

Abstract
Tibial tubercle avulsion fracture caused by knee extensor is very rare; furthermore, non-traumatic fractures during running or bilateral fractures have been reported. The purpose of this study was to evaluate any differences according to the mechanisms of injury in adolescents with tibial tubercle avulsion fracture.
Thirty patients with tibial tubercle avulsion fractures were reviewed and the average age was 13 years 1 month. Seven patients (low-stress group) had a spontaneous fracture during running without definite trauma. Twenty-three patients (high-stress group) experienced pain during jumping and landing, or definite trauma. The mechanisms of injury, age, height, weight, body mass index (BMI), BMI percentile, fracture type, as well as any complication, such as limitation of motion and deformity related to the physeal arrest, were compared between groups.
There was no definite difference in age, fracture type, and surgical outcomes between groups. There was no patient with significant early physeal arrest in both groups. The weight (P = .02), BMI (P = .03) and BMI percentile (P = .01) in low-stress group were higher than those in high-stress group. In low-stress group, 6 patients’ BMIs were in the 97th percentile, and 1 patient's BMI was in the 5th percentile.
Extreme BMI may be a risk factor for tibial tubercle avulsion fractures in adolescents during running without definite trauma. However, there was no difference in the final outcome according to injury mechanisms.
Keywords: adolescent, avulsion fracture, body mass index, tibial tubercle
1. Introduction
Tibial tubercle avulsion fracture is very rare and its incidence has been reported to account for only 3% of all proximal tibia fractures and less than 1% of all growth plate injuries.[1–3] This type of fracture occurs when the quadriceps are forcefully contracted against resistance, such as during jumping, or when rapid knee flexion occurs with contracted quadriceps, such as during landing.[2–6] Therefore, sports are known to be risk factors for this fracture, and the avulsion fracture of tibial tubercle occurs more frequently in males, due to their more prevalent participation in sports activities and the fact that physeal closure occurs later in males than in females.[4,6,7]
Interestingly, spontaneous fractures during running without trauma have been reported.[8–11] The stress in quadriceps has been presented to be 289 to 307 kN/m2 during jumping, 292 kN/m2 during landing, and 241 kN/m2 during running.[12] Fracture during running is developed by low-stress compared to jumping and landing, and it may be related to other risk factors, such as weakness of physis relative to the tension applied during intense muscle loading. Gilbert et al reported that obese patients were more likely to sustain fractures involving the physis, and other studies have also reported that obesity is associated with fracture in children.[13–17]
We experienced several cases of tibial tubercle avulsion fractures during running without definite trauma. The purpose of this study was
-
(1)
to find any potential risk factors, including obesity, that are related to the spontaneous fracture during running without definite trauma, and
-
(2)
to evaluate any difference in the final outcome according to the mechanisms of injury.
2. Materials and methods
This retrospective review was approved by the institutional review board of the hospital (4–2017–0523). Between 2007 and 2016, we reviewed children and adolescents with tibial tubercle avulsion fracture at children's hospital and urban general hospitals. The inclusion criteria were as follows:
-
(1)
tibial tubercle avulsion fracture with traumatic/non-traumatic injury,
-
(2)
age below 18 years, and
-
(3)
more than 2 years of follow-up.
The exclusion criteria were as follows:
-
(1)
genetic/metabolic/endocrinologic/neuromuscular disease related to bone strength or growth,
-
(2)
≥2 cm of leg length discrepancy,
-
(3)
diagnosis of malalignment syndrome,
-
(4)
previous operation for lower extremity,
-
(5)
previous fracture history,
-
(6)
multiple fractures, and
-
(7)
multiple organ injuries.
Thirty patients with tibial tubercle avulsion fractures were included. Two patients were female and the average age of patients was 13 years 10 months (range, 10–16 years). The average follow-up period was 26 months (range, 24–40 months).
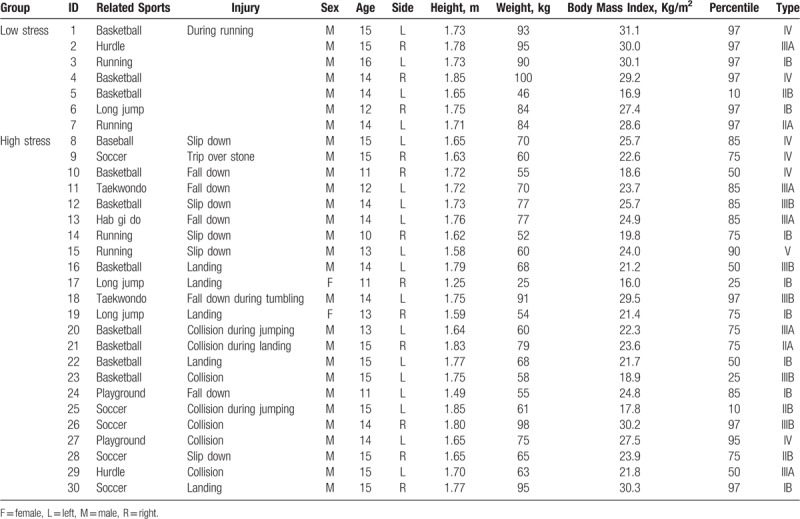
To evaluate the mechanisms of injury, medical record was reviewed, and each patient was contacted to ascertain the situation that led to injury. If the patient reported a sudden pain or weakness while just running without definite trauma, such as a collision or slip down, the patient was assigned to low-stress group. If the patient described a pain or weakness during jumping or landing, a slip or fall while engaging in sports, or a collision with other players, the patient was assigned to high-stress group. A total of 7 patients were assigned to low-stress group, and 23 patients were assigned to high-stress group. The median age of low-stress group was 14 years (range, 12–16 years). The median age of high-stress group was 14 years (range, 10–15 years) and 2 patients were girls (Table 1).
Table 1.
Patients’ details.
Two pediatric orthopedic surgeons reviewed the radiography. Treatment outcome was evaluated by complications such as leg-length discrepancy, varus or valgus, genu recurvatum or procurvatum, and limitation of motion. Body mass index (BMI) percentiles, based on the standard distribution of adolescents in our country, were evaluated.
Statistical analyses were performed using SPSS statistics software package (version 23; IBM corp., Armonk, New York). Differences between groups were examined using Mann–Whitney U tests and Fisher exact test. Values were presented as median (range, min-max value). The level of significance was set at P <.05.
3. Results
According to the Ogden classification, 8 fractures were type IB, 2 fractures were type IIA, 3 fractures were type IIB, 5 fractures were type IIIA, 5 fractures were type IIIB, 6 fractures were Ryu & Debenham type IV, and 1 fracture was type V.[18,19] To evaluate injury to the knee joint, magnetic resonance images were taken in the 6 cases of type IIIA and IIIB, but pathologic lesions were not evident. The injuries involved the right knee in 12 cases and the left knees in the remaining 18 cases. There was no bilateral case.
One patient with an Ogden type IB fracture was treated with tension band wiring (Fig. 1), whereas open reduction and screw fixation were performed for other patients (Fig. 2). The patient who underwent tension band wiring was immobilized for only 1 week. Full weight-bearing began at 8 weeks after injury in each of the cases. An average of 10 weeks was needed to regain a normal range of motion, and all of the patients had a full range of motion of the knee. At the final follow-up, all patients in both groups had healed without any sequelae, such as infection, nonunion, or malunion. There was no significant early physeal arrest or deformity in both groups when radiography was compared to the normal side at the final follow-up.
Figure 1.
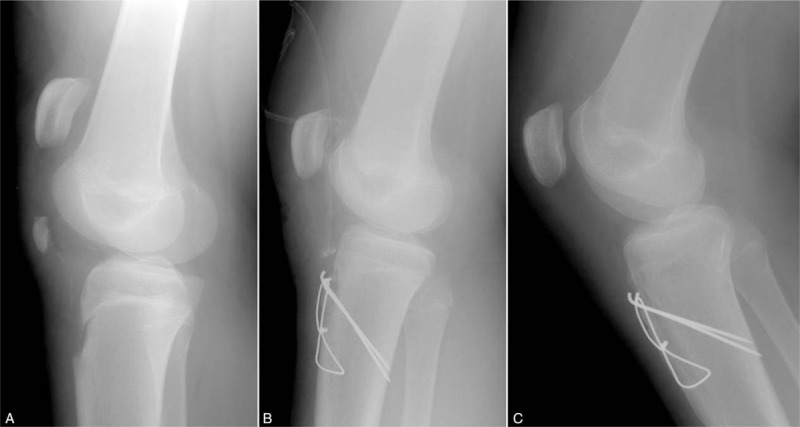
(a) A 16-year-old boy (No. 3) reported sudden onset anterior knee pain while running. An initial lateral radiograph of the knee showing a displaced tibial tubercle fragment and patella alta. (b) Postoperative lateral radiograph of the knee showing fixation of the fragment with Kirschner wire and tension band wire fixation.
Figure 2.

(a) A 12-year-old boy (No. 11) fell down during Taekwondo. Ogden type IIIA tibial tubercle avulsion fracture was noted. In magnetic resonance image, (b) there was no intraarticular pathology. (c) Open reduction and internal fixation with cannulated screw was performed.
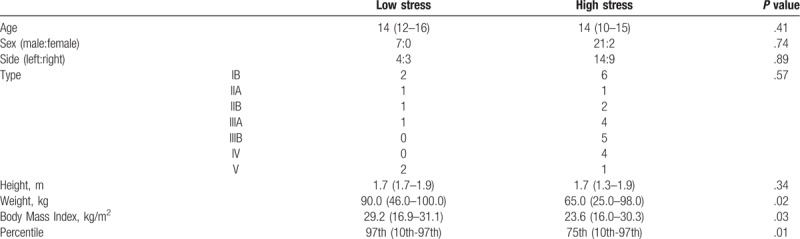
There was no difference between groups in age (P = .41), sex (P = .74), side (P = .89), height (P = .34), and fracture type (P = .67). The weight, BMI, and BMI percentile were higher in low-stress group (P = .02, .03, .01, respectively) (Table 2). Patients in low-stress group had an extreme BMI above the 97th percentile, and 1 patient's BMI was in the 5th percentile.
Table 2.
Comparison of variables between groups.
4. Discussion
The formation of tibial tubercle has been divided into 4 stages by Ehrenborg.[6,20,21] Cartilaginous stage occurs first, before the appearance of tibia tubercle's secondary ossification center. Apophyseal stage begins upon the appearance of the secondary ossification center signal; epiphyseal stage begins with the formation of anterior tongue of bone that the secondary ossification center of proximal tibia joins to the tubercle. The final stage results in bony fusion. Physeal closure starts from the center of proximal tibial physis, and proceeds to the distal end of the physis, and avulsion fractures occur in the area that is too weak to resist the tension produced by muscle loading.[6]
Avulsion fracture of tibial tubercle has been known to be related to the functioning of the lower limb's extensor mechanism during sports.[4,6,7] Maffulli and Grewal reported that a maximal contraction of the quadriceps in athletic adolescents is able to overcome the strength of upper tibial epiphysis and suggested that above-normal strength may play a role in avulsion injuries involving major muscles.[22] In this series, all of the fractures occurred during sports. However, the stress of quadriceps is different according to the type of sports, and stress during running is lower than those during jumping or landing.[12]
We hypothesized there may be additional risk factors that would weaken the physis or those that were related to the increased traction force of the knee extensor in patients who had experienced a fracture during running without definite trauma. In this study, the weight, BMI, and BMI percentile in patients with low-stress group were elevated. Obesity is also known to be a risk factor for fracture in children and may cause abnormal loading to the physis.[13–15,17] However, 1 patient (No. 5)'s BMI was 16.9 kg/m2, and his BMI was in the 5th percentile. Sabhaney et al noted that increased odds of fractures among underweight children compared with normal-weight children and bone mineral density have been found to be proportional to BMI in children.[15,16] We cannot conclude that the elevated weight or BMI was a risk factor related to tibial tubercle avulsion fracture during running without definite trauma. In our opinion, inappropriate knee extensor mechanisms compared to the extreme BMI, for example, weak physis due to abnormal loading in obese children, low bone strength related to bone mineral density in skinny children, or strong extensor power due to heavy weight compared to physeal strength, may be related to tibial tubercle avulsion fracture without definite trauma.
Chow et al suggested the existence of a left-sided predominance for these fracture types, since all of the patients in their series were right-handed but most of them had sustained injury to their left knee.[4] Non-dominant leg may thrust jumping/landing during sports and avulsion fracture may be more common. In the present case series, 18 of the 30 patients also sustained injury to the left knee; however, only 8 patients were injured during jumping/landing, and this series was relatively small in size to ascertain predominance in either the left or the right knee. Osgood-Schlatter disease has also been suggested as a risk factor.[2,4,5,19] However, a direct relationship between Osgood–Schlatter disease and tibial tubercle avulsion fractures has not been reported and there was no patient with Osgood–Schlatter disease in our series.[4,6]
In our series, all of the patients recovered full range of motion and there was no significant complication in both groups. Although premature closure of anterior physis had been suggested to occur as a complication of surgery, we could not find any radiologic evidence of premature closure in this study. To our knowledge, there have not been any reports regarding the premature closure of the physis after operative treatment, except for 1 patient with myelomeningocele.[19] Another report suggested that genu recurvatum, resulting from the premature closure of anterior physis, is not seen as tibial tubercle avulsion fractures are most common in adolescents approaching physiologic physeal closure.[6] In addition, compartment syndrome related to anterior tibial recurrent artery injury was not observed in our series.[23,24]
This study had several limitations as it included a small number of cases due to the rarity of tibial tubercle avulsion fracture. Larger cohort studies are required to determine extreme BMI as a risk factor for tibial tubercle avulsion fracture during running without definite trauma. However, this study is the first to suggest extreme BMI as a potential risk factor for this type of fracture. We did not perform histopathological examinations in low-stress group in the suspicion of overloading the proximal tibial physis since the subjects of the present study were growing adolescents. We used the standard BMI of age-matched normal controls in our country and there may be some differences according to subject's ethnicity.
5. Conclusion
There was no significant difference between fracture during running without definite trauma and fracture during jumping and landing or with definite trauma in terms of age, fracture type, or treatment outcome. However, patients who had experienced a fracture during running without definite trauma had extremely increased or decreased BMI. The mismatch between the strength of physis/bone and power of quadriceps may be a risk factor for tibial tubercle avulsion fractures during running without definite trauma.
Author contributions
Conceptualization: Yong-Woon Shin, Kun-Bo Park.
Data curation: Yong-Woon Shin, Dae-Wook Kim, Kun-Bo Park.
Formal analysis: Yong-Woon Shin.
Investigation: Yong-Woon Shin, Kun-Bo Park.
Methodology: Yong-Woon Shin, Kun-Bo Park.
Supervision: Yong-Woon Shin.
Writing – original draft: Kun-Bo Park.
Writing – review & editing: Yong-Woon Shin, Dae-Wook Kim.
Kun-Bo Park orcid: 0000-0002-8839-4870.
Footnotes
Abbreviation: BMI = body mass index.
The authors have no conflicts of interest to disclose.
References
- [1].Slongo TF, Audigé L. Fracture and dislocation classification compendium for children. J Orthop Trauma 2007;21:S135–60. [DOI] [PubMed] [Google Scholar]
- [2].Bolesta MJ, Fitch RD. Tibial tubercle avulsions. J Pediatr Orthop 1986;6:186–92. [DOI] [PubMed] [Google Scholar]
- [3].Shelton W, Canale T. Fractures of the tibia through the proximal tibial epiphyseal cartilage. J Bone Joint Surg Am 1979;61:167–73. [PubMed] [Google Scholar]
- [4].Chow SP, Lam JJ, Leong JC. Fracture of the tibial tubercle in the adolescent. J Bone Joint Surg Br 1990;72:231–4. [DOI] [PubMed] [Google Scholar]
- [5].Christie MJ, Dvonch VM. Tibial tuberosity avulsion fracture in adolescents. J Pediatr Orthop 1981;1:391–4. [DOI] [PubMed] [Google Scholar]
- [6].McKoy BE, Stanitski CL. Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397–403. [DOI] [PubMed] [Google Scholar]
- [7].Jakoi A, Freidl M, Old A, et al. Tibial tubercle avulsion fractures in adolescent basketball players. Orthopedics 2012;35:692–6. [DOI] [PubMed] [Google Scholar]
- [8].Özokyay L, Michler K, Müsgens J. Beidseitige atraumatische tibiakopfepiphysiolyse. Unfallchirurg 2002;105:735–9. [DOI] [PubMed] [Google Scholar]
- [9].Nicolini AP, Carvalho RT, Ferretti M, et al. Simultaneous bilateral tibial tubercle avulsion fracture in a male teenager. J Pediatr Orthop B 2018;27:40–6. [DOI] [PubMed] [Google Scholar]
- [10].Khoriati AA, Guo S, Thakrar R, et al. Bilateral atraumatic tibial tubercle avulsion fractures: case report and review of the literature. Injury 2015;46:767–9. [DOI] [PubMed] [Google Scholar]
- [11].McKoy BE, Stanitski CL, Hartsock LA. Bilateral tibial tubercle avulsion fractures with unilateral recurrence. Orthopedics 2006;29:731–3. [DOI] [PubMed] [Google Scholar]
- [12].Thorpe SK, Li Y, Crompton RH, et al. Stresses in human leg muscles in running and jumping determined by force plate analysis and from published magnetic resonance images. J Exp Biol 1998;201:63–70. [DOI] [PubMed] [Google Scholar]
- [13].Dimitri P, Bishop N, Walsh JS, et al. Obesity is a risk factor for fracture in children but is protective against fracture in adults: a paradox. Bone 2012;50:457–66. [DOI] [PubMed] [Google Scholar]
- [14].Kessler J, Koebnick C, Smith N, et al. Childhood obesity is associated with increased risk of most lower extremity fractures. Clin Orthop Relat Res 2013;471:1199–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Leonard MB, Shults J, Wilson BA, et al. Obesity during childhood and adolescence augments bone mass and bone dimensions. Am J Clin Nutr 2004;80:514–23. [DOI] [PubMed] [Google Scholar]
- [16].Sabhaney V, Boutis K, Yang G, et al. Bone fractures in children: Is there an association with obesity. J Pediatr 2014;165:313–8. [DOI] [PubMed] [Google Scholar]
- [17].Gilbert SR, Maclennan PA, Backstrom I, et al. Altered lower extremity fracture characteristics in obese pediatric trauma patients. J Orthop Trauma 2015;29:e12–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Ryu RK, Debenham JO. An unusual avulsion fracture of the proximal tibial epiphysis. Case report and proposed addition to the Watson-Jones classification. Clin Orthop Relat Res 1985;194:181–4. [PubMed] [Google Scholar]
- [19].Ogden Ja, Tross RB, Murphy MJ. Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205–15. [PubMed] [Google Scholar]
- [20].Ehrenborg G, Engfeldt B. The insertion of the ligamentum patellae on the tibial tuberosity. Some views in connection with the Osgood-Schlatter lesion. Acta Chir Scand 1961;121:491–9. [PubMed] [Google Scholar]
- [21].Ehrenborg G, Lagergren C. Roentgenologic changes in the Osgood-Schlatter lesion. Acta Chir Scand 1961;121:315–27. [PubMed] [Google Scholar]
- [22].Maffulli N, Grewal R. Avulsion of the tibial tuberosity: muscles too strong for a growth plate. Clin J Sport Med 1997;7:123–9. [PubMed] [Google Scholar]
- [23].Wiss DA, Schilz JL, Zionts L. Type III fractures of the tibial tubercle in adolescents. J Orthop Trauma 1991;5:475–9. [DOI] [PubMed] [Google Scholar]
- [24].Pape JM, Goulet JA, Hensinger RN. Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop Relat Res 1993;295:201–4. [PubMed] [Google Scholar]