

Abstract
Background/Objective:
Studies show the need for improved communication and social skills of adolescents with autism spectrum disorders (ASDs). Therefore, the present study aimed to analyze the effect of using rational-emotive language education (RELE) to pursue this need for adolescents in Nigeria.
Methods:
The design of the study was a group randomized trial, with pretest, post-test, and follow-up. Sixty-eight adolescents with ASDs participated in the study. Autism Communication and Social Skills Scale for Adolescent (ACSSSA) was used for data collection. The method of data analysis in the study was repeated measures ANOVA procedure, with Partial eta squared ( ), adjusted R2, mean, standard deviation, and upper/lower limit.
), adjusted R2, mean, standard deviation, and upper/lower limit.
Results:
The RELE program significantly improved communication and social skills of adolescents with ASDs exposed to the treatment intervention when compared with waitlist control group.
Conclusion:
Exposure to RELE significantly improved communication and social skills of adolescents with ASDs in this study. Therefore, we recommend that language educators, speech pathologists, language therapists, special educators and counsellors, and other professionals involved in the treatment and caring for ASDs patients be trained on the application of the RELE technique so as to enable them to employ the program in their professional practices.
Keywords: adolescents, autism syndromes disorders, rational-emotive language education
1. Introduction
In recent times, adolescents are reportedly suffering from autism spectrum disorders (ASDs). The ASDs include autism, Asperger syndrome, and atypical autism or pervasive developmental disorder, not otherwise specified.[1] These disorders are defined as neurodevelopmental disorders, which are displayed with persistent deficiencies in communication, social interaction, and repetitive patterns of behaviors, interests, or activities.[2,3] Recent studies have found that individuals with ASDs have significant deficits in sensory perception, sleep habits, and autonomic regulation, as well as substantial health loss across their lifespans.[4–8] Studies have shown evidence that ASDs are also associated with high levels of functional limitations, poor health status in children,[9] increased parenting stress and family burden.[10] Findings from other studies have emphasized that symptoms of ADSs among adolescents include deficiency in social interaction, communication, and a repetitive repertoire of behavior.[11]
The challenges faced by adolescents with ASDs can be summed up as poor communication and social skills.[12] It is possible that adolescents with ASDs might have trouble taking turns in conversations. They might talk a lot about a favorite topic but find it problematic to talk about a variety of topics. They might be confused by language and take things literally and might speak in an unusual tone of voice. Nonverbally, adolescents with ASDs might have trouble reading nonverbal cues like body language or tone of voice to deduce how someone else might be feeling. They might use eye contact in an unusual way; express few emotions on his face; or not be able to read other people's facial expressions. In terms of relationships, it is also possible that adolescents with ASDs might prefer to spend time on their own rather than with friends. They might require other adolescents to play by their rules; have trouble understanding the social rules of friendship; have few or no real friends; have trouble relating to children of their own age; prefer to play with younger children or adults; and have difficulty adjusting their behavior in different social situations.[13]
Studies have found that ASDs accounted for 53 disability-adjusted life-years (per 100,000 populations of children. Baxter et al[8] reported that there were an estimated 52 million cases of ASDs globally in 2010. Other studies show increasing diagnostic data of ASDs among children or pupils.[10,14] According to Centre for Disease Control and Prevention,[15] studies in the United State of America have reported the prevalence of ASDs, ranging from 50 to 90 in 10,000 children. Despite the high prevalence of ASDs, little attention has been given to its treatment at the global public.[16]
In African societies, there is evidence of a high prevalence of ASDs. For instance, 33.6% and 11.5% of the population was found in in Egypt and Tunisia, respectively.[17] In Nigeria, a study found 11.4% children with ASDs according to diagnostic criteria for childhood autism.[18,19] However, studies within African countries reported a lack of expressive language as the common symptom of ADSs. Belhadj et al[20] recounted that 51.2% of children demonstrated a lack of expressive language in cases of ASDs in this age group. In another study, Mankoski et al [17] reported 71% lack of expressive language cases of ASDs in their study. Seltzer et al[21] reported that 405 individuals between the ages of 10 and 53 manifested symptoms of ASDs.
The known cases of ADSs appear to be increasing in Nigeria. Recent studies recounted that patients in Africa, Nigeria in particular, often fail to develop expressive language ability, with little or no speech at all.[22] In South-East Nigeria, a case of a boy with an ASD was reported [22,23] as showing that the boy tended to be mute with little or no speech and was being seen for the first time at the age of 15 years in a psychiatric clinic of a university teaching hospital.[22] Still in the South-East Nigeria, a case of a boy with comorbid ASD and oculocutaneous albinism, characterized by a lack of expressive language, with little or no speech, was reported, and the boy was being seen in an orthodox clinical practice for the first time at the age of 13 years.[18] This shows that there is lack of early diagnosis and treatment for ASDs in the Nigerian communities. Meanwhile, rational emotive language education (RELE) would enhance early recognition and intervention, which has been observed to improve prognosis in individuals with ASDs.[18]
Evidence indicated that individuals with ASDs have significant cognitive, communicative, emotional, social, and behavioral impairments that affect them and their families.[24] It could be possible that the adolescents with ASDs experience harmful thoughts and beliefs that bar them from taking part in social interactions and communication. In comparison to adolescents who experience typical development, adolescents with ASDs experience significant problems related to psychological, social, and emotional health.[25] Anderson et al[26] and Colgan et al[27] observed that individuals with ASDs face challenges with social engagement and age-appropriate play. Bauminger and Shulman[28] emphasized that such individuals have difficulty processing their own and the emotions of others.[29] These challenges, in combination with communication deficits and nonconforming behavior, often lead to poor communication and social adjustment.[25]
The consequence of such communication deficits is poor verbal interaction and language development.[30] The authors further stressed that individuals with ASDs require a high level of adapted parental communication, which focuses specifically on the subtle details of interaction in the context of their specific impairments. The potential causes of ASDs are reportedly said to be cognitive deficit, language impairment, and poor perception.[31] Therefore, intervention programs that address cognitive, communicative, emotional, social, and behavioral aspects of language development might have a significant, positive effect on adolescents with ASDs. The increasing prevalence of ASDs in the studies cited earlier in the paper demonstrates that so far successful methods of treatment for ASDs have not been found and there is a need for more research to test new interventions. It was at this premise that the current study focused on investigating the effectiveness of RELE on improving communication and social skills among adolescents with ASDs.
RELE can be very effective from the perspective of many groups of adolescents with ASDs. Many programs are dedicated to improving students’ social and emotional skills.[32–34] Special schools, rehabilitation centres, and hospitals try to support the development of adolescents with ASDs as responsible citizens. Adolescents with ASDs are expected to have learned to cope with their disorders; to develop a modicum of social skills; and to have the ability to manage emotions in an age- and context-appropriate manner. However, due to the harmful thoughts and beliefs they struggle with, many are afraid to socialize freely with other people.[35] Even schools, rehabilitation centers, and hospitals with the highest behavioral standards for their staff in terms of mindfulness, gender competence, intercultural competence, friendliness, awareness, rational language, a willingness to discuss, among others, have not been able to successfully teach communication and social skills to adolescents with ASDs.[36] Studies have shown that the rational, explicit, and direct teaching of content is important for the development of stable knowledge and skills.[12] From this frame of reference, we chose the RELE, which is based on the applied principles of Rational Emotive Behavior Therapy (REBT).
REBT is committed to the establishment and maintenance of mental health. REBT holds the individual at the center of attention.[12] The basic idea underlying REBT is that emotional disturbances emerge from defective thinking about events rather than the events themselves.[36] A distinct feature of REBT has been the notion that the individual is not independent of the social context but is also responsible and has degrees of freedom.[12] Studies show that REBT-based intervention can be used to strengthen the components of communication and social skills within a scientifically oriented frame of reference.[12,37–39] Different REBT-based interventions exist in the literature, but there are limitations. Therefore, as part of our research we developed RELE as a REBT-based intervention to improve communication and social skills among adolescents with ASDs. We developed RELE by transferring the knowledge of REBT to the language education discipline and through deep collaboration with REBT experts. In our research, we tested the following hypothesis: using RELE will significantly improve communication and social skills of adolescents with ASDs.
2. Method
2.1. Ethical consideration
To comply with ethical issues in randomized trial, we observed the human research standards by Human Research and Ethics committee of the faculty of Education, University of Nigeria, Nsukka; the American Psychology Association; and the American Medical Association and Medical Association of Nigeria. Participants’ rights were also observed, and their informed consent was obtained prior to participation in the study.
2.2. Participants
The participants of the present study consisted of 68 adolescents with ASDs. The participants were selected from communities in South-East Nigeria. The study focused on using RELE to improve communication and social skills of adolescents with ASDs in communities where adolescents with ASDs were particularly disadvantaged. We were dealing with adolescents whose parents, for various reasons, did not educate their children on how to deal adequately with themselves or others. These adolescents’ access to the world was often very limited as they had very few real-life experiences.[12]
To qualify for the study, all potential participants had to meet specific criteria. They had to have received a diagnosis of an ASD from a medical, psychological, or educational professional, as reported by their parents. Other criteria included being able to participate in the intervention with 2 family members; being an adolescent with ASDs between the ages of X and Y; and having the ability to communicate in English. On the whole, the participants met DSM-IV-TR criteria for ASDs as recommended by Seltzer, Krauss (21), Lord, Risi (40), and had lower communication and social skills based on ACSSSA measure.
Adolescents with Rett Disorder, Childhood Disintegrative Disorder, tuberous sclerosis, and fragile X syndrome were excluded from the study because each of these disorders had a distinct medical or developmental course. The families of these 68 individuals with ASDs diagnoses were recruited for the study through agencies, schools, diagnostic clinics, and the media. The parents signed informed consent forms before the commencement of the study. Informational packets were distributed to families who were invited to participate in the study. The participants were randomized into treatment (n = 33) group and waitlist control group (n = 35). The mean age of the participants in the treatment group was 15.67 ± 086 years of age, while participants in the waitlist group had a mean age of 16.02 ± 0.34.
The majority (n = 25, 75.8%) of the participants in the treatment group were males, and n = 25, 71.4% of the participants in the waitlist control group were male, which was reflective of the gender distribution in the population (1). Females represented n = 8, 24.2% in the treatment group and n = 10, 28.6% in the waitlist control group. There were n = 21, 63.6% Christian participants in the treatment group and n = 18, 51.4% in the waitlist group and 12 (36.4%), Muslim participants in the treatment group, and 17 (48.6%) in the waitlist group. About parenting, 9(27.3%) of the participants in the treatment group and 8 (22.9%) of the participants in the waitlist control group came from single-parent homes; 9 (27.3%) in the treatment group and 11 (33.4%) in the waitlist group came from homes where both parents were present; 11(33.3%) in the treatment group and 8 (22.9%) in the waitlist group had no parents; and 4 (12.1%) and 8 (22.8%) in the waitlist control group were living under the care of foster parents (refer to Table 1 for their demographic details).
Table 1.
Demographic analysis.

2.3. Procedure
The participants were divided into 2 groups: X and Y. The process of randomization into treatment (n = 33) and waitlist control (n = 35) groups was undertaken by an independent statistician after the completion of a baseline assessment, using a random allocation software.[40] Also, closed envelopes were used to do the randomization. The person allocating participants to the 2 groups was not aware of the identity of the participants and did not have direct contact with the participants. The participants who chose closed envelopes inscribed with the word “Yes” formed the treatment group, while those who chose envelopes inscribed with the word “No” formed the waitlist control group.
The participants responded 3 times of measure: before the treatment (Time 1); after the treatment (Time 2); and after the follow-up (Time 3). The participants in the treatment group were exposed to a 12-week of RELE program with 2 sessions per week, with each 2 hours in length. There was also a follow-up event that was held 2 months after the initial RELE treatment intervention. The participants in the waitlist group did not receive any therapeutic treatment within the period of RELE program or follow-up. After the completion of the study, a social life support program was organized for them. Data collected in the 3 measures were analyzed by a professional data analyst who did not partake in the assessment and was not involved in the RELE implementation; this design was in line with previous study.[41]
3. Intervention
3.1. Rational emotive language education (RELE)
RELE was a 12-week intervention program, which aimed at improving communication and social skills of adolescents with ASDs. The RELE intervention consisted of 24 sessions, which lasted 2 hours each and occurred twice a week for the duration of the study. Each adolescent with ASDs was required to attend the RELE intervention program with 2 family members, preferably their mother and a close sibling. If their mother or sibling could not attend the program, they could bring a close family member or caregiver instead. The responsibility of the family members was to serve as the adolescent's communication and social partners and assistants with whom the adolescents with ASDs interacted during the intervention break sessions and at home. The reason for involving family members in RELE program was because evidence has shown that consequence of communication impairment sin ASDs can result in the parent and child failing to establish a communicative “meshing” and verbal interaction of a kind that is known to facilitate language development.[30] Therefore, we deduced that involving the family members in the RELE program would promote their interactions with the adolescents and thereby facilitate the adolescents’ communication and social skills.
The major focus of the RELE program was to help the participants to improve communication and social skills by disputing harmful thoughts and beliefs they were holding as reasons for their inability to communicate and socialize with others.[42] The RELE identified pivotal areas such as motivation, self-initiation, and self-management, which have been proven to be critical in eliciting broader treatment gains.[42] The RELE focuses on using a number of strategies to help increase participants’ motivation during intervention, such as using a variety of adolescent-chosen activities that are intrinsically motivating to each adolescent, and interspersing maintenance and acquisition tasks to strengthen adolescents’ exposure to well-established response-reinforcer contingency. To overcome the challenges of therapists’ initial relationship with the autistic adolescents and their family, the RELE employed some important strategies to engage the participants. The strategies include: careful explanation of the service context and our role; beginning with what the adolescents sees as the problem; maintenance of a warm, empathic respectful attitude; careful listening, including taking the individual and their views on the problem seriously; and working at a pace that allows the adolescents to feel safe.[43,44]
The RELE was taught in a systematic manner and set clear behavioral standards for the adolescents and their family members. The adolescents were taught to identify and dispute harmful and unhelpful thoughts and beliefs behind their inability to take part in conversations appropriately, make friends, and engage in age-appropriate interests. Using the classic ABCDE framework, RELE begins with relationship building followed by problem solving.[36] In the first dimension, RELE practitioners (who were language therapists, language educators, and REBT experts) establish rapport with the patients by using numerous relationship-building skills such as attending, empathy, respect, understanding, and acceptance.[36] Second, RELE practitioners employed problem identification and problem analysis strategies by identifying and evaluating erroneous and harmful beliefs that are considered to mediate emotional disturbance that might result in poor communication and social skills. In the third dimension, the RELE followed the intervention goals to reduce the intensity, duration, and frequency of disturbed emotions that often lead to poor communication and social interactions or skills. In the fourth dimension, cognitive change is brought about through disputation.
The participants with ASDs initially thought that their problems were caused by people; that interacting with someone would increase their problem; that someone might kill them; that life was not interesting; that there was nothing good about them; that all hope was lost; that they could never recover from their conditions; that their family members and caregivers were not doing enough to help them; that people were laughing at them; that they had no need for friends; etc. Through the RELE program, the participants were able to learn to shift harmful thoughts and beliefs, which they had held for many years. They also learned to replace them with helpful thoughts and beliefs, which were rational, fact-based, and scientifically proven to be accurate. For instance, the participants were encouraged to think and believe that people in their lives loved and cared for them; that interacting with someone would decrease their problems; that life was not interesting; that there was still hope for them in the social sphere; that they could be happy with themselves and others around them; etc. Evidence holds that the communicative signals of adolescents with ASDs are often weak, infrequent, or poorly timed.[45] Thus, in RELE, the practitioners draw family members into a didactic controlling style of discourse, which uses adult-orientated initiations and strategies to take over from the adolescent's “topic” to control and redirect the their focus of attention. Also, the family members were trained to become more sensitive and responsive to the autistic adolescent's communicative initiations so their initiations and language development can increase, which was inspired by a previous study's recommendation.[24]
4. Measure
4.1. Autism communication and social skills scale for adolescent (ACSSSA)
We generated the ACSSSA items in line with autism literature and scales[46] and the Autism Diagnostic Observation Schedule–Generic by Lord et al.[47] The ACSSSA had 22 items that tested the communication and social skills of adolescents with ASDs. The items were selected in line with DSM-IV-TR criteria for ASDs. The 22 items were weighed on a 4-point scale: strongly agreed (4 point); agreed (3 point); disagreed (2 point); and strongly disagreed (1 point). The scale measured communicative and social skills used in the diagnosis of autism. Mean scores of 60 to 88 represented high communication and social skills, while mean scores of 0 to 59 represented low communication and social skills in the current study. Experts in speech and language pathologists validated the ACSSSA. Also, the reliability of the instrument was determined to be 0.88 Alpha.
4.2. Design/data analysis
The design of the study was a group randomized trial, with pretest-post-test and follow-up. The design involved separating the study participants into 2 groups and obtaining a pretest measure prior to administering RELE program, followed by a posttest and follow-up test on the same measure after RELE treatment. The data collected in the study was analyzed with repeated measures ANOVA in which with Partial eta squared ( ), adjusted R2, mean, standard deviation, and upper/lower limit were reported, and the decision regarding the significance value was taken at P≤.05.
), adjusted R2, mean, standard deviation, and upper/lower limit were reported, and the decision regarding the significance value was taken at P≤.05.
5. Results
Table 2 indicated pretreatment, posttreatment, and follow-up results of improved communication and social skills of adolescents with ASDs, using the ACSSSA. At the pretreatment measure, the adolescents in the treatment and waitlist control groups had low mean scores of 16.59 ± 1.23 and 17.28 ± 2.65, respectively (Fig. 1). However, there was no significant difference between the treatment and waitlist control groups in communication and social skills of adolescents with ASDs, F (1,66) = 0.578, P = .450,  = 0.009, R2 = −0.006. At the posttreatment measure, the adolescents in the treatment group had a high mean score of 67.93 ± 2.02, while their counterparts in the waitlist control group had low mean scores of 15.14 ± 3.09. However, after the RELE program, the measure indicated a significant improvement in communication and social skills of adolescents with ASDs in the treatment group when compared with their counterparts in the waitlist control group: F(1,66) = 1164.18, P = .000,
= 0.009, R2 = −0.006. At the posttreatment measure, the adolescents in the treatment group had a high mean score of 67.93 ± 2.02, while their counterparts in the waitlist control group had low mean scores of 15.14 ± 3.09. However, after the RELE program, the measure indicated a significant improvement in communication and social skills of adolescents with ASDs in the treatment group when compared with their counterparts in the waitlist control group: F(1,66) = 1164.18, P = .000,  = 0.945, R2 = 0.946. At the follow-up measure, the participants in the treatment group maintained high mean score, 70.65 ± 2.04 while their counterpart in the waitlist control group maintained low mean score, 16.11 ± 0.34. However, the measure further indicated a significant improvement in communication and social skills of adolescents with ASDs in the treatment group when compared with their counterparts in the waitlist control group: F(1,66) = 1094.22, P = .000,
= 0.945, R2 = 0.946. At the follow-up measure, the participants in the treatment group maintained high mean score, 70.65 ± 2.04 while their counterpart in the waitlist control group maintained low mean score, 16.11 ± 0.34. However, the measure further indicated a significant improvement in communication and social skills of adolescents with ASDs in the treatment group when compared with their counterparts in the waitlist control group: F(1,66) = 1094.22, P = .000,  = 0.945, R2 = 0.946. Based on the results, our hypothesis was correct: using RELE will significantly improve communication and social skills of adolescents with ASDs.
= 0.945, R2 = 0.946. Based on the results, our hypothesis was correct: using RELE will significantly improve communication and social skills of adolescents with ASDs.
Table 2.
Repeated-measures ANOVA showing the effect of RELE to improve communication and social skills of adolescents with autism spectrum disorders.

Figure 1.
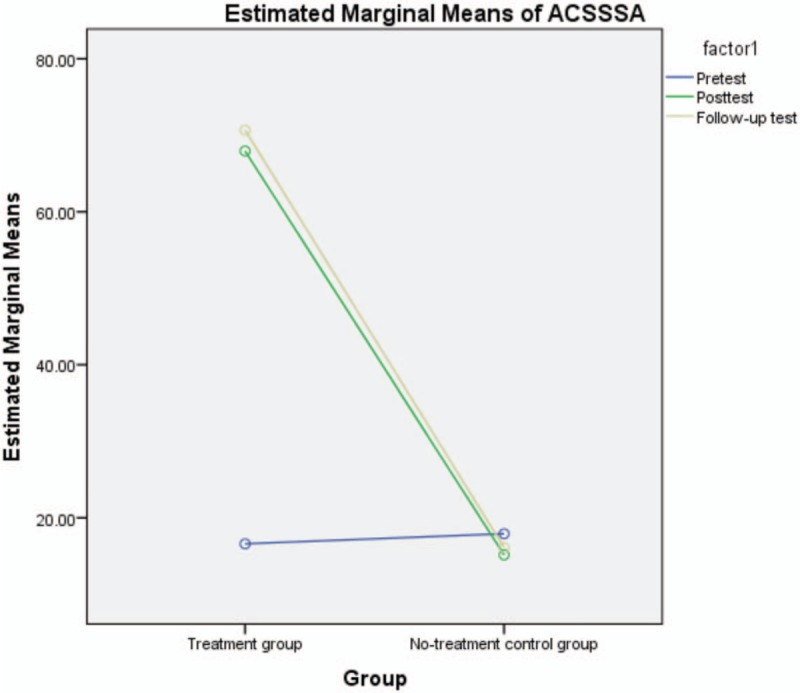
Mean graph.
6. Discussion
The finding at the pretreatment measure indicated that there was no significant difference between the treatment and waitlist control groups in communication and social skills of adolescents with ASDs. The participants showed symptoms of low communication and social skills expressed in symptoms such as being troubled taking turns in conversations; talking a lot about a favorite topic but finding it problematic to talk about a variety of topics; being confused by language and taking things literally; speaking with an unusual tone of voice; having trouble reading nonverbal cues like body language or tone of voice; not being able to guess how someone else might be feeling; etc., in support of previous study.[13] The findings further supported evidence of high rates of ASDs.[10,14,17,18]
The findings of the current study further revealed that using RELE significantly improved communication and social skills of adolescents with ASDs. Participants experienced significant improvements in their communication and social skills after experiencing the RELE program compared with those participants who did not experience the RELE program. This finding supported previous findings that individuals with ASDs had significant cognitive, communicative, emotional, social, and behavioral impairment that affected both the individuals and their families.[24] The RELE program addressed the cognitive, communicative, emotional, social, and behavioral dimension of ASDs that impaired the communication and social abilities of the adolescents with ASDs. The RELE program helped the adolescents to improve communication and social skills by disputing harmful thoughts and beliefs that affected their communication abilities before the program. The finding further supported evidence that adolescents with ASDs who experience significant problems related to social and emotional health can be helped using a REBT-based intervention.[25] Our findings further strengthened the previous assertion that a REBT-based intervention can be used to strengthen the components of communication and social skills within a scientifically oriented frame of reference.[12,37–39] We therefore encourage language education practitioners, speech pathologists, special education teachers, medical professionals, rehabilitation workers, counselors, and psychologists to incorporate the principles of RELE into their practices so as to help adolescents with ASDs improve upon their communication and social abilities.
7. Limitations
The study could not cover a very wide sample of the population of adolescents with ASDs due to the fact that many potential participants did not meet the inclusion criteria for the study. The smallness of the sample may have an impact on the total generalization of the findings. Therefore, it is advisable that future researchers will test the effect of using RELE to improve communication and social skills of adolescents with ASDs so as to confirm its generalizability to a wider audience. Using qualitative method to analyze the data collected in the study may have made a difference in the study findings, but we used only quantitative methods to analyze the data. We therefore recommend that future studies on RELE should endeavor to use both quantitative and qualitative methods of analysis.
We also were not able to include the demographic mediation analysis in the study. Even though that was primarily due to the unequal distribution of the demographic variables in the study, we encourage the future researchers to endeavor to provide demographic mediation analysis in a study with RELE program to further strengthen the effect of the program. Also, we recommend that the future researchers should attempt to use equal demographic distribution.
7.1. Implications for research and practice
Apart from contributing to the body of knowledge of this subject area, we drew some implications from the current findings. The findings have implication on research collaborations across disciplines. Though few researchers have suggested that the conventional knowledge practices of disciplines were the fundamental obstacle to mutual understanding between academic experts,[48] our findings provided evidence that disciplines could collaborate effectively in a study. We therefore recommend more research collaborations between academic experts in language education, medical profession, psychology, special education, and counselling. This is because study with RELE requires knowledge sharing among different academic experts for effectiveness. The findings and the limitation of our study further implied that experts in language education, special education, medicine, rehabilitation counseling, and other related disciplines should conduct large-scale, randomized, and controlled trials aimed at improving communication and social skills of adolescents with ASDs. The effectiveness of such studies will further strengthen and support the claims of the current study.
It may be important for future studies to investigate how RELE can be applied for the treatment of other aspects of ASDs other than communication and social skills. It appears that RELE might be significant in treating other aspects of ASDs, but future researchers should test this notion. Our findings also implied that researchers all over the world should attempt to use RELE for different speech and language-related problems such as aphasia, stammering, and beyond. Also, language therapists, speech pathologist, counselors, and other experts working with ASDs patients should adopt the principles of RELE in treating the patients.
8. Conclusion
The present study showed that using RELE could improve communication and social skills in adolescents with ADSs. RELE effectively increased communication and social skills of adolescents with ASDs. Therefore, we recommend that language educators, speech pathologists, language therapists, special educators, and counsellors and other professionals involved in the treatment and caring for ASDs patients be trained on the application of RELE technique so as to enable them to adopt the RELE program in their professional practices. A future paper will address the critical question of whether RELE is able to improve communication and social skills of children with ASDs. In the meantime, evidence from this study demonstrates that RELE is a reliable means of improving early signs thought to communication and social skills of adolescents with ASDs.
Acknowledgments
The authors’ gratitude goes to the participants and their families for their willingness to participate in the study. The authors also appreciate the experts who provided technical assistance and who supported the implementation of the study.
Author contributions
Conceptualization: Mkpoikanke Sunday Otu, Evelyn Ukoha, Maureen Nnenna Obiezu.
Data curation: Mkpoikanke Sunday Otu, Maureen Nnenna Obiezu, Favour Mkpoikanke Otu.
Formal analysis: Amuche Nnamani, Mkpoikanke Sunday Otu, Maureen Nnenna Obiezu, Chioma Vivian Ike, Favour Mkpoikanke Otu, Chiedu Eseadi.
Funding acquisition: Mkpoikanke Sunday Otu, Maureen Nnenna Obiezu, Chioma Vivian Ike.
Investigation: Amuche Nnamani, Mkpoikanke Sunday Otu, Annah C Uloh-Bethels, Chioma Vivian Ike, Favour Mkpoikanke Otu, Chiedu Eseadi.
Methodology: Amuche Nnamani, Josephine Akabogu, Chioma Vivian Ike, Favour Mkpoikanke Otu, Chiedu Eseadi.
Project administration: Mkpoikanke Sunday Otu, Evelyn Ukoha, Anastasia E. Dike.
Resources: Josephine Akabogu, Evelyn Ukoha, Anastasia E. Dike.
Software: Amuche Nnamani, Jacinta Chinwe Omile, Anastasia E. Dike, Chiedu Eseadi.
Supervision: Josephine Akabogu, Mkpoikanke Sunday Otu, Evelyn Ukoha, Jacinta Chinwe Omile, Anastasia E. Dike.
Validation: Amuche Nnamani, Josephine Akabogu, Mkpoikanke Sunday Otu, Annah C Uloh-Bethels, Evelyn Ukoha, Olayinka M. Iyekekpolor, Jacinta Chinwe Omile.
Visualization: Amuche Nnamani, Josephine Akabogu, Annah C Uloh-Bethels, Olayinka M. Iyekekpolor, Jacinta Chinwe Omile.
Writing – original draft: Annah C Uloh-Bethels.
Writing – review & editing: Josephine Akabogu, Olayinka M. Iyekekpolor.
Mkpoikanke Sunday Otu orcid: 0000-0002-7251-2561.
Footnotes
Abbreviations: ACSSSA = Autism Communication and Social Skills Scale for Adolescent, RELE = rational-emotive language education.
The authors have no conflicts of interest to disclose.
