

Abstract
Rationale:
The purpose of this study is to introduce the application of screw view model of navigation (SVMN) for adolescent idiopathic scoliosis (AIS). It is a challenge to insert pedicle screw into the vertebral body of scoliosis, and the misplaced screw may lead to neurovascular injury. In order to minimize surgical complications, we used a novel method of SVMN technology to facilitate pedicle screw insertion.
Patient concerns:
Her mother brought her to our outpatient department upon noticing the girl's different heights of shoulders and unbalance of the trunk.
Diagnoses:
She was diagnosed with AIS and syringomyelia.
Interventions:
We used an SVMN technology to assist pedicle screw insertion and correction surgery in this 20-year-old patient.
Outcomes:
This study indicates that the SVMN could obtain a satisfactory surgical effect for AIS. The Cobb angle of segmental scoliosis (T7-L2) was 55° before surgery, and 3.5° after surgery, and the rate of correction was 93.6%. The segmental kyphosis (T7-L1) was 56.8° preoperatively and 32° postoperatively with the rate of correction of 43.6%. The distance between the center sacral vertical line (CSVL) and the C7 plumb line (CPL) was reduced from 56.2 mm to 0.2 mm, and the sagittal imbalance of 35.8 mm was improved to 3.5 mm. In addition, the misplacement of pedicle screws, the volume of blood loss, the operation time, and surgical complications were also recorded. The follow-up duration was 33 months.
Lessons:
The utilization of SVMN in AIS might reduce the incidence of screw misplacement and avoid neurovascular damage, as well as a satisfactory correction. The application of SVMN for AIS is an efficacious and safe method.
Keywords: corrective surgery, navigation, scoliosis, screw view model
1. Introduction
Adolescent Idiopathic Scoliosis (AIS) is a three dimensional (3D) anatomical deformity of the vertebral column, mainly including variations in alignment of the sagittal plane, deviations in coronal plane and vertebral rotation in axial plane.[1–4] At present, screw-rod system fixation in posterior approach has become the primary measure for AIS.[5,6] On the one hand, a satisfactory orthopedic effect should be achieved, on the other hand, complications should be avoided during operation.
More accurate pedicle screw implantation could decrease the probability of neurovascular structures injury. Over the last 2 decades, pedicle screw placement with free-hand for scoliosis has obtained acceptable outcomes. However, with the increasing angle of scoliosis and degree of vertebra rotation, the difficulty of screw implantation increased gradually,[7,8] and the incidence of screw misplacement is 1.7% to 15.7% by free-hand.[9,10] Numerous methods have been applied to facilitate scoliosis correction and promote pedicle screw insertion, involving computer-assisted surgery,[11] pedicle screw insertion guiding devices,[12] 3D rapid prototyping technique5.6%,[7] and robot-assisted surgery,[13] but the effect was not satisfactory. The application of these measures still has 5.6% to 11.4% screw malposition rate.[7,12–14] In order to minimize surgical complications, we used a novel method of SVMN technology, which could facilitate pedicle screw insertion. To our knowledge, the use of this SVMN technology for AIS has rarely been reported.
2. Ethics
The patient signed written informed consent and her information was hidden. This study has been approved by the Ethics Committee of the Second Hospital of Jilin University, Changchun Province, China. (2019) Research and Inspection No. (008).
3. Case report
3.1. Patient characteristics
This is a healthy female patient at 20 years old (Table 1). Her mother brought her to our outpatient department upon noticing the girl's unbalance of the trunk. The girl had no obvious uncomfortableness.
Table 1.
Patient characteristics.

Physical examination displayed different heights of shoulders and “razor back” deformity. There was no obvious hypoaesthesia. The muscle strengths of bilateral iliocsoas muscle, quadriceps femoris muscle, anterior tibial muscle, peroneal longus, and soleus muscle are all V grade. Both Achilles tendon reflex and knee reflex were normal. Bilateral Chaddock signs, Babiskin signs, and Patellar clonus were negative. The Bragard sign and Lasegue test were negative.
Imaging examination demonstrated that the segmental scoliosis (T7-L2) was 55° (Fig. 1A) and the segmental kyphosis (T7-L1) was 56.8° (Fig. 1B). The distance between the CPL and the CSVL was improved from 56.2 mm to 0.2 mm, and the sagittal imbalance of 35.8 mm was reduced to 3.5 mm. The upper end vertebra, apex vertebra, and the lower end vertebra were T7, T11, and L2 respectively (Table 1). The total spine magnetic resonance imaging displayed the formation of syringomyelia in C5–7 and T3–6 segments (Fig. 2). Ultrasonic cardiography was examined to estimate whether heart disease was existent. The result of pulmonary function tests showed that the percentage of residual gas and total lung increased slightly, and the diffusion function of lung was normal. Results of electromyography showed that there was no neurogenic lesion in the muscles of the lower extremities and motor and sensory nerve conduction velocity and the double tibial nerve's H reflex were normal. The Risser grade of this patient was V grade. The primary diagnosis was AIS and syringomyelia.
Figure 1.

Anterior-posterior and lateral standing full-length spinal X-rays were obtained preoperatively (A–B).
Figure 2.
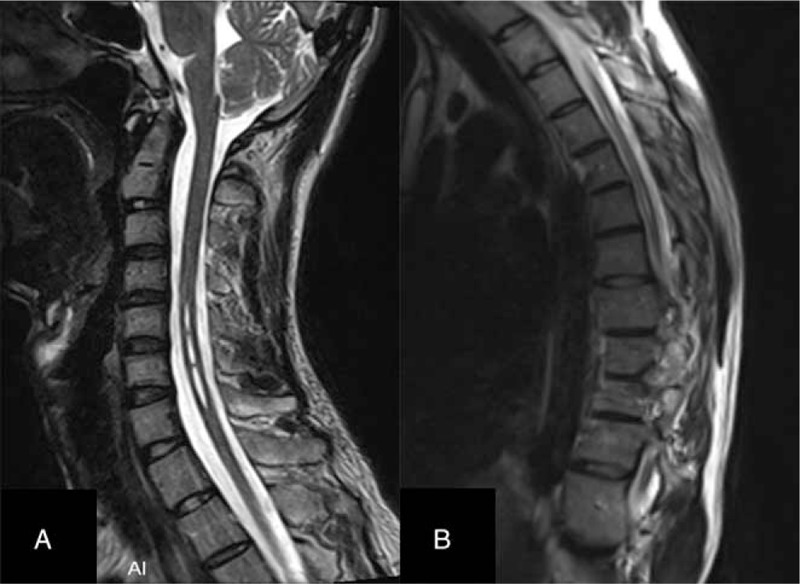
Magnetic resonance imaging displayed formation of syringomyelia in C5–7 and T3–6 segments.
3.2. Surgical technique
Preoperative CT scans of the whole spine was performed (Fig. 3), and the image data was burned on a CD that could be recognized by the computer-navigation workstation so as to facilitate preoperative design, including the length, diameter, and trajectory of pedicle screws.
Figure 3.
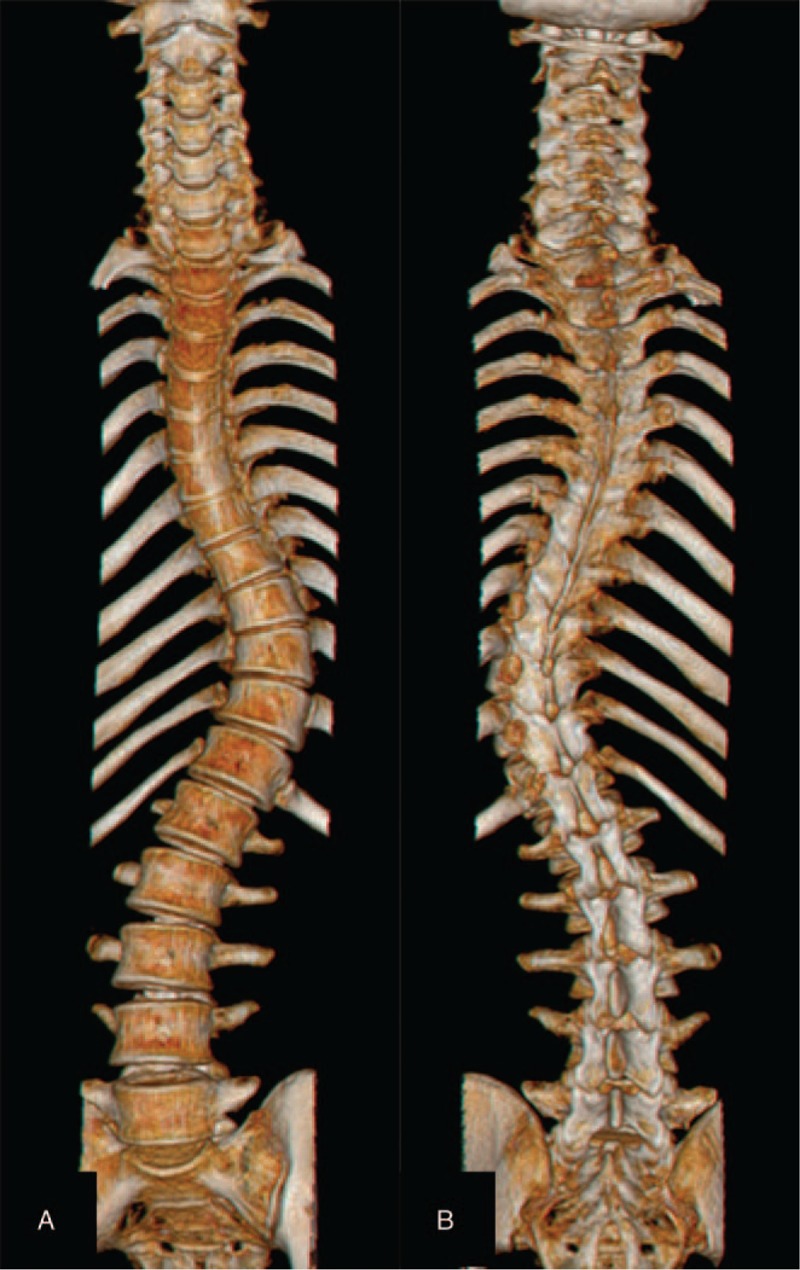
Preoperative 3D CT scan revealed spinal deformity (A–B).
The patient was placed in prone position after general anesthesia took effect. The posterior structures of T5-L3 were exposed. A patient tracker for locating the patient's spatial location was installed on the spinous process of T5 vertebra. The SpineMap 3D 2.0 (Stryker Navigation, Kalamazoo, MI, USA) software was selected in Navigation System workstation. The C-arm tracker, the patient tracker and the surgical instrument tracker (Stryker Leibinger GmbH & Co., Freiburg, Germany) were activated in turn. We finished image acquisition after 190° scanning at the segmental lesion and made automatic fusion of scanned image intraoperative and CT image preoperative. We chose SVMN in the workstation and moved the position of the surgical instrument until the direction of surgical instrument was completely consistent with the planned trajectory preoperatively. The surgical instrument was not inserted until the lower right corner of the screen turned green (Fig. 4). Then scoliosis was corrected. Anteroposterior position and lateral X-rays were performed intraoperatively to examine the position of inserted screw. A multimodal intraoperative monitoring system was applied throughout the operation, mainly monitoring motor evoked potentials and somatosensory evoked potentials.[15] Brace was used for 3 months after operation to ensure the stability of the spine.
Figure 4.
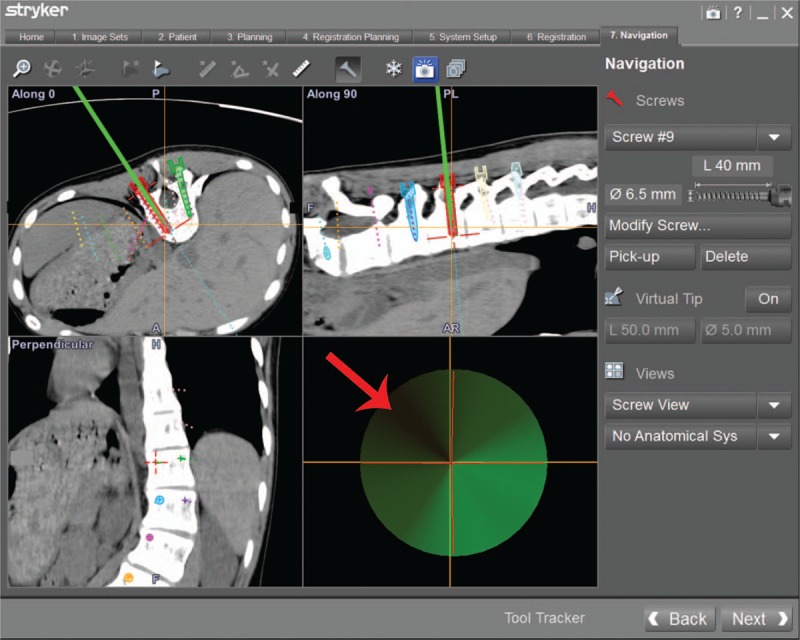
The screw view model of navigation displays the trajectory of surgical instrument during screw implantation, and the guide wire is not inserted until the area indicated by the yellow arrow turns green.
The surgical complications, the operation time, and the bleeding volume were collected from the medical records. The frontal and lateral of total spine X-rays were taken (Fig. 5A–B) and CT image was scanned postoperatively. We estimated the position of pedicle screw reported by Ughwanogho et al.[16] The clinical pictures were also collected postoperatively (Fig. 6A–B).
Figure 5.

Clinical pictures of the patient postoperatively (A–-B).
Figure 6.

Postoperative total spine X-rays revealed good correction of segmental scoliosis (A) and segmental kyphosis (B).
The blood loss volume was 768 ml, and the operation time was 186 minutes. The distance between the CPL and the CSVL was improved from 56.2 mm to 0.2 mm, and the sagittal imbalance of 35.8 mm was reduced to 3.5 mm. The main curve was 3.5° postoperative with 93.6% correction rate. The segmental kyphosis (T5-T12) was 32° after surgery with 43.6% correction rate (Table 2). No screw misplacement and neurological impairment were found postoperatively. No curve progression, pseudarthrosis formation, or loosening of pedicle screw was discovered during 33 months of follow-up duration.
Table 2.
Scoliosis correction pre- and postoperatively.

4. Discussion
At present, the major approach for AIS is the posterior screw-rod system fixation.[1,3,5,8] Screw misplacement is a primary factor that leads to disastrous neurovascular compromise.[2–4] Literature[1,17] reported that navigation system allows the surgeon to implant pedicle screw more accurately than free hand technique, whereas the pedicle violation was still observed 11.4% with navigation. Research reported that computer navigation system could improve the accuracy of screw implantation in scoliosis patients, while the malposition rate was as high as 16.9%.[6] To minimize surgical risk, we used a novel SVMN technology to promote the success of the operation.
In this study, there was no pedicle screws misplacement, and the neurologic function was intact postoperatively. The major Cobb angle correction was 93.6%, which is slightly better than Quan GM (69.9% correction).[18] We attribute the excellent correction rate and the precise pedicle screw insertion to SVMN technique. To our way of thinking, this SVMN technology could help surgeons prevent neurovascular injury and pedicle invasion as well as increase the stability of the spine.
Postoperative screw loosening is a very familiar surgical complication of spinal surgery.[19,20] Morr et al.[19] and Ohtori et al.[20] stated that the incidence of pedicle screw loosening was in the range of 7% to 19.6%. The main reasons for screw loosening include insufficient length of the selected screw, poor angle of screw placement, repeated screw placement, and excessive postoperative spinal load. Pedicle screw loosening was also associated with many other surgical complications, such as pseudarthrosis, screw breakage, and even loose correction.[21] In this study, no screw loosening was detected during 33 months of follow up. In our opinion, we attribute these positive outcomes to screw insertion with SVMN technology so that all screws were successfully implanted at the best trajectory at one time and we applied a brace to maintain stability of spine postoperatively.
The operation time was 186 minutes with SVMN technology. This outcome was similar to a literature reported by Yang et al.[12] This positive outcome was most likely to be attributed to the full understanding of the deformity spinal anatomical structures via 3D models in navigation workstation, so we could quickly identify the entry point and trajectory intraoperatively. Besides, the duration of surgery was associated with the total intraoperative bleeding volume, and there usually is a large volume of blood loss in deformity correction surgery.[22] Effective measures to reduce intraoperative bleeding are crucial for doctors, as blood transfusion can result in infection, hemodynamic changes, fever, acute lung injury, and even death.[23–25] In this study, the blood loss was 768 ml with SVMN technology. We attribute this good result to much shorter operation time with the SVMN technology.
Our study obtained satisfactory outcomes, however, it also has many limitations. Firstly, the case report was a small sample size and there were no randomized controlled trials. Secondly, the patient may have suffered more X-ray radiation because the whole operation was carried out 3 times of image acquisition. Therefore, a multicenter and randomized controlled trial should be conducted and radiographic exposure duration should be reduced to assess the effectiveness of SVMN technology for the patients with AIS.
5. Conclusion
This study demonstrates that the SVMN could achieve a better therapeutic effect for AIS. The application of SVMN in AIS might decrease operation time, screw loosening rate, and the risk of screw malposition. Besides, we obtained a successful correction. Therefore, SVMN for AIS is a safe and efficacious method.
Acknowledgments
We would like to thank Professor Lu for her meticulous correction of the manuscript. We are also grateful to all the staff in the operating room, it would be difficult to achieve perfect results without their active cooperation.
Author contributions
Conceptualization: Shuang Zheng, Rongpeng Dong.
Data curation: Rongpeng Dong.
Methodology: Shuang Zheng, Yang Qu, Jianwu Zhao.
Project administration: Yang Qu.
Validation: Mingyang Kang.
Visualization: Xiwen Zhang, Mingyang Kang.
Writing – original draft: Tong Yu, Yang Qu, Xiwen Zhang, Jianwu Zhao.
Writing – review & editing: Lili Yang, Rongpeng Dong, Jianwu Zhao.
Footnotes
Abbreviations: 3D = three dimensional, AIS = adolescent idiopathic scoliosis, CPL = C7 plumb line, CSVL = center sacral vertical line, CT = computer tomography, EMG = electromyography, L = lumbar, T = thoracic.
TY and LY contributed equally to this work.
The authors have no conflicts of interest to disclose.
References
- [1].Dunn J, Henrikson NB, Morrison CC, et al. Screening for adolescent idiopathic scoliosis: evidence report and systematic review for the US preventive services task force. JAMA 2018;319:173–87. [DOI] [PubMed] [Google Scholar]
- [2].Zhao J, Fan J, Shen H, et al. Characteristics of Cobb angle distribution in the main thoracolumbar/lumbar curve in adolescent idiopathic scoliosis: a retrospective controlled clinical study. Medicine 2018;97:e11216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Faldini C, Ruffilli A, Perna F, et al. Surgical correction of double major adolescent idiopathic scoliosis. Eur Spine J 2018;27:571–3. [DOI] [PubMed] [Google Scholar]
- [4].Pasha S, Flynn JM, Sankar WN. Outcomes of selective thoracic fusion for Lenke 1 adolescent idiopathic scoliosis: predictors of success from the sagittal plane. Eur Spine J 2018;27:2223–32. [DOI] [PubMed] [Google Scholar]
- [5].Li N, Xu C, Shen MK, et al. Clinical outcomes of posterior pedicle screw instrumentation without osteotomy in the management of adolescent idiopathic scoliosis. Medicine 2018;97:e12122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].O’Donnell C, Michael N, Pan X, et al. Anterior spinal fusion and posterior spinal fusion both effectively treat Lenke type 5 curves in adolescent idiopathic scoliosis: a multicenter study. Spine Deform 2018;6:231–40. [DOI] [PubMed] [Google Scholar]
- [7].Yang M, Li C, Li Y, et al. Application of 3D rapid prototyping technology in posterior corrective surgery for Lenke 1 adolescent idiopathic scoliosis patients. Medicine 2015;94:e582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Tian W, Lang Z, Liu YJ, et al. [Study of pedicle screw placement assisted by intraoperative three-dimensional navigation in lumbar vertebrae with axial rotation]. Zhonghua wai ke za zhi [Chin J Surg] 2010;48:838–41. [PubMed] [Google Scholar]
- [9].Hicks JM, Singla A, Shen FH, et al. Complications of pedicle screw fixation in scoliosis surgery: a systematic review. Spine 2010;35:E465–470. [DOI] [PubMed] [Google Scholar]
- [10].Di Silvestre M, Parisini P, Lolli F, et al. Complications of thoracic pedicle screws in scoliosis treatment. Spine 2007;32:1655–61. [DOI] [PubMed] [Google Scholar]
- [11].Uehara M, Takahashi J, Kuraishi S, et al. Computer-assisted skip pedicle screw fixation for adolescent idiopathic scoliosis. J Orthop Sci 2017;22:218–23. [DOI] [PubMed] [Google Scholar]
- [12].Yang L, Li H, Tang J, et al. A novel guide device improves the accuracy of pedicle screw placement. Int J Clin Exp Med 2015;8:8634–40. [PMC free article] [PubMed] [Google Scholar]
- [13].Macke JJ, Woo R, Varich L. Accuracy of robot-assisted pedicle screw placement for adolescent idiopathic scoliosis in the pediatric population. J Robot Surg 2016;10:145–50. [DOI] [PubMed] [Google Scholar]
- [14].Sakai Y, Matsuyama Y, Nakamura H, et al. Segmental pedicle screwing for idiopathic scoliosis using computer-assisted surgery. J Spinal Disord Tech 2008;21:181–6. [DOI] [PubMed] [Google Scholar]
- [15].Yu T, Wang Y, Zhang XW, et al. Multimodal intraoperative monitoring during reduction of spine burst fracture and dislocation prevents neurologic injury. Medicine 2018;97:e0066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Ughwanogho E, Patel NM, Baldwin KD, et al. Computed tomography-guided navigation of thoracic pedicle screws for adolescent idiopathic scoliosis results in more accurate placement and less screw removal. Spine 2012;37:E473–478. [DOI] [PubMed] [Google Scholar]
- [17].Li QJ, Yu T, Liu LH, et al. Combined 3D rapid prototyping and computer navigation facilitate surgical treatment of congenital scoliosis: a case report and description of technique. Medicine 2018;97:e11701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Quan GM, Gibson MJ. Correction of main thoracic adolescent idiopathic scoliosis using pedicle screw instrumentation: does higher implant density improve correction? Spine 2010;35:562–7. [DOI] [PubMed] [Google Scholar]
- [19].Morr S, Carrer A, Alvarez-Garcia de Quesada LI, et al. Skipped versus consecutive pedicle screw constructs for correction of Lenke 1 curves. Eur Spine J 2015;24:1473–80. [DOI] [PubMed] [Google Scholar]
- [20].Ohtori S, Inoue G, Orita S, et al. Comparison of teriparatide and bisphosphonate treatment to reduce pedicle screw loosening after lumbar spinal fusion surgery in postmenopausal women with osteoporosis from a bone quality perspective. Spine 2013;38:E487–492. [DOI] [PubMed] [Google Scholar]
- [21].Kotani Y, Abumi K, Ito M, et al. Improved accuracy of computer-assisted cervical pedicle screw insertion. J Neurosurg 2003;99(3 Suppl):257–63. [DOI] [PubMed] [Google Scholar]
- [22].Ialenti MN, Lonner BS, Verma K, et al. Predicting operative blood loss during spinal fusion for adolescent idiopathic scoliosis. J Pediatr Orthop 2013;33:372–6. [DOI] [PubMed] [Google Scholar]
- [23].Hart A, Khalil JA, Carli A, et al. Blood transfusion in primary total hip and knee arthroplasty. Incidence, risk factors, and thirty-day complication rates. J Bone Joint Surg Am 2014;96:1945–51. [DOI] [PubMed] [Google Scholar]
- [24].Pereira A. Red blood cell alloimmunisation: still a major complication of blood transfusion. Br J Haematol 2018;181:575–6. [DOI] [PubMed] [Google Scholar]
- [25].Reed W, Lee TH, Norris PJ, et al. Transfusion-associated microchimerism: a new complication of blood transfusions in severely injured patients. Semin Hematol 2007;44:24–31. [DOI] [PubMed] [Google Scholar]