migrants have more depressive symptoms, and less likely to have hypertension and diabetes.
Table 2.
Health Status by Hukou and Residential Types
| Panel A. Comparing Groups with Rural Hukouers in Rural Areas | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Rural Residents | Urban Residents | ||||||||
| Health Measures | Rural Hukouers | Urban Hukouers | Diffa. | Urban Hukouers, Urban Born | diffa. | Urban Hukouers, Rural Born | diffa. | Rural Hukouers | Diffa. |
| Self-rated health | 3.04 | 3.17 | *** | 3.22 | *** | 3.2 | *** | 3.17 | *** |
| IADLs | 4.94 | 3.51 | *** | 3.4 | *** | 4.06 | 4.25 | ||
| Depression Symptoms | 0.86 | 0.66 | *** | 0.63 | *** | 0.65 | *** | 0.75 | *** |
| Hypertension | 0.38 | 0.43 | ** | 0.44 | *** | 0.45 | *** | 0.41 | * |
| Diabetes | 0.13 | 0.16 | * | 0.17 | *** | 0.18 | *** | 0.14 | |
| Panel B. Comparing Hukou Converters and Rural Hukouers in Urban Residence | |||
|---|---|---|---|
| Health Measures | Urban Hukouers, Rural Born | Rural Hukouers | Diffb. |
| Self-rated health | 3.2 | 3.17 | |
| IADLs | 4.06 | 4.25 | |
| Depression Symptoms | 0.65 | 0.75 | *** |
| Hypertension | 0.45 | 0.41 | * |
| Diabetes | 0.18 | 0.14 | *** |
Diff: reference group is rural hukouers in rural areas.
Diff: reference group is rural hukouers in urban areas (hukou non-converters).
Note: t-tests are carried out for self-rated health, IADLs, and depression symptoms; proportion tests are carried out for hypertension and diabetes.
p<0.001
p<0.01
p<0.05
p<0.1
6. Regression results
6.1. Mechanisms
We first examine and predict each pathway through which rural\urban hukou and residential types may get under the skin. Outcomes in Tables 3 are shown in each row after controlling for demographic and education characteristics (full results in Appendix B). In terms of childhood health and experiences, according to Panel A, urban-urban born did not have a statistically significant better self-rated childhood health than rural hukouers in rural areas, but were more likely to have usual source of care, and less likely to experience hunger during Grant Famine Period. The urban-urban born were more likely to be hospitalized, suggesting better accessibility to a hospital in childhood than rural hukouers in rural areas. Both being in rural areas, those born with urban hukou did not seem to have a health or healthcare advantage in childhood than rural hukouers.
Table 3.
Regression Results for Mechanisms (Modeling the Outcomes in Each Row)
| Panel A. Comparing Groups with Rural Hukouers in Rural Areasa | ||||
|---|---|---|---|---|
| Rural Residence | Urban Residence | |||
| Urban hukouers | Urban Hukouers, Urban Born | Urban Hukouers, Rural Born | Rural Hukouers | |
| Childhood Health and Experiences | ||||
| Self-rated childhood health (0-4) | −0.037 | 0.047 | 0.198*** | 0.067 |
| Not having usual source of care in childhood | −0.173 | −0.996*** | 0.128 | −0.073 |
| Experienced hunger during the Great Famine (1958-1962) | −0.104 | −0.730*** | −0.037 | −0.016 |
| Ever confined to bed in childhood | −0.044 | −0.074 | 0.005 | −0.234+ |
| Ever hospitalized for 1 month or more in childhood | 0.140 | 0.395* | 0.329+ | −0.092 |
| Healthcare Access | ||||
| Time of first health insurance (ref. before 41 years old) | ||||
| First health insurance after 41 years old | −1.465*** | −2.312*** | −1.639*** | 0.341*** |
| Never had health insurance | −0.160 | −0.932*** | −0.818*** | 0.444** |
| Time of last physical exam (ref. <=2 years ago) | ||||
| Last physical exam >2 years ago | −0.238** | −0.394*** | −0.609*** | −0.208** |
| Never had physical exam | −0.585*** | −0.676*** | −0.952*** | −0.263** |
| Inadequate hospitalization | 0.084 | 0.109 | 0.017 | 0.103 |
| Health Behaviors | ||||
| Ever smoked | −0.074 | −0.402*** | −0.396*** | −0.210** |
| Currently smoke | −0.119 | −0.378*** | −0.512*** | −0.159* |
| Ever drunk alcohol | 0.0282 | −0.003 | 0.0435 | 0.016 |
| Currently drink alcohol | −0.064 | 0.059 | 0.003 | 0.024 |
| Adopted healthier lifestyle after 41 years old | 0.407*** | 0.812*** | 0.888*** | 0.327*** |
| Family Contexts and Socioeconomic Status | ||||
| Living alone | −0.232+ | −0.388*** | −0.565*** | −0.316** |
| Annual household expenditure (logged) | 0.204*** | 0.332*** | 0.248*** | 0.063+ |
| Party membership | 0.802*** | 0.332*** | 0.985*** | 0.072 |
| Occupation (ref. agriculture) | ||||
| Government/public sector | 2.315*** | 4.630*** | 3.413*** | 1.293*** |
| Private firms | 1.458*** | 4 927*** | 3.204*** | 0.829*** |
| Self-employed | 0.631*** | 3.701*** | 2.241*** | 1.042*** |
| Other | 0.575* | 3.572*** | 1.880*** | 0.588*** |
| Panel B. Comparing Hukou Converters and Rural Hukouers in Urban Residenceb | |
|---|---|
| Urban Hukouers, Rural Born (Hukou Converters) | |
| Childhood Health and Experiences | |
| Self-rated childhood health (0-4) | 0.131+ |
| Not having usual source of care in childhood | −0.022 |
| Experienced hunger during the Great Famine (1958-1962) | 0.200 |
| Ever confined to bed in childhood | 0.239 |
| Ever hospitalized for 1 month or more in childhood | 0.422+ |
| Healthcare Access | |
| Time of first health insurance (ref. before 41 years old) | |
| First health insurance after 41 years old | −1.298*** |
| Never had health insurance | −1.262*** |
| Time of last physical exam (ref. <=2 years ago) | |
| Last physical exam >2 years ago | −0.402*** |
| Never had physical exam | −0.689*** |
| Inadequate hospitalization | −0.086 |
| Health Behaviors | |
| Ever smoked | −0.187+ |
| Currently smoke | −0.352*** |
| Ever drunk alcohol | 0.0274 |
| Currently drink alcohol | −0.021 |
| Adopted healthier lifestyle after 41 years old | 0.562*** |
| Family Contexts and Socioeconomic Status | |
| Living alone | −0.249+ |
| Annual household expenditure (logged) | 0.186*** |
| Party membership | 0.913*** |
| Occupation (ref. agriculture) | |
| Government/public sector | 2.120*** |
| Private firms | 2.375*** |
| Self-employed | 1.199*** |
| Other | 1.291*** |
reference group is rural hukouers in rural areas.
reference group is rural hukouers in urban areas (hukou non-converters).
p<0.001
p<0.01
p<0.05
p<0.1
There is evidence of selectivity on childhood health for two urban groups with rural origins. The urban-rural born have better self-rated childhood health, and rural-urban migrants are less likely to be confined to bed in childhood than rural-rural born, suggesting both hukou conversion and migration are positively selected on individual childhood health. It’s worth noting that when two urban groups with rural origins are compared (Panel B), hukou converters have better self-rated childhood health (p<0.1), suggesting that hukou conversion has a stronger health selection in childhood health than simply migrating to urban areas.
In terms of healthcare utilization, Panel A reveals that as expected, all other groups, especially urban-urban born have better healthcare access than rural hukouers in rural areas. There is one striking exception – rural-urban migrants, though are more likely to have health insurance coverage early in life and take more frequent physical exams, are less likely to have ongoing health insurance than rural hukouers in rural areas. This underlines dreadful situation for rural-urban migrants in urban areas. When two urban groups with rural origins are compared, hukou converters in urban areas have a clear and significant advantage in healthcare access than their counterparts who haven’t converted their hukou type.
Comparing health behaviors, urban-urban born have an advantage – they are less likely to smoke or have a smoking history, and more likely to adopt healthier lifestyles in or after mid-life. Both with rural origins, hukou converters have better health behaviors than urban migrants with rural hukou – they are less likely to smoke or start smoking, and more likely to adopt a healthier lifestyle later in life. Supplemental analysis (full results in Appendix C) identifies and predicts specific health behaviors that individuals adopted. Results show that differences observed regarding health behaviors are mostly derived from differences in increasing physical activities and adopting a healthier diet. It should be noted, though, that these healthier lifestyles they adopted later in life is in comparison with themselves earlier in time.
Rural hukouers in rural areas are consistently at bottom of SES rung in terms of household consumptions, party membership, and occupation. They are more likely to live alone, a less preferred living arrangement in China. Interestingly, both living in rural areas, urban hukouers are also less likely to live alone than rural hukouers. Between two urban groups with rural origins, there are significant SES differences with hukou converters advantageous in all measures examined here. The hukou converters are less likely to live alone, suggesting more social support from family for them than for urban migrants with rural hukou.
6.2. Health
Models in Table 4 summarize regression results predicting health while controlling for basic demographic characteristics and education (full results from Tables 4–6 are in Appendix D–G respectively). Each row represents a modeling outcome. Compared to rural hukouers in rural areas (Panel A), urban-urban born, as well as other comparison groups have better self-rated health, less physical impairments and depressive symptoms, but are more likely to be hypertensive and diabetic. When two urban groups with rural origins are compared (Panel B), hukou converters have significantly less depressive symptoms, but more risks of diabetes.
Table 4.
Regression Results Predicting Health Controlling for Demographic Characteristics and Education (Modeling the Outcomes in Each Row)
| Panel A. Comparing Groups with Rural Hukouers in Rural Areasa | ||||
|---|---|---|---|---|
| Rural Residence | Urban Residence | |||
| Urban hukouers | Urban Hukouers, Urban Born | Urban Hukouers, Rural Born | Rural Hukouers | |
| SRH | 0.078* | 0.121*** | 0.130*** | 0.121*** |
| IADL | −0.827*** | −0.721*** | −0.608*** | −0.385* |
| Depression | −0.111*** | −0.128*** | −0.155*** | −0.091*** |
| Hypertension | 0.135+ | 0.265*** | 0.251*** | 0.192** |
| Diabetes | 0.205+ | 0.292** | 0.353*** | 0.041 |
| Panel B. Comparing Hukou Converters and Rural Hukouers in Urban Residenceb | ||
|---|---|---|
| Urban Hukouers, Rural Born (Hukou Converters) | ||
| SRH | 0.010 | |
| IADL | −0.223 | |
| Depression | −0.064** | |
| Hypertension | 0.059 | |
| Diabetes | 0.312* | |
reference group is rural hukouers in rural areas.
reference group is rural hukouers in urban areas (hukou non-converters).
p<0.001
p<0.01
p<0.05
p<0.1
Table 6.
Regression Results Predicting Health Controlling for Demographic Characteristics, Education, Childhood Health, Healthcare Utilizations, Health Behaviors, Family Contexts, and SES, Fixed Effects (Modeling the Outcomes in Each Row)
| Panel A. Comparing Groups with Rural Hukouers in Rural Areasa | ||||
|---|---|---|---|---|
| Rural Residence | Urban Residence | |||
| Urban Hukouers | Urban Hukouers, Urban Born | Urban Hukouers, Rural Born | Rural Hukouers | |
| SRH | 0.085* | 0.029 | 0.042 | 0.064+ |
| IADL | −0.559** | −0.524* | −0.242 | −0.294 |
| Depression | −0.095*** | −0.052* | −0.079*** | −0.051* |
| Hypertension | 0.103 | 0.218* | 0.182* | 0.058 |
| Diabetes | 0.070 | 0.093 | 0.068 | −0.028 |
| Panel B. Comparing Hukou Converters and Rural Hukouers in Urban Residenceb | |
|---|---|
| Urban Hukouers, Rural Born (Hukou Converters) | |
| SRH | −0.021 |
| IADL | 0.052 |
| Depression | −0.028 |
| Hypertension | 0.125 |
| Diabetes | 0.096 |
reference group is rural hukouers in rural areas.
reference group is rural hukouers in urban areas (hukou non-converters).
p<0.001
p<0.01
p<0.05
p<0.1
To assess pathway of childhood health and experiences, Models in Table 5A further incorporate childhood variables as controls. Results show that none of the differences observed previously in two pairs of comparisons is explained away by childhood alone. This suggests that differences in childhood health, resources, and experiences do not play an important role in creating hukou and residential related health disparities.
Table 5A.
Regression Results Predicting Health Controlling for Demographic Characteristics, Education and Childhood Health/Experiences (Modeling the Outcomes in Each Row)
| Panel A. Comparing Groups with Rural Hukouers in Rural Areas | ||||
|---|---|---|---|---|
| Rural Residence | Urban Residence | |||
| Urban hukouers | Urban Hukouers, Urban Born | Urban Hukouers, Rural Born | Rural Hukouers | |
| SRH | 0.081* | 0.097*** | 0.113*** | 0.108*** |
| IADL | −0.774*** | −0.606*** | −0.564*** | −0.341* |
| Depression | −0.110*** | −0.111*** | −0.149*** | −0.088*** |
| Hypertension | 0.152+ | 0.250*** | 0.248*** | 0.195** |
| Diabetes | 0.207+ | 0.300** | 0.358*** | 0.042 |
| Panel B. Comparing Hukou Converters and Rural Hukouers in Urba Residenceb | |
|---|---|
| Urban Hukouers, Rural Born (Hukou Converters) | |
| SRH | 0.005 |
| IADL | −0.224 |
| Depression | −0.062** |
| Hypertension | 0.053 |
| Diabetes | 0.316* |
reference group is rural hukouers in rural areas.
reference group is rural hukouers in urban areas (hukou non-converters).
p<0.001
p<0.01
p<0.05
p<0.1
Models in Table 5B continue to include healthcare utilization, health behaviors, family contexts, and SES as controls. A comparison with models in Table 5A shows that first, as shown in Panel A, these factors explained physical health disparities between rural hukouers in rural areas and urban-urban born in terms of SRH and IADLs. They explained physical activity advantages of other groups, as well as higher risks of hypertension and diabetes for urban hukouers in rural areas compared to rural hukouers in rural areas. Supplemental analyses incorporating factors in an additive manner show that SES has most powerful explanation power (full results of models leaving out SES variables are in Appendix H). Second, according to Panel B, mental health disparities and differences in risks of diabetes for hukou converters and nonconverters in urban areas have also been explained away by these factors. Supplemental analyses show that differences in both histories of healthcare access and SES have contributed to these disparities between the two groups (full results of models leaving out healthcare access and SES variables are in Appendix I).
Table 5B.
Regression Results Predicting Health Controlling for Demographic Characteristics, Education, Childhood Health, Healthcare Utilizations, Health Behaviors, Family Contexts, and SES (Modeling the Outcomes in Each Row
| Panel A. Comparing Groups with Rural Hukouers in Rural Areasa | ||||
|---|---|---|---|---|
| Rural Residence | Urban Residence | |||
| Urban hukouers | Urban Hukouers, Urban Born | Urban Hukouers, Rural Born | Rural Hukouers | |
| SRH | 0.074* | 0.037 | 0.052+ | 0.093** |
| IADL | −0.498** | −0.088 | −0.039 | −0.122 |
| Depression | −0.077*** | −0.046* | −0.078*** | −0.072*** |
| Hypertension | 0.105 | 0.235** | 0.203** | 0.179* |
| Diabetes | 0.123 | 0.191+ | 0.207* | 0.037 |
| Panel B. Comparing Hukou Converters and Rural Hukouers in Urban Residenceb | |
|---|---|
| Urban Hukouers, Rural Born (Hukou Converters) | |
| SRH | −0.041 |
| IADL | 0.083 |
| Depression | −0.006 |
| Hypertension | 0.025 |
| Diabetes | 0.170 |
reference group is rural hukouers in rural areas.
reference group is rural hukouers in urban areas (hukou non-converters).
p<0.001
p<0.01
p<0.05
p<0.1
Fixed effects at county level are further added in models in Table 6. Compared with results in Table 5B (Panel A), one change is that local environment where rural-urban migrants live attenuated their higher risks of hypertension compared to rural hukouers in rural areas, suggesting the important role of localized hukou policy and environment in shaping migrants’ blood pressure. The cities where people reside explained away higher risks of diabetes among urban-urban born areas but suppressed their advantages in IADLs compared to rural hukouers in rural areas. These findings highlight the import of city environment in mediating urban-urban born’s diet and lifestyles.
7. Conclusion
Despite the social transformations that happened in past few decades in China, hukou system remains an important institutional constraint on individuals. How do individuals experience their hukou identity and how does hukou status get under the skin and stratify their health and wellbeing in later life? Our answers lie in their childhood resources and experiences, histories of healthcare access and health behaviors throughout their life, SES and family contexts, and how intersections of their hukou histories and place of residents stratify ways in which individual experience these circumstances, with outcomes depending on specific health conditions.
Overall, rural hukouers in rural areas have accumulated highest level of hardships and adversities, especially when they are compared with urban-urban born: from starvation and limited healthcare access in early life, to unhealthy behaviors and timing of behavior change, reduced family support, and low SES throughout their life course. This supports the pathways we proposed lying between rural hukouers in rural areas and urban-urban born, and offers strong evidence to support the four principles of life course framework. From childhood to adult life, rural hukouers in rural areas are confined by limited accessible resources and opportunities. The vulnerabilities resulting from these deprivations have set them off with a life trajectory conducing to adverse health in middle and later life, compared to urban-urban born. This offers support of accumulative dis/advantage theory. Differences in SES is proved to be the major pathway through which rural hukouers in rural areas are disadvantaged in a variety of health measures.
At the same time, after considering all mechanisms examined here, there are still unexplained health inequalities between the two groups. Reasons for these disparities can be inequalities in resources in rural and urban China – rural China has limited accessibility to sewage water, flushing toilet, and higher water pollution (Wang et al., 2008), as well as resources and social status conferred by having rural/urban hukou, such as differences in number and quality of healthcare and facilities that a rural or urban health insurance covered (Shi, 1993). In addition, increased stress associated with financial insecurity and lower social identity of having rural hukou and living in rural areas may matter.
Rural-urban migration plays an important role in determining wellbeing of rural hukouers in both rural and urban areas. First, rural hukouers in rural areas are most likely to be in most detrimental living arrangement in China – solitary living, which is likely to come from outmigration of their spouses and/or children, who migrated to cities for higher pay. Urban hukouers in rural areas are comparatively better off in this regard, probably because their families may have better opportunities in securing the preferable local employment jobs than do rural hukouers. Second, in urban areas, rural hukouers have higher level of solitary living compared to hukou converters. This might reflect rural hukouers’ transitory life stage. Given their adverse conditions in urban areas, they tend to leave their families behind in rural areas. For these middle aged and older migrants, living alone in an urban environment without sufficient protections from the state may be an increasing concern for urban social inequality.
In urban spaces, rural hukouers have pronounced disadvantages in accessing healthcare and SES throughout their life than hukou converters. These are direct consequences of discriminatory hukou-based social welfare system and employment in public sectors, which have largely created occupation segregation, excluded rural hukouers from state provided local healthcare, and set institutional barriers for rural hukouers to upward mobility in workplace (Meng & Zhang, 2001; Xu, Guan, & Yao, 2011). Rural hukouers’ reluctance to adopt healthier behaviors in later in life compared to hukou converters may reflect their unstable social networks and higher stress levels derived from job and housing instability (Knight &Yueh, 2004; Pampel, Krueger, & Denney, 2010).
Our results also highlight county/city level heterogeneities in shaping health outcomes of individuals in China. The differences in social environment created by localized city hukou policies explained rural-urban migrants’ high risks of hypertension. Some major wealthy cities, such as Beijing or Shanghai, have the strictest hukou policies and most draconian social policies towards rural-urban migrants. Migrants may supper from high stress due to residential and occupational segregation and poor living and working conditions in these cities (Z. Li & Wu, 2008; Meng & Zhang, 2001). High stress is associated with elevated blood pressure (Touyz, 2004). Therefore, our results call for a policy change in cities with strict hukou policies in improving working and living conditions of rural-urban migrants. The exposure to highly urbanized metropolitan cities, where high sugar diet is more available and people are less physically active (Miao & Wu, 2016; Xu et al., 2013), might be the reason why places of residence are important for shaping diabetes of urban-urban born.
We also note that there is a silver lining for being a rural-urban migrant at mid-age or older. Compared with their counterparts who remained in rural areas, they take more frequent physical examinations and more likely to adopt a healthier lifestyle later in life and live with others. More recently, some social provisions in urban areas, such as free physical exams for older adults, are becoming increasingly embracive to all urban residents, regardless of their hukou status (Dayoo news, 2017). An urban environment can be more conducive to adopting healthy behaviors later in life, as urban culture is usually more health literate, and urban space is usually less friendly to unhealthy behaviors such as smoking. Certain urban spaces are utilized by middle aged and older adults for activities and exercises, such as “square dance”, which are beneficial to their physical and mental health (L. Gao et al., 2016).
We note several limitations of the study. First, endogeneities may exist as both migration and hukou conversion can be positively selected on prior health and some latent individual characteristics. Previous research has found that hukou conversion selects the “best and brightest” of rural population (X. Wu & Treiman, 2004), and migration selects better physical health but not mental health (J. Chen, 2011). Though we also found evidence of positive selection on childhood health for hukou converters and migrants, we may not take full account of these selections in this study. Nevertheless, this study controlled a wide range of early life experiences and health variables, as well as used fixed effects models to take account of endogeneities lying in early life experiences and contextual characteristics, which have reduced issues of endogeneities. Second, selectivity on hukou conversion may vary by age, period, and cohort, and reasons of hukou conversion (Zhang & Treiman, 2013). Future research would benefit from investigating differences in individual early and later life experiences across life course by stratifying them according to these characteristics.
In recent years, hukou reforms continue to unfold at local levels. Provinces and cities have developed strategic plans to incorporate different hukou types into unified residence hukou. It is foreseeable that in the future the distinction of rural and urban hukou will become history. However, under current reforms, some major concerns persist. For rural-urban migrants who are mostly from counties outside their destinations – as social entitlements are still localized and confined to those who have a hukou in same county, the clear majority of rural-urban migrants are still not entitled for these public provisions. It is advisable that local urban governments in major migrant destinations develop plans to incorporate those migrants and their families in their welfare system. At the same time, industries and factories should move to counties and towns in migrant origins. This way, not only migrants’ social entitlements are naturally secured by local government of their hukou place, but opportunities for family reunion for migrants are improved. Finally, we call for more attention to accommodating needs of middle aged and older migrants, who are taking an increasing proportion of entire migrant population, with regard to their financial and social security, family support, and ways to improve their healthcare access and health behaviors.
Supplementary Material
Figure 1A.
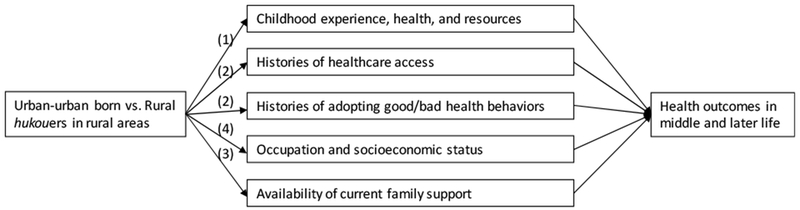
Life Course Approach: Pathways to Predict Health Disparities between Urban-urban Born and Rural Hukouers in Rural Areas in Middle and Later Life
Note: (1) historical time and place principle; (2) timing of lives principle; (3) linked lives principle; (4) human agency principle.
Figure 1B.
Life Course Approach: Pathways to Predict Health Disparities between Hukou Converters and Rural Hukouers in Urban Residence in Middle and Later Life
Note: (1) historical time and place principle; (2) timing of lives principle; (3) linked lives principle; (4) human agency principle.
Highlights.
We comprehensively assess how hukou status is associated with health in China.
Rural hukouers in rural areas are exposed to highest adversities throughout life.
For urban residents, health disparities exist for urban hukouers and rural hukouers.
Disparities in SES, healthcare access history, and local contexts are major mechanisms.
Equal access to social welfare for rural hukouers in rural and urban China is advised.
Acknowledgments
This research is partly supported by NIH 5T32AG000244.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Individuals are mostly only eligible for health insurance program in their hukou locations, and not able to get reimbursement of medical expenses in their destination cities. After 2010, migrant workers can get access to employment-based social insurance programs. However, due to employers’ low social security contribution rates, only 10% of migrants had actual coverage (Chan, 2012).
Sample size for diabetes is relatively smaller (13,178).
We did a robustness check for depression symptoms using a cutoff of 12 as threshold for clinically significant depression. Results are consistent with that using mean scores of depression symptoms.
The cutoffs for hypertension are 140mmHg for systolic readings and 90 mmHg for diastolic readings. Diabetes are defined as either having Hb1c >=6.5 or glucose >=126. Blood pressure is measured three times. Average values are taken.
Contributor Information
Qian Song, Department of Gerontology, University of Massachusetts Boston.
James P. Smith, Labor and Population, RAND Corporation
References
- Arcury TA, Preisser JS, Gesler WM, & Powers JM (2005). Access to transportation and health care utilization in a rural region. The Journal of Rural Health, 21(1), 31–38. [DOI] [PubMed] [Google Scholar]
- Banister J (1987). China’s changing population. Stanford: Stanford University Press. [Google Scholar]
- Brondolo E, Gallo LC, & Myers HF (2009). Race, racism and health: disparities, mechanisms, and interventions. Journal of behavioral medicine, 32(1), 1. [DOI] [PubMed] [Google Scholar]
- Chan KW (2010). The household registration system and migrant labor in China: Notes on a debate. Population and development review, 36(2), 357–364. [DOI] [PubMed] [Google Scholar]
- Cheng T, & Selden M (1994). The origins and social consequences of China’s hukou system. The China Quarterly, 139, 644–668. [Google Scholar]
- Chen J (2011). Internal migration and health: re-examining the healthy migrant phenomenon in China. Social Science & Medicine, 72(8), 1294–1301. [DOI] [PubMed] [Google Scholar]
- China Statistics Press. (2012). Tabulation on the 2010 Population Census of the People’s Republic of China. Beijing, China: China Statistics Press. [Google Scholar]
- Cui X, Rockett IR, Yang T, & Cao R (2012). Work stress, life stress, and smoking among rural-urban migrant workers in China. BMC Public Health, 12(1), 979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elder GH Jr (1994). Time, human agency, and social change: Perspectives on the life course. Social psychology quarterly, 4–15. [Google Scholar]
- Elder GH Jr (1998). The life course as developmental theory. Child development, 69(1), 1–12. [PubMed] [Google Scholar]
- Gao L, Zhang L, Qi H, & Petridis L (2016). Middle-aged female depression in perimenopausal period and square dance intervention. Psychiatria Danubina, 25(4), 372–378. [PubMed] [Google Scholar]
- Hartley D (2004). Rural health disparities, population health, and rural culture. American Journal of Public Health, 94(10), 1675–1678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dayoo news (2017). Retrieved May 28, 2019 from http://news.dayoo.com/guangzhou/201708/01/151407_51590738.htm.
- Khan NY, Ghafoor N, Iftikhar R, & Malik M (2012). Urban annoyances and mental health in the city of Lahore, Pakistan. Journal of Urban Affairs, 34(3), 297–315. [Google Scholar]
- Knight J, & Yueh L (2004). Job mobility of residents and migrants in urban China. Journal of comparative economics, 32(4), 637–660. [Google Scholar]
- Liu Z (2005). Institution and inequality: the hukou system in China. Journal of comparative economics, 33(1), 133–157. [Google Scholar]
- Li J, & Rose N (2017). Urban social exclusion and mental health of China’s rural-urban migrants-A review and call for research. Health & place, 48, 20–30. [DOI] [PubMed] [Google Scholar]
- Li L, Li SM, & Chen Y (2010). Better city, better life, but for whom?: The hukou and resident card system and the consequential citizenship stratification in Shanghai. City, Culture and Society, 1(3), 145–154. [Google Scholar]
- Li X, Stanton B, Fang X, & Lin D (2006). Social stigma and mental health among rural-to-urban migrants in China: A conceptual framework and future research needs. World health & population, 5(3), 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li Z, & Wu F (2008). Tenure-based residential segregation in post-reform Chinese cities: a case study of Shanghai. Transactions of the Institute of British Geographers, 33(3), 404–419. [Google Scholar]
- Logan JR, Fang Y, & Zhang Z (2010). The winners in China’s urban housing reform. Housing Studies, 25(1), 101–117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meng X, & Zhang J (2001). The two-tier labor market in urban China: occupational segregation and wage differentials between urban residents and rural migrants in Shanghai. Journal of comparative Economics, 29(3), 485–504. [Google Scholar]
- Miao J, & Wu X (2016). Urbanization, socioeconomic status and health disparity in China. Health & place, 42, 87–95. [DOI] [PubMed] [Google Scholar]
- Pampel FC, Krueger PM, & Denney JT (2010). Socioeconomic disparities in health behaviors. Annual review of sociology, 36, 349–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts KD (1997). China’s” tidal wave” of migrant labor: What can we learn from Mexican undocumented migration to the United States?. International Migration Review, 249–293. [PubMed] [Google Scholar]
- Silverstein M, Cong Z, & Li S (2006). Intergenerational transfers and living arrangements of older people in rural China: Consequences for psychological well-being. The Journals of Gerontology, Series B: Psychological Sciences & Social Sciences, 61(5), S256–S266. [DOI] [PubMed] [Google Scholar]
- Shi L (1993). Health care in China: a rural-urban comparison after the socioeconomic reforms. Bulletin of the World Health Organization, 71(6), 723. [PMC free article] [PubMed] [Google Scholar]
- Song Q (2017). Facing “Double Jeopardy”? Depressive Symptoms in Left-Behind Elderly in Rural China. Journal of aging and health, 29(7), 1182–1213. [DOI] [PubMed] [Google Scholar]
- Strauss J, & Thomas D (2008). Health over the life course, in Schultz TP and Strauss J (Eds), Handbook of development economics, Volume 4 Amsterdam: North Holland Press. [Google Scholar]
- Touyz RM (2004). Reactive oxygen species, vascular oxidative stress, and redox signaling in hypertension: what is the clinical significance?. Hypertension, 44(3), 248–252. [DOI] [PubMed] [Google Scholar]
- Wang M, Webber M, Finlayson B, & Barnett J (2008). Rural industries and water pollution in China. Journal of Environmental Management, 86(4), 648–659. [DOI] [PubMed] [Google Scholar]
- Whyte MK (Ed.). (2010). One country, two societies: rural-urban inequality in contemporary China (Vol. 16). Harvard University Press. [Google Scholar]
- Wu L (2013). Decentralization and hukou reforms in China. Policy and Society, 32(1), 33–42. [Google Scholar]
- Wu X, & Treiman DJ (2004). The household registration system and social stratification in China: 1955–1996. Demography, 41(2), 363–384. [DOI] [PubMed] [Google Scholar]
- Wu X, & Treiman DJ (2007). Inequality and equality under Chinese socialism: The hukou system and intergenerational occupational mobility. American Journal of Sociology, 113(2), 415–445. [Google Scholar]
- Xu Q, Guan X, & Yao F (2011). Welfare program participation among rural-to-urban migrant workers in China. International Journal of Social Welfare, 20(1), 10–21. [Google Scholar]
- Xu Y, Wang L, He J, Bi Y, Li M, Wang T, Wang L, Jiang Y, Dai M, Lu J and Xu M (2013). Prevalence and control of diabetes in Chinese adults. Jama, 310(9), 948–959. [DOI] [PubMed] [Google Scholar]
- Zhang D, & Unschuld PU (2008). China’s barefoot doctor: past, present, and future. The Lancet, 372(9653), 1865–1867. [DOI] [PubMed] [Google Scholar]
- Zhang Z, & Treiman DJ (2013). Social origins, hukou conversion, and the wellbeing of urban residents in contemporary China. Social science research, 42(1), 71–89. [DOI] [PubMed] [Google Scholar]
- Zhao Y, Hu Y, Smith JP, Strauss J, & Yang G (2012). Cohort profile: the China health and retirement longitudinal study (CHARLS). International journal of epidemiology, 43(1), 61–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.