References
- [1].American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. revised 4th ed. Washington, DC: Author 2000. [Google Scholar]
- [2].Wan H, Zhang C, Li H, et al. Association of maternal diabetes with autism spectrum disorders in offspring: a systemic review and meta-analysis. Medicine (Baltimore) 2018;97: e9438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Xiang AH, Wang X, Martinez MP, et al. Association of maternal diabetes with autism in offspring. JAMA 2015;313:1425–34. [DOI] [PubMed] [Google Scholar]
- [4].Precenzano F, Ruberto M, Parisi L, et al. Executive functioning in preschool children affected by autism spectrum disorder: a pilot study. Acta Medica Mediterranea 2017;33:35–9. [Google Scholar]
- [5].Parisi L, Fortunato M, Salerno M, et al. Sensory perception in preschool children affected by autism spectrum disorder: a pilot study. Acta Medica Mediterranea 2017;33:49–53. [Google Scholar]
- [6].Precenzano F, Ruberto M, Parisi L, et al. Sleep habits in children affected by autism spectrum disorders: a preliminary case-control study. Acta Medica Mediterranea 2017;33:405–9. [Google Scholar]
- [7].Parisi L, Salerno M, Maltese A, et al. Autonomic regulation in autism spectrum disorders. Acta Med Mediterranea 2017;33:491–4. [Google Scholar]
- [8].Baxter AJ, Brugha T, Erskine H, et al. The epidemiology and global burden of autism spectrum disorders. Psychol Med 2015;45:601–13. [DOI] [PubMed] [Google Scholar]
- [9].Boulet SL, Boyle CA, Schieve LA. Health care use and health and functional impact of developmental disabilities among US children, 1997-2005. Arch Pediatr Adolesc Med 2009;163:19–26. [DOI] [PubMed] [Google Scholar]
- [10].Kogan MD, Blumberg SJ, Schieve LA, et al. Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics 2009;124:1395–403. [DOI] [PubMed] [Google Scholar]
- [11].Bakare MO, Munir KM. Autism spectrum disorders (ASD) in Africa: a perspective. Afr J Psychiatry (Johannesbg) 2011;14:208–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Steins G, Haep A. Social learning and rational-emotive education: an exploratory investigation of students’ perspective. Psychology 2015;6:1096. [Google Scholar]
- [13].Johnson CP, Myers SM. Identification and evaluation of children with autism spectrum disorders. Pediatrics 2007;120:1183–215. [DOI] [PubMed] [Google Scholar]
- [14].Elsabbagh M, Divan G, Koh YJ, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res 2012;5:160–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Centers for Disease Control and Prevention. Mental health in the United States: parental report of diagnosed autism in children aged 4-17 years—United States, 2003-2004. MMWR Morbidity Mortality Weekly Rep 2006;55:481. [PubMed] [Google Scholar]
- [16].Kogan MD, Strickland BB, Blumberg SJ, et al. A national profile of the health care experiences and family impact of autism spectrum disorder among children in the United States, 2005–2006. Pediatrics 2008;122:e1149–58. [DOI] [PubMed] [Google Scholar]
- [17].Mankoski RE, Collins M, Ndosi NK, et al. Etiologies of autism in a case-series from Tanzania. J Autism Dev Disord 2006;36:1039. [DOI] [PubMed] [Google Scholar]
- [18].Bakare MO, Ebigbo PO, Ubochi VN. Prevalence of autism spectrum disorder among Nigerian children with intellectual disability: a stopgap assessment. J Health Care Poor Underserved 2012;23:513–8. [DOI] [PubMed] [Google Scholar]
- [19].Santé Omdl, Organization WH, Staff W. WHO. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. World Health Organization 1992. [Google Scholar]
- [20].Belhadj A, Mrad R, Halayem M. A clinic and a paraclinic study of Tunisian population of children with autism. About 63 cases. La Tunisie Medicale 2006;84:763–7. [PubMed] [Google Scholar]
- [21].Seltzer MM, Krauss MW, Shattuck PT, et al. The symptoms of autism spectrum disorders in adolescence and adulthood. J Autism Dev Disord 2003;33:565–81. [DOI] [PubMed] [Google Scholar]
- [22].Bakare MO, Munir KM. Excess of non-verbal cases of autism spectrum disorders presenting to orthodox clinical practice in Africa–a trend possibly resulting from late diagnosis and intervention. South African J Psychiatry 2011;17:118–20. [PMC free article] [PubMed] [Google Scholar]
- [23].Dhadphale M, Lukwago MG, Gajjar M. Infantile autism in Kenya. Indian J Pediatr 1982;49:145–8. [PubMed] [Google Scholar]
- [24].Jocelyn LJ, Casiro OG, Beattie D, et al. Treatment of children with autism: a randomized controlled trial to evaluate a caregiver-based intervention program in community day-care centers. J Dev Behav Pediatr 1998;19:326–34. [DOI] [PubMed] [Google Scholar]
- [25].Kuhlthau K, Orlich F, Hall TA, et al. Health-related quality of life in children with autism spectrum disorders: results from the autism treatment network. J Autism Dev Disord 2010;40:721–9. [DOI] [PubMed] [Google Scholar]
- [26].Anderson A, Moore DW, Godfrey R, et al. Social skills assessment of children with autism in free-play situations. Autism 2004;8:369–85. [DOI] [PubMed] [Google Scholar]
- [27].Colgan SE, Lanter E, McComish C, et al. Analysis of social interaction gestures in infants with autism. Child Neuropsychol 2006;12:307–19. [DOI] [PubMed] [Google Scholar]
- [28].Bauminger N, Shulman C. The development and maintenance of friendship in high-functioning children with autism: maternal perceptions. Autism 2003;7:81–97. [DOI] [PubMed] [Google Scholar]
- [29].Bauminger N, Shulman C. The development and maintenance of friendship in high-functioning children with autism. Int J Res Pract 2003;7:1. [DOI] [PubMed] [Google Scholar]
- [30].Aldred C, Green J, Adams C. A new social communication intervention for children with autism: pilot randomised controlled treatment study suggesting effectiveness. J Child Psychol Psychiatry 2004;45:1420–30. [DOI] [PubMed] [Google Scholar]
- [31].Frith U, Morton J, Leslie AM. The cognitive basis of a biological disorder: autism. Trends Neurosci 1991;14:433–8. [DOI] [PubMed] [Google Scholar]
- [32].Forness SR, Kavale KA. Treating social skill deficits in children with learning disabilities: a meta-analysis of the research. Learn Disability Quart 1996;19:2–13. [Google Scholar]
- [33].Solomon D, Battistich V, Watson M, et al. A six-district study of educational change: direct and mediated effects of the Child Development Project. Social Psychol Educ 2000;4:3–51. [Google Scholar]
- [34].Payton J, Weissberg RP, Durlak JA, et al. The Positive Impact of Social and Emotional Learning for Kindergarten to Eighth-Grade Students: Findings from Three Scientific Reviews. Technical Report. Collaborative for Academic. Social, and Emotional Learning (NJ1) 2008. [Google Scholar]
- [35].Fleming JL, Mackrain M, LeBuffe PA. Caring for the caregiver: Promoting the resilience of teachers. Handbook of Resilience in Children 2013;New York: Springer, 387–397. [Google Scholar]
- [36].Gonzalez JE, Nelson JR, Gutkin TB, et al. Rational emotive therapy with children and adolescents: a meta-analysis. J Emotional Behavl Disord 2004;12:222–35. [Google Scholar]
- [37].Ellis A. Can rational emotive behavior therapy (REBT) be effectively used with people who have devout beliefs in God and religion? Professional Psychol Res Pract 2000;31:29. [Google Scholar]
- [38].Dryden W. Flexibility and passionate non-extremism versus absolutism and extremism: teaching the basics of REBT theory and showing its wider applicability. J Rational Emotive Cognitive Behavior Ther 2012;30:38–51. [Google Scholar]
- [39].Vernon A. What works when with children and adolescents. A Handbook of Individual Counseling Techniques. Champaign, IL, USA: Research Press; 2002. [Google Scholar]
- [40].Saghaei M. Random allocation software for parallel group randomized trials. BMC Med Res Methodol 2004;4:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].David R, Enderby P, Bainton D. Treatment of acquired aphasia: speech therapists and volunteers compared. J Neurol Neurosurg Psychiatry 1982;45:957–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Lei J, Ventola P. Pivotal response treatment for autism spectrum disorder: current perspectives. Neuropsychiatr Dis Treat 2017;13:1613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Gerhardt PF, Lainer I. Addressing the needs of adolescents and adults with autism: a crisis on the horizon. J Contemp Psychother 2011;41:37–45. [Google Scholar]
- [44].Myers SM, Johnson CP. Management of children with autism spectrum disorders. Pediatrics 2007;120:1162–82. [DOI] [PubMed] [Google Scholar]
- [45].Reddy V, Hay D, Murray L, et al. Communication in infancy: mutual regulation of affect and attention. Infant Dev Recent Adv 1997. 247273. [Google Scholar]
- [46].Bryson SE, Zwaigenbaum L, McDermott C, et al. The Autism Observation Scale for Infants: scale development and reliability data. J Autism Dev Disord 2008;38:731–8. [DOI] [PubMed] [Google Scholar]
- [47].Lord C, Risi S, Lambrecht L, et al. The autism diagnostic observation schedule—generic: a standard measure of social and communication deficits associated with the spectrum of autism. J Autism Dev Disord 2000;30:205–23. [PubMed] [Google Scholar]
- [48].Lowe P, Phillipson J. Barriers to research collaboration across disciplines: scientific paradigms and institutional practices. Environ Planning A 2009;41:1171–84. [Google Scholar]