

Abstract
Rheumatoid arthritis (RA) is a chronic debilitating inflammatory disease affecting mainly the joint, surrounding tissue and other extra-articular structures in the body. RA can lead to destruction of bone and cartilage which may cause severe disability and it is characterized by the presence of serum rheumatoid factor (RF). The anti-cyclic citrullinate peptide (anti-CCP) antibody is another serum biomarker used in RA diagnosis with higher sensitivity and specificity.
In this cross-sectional study with retrospective record review, 159 established RA patients from Hospital Universiti Sains Malaysia (HUSM) were recruited. Enzyme-linked immunosorbent assays (ELISAs) for serum RF and anti-CCP were performed. Our goal was to evaluate the significance of anti-CCP antibody in predicting the disease activity and progression in terms of radiological and extra-articular manifestations upon diagnosis.
Of the 159 RA patients included in this study, mean age was 48.3 years old and majority (n = 134; 84.3%) were female. A total of 83 (52.2%) and 99 (62.3%) patients had anti-CCP antibody and RF, respectively. Mean Disease Activity Score-28 for Rheumatoid Arthritis with erythrocyte sedimentation rate (ESR) (DAS28-ESR) score for all patients was 4.74 (medium and high disease activity). Fifty-eight (36.5%) patients had radiological defects and 49 (30.8%) patients had extra-articular involvement manifested by rheumatoid nodule, pulmonary involvement, and anemia.
In terms of anti-CCP antibody association with clinical and laboratory parameters, a significant co-occurrence of RF and anti-CCP antibody (P = .002) was observed. Anti-CCP antibody was significantly associated with radiological defects in which majority of patients with such defects (n = 40/58; 68.9%) were positive for anti-CCP antibody (P = .001). However, there was no significant difference between mean and classes of disease activity score and extra-articular manifestations between different anti-CCP antibody groups. In addition, extra-articular manifestations were not associated with high disease activity upon RA diagnosis
There was a significant association between anti-CCP antibody positivity and positive RF. Radiological defects were the sole clinical parameter significantly associated with anti-CCP antibody positivity, indicating that patients positive for anti-CCP antibody should be routinely monitored for radiological defects and their onset.
Keywords: anti-cyclic citrullinated peptide antibody, rheumatoid arthritis, rheumatoid factor
1. Introduction
Rheumatoid arthritis (RA) is a chronic debilitating inflammatory disease affecting mainly the joint and surrounding tissue. The etiology or precipitating factor of this disease is unknown; however interaction between both genetic and environmental factors is thought to contribute to its occurrence.[1] The condition affecting approximately 0.5% to 1% of the world population based on the geographical distribution and ethnically diverse population.[2] RA is a systemic disease that also involves numerous extra-articular organs such as lung, eye, vessels, blood cells, and others. Early and aggressive intervention with established or new drugs can reduce the pathogenic process, improve the function of the joint, and increase the quality of life.[3]
In order to facilitate the diagnosis of early RA, the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) RA classification criteria were introduced in 2010. The criteria redefine RA at the very early stage of diagnosis, compared to the previous 1987 ACR criteria that primarily predicted erosive disease. The introduction of anti-cyclic citrullinated peptide (anti-CCP) antibody assay as a second domain in the criteria is a significant advance in rheumatological field. Anti-CCP antibodies are principally autoantibodies directed against citrullinated proteins in the synovium of RA patients.[4] The importance of this assay in the diagnosis and prognostication of RA has not been determined in Malaysian population of RA patients. Thus the aim of this study is to elucidate the association and efficacy of anti-CCP antibody in different aspects of disease activity, rheumatoid factor (RF), radiological defects, and extra-articular manifestations in the diagnosis of RA.
2. Methods
2.1. Patients and data collection
We retrospectively reviewed the records of 159 RA patients who were diagnosed between 2010 and 2017 at Hospital Universiti Sains Malaysia (HUSM). All the patients met the 2010 ACR/EULAR classification criteria for the disease. Patient who were less than 16 years old, probable RA or overlap syndromes were excluded.
The following clinico-demographic data were retrieved from the Medical Records Unit at HUSM: age, age at onset of RA, gender, Disease Activity Score-28 for Rheumatoid Arthritis with erythrocyte sedimentation rate (ESR) (DAS28-ESR) score and extra-articular manifestations. Data for extra-articular involvements were based on history taking, routine physical examination for pulmonary system, abdomen, rheumatoid nodule, vasculitis, and full blood count for anemia and leucopenia. Rheumatoid nodule and vasculitic lesion over the skin that had been assessed by rheumatologist, dermatologist, or any general physician were counted. Patient with positive lung finding by clinical examination was evaluated by chest radiograph and high-resolution CT (HRCT) thorax if indicated. The study protocol was approved by the local ethics committee of Universiti Sains Malaysia (USM/JEPeM/17020077).
Disease activity was assessed by using DAS28-ESR which includes 28 joints count of swelling and tender joints, ESR and general health assessment using visual analog score (VAS). Elevated ESR levels were defined as >15 mm/h and >20 mm/h in male and female, respectively. It was calculated using DAS28-ESR calculator version 1.2 by A. den Broeder, M. Zandbelt and M. Flendrie (website address: https://www.das-score.nl/das28/DAScalculators/DAS28_4VAR.html). Result of this score was reported in quantitative value divided into 4 categories: remission with score of <2.6, mild activity if score of ≥2.6 to <3.2, moderate activity if score of ≥3.2 to <5.1 and high activity if score of ≥5.1.
2.2. Immunoassays
The patients’ anti-CCP antibodies were analyzed by enzyme-linked immunosorbent assay (ELISA) (Immunoscan RA CCP2, Euro-Diagnostica, Arnhem, the Netherlands) according to the manufacturer's instructions. The results were reported qualitatively where negative or positive for anti-CCP antibody was defined as <20.0 U/mL or ≥20.0 U/mL, respectively. RF status was obtained using the latex agglutination method (RF Direct Latex; VEDALAB, France), and the presence of agglutination was considered as positive for RF.
2.3. Radiological assessment
Radiological defects in RA patients were evaluated using plain radiograph of bilateral hands and feet. Radiological findings of joint erosion and joint space narrowing were identified in any 16 joints of the hand and 6 joints of the feet. Radiological findings were reported and discussed with a radiologist (WAWA).
2.4. Statistical analysis
All data entry and statistical analyses were performed using SPSS Statistics version 22.0 (IBM, Armonk, NY). Numerical variable was expressed in mean (standard deviation, SD) while data for categorical variable was expressed in frequency and percentage. The correlation of study variables was analyzed using proportion formula for prevalence, independent t test for numerical variables, and chi-square or Fisher exact test for categorical variables. The power of this study was set at 80% and confidence interval (CI) was 95%. In all the analyses, a 2-tailed P <.05 was considered statistically significant.
3. Results
3.1. Clinico-demographic characteristics
A total of 182 patients were available for this study, however, 23 patients had incomplete data, and thus 159 patients were included in the analysis. From 159 patients, 134 patients (84.3%) were female. Majority ethnic group in this study was Malay (87.4%) followed by Chinese (n = 16; 10.1%) Siamese (n = 3; 1.9%) and Indian (n = 1; 0.6%) (Table 1). The mean age of the cohort was 48.3 years old ranging from 17 to 79 years old. A total of 99 patients (62.3%) had positive RF while 83 (52.2%) were positive for anti-CCP antibody.
Table 1.
Clinico-demographic and laboratory parameters of RA patients (n = 159).
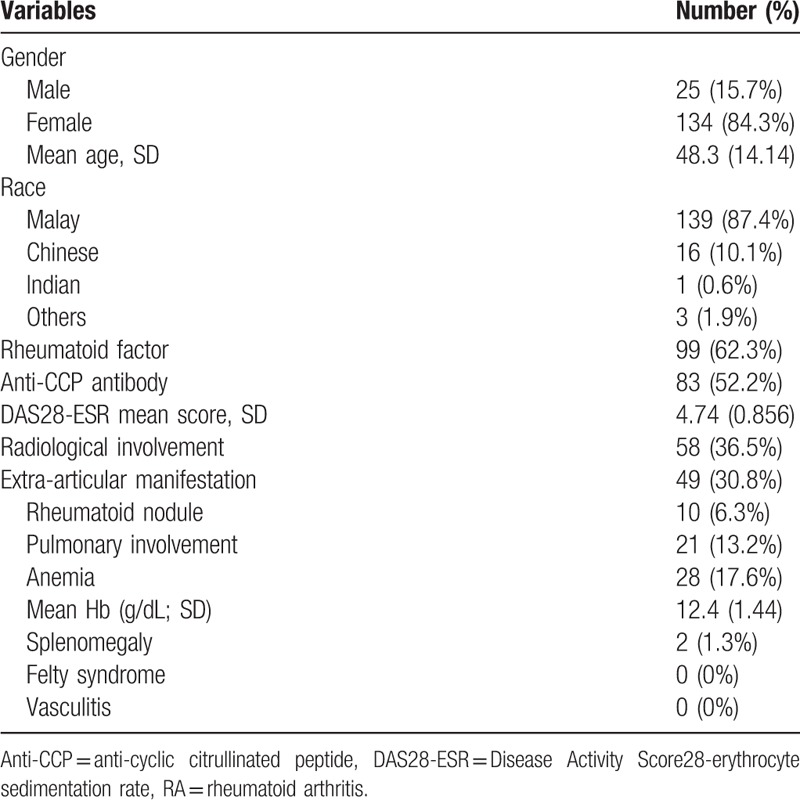
For other variables, mean DAS28-ESR score for all patients upon diagnosis was 4.74 indicating medium disease activities. The 58 patients (36.5%) had radiological involvement upon diagnosis while 49 patients (30.8%) had extra-articular manifestation (Table 1). Rheumatoid nodule was found in 10 patients (6.3%), pulmonary involvement in 21 patients (13.2%) and anemia in 28 patients (17.6%). Mean hemoglobin from total patients was within normal range (12.4 g/dL) and none of the patients had Felty syndrome or vasculitis although 2 patients (1.3%) had splenomegaly without neutropenia.
3.2. Association of anti-CCP antibody with RF and clinical parameters in RA patients
A significant association of RF and anti-CCP antibody co-occurrence (P = .002) was observed where majority of the patients (n = 61; 38.4%) were positive for both RF and anti-CCP antibody followed by RF-positive/anti-CCP antibody-negative (n = 38; 23.9%), RF-negative/anti-CCP antibody-positive (n = 38; 23.9%), and negativity for both RF and anti-CCP antibody (n = 22; 13.8%) (Table 2).
Table 2.
Association of anti-CCP antibody with RF and clinical parameters in RA patients (n = 159). Significant P value in bold.
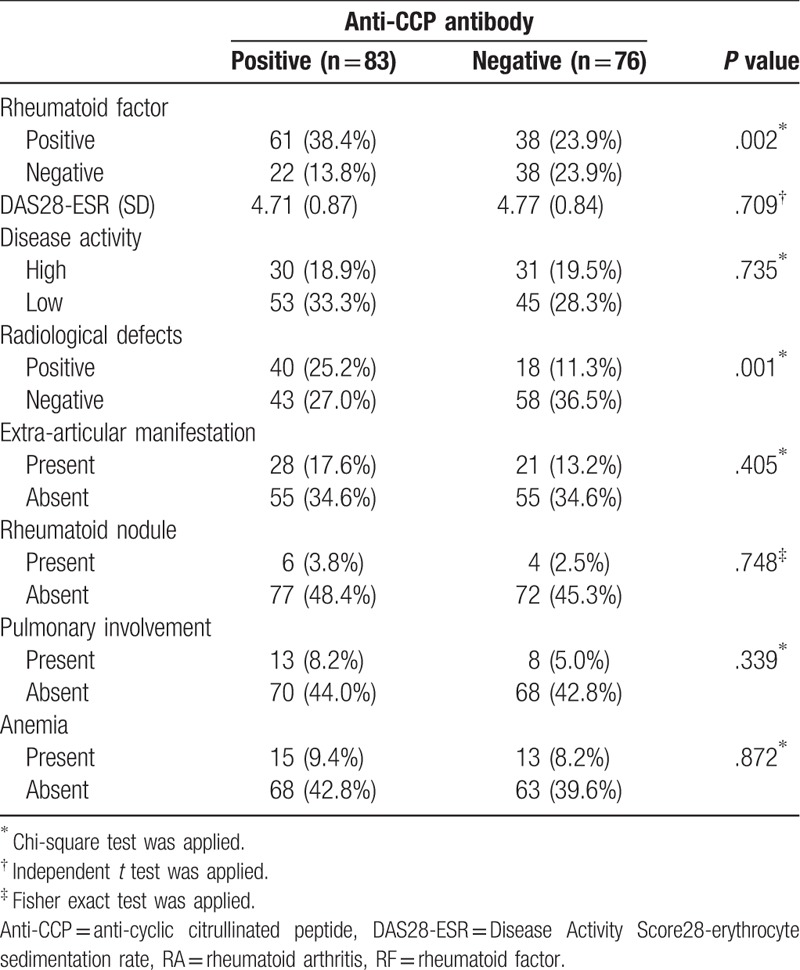
Anti-CCP antibody was not significantly associated with the following clinical parameters: extra-articular manifestations (P = .405) which included rheumatoid nodule (P = .610), pulmonary fibrosis (P = .339) or anemia (P = .873). Anti-CCP antibody was significantly associated with radiological defects whereby majority of patients with radiological defects (n = 40/58; 68.9%) were positive for anti-CCP antibody (P = .001) (Table 2). Radiological defects were the only clinical parameter with significant association with anti-CCP antibody positivity, and the radiological findings of 4 representative patients who were positive for anti-CCP antibody are as follows:
Patient 1 (Fig. 1A): Right wrist radiograph [posteroanterior (PA)] and lateral view revealed diffuse loss of joint space in between carpal bones with periarticular osteopenia of metacarpal bones, distal radius, and distal ulnar. Erosions noted at ulnar and radial styloid erosions with ulnar translocation and marginal erosions with joint space reduction of first metacarpal-phalangeal joint (MCP).
Patient 2 (Fig. 1B): Bilateral hand radiograph (PA) view showed bony ankylosing especially midcarpal compartment, joint space reduction with marginal erosion of all proximal interphalangeal (PIP) joints and bilateral second MCP and periarticular osteopenia.
Patient 3 (Fig. 1C): Bilateral ankle radiograph oblique view revealed bilateral symmetrical diffuse sclerotic, subchondral cyst of tarsal bones with marginal bony erosions.
Patient 4 (Fig. 1D): Left foot radiograph (anteroposterior) and oblique view showed marginal bony erosion of first, third, and fifth metatarsal bone with periarticular joint swelling joint reduction of all PIP joints and periarticular osteopenia.
Figure 1.

Four representative RA patients positive for anti-CCP antibody with radiological defects. A, B: Hand radiographs; C, D: Foot radiographs. L: left; R: right. Anti-CCP = anti-cyclic citrullinated peptide antibody, RA = rheumatoid arthritis.
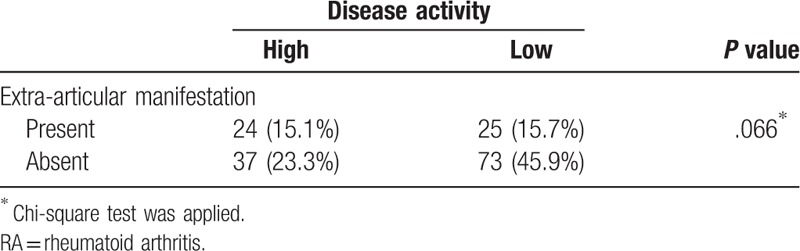
Figure 2 shows the distribution of DAS28-ESR disease activity classes based on the status of anti-CCP antibody. Majority of the patients positive for anti-CCP antibody were categorized into moderate (n = 47/83; 56.6%) or high (n = 30/83; 36.1%) DAS28-ESR class, but similar distributions were also observed for patients negative for anti-CCP antibody in moderate (n = 40/76; 52.6%) or high (n = 31/76; 40.8%) DAS28-ESR class. Indeed, the status of anti-CCP antibody was not significantly associated with DAS28-ESR score (P = .709), or with high or low disease activity (P = .735) (Table 2). Finally, RA patients with low disease activity showed a trend, although insignificant, association with absence of extra-articular manifestations (P = .066) (Table 3).
Figure 2.
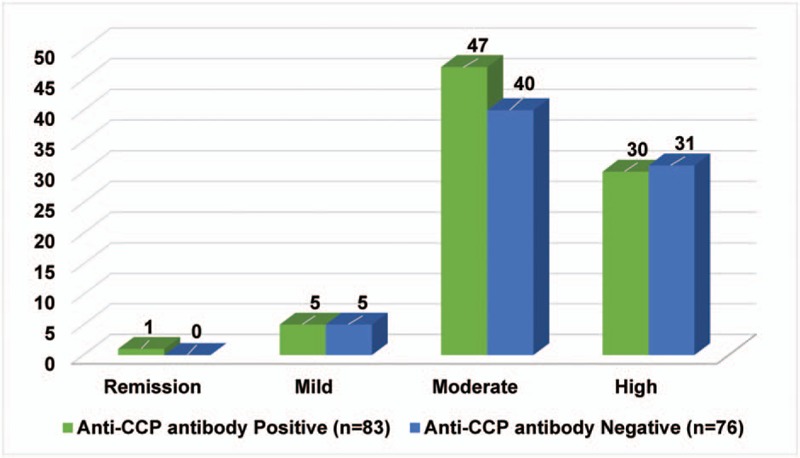
ESR classes based on the status of anti-CCP antibody. Anti-CCP = anti-cyclic citrullinated peptide antibody, ESR = erythrocyte sedimentation rate.
Table 3.
Comparison between disease activity and extra-articular manifestation in RA patients (n = 159).
4. Discussion
4.1. Clinico-demographic and clinical characteristics
In this study, we assessed the association between the status of anti-CCP antibody (positive or negative) with various clinico-demographic and laboratory characteristics in a cohort of 159 RA patients. Majority of the patients were of middle age group at diagnosis with female predominance, consistent with other studies showing similar age group distribution and female preponderance.[5,6] For ethnic distribution in this study, Malay formed the largest ethnic group affected followed by Chinese and Siamese reflecting the local population of the Kelantan state in Malaysia consisting of approximately 85% Malays. Other parameters showed most of the patients had moderate disease activity upon diagnosis with mean DAS28-ESR score of 4.74. Radiological involvement and extra-articular manifestation only occurred in about one-third of the total patients with rheumatoid nodule, pulmonary involvement and anemia became among the most common extra-articular manifestation detected. The development of radiological involvement with extra-articular manifestation in high disease activity patients was consistent with previous studies.[7–9]
4.2. Distribution of RF and anti-CCP antibody in RA patients
For serological tests, both RF and anti-CCP antibody were positive in more than half of the patients with prevalence of 52.2%, consistent with previous studies.[10,11] Our study demonstrated that RF was significantly associated with anti-CCP antibody positivity and this finding was supported by Chou et al[12] where RF was found to be significantly co-occurred with anti-CCP antibody in a cohort of 155 Chinese RA patients. At early stages of disease, RA is often difficult to differentiate from other inflammatory arthritis conditions and RF alone has low sensitivity in diagnosing early RA.[3] Combination of both RF and anti-CCP antibody has been shown to improve the sensitivity of early RA diagnosis[13,14] and might help in predicting poor prognosis in terms of disease activity.[15]
4.3. Anti-CCP antibody and disease activity
RA patients showed variability in disease activity upon diagnosis, which can be difficult to predict at the onset of disease. In this study, majority of the patients had moderate and high disease activity; however, there was no significant difference in both groups in terms of anti-CCP antibody. A study conducted by Serdaroglu et al[16] also found no difference in mean disease activity in both anti-CCP antibody groups. However, this is inconsistent with few other studies that reported significantly higher DAS28-ESR score in anti-CCP antibody positive group.[17,18] The discrepancy in the results was most likely due to disease duration. Longer disease duration associated with higher DAS28-ESR score. This was exemplified in a study by Kastbom et al[19] who did not find significant association between both groups of anti-CCP antibody positivity and DAS28-ESR at 0 month but was significantly higher in the anti-CCP antibody positive group after 12 months of diagnosis. It showed that at certain duration, disease activity was persistently higher in anti-CCP positive group which indicated that these patients experienced a more aggressive disease course. However, in this study, there was no significant difference in disease activity in both anti-CCP antibody groups and this was most likely due to assessment of the disease activity was done only upon diagnosis and we did not assess the disease duration at the beginning of the diagnosis.
4.4. Radiological involvement upon RA diagnosis
There is increasing evidence that radiographic progression, as measured by bony changes in the hands and feet, is associated with active inflammatory activity.[20,21] In this study, we found out that RA patients positive for anti-CCP antibody had significant radiological changes compared to other groups, consistent with the observations reported by other studies.[22,23] Both studies reported a poorer radiological outcome in the presence of RA associated antibodies (anti-CCP or RF). Our study also demonstrated that anti-CCP antibody added prognostic information to ESR and RF. As reported by Vencovsky et al, radiological damage and early erosions were higher in combination with RF and anti-CCP antibodies.[13]
Early detection of radiological involvement is pivotal to prevent irreversible complication and anti-CCP antibody has been shown to be predictive of radiological involvement. It is ideal if the disease progression can be monitored using ultrasound musculoskeletal in addition to DAS28-ESR score as it is easily performed[24] but further studies are required to validate this. We also suggest that novel therapeutic agents targeting anti-CCP antibody might be effective in the treatment of RA patients with radiological defects.
4.5. Extra-articular manifestation associated with anti-CCP antibody and disease activity
Extra-articular manifestation occurred in approximately 40% of RA patients either at the beginning of the diagnosis or during the course of their disease.[25,26] In this study, 30.8% of patients had extra-articular manifestation similar with previous studies.[27,28] The most common extra-articular manifestation found in this study was anemia, followed by pulmonary involvement and rheumatoid nodule. The cause of anemia in RA can be multifactorial, either due to disease activity itself, anemia of chronic disease, drug-induced, nutritional problem, or gastrointestinal bleed[29] but it was not assessed in detail in this study. Further studies on the cause of anemia in RA patients should be conducted to improve the outcome and prevent the complication.
Pulmonary involvement in this study was screened through clinical examination or chest radiograph. However, other pulmonary involvement such as pleural disease and asymptomatic parenchymal pulmonary nodule might have been missed. Rheumatoid nodule was known to be associated with severe form of extra-articular manifestation[8] and in this study, only 10 patients were found to have rheumatoid nodule.
RA patients with positive RF had more extra-articular involvement compared to those with negative RF.[30,31] However, several studies did not find association between anti-CCP antibody and extra-articular manifestation. In this study, we found that the association between RA patients positive for anti-CCP antibody and extra-articular manifestations was not statistically significant. This finding was supported by other similar studies of extra-articular manifestation.[22,26] Many factors may affect the negative results, including patient sample sizes, disease duration, and treatment. As extra-articular manifestation is said to be associated with higher disease activity, higher mortality, poorer functional status, and significantly greater comorbidity,[8,31] anti-CCP antibody might help in the prevention of disease progression. Although anti-CCP antibody was not significant in addressing extra-articular manifestation, but detecting anti-CCP antibody in this type of patient hopefully might help in the prevention of disease progression and further complication.
There was no association between extra-articular manifestation and disease activity in RA patients, suggesting that although extra-articular manifestation was reported upon diagnosis, the patient did not necessarily demonstrate active disease. This observation was different from another study[9] that suggested a significant association between extra-articular manifestation and disease severity. This might be due to differences in extra-articular manifestations in the authors’ study which included pulmonary manifestation namely interstitial lung disease, pleural effusion, and obstructive airway disease, and neurological manifestation.
In conclusion, the usage of anti-CCP antibody is useful in the detection of early disease as evidenced by significant association between anti-CCP antibody, RF, and radiological involvement in our study. Extra-articular manifestations were not associated with high disease activity upon diagnosis of RA.
Acknowledgments
We thank the Director of the Hospital Universiti Sains Malaysia (USM), Kubang Kerian, Kelantan for granting the permission to the investigators to use patients’ medical record; space and assets belong to the hospital during the process of conducting the research. Special thank goes to the staff of the hospital USM who has relentlessly assisted us in making the research work successful.
Author contributions
WSWG and FNS developed the study design. FNS engaged in collecting data, summarized the literature and drafted the manuscript. WAWA provided and reported the X-ray images. WSWG and KKW revised and edited the manuscript. All authors have read and approved the final version of the manuscript.
This study was approved by the ethics committee of Universiti Sains Malaysia. Approval registration number: USM/JEPeM/17020077.
Data curation: Farah Nadiah Sulaiman, Kah Keng Wong.
Formal analysis: Farah Nadiah Sulaiman, Kah Keng Wong, Wan Aireene Wan Ahmed.
Investigation: Farah Nadiah Sulaiman, Wan Aireene Wan Ahmed.
Methodology: Farah Nadiah Sulaiman.
Supervision: Wan Syamimee Wan Ghazali.
Validation: Kah Keng Wong, Wan Syamimee Wan Ghazali.
Writing – original draft: Farah Nadiah Sulaiman.
Writing – review & editing: Kah Keng Wong, Wan Aireene Wan Ahmed, Wan Syamimee Wan Ghazali.
Wan Syamimee Wan Ghazali orcid: 0000-0002-7872-4581.
Footnotes
Abbreviations: ACR = American College of Rheumatology, anti-CCP = anti-cyclic citrullinated peptide, DAS28-ESR = Disease Activity Score-28 for Rheumatoid Arthritis with ESR, ESR = erythrocyte sedimentation rate, EULAR = European League Against Rheumatism, HUSM = Hospital Universiti Sains Malaysia, RA = rheumatoid arthritis, RF = rheumatoid factor.
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
This research received no specific grant from any finding agency in the public, commercial, or not-for-profit sector.
The authors have no conflicts of interest to disclose.
References
- [1].Alamanos Y, Drosos AA. Epidemiology of adult rheumatoid arthritis. Autoimmun Rev 2005;4:130–6. [DOI] [PubMed] [Google Scholar]
- [2].Gabriel SE, Michaud K. Epidemiological studies in incidence, prevalence, mortality, and comorbidity of the rheumatic diseases. Arthritis Res Ther 2009;11:229–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Niewold TB, Harrison MJ, Paget SA. Anti-CCP antibody testing as a diagnostic and prognostic tool in rheumatoid arthritis. QJM 2007;100:193–201. [DOI] [PubMed] [Google Scholar]
- [4].Szekanecz Z, Soos L, Szabo Z, et al. Anti-citrullinated protein antibodies in rheumatoid arthritis: as good as it gets? Clin Rev Allergy Immunol 2008;34:26–31. [DOI] [PubMed] [Google Scholar]
- [5].Lee DM, Schur PH. Clinical utility of the anti-CCP assay in patients with rheumatic diseases. Ann Rheum Dis 2003;62:870–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Shakiba Y, Koopah S, Jamshidi AR, et al. Anti-cyclic citrullinated peptide antibody and rheumatoid factor isotypes in Iranian patients with rheumatoid arthritis: evaluation of clinical value and association with disease activity. Iran J Allergy Asthma Immunol 2014;13:147–56. [PubMed] [Google Scholar]
- [7].Eltokhy HM, Ali ST, Rabo SAA, et al. Relationship between anti-cyclic citrullinated peptide antibodies and disease activity and extra-articular manifestations of rheumatoid arthritis in Egyptian patients. Al-Azhar Assiut Med J 2011;9:21–35. [Google Scholar]
- [8].Richman NC, Yazdany J, Graf J, et al. Extraarticular manifestations of rheumatoid arthritis in a multiethnic cohort of predominantly Hispanic and Asian patients. Medicine (Baltimore) 2013;92:92–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Kalappan M, Abubacker NRT, Shetty M, et al. Study of extra-articular manifestations and disease severity in patients with rheumatoid arthritis 2016;3:53–6. [Google Scholar]
- [10].Sockalingam S, Khuan CS, Sthaneshwar P. Prevalence of anti cyclic citrullinated peptide antibodies in Malaysian rheumatoid arthritis patients and its correlation with disease activity. Int J Rheum Dis 2009;12:211–5. [DOI] [PubMed] [Google Scholar]
- [11].Abdul Wahab A, Mohammad M, Rahman MM, et al. Anti-cyclic citrullinated peptide antibody is a good indicator for the diagnosis of rheumatoid arthritis. Pak J Med Sci 2013;29:773–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Chou C, Liao H, Chen C, et al. The clinical application of anti-CCP in rheumatoid arthritis and other rheumatic diseases. Biomark Insights 2007;2:165–71. [PMC free article] [PubMed] [Google Scholar]
- [13].Vencovsky J, Machacek S, Sedova L, et al. Autoantibodies can be prognostic markers of an erosive disease in early rheumatoid arthritis. Ann Rheum Dis 2003;62:427–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Dubucquoi S, Solau-Gervais E, Lefranc D, et al. Evaluation of anti-citrullinated filaggrin antibodies as hallmarks for the diagnosis of rheumatic diseases. Ann Rheum Dis 2004;63:415–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Bas S, Genevay S, Meyer O, et al. Anti-cyclic citrullinated peptide antibodies, IgM and IgA rheumatoid factors in the diagnosis and prognosis of rheumatoid arthritis. Rheumatology (Oxford) 2003;42:677–80. [DOI] [PubMed] [Google Scholar]
- [16].Serdaroglu M, Cakirbay H, Deger O, et al. The association of anti-CCP antibodies with disease activity in rheumatoid arthritis. Rheumatol Int 2008;28:965–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].del Val del Amo N, Ibanez Bosch R, Fito Manteca C, et al. Anti-cyclic citrullinated peptide antibody in rheumatoid arthritis: relation with disease aggressiveness. Clin Exp Rheumatol 2006;24:281–6. [PubMed] [Google Scholar]
- [18].Zendman AJ, van Venrooij WJ, Pruijn GJ. Use and significance of anti-CCP autoantibodies in rheumatoid arthritis. Rheumatology (Oxford) 2006;45:20–5. [DOI] [PubMed] [Google Scholar]
- [19].Kastbom A, Strandberg G, Lindroos A, et al. Anti-CCP antibody test predicts the disease course during 3 years in early rheumatoid arthritis (the Swedish TIRA project). Ann Rheum Dis 2004;63:1085–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Meyer O, Labarre C, Dougados M, et al. Anticitrullinated protein/peptide antibody assays in early rheumatoid arthritis for predicting five year radiographic damage. Ann Rheum Dis 2003;62:120–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Forslind K, Ahlmen M, Eberhardt K, et al. Prediction of radiological outcome in early rheumatoid arthritis in clinical practice: role of antibodies to citrullinated peptides (anti-CCP). Ann Rheum Dis 2004;63:1090–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].De Rycke L, Peene I, Hoffman IE, et al. Rheumatoid factor and anticitrullinated protein antibodies in rheumatoid arthritis: diagnostic value, associations with radiological progression rate, and extra-articular manifestations. Ann Rheum Dis 2004;63:1587–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Fathi NA, Ezz-Eldin AM, Mosad E, et al. Diