

Abstract
The study sought to characterize back pain (BP) (in the period of 12 months) in children and youth aged 10 to 19 from eastern Poland.
The study included 11619 children and youth (6254 girls and 5365 boys) aged 10 to 19 from eastern Poland. An original questionnaire was applied as a research tool. Before the study, the reliability of the questionnaire had been assessed. The Kappa coefficient value for all the analyzed variables was equal to or higher than 0.91.
Over 74.4% of the respondents admitted that within the last 12 months, they had experienced BP which was usually located in the lumbar spine (55.8%). The percentage of individuals reporting BP increased with age of participants. Girls reported BP more often than boys (82.8% vs 64.3%). The main circumstances in which BP occurred included lifting heavy objects, carrying school backpack and maintaining a sedentary position (70.7% vs 67.4% vs 67.8%). Over 67% of the respondents declared they did not know ergonomic principles.
High prevalence of BP was noted. The declared BP was mainly located in the lumbar spine. Girls reported BP more often than boys. The students presented a very low level of knowledge about ergonomics. Therefore, the appropriate education should be included at school.
Keywords: back pain, children and youth, prevention, risk factors, treatment
1. Introduction
Back pain (BP) is one of the most prevalent musculoskeletal disorders and, as a consequence, it has become a significant problem of the contemporary society.[1,2,3] Epidemiological data indicate that BP exists not only among adults but also among children and youth.[3–9] What is more, BP experienced in young age leads to its more common occurrence in adulthood.[10,11] Unsurprisingly, the high prevalence and care-seeking translate into a substantial financial burden for the society. A study in the US estimated that the annual costs of chronic pain in adolescents aged 10 to 17, where musculoskeletal pain comprised the largest proportion, were $19.5 billion.[12] A large survey in Germany estimated minimum direct costs of the treatment of individuals under 25 with back disorders at the level of 100 million per year.[13] Although data documenting the costs associated with children's BP are sparse, they appear to be substantial, which means that investigation into prevention and treatment is worthwhile from an economic perspective.
What is important, BP is not only a musculoskeletal system disease, but it may also lead to many different disturbances determining the quality of life. Lopez-Lopez et al and Calvo-Lobo at al, indicated the relation between BP and depression.[14–15] Other authors emphasized the connection between chronic BP and a compromised quality of life,[16] sleep disturbance,[17] and increased utilization of health care resources.[18]
To date, a few interesting studies have been published concerning BP in Polish children and youth.[19–20] However, they included relatively small study groups, which could limit their conclusions. What is more, most of the papers in this field have focused only on 1 part of the spine (e.g., lumbar or cervical pain).
The aim of the study is to characterize BP (in the period of 12 months) in more than 11,000 children and youth aged 10 to 19 from eastern Poland. A big sample size, wide age range, and the fact that all parts of the spine (cervical, thoracic, and lumbar) were taken into account will make it possible to comprehensively assess the characteristics of BP in the population of Polish children and youth.
2. Methods
2.1. Materials
The study included 11619 children and youth (6254 girls and 5365 boys) from eastern Poland. The sample was selected in 2-phase group sampling. In the first phase, schools from 3 levels of education (primary, lower-secondary, and upper-secondary schools) were randomly selected in particular towns. In the second phase, particular classes were selected (stratified phase sampling).[21] Ultimately, the study included students from the 4th to 6th grade of primary school (children aged 10–13), the 1st to 3rd grade of lower-secondary school (14–16 years) and the 1st to 3rd grade of upper-secondary school (17–19 years). Students who gave their consent to participate in the study were qualified to it. A final analysis included 11424 questionnaires, which constitutes 98.3% of the total number of the participants.
2.2. Methods
An original questionnaire was applied as a research tool. All the students completed the questionnaire during school classes with the one of the study authors present. The questionnaire included single-choice (9) and multiple-choice (7) questions.
The main part of the questionnaire concerned the following aspects:
-
a.
experiencing or not BP within the last year (12 months). Individuals who gave a negative response to this question did not complete the remaining part of the questionnaire,
-
b.
the frequency and location of BP,
-
c.
types of situations in which BP occurred or increased,
-
d.
ways of dealing with pain and the knowledge of ergonomics.
Before the study, the reliability of the questionnaire was assessed by conducting the survey twice in a group of 60 individuals (20 students from 3 levels of education) with a month-long interval.
The survey was anonymous and voluntary.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Senate Research Ethics Committee of Jozef Pilsudski University of Physical Education in Warsaw, Poland (research number—Statutory Research DS. 183).
2.3. Statistical analysis
Calculations were made with the use of Microsoft Excel 2007 and SPSS 9.0 (SPSS, IL) software. In the statistical analysis, descriptive statistics were used. To analyze the collected research results, a non-parametric test based on Chi-square function was employed. The reliability of the questionnaire was evaluated with Kappa coefficient. The value of alpha <.05 was established as the significance level.
3. Results
3.1. Pilot reliability study
The Kappa coefficient value for all the analyzed variables was equal to or higher than 0.91. No significant differences between the results obtained in the 2 tests were revealed (P <.05).
3.2. Prevalence of BP
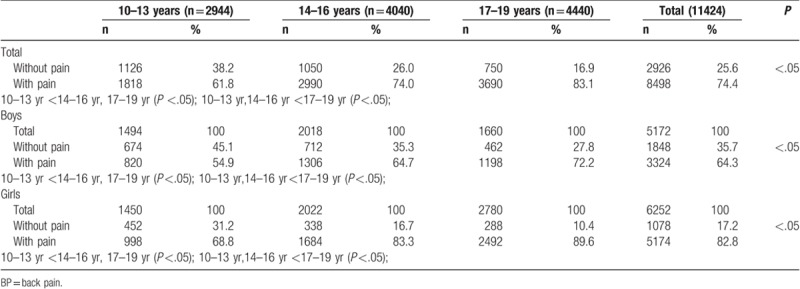
From among 11424 of the participants, 8498 (74.4%) respondents declared that they had experienced BP within the last 12 months. Girls reported BP more often than boys (82.8% vs 64.3%). Such a situation occurred in all the age groups. The percentage of individuals reporting BP increased with age of participants, both among girls and boys (P <.05) (Table 1).
Table 1.
The prevalence of BP with regard to sex and age of the respondents (n = 11424).
Afterward, the frequency of BP with regard to the number of hours a day spent in a sedentary position was analyzed. The percentage of individuals who spent more than 5 hours a day in a sedentary position increased with age (72.4% vs 86.9% vs 92.6%) (P <.05). Simultaneously, the percentage of the respondents who spent less than 5 hours in this position decreased (27.6% vs 13.1% vs 7.4%) (P <.05). Such a situation occurred both in the group of individuals who declared BP and among those who did not (Table 2).
Table 2.
The prevalence of BP with regard to the number of hours spent in a sedentary position and students’ age (n = 11424).
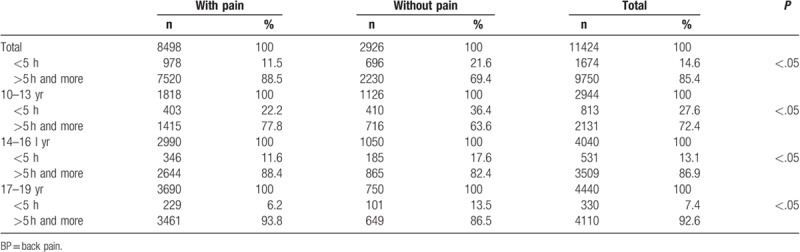
Students with BP spent more than 5 hours per day in a sedentary position more often than students without BP (88.5% vs 69.4) (P <.05) (Table 2).
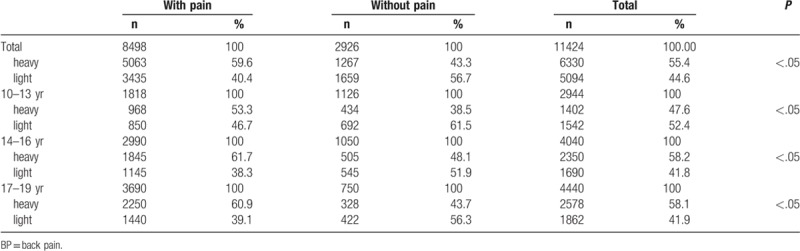
The frequency of occurrence of BP depending on school backpack weight was the next aspect included in the analysis. The results indicate that students reporting BP declared that their backpack was heavy more often than their counterparts who did not report BP (59.6% vs 43.3%). This situation occurred in all the age groups (P <.05) (Table 3).
Table 3.
The prevalence of BP in students with regard to the declared backpack weight and students’ age (n = 11424).
3.3. Frequency, location, and circumstances of BP
While analyzing the frequency of occurrence of BP, it was noted that the respondents who experienced pain rarely, that is, 1 to 2 times a year constituted the largest group. This state was declared by 55.1% of the respondents. The analysis of the frequency of BP with regard to sex revealed that boys declared BP occurring 1 to 2 times a year more often than girls (61.2% vs 51.2%); however, the percentage of boys declaring frequent or constant pain was lower than the percentage of girls (7.9% vs 10.8%) (Table 4).
Table 4.
The frequency, location and circumstances in which BP occurred in the group of students with regard to their age (n = 8498).
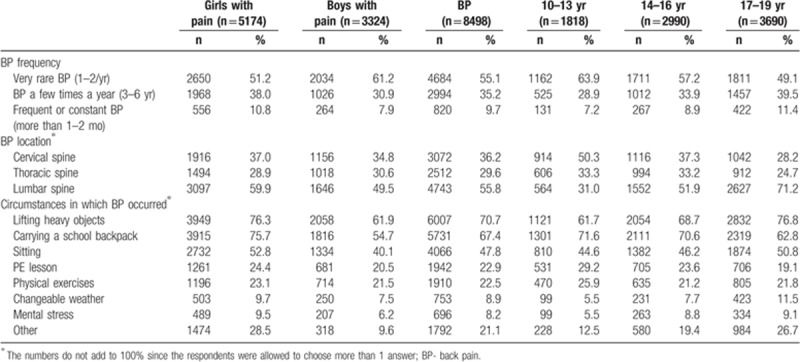
When analyzing the frequency of BP with regard to age, it was observed that the percentage of the respondents reporting very rare cases of BP (1–2 times a year) decreased with age (63.9% vs 57.2% vs 49.1%). In turn, the percentage of individuals declaring frequent or constant pain (more than 1–2 months) increased (7.2% vs 8.9% vs 11.4%) (Table 4).
BP was mainly located in the lumbar spine, which was declared by 55.8% of the respondents. The analysis of pain location depending on the respondents’ age showed that in the group of 10 to 13-year-olds, pain was located mainly in the cervical spine (50.3%), while in the groups of 14 to 16-year-olds and 17 to 19-year-olds in the lumbar spine (51.9%, 71.2%) (Table 4).
Students aged 10 to 13 and 14 to 16 mainly experienced BP when carrying a school backpack, while in the group of 17 to 19-year-olds, BP occurred most often when lifting heavy objects. A considerable group of students declared that they felt BP during physical activities (21.8%) and during physical education (PE) classes (19.1%) (Table 4).
3.4. Ways of dealing with BP and the students’ knowledge of ergonomics
Only 20.0% students sought medical help due to BP. The percentage of the respondents who went to a physician because of their BP decreased with age (28.8% vs 19.5% vs 16.2%).
The analysis revealed that rest was the most common method of dealing with pain (71.3%), while physiotherapy procedures other than electrotherapy were the second most common way (44.4%). It occurred in all the age groups. A considerable group of students aged 10 to 13 (14.9%), 14 to 16 (12.7%) and 17 to 19 (17.5%) used painkillers to relieve BP (Table 5).
Table 5.
Ways of coping with BP and the knowledge of ergonomics among the students with regard to their age (n = 8498).
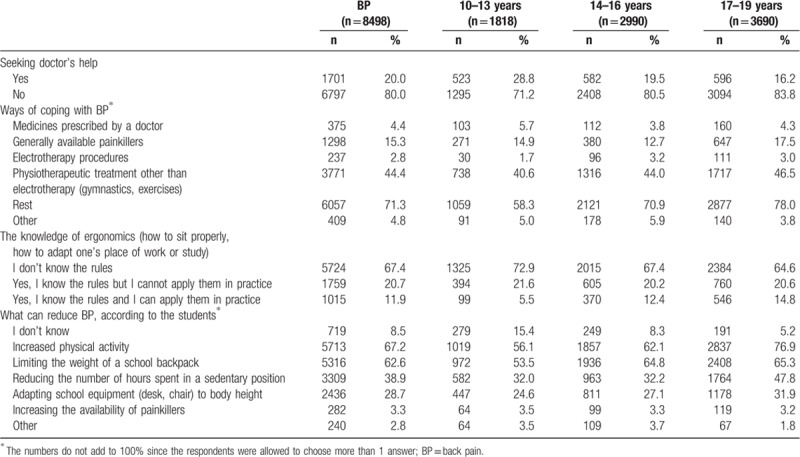
Next, the respondents experiencing BP were asked about their knowledge of ergonomics (i.e., how to sit properly or how to prepare a place of work and study). Students who declared the lack of such knowledge constituted the largest group (67.4%). This situation was noted in all the age groups. The 11.9% of the study participants declaring the knowledge of the rules of ergonomics and the ability to apply them constituted 11.9%, however, the number of students declaring this knowledge increased with age (Table 5).
The largest group was constituted by the respondents who claimed that increasing the level of physical activity (67.2%) and decreasing the weight of a school backpack may reduce BP. According to a considerable group of students (38.9%), limiting the weight of a school backpack could reduce BP as well (Table 5).
4. Discussion
The study sought to characterize BP (in the period of 12 months) in children and youth aged 10 to 19 from eastern Poland.
The study revealed that BP affected a considerable group of children and youth aged 10 to 19 (74.4%). It could be noted that girls reported BP more often than boys (82.8% vs 64.3%) and the percentage of individuals reporting BP increased with age. Students with BP more often spent more than 5 hours in a sedentary position than students without pain (96.4% vs 63.6%) (P <.05). It was also revealed that students who reported BP more often declared that their backpack was heavy than students without pain (59.6% vs 43.3%).
Similar research on BP in children and youth was carried out in other countries. The study by Wedderkopp et al conducted in Denmark revealed that BP (occurring within the last month before the investigation) occurs in 39% of the children and youth aged 8 to 10 and 14 to 16.[22] In the American study on children aged 12 to 18, Sheir-Neiss et al revealed that BP occurred in 74.4% youths.[7] Ayanniyi et al observed that BP was reported by nearly 60% of the children from Nigeria.[23] Differences in the percentage values obtained in the cited studies may result from the fact that they analyzed different periods in which BP occurred. Some studies analyzed BP occurring within 1 or 2 months preceding the investigation, while other researchers focused on a longer period of 1 year (12 months). The results presented in our study regarded 1 year preceding the investigation, which may have led to the fact that the percentage of the respondents reporting BP was bigger.
The study revealed that BP was mainly located in the lumbar spine, which was reported by over 55.8% of the respondents. The next most common locations were cervical (36.1%) and thoracic (29.6%) spine. Similar findings were presented by Wagenhauser, who concluded that BP was mainly located in the lumbar (53.5%) and cervical spine (23.4%).[24] In turn, the research carried out by Diepenmaat et al indicated that BP was most often located in the cervical spine and then in the lumbar spine.[25] In the study by Wedderkopp et al, it was concluded that in children (8–10 years old) BP was noted mainly in the thoracic spine, while in adolescents (14–16 years old), the prevalence of BP in the thoracic spine was similar to that in the lumbar spine.[9] The obtained results are also contrary to the findings of Vikat et al, who revealed that BP was located in the cervical spine more often than in the lumbar spine.[2] It is difficult to conclude unanimously what causes such big differences regarding the location of BP. However, according to Wedderkopp et al, in the research on children and youth, BP should be analyzed separately for the cervical, thoracic and lumbar spine for clinical and scientific reasons.[9]
Our research revealed that the BP occurs mainly during lifting heavy objects (70.7%), carrying a school backpack (67.4%) and maintaining a sedentary position (47.8%). The fact that a considerable group of students felt BP during physical exercises (22.5%) or even during PE classes (22.8%) is an alarming situation.
The data concerning the influence of physical activity on BP which are available in the literature are not unanimous. The study by Harreby et al revealed that high-intensity physical activity correlated with the occurrence of BP.[26] In turn, the lack of correlation between pain and physical activity was confirmed by Diepenmatt and Morgensen et al.[25,27] Contrary results were revealed by Wedderkopp et al, who concluded that high-intensity physical activity in childhood may be treated as a way of preventing BP in older age.[22] The studies by other authors revealed that taking up physical activity by persons experiencing BP protects them against recurring or chronic pain.[28] Very interesting observations were made by Heneweer et al in their study on a group of 3664 participants. They concluded that the correlation between BP and physical activity may be U-shaped. Both a sedentary lifestyle and high-intensity physical activity increased the risk of BP.[29] It shows that both passive lifestyle and excessive activity may increase the risk of BP. The authors concluded that it was the quality, not the quantity of physical activity that was significant. The boundary between moderate and excessive physical activity is also determined by physical fitness. The authors also pointed to the fact that it was significant whether physical activity was taken up as an obligation or voluntarily.[29]
The ways of relieving or eliminating BP observed in the study are alarming. Only 20% of the respondents sought physician's help. In future studies, it would be worth analyzing reasons for BP in a young population, which can improve the quality of the prevention programs. Considerable groups of students used generally available painkillers to relieve BP. The knowledge of ergonomics and an ability to adapt a place of work and study was also very low (11.9%) and indicates very important role of education in this area.
4.1. Study limitations
The presented results are a subjective assessment of the reported BP; however, it should be noted that these are recognized methods of assessing BP.[2,22,26,29] Moreover, the questionnaire was validated, so these limitations did not affect the value of the obtained results significantly.
4.2. Study strengths
In the available literature, there are studies which analyze the prevalence of BP in children and youth; however, they are mainly analyses of low BP (LBP) only. We did not limit our study to LBP, as all the segments of the spine (cervical, thoracic, lumbar) were taken into account. A large population sample (11619 study participants) and a broad age range (10–19 years) constitute study strength as it makes it possible to verify the spinal pain occurrence in particular age groups. To our knowledge, this is the first study concerning BP on such a large group of children and youth from Poland.
The reliability of the questionnaire applied in this study was assessed. The Kappa coefficient value for all the analyzed variables was equal to or higher than 0.91, which proves high validity of the questionnaire and the reliability of information gathered with it (a large percentage of responses was obtained (98.3%). This was a basis for an appropriate analysis of the collected material.
5. Conclusions
-
1.
BP occurred in a large group of students (74.4%) and its prevalence increased with age. The pain was usually rare (1–2 times a year).
-
2.
The declared BP was mainly located in the lumbar spine. The results of the research showed that a small group of students (20.0%) sought medical help because of BP. Rest was the most common method of dealing with pain (71.3%), while physiotherapy procedures were the second most common way of relieving the pain (44.4%).
-
3.
Increasing the level of physical activity (67.2%) and decreasing the weight of a school backpack were indicated as factors which may reduce BP.
-
4.
The students present very low level of knowledge about ergonomics. Therefore, the appropriate education should be included at school.
Author contributions
Conceptualization: Agnieszka Kędra, Dariusz Czaprowski.
Data Curation: Agnieszka Kędra.
Formal Analysis: Agnieszka Kędra, Dariusz Czaprowski.
Funding acquisition: Dariusz Czaprowski, Agnieszka Kędra.
Investigation: Agnieszka Kędra, Aleksandra Kolwicz-Gańko, Dominik Sitarski, Przemysław Kędra, Dariusz Czaprowski.
Methodology: Agnieszka Kędra, Aleksandra Kolwicz-Gańko, Dominik Sitarski, Przemysław Kędra, Dariusz Czaprowski.
Project administration: Agnieszka Kędra.
Resources: Agnieszka Kędra, Dariusz Czaprowski.
Software: Dariusz Czaprowski.
Supervision: Agnieszka Kędra, Aleksandra Kolwicz-Gańko, Przemysław Kędra, Dariusz Czaprowski.
Validation: Agnieszka Kędra, Aleksandra Kolwicz-Gańko, Dominik Sitarski, Przemysław Kędra, Dariusz Czaprowski.
Visualization: Agnieszka Kędra, Aleksandra Kolwicz-Gańko, Dominik Sitarski, Przemysław Kędra, Dariusz Czaprowski.
Writing – original draft: Agnieszka Kędra, Aleksandra Kolwicz-Gańko, Dominik Sitarski, Przemysław Kędra, Dariusz Czaprowski.
Writing – review & editing: Agnieszka Kędra, Aleksandra Kolwicz-Gańko, Dominik Sitarski, Przemysław Kędra, Dariusz Czaprowski.
Footnotes
Abbreviations: BP = back pain, LBP = low back pain, PE = physical education.
The work was not funded from a grant but it was supported by the Ministry of Science and Higher Education (project no. DS-183 of the Faculty of Physical Education and Sport in Biała Podlaska, Józef Piłsudski University of Physical Education in Warsaw).
The authors declare no conflict of interest.
References
- [1].El-Metwally A, Salminen JJ, Auvinen A, et al. Risk factors for development of non-specific musculoskeletal pain in preteens and early adolescents: a prospective 1-year follow-up study. BMC Musculoskelet Disord 2007;8:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Vikat A, Rimpelä M, Salminen JJ, et al. Neck or shoulder pain and low back pain in Finnish adolescents. Scand J Public Health 2000;28:164–7. [PubMed] [Google Scholar]
- [3].Calvo-Lobo C, Diez-Vega I, Martínez-Pascual B, et al. Tensiomyography, sonoelastography, and mechanosensitivity differences between active, latent, and control low back myofascial trigger points: a cross-sectional study. Medicine (Baltimore) 2017;96:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Boćkowski L, Sobaniec W, Kułak W, et al. Low back pain in school-age children: risk factors, clinical features and diagnostic managment. Adv Med Sci 2007;52:221–3. [PubMed] [Google Scholar]
- [5].Masiero S, Carraro E, Celia A, et al. Prevalence of nonspecific low back pain in schoolchildren aged between 13 and 15 years. Acta Paediatr 2008;97:212–6. [DOI] [PubMed] [Google Scholar]
- [6].Pellisé F, Balagué F, Rajmil L, et al. Prevalence of low back pain and its effect on health-related quality of life in adolescents. Arch PediatrAdolesc Med 2009;163:65–71. [DOI] [PubMed] [Google Scholar]
- [7].Sheir-Neiss G, Kruse R, Rahman T, et al. The association of backpack use and back pain in adolescents. Spine 2003;28:922–30. [DOI] [PubMed] [Google Scholar]
- [8].Tsirikos AI, Kalligeros K. Back pain in children and adolescents: etiology, clinical approach and treatment. CurrPediatr Rev 2006;3:265–86. [Google Scholar]
- [9].Wedderkopp N, Leboeuf-Yde C, Andersen LB, et al. Back pain reporting pattern in a Danish population-based sample of children and adolescents. Spine 2001;26:1879–83. [DOI] [PubMed] [Google Scholar]
- [10].Adams MA, Mannion AF, Dolan P. Personal risk factors for first-time low back pain. Spine 1999;24:2497–505. [DOI] [PubMed] [Google Scholar]
- [11].Salminen JJ, Erkintalo MO, Pentti J, et al. Recurrent low back pain and early disc degeneration in the young. Spine 1999;24:1316–21. [DOI] [PubMed] [Google Scholar]
- [12].Groenewald CB, Essner BS, Wright D, et al. The economic costs of chronic pain among a cohort of treatment-seeking adolescents in the United States. J Pain 2014;15:925–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Ochsmann EB, Pinzón CLE, Letzel S, et al. Prevalence of diagnosis and direct treatment costs of back disorders in 644,773 children and youths in Germany. BMC Musculoskelet Disord 2010;11:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Lopez-Lopez D, Vilar-Fernandez JM, Calvo-Lobo C, et al. Evaluation of depression in subacute low back pain: a case control study. Pain Physician 2017;20:499–505. [PubMed] [Google Scholar]
- [15].Calvo-Lobo C, Vilar Fernández JM, Becerro-de-Bengoa-Vallejo R, et al. Relationship of depression in participants with nonspecific acute or subacute low back pain and no-pain by age distribution. J Pain Res 2017;11:129–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Lawrence RC, Helmick CG, Arnett FC, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum 1998;41:778–99. [DOI] [PubMed] [Google Scholar]
- [17].Wilson KG, Watson ST, Currie SR. Daily diary and ambulatory activity monitoring of sleep in patients with insomnia associated with chronic musculoskeletal pain. Pain 1998;75:75–84. [DOI] [PubMed] [Google Scholar]
- [18].Becker N, Bondegaard Thomsen A, Olsen AK, et al. Pain epidemiology and health related quality of life in chronic non-malignant pain patients referred to a Danish multidisciplinary pain center. Pain 1997;73:393–400. [DOI] [PubMed] [Google Scholar]
- [19].Drozda K, Lewandowski J, Górski P. Back pain in lower and upper secondary school pupils living in urban areas of Poland. The case of Poznań. OrtopTraumatol Rehabil 2011;13:489–503. [DOI] [PubMed] [Google Scholar]
- [20].Romicka AM, Rostropowicz-Denisiewicz K, Moskalewicz B, et al. Bóle spondylogenne u dzieci. Med Wieku Rozw 2003;7:165–72. [PubMed] [Google Scholar]
- [21].Brown KW, Cozby PC, Kee DW, et al. Research Methods in Human Development. 2d ed.1999;Mountain View, CA: Mayfield Publishing Company, p. 26. [Google Scholar]
- [22].Wedderkopp N, Kjaer P, Hestbaek L, et al. High-level physical activity in childhood seems to protect against low back pain in early adolescence. Spine J 2009;9:134–41. [DOI] [PubMed] [Google Scholar]
- [23].Ayanniyi O, Mbada ChE, Muolokwu ChA. Prevalence and profile of back pain in nigerian adolescents. Med PrincPract 2011;20:368–73. [DOI] [PubMed] [Google Scholar]
- [24].Wagenhauser J. Classification acute back pain: a clinical approach to differential diagnosis. In: current concepts and treatment. 1989;Sandoz: Pennine Press, p. 14. [Google Scholar]
- [25].Diepenmaat AC, van der Wal MF, de Vet HC, et al. Neck/shoulder, low back, and arm pain in relation to computer use, physical activity, stress, and depression among Dutch adolescents. Pediatrics 2006;117:412–6. [DOI] [PubMed] [Google Scholar]
- [26].Harreby M, Nygaard B, Jessen T, et al. Risk factors for LBP in a cohort of 1389 Danish school children: an epidemiologic study. Eur Spine J 1999;8:444–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Morgensen AM, Gausel AM, Wedderkopp N, et al. Is active participation in specific sport activities linked with back pain. Scand J Med Sci Sports 2007;17:680–6. [DOI] [PubMed] [Google Scholar]
- [28].Torstensen TA, Ljunggren AE, Meen HD, et al. Efficiency and costs of medical exercise therapy, conventional physiotherapy, and self-exercise in patients with chronic low back pain. A pragmatic, randomized, single-blinded, controlled trial with 1-year follow-up. Spine 1998;23:2616–24. [DOI] [PubMed] [Google Scholar]
- [29].Heneweer H, Vanhees L, Picavet HS. Physical activity and low back pain: a U-shaped relation. Pain 2009;143:21–5. [DOI] [PubMed] [Google Scholar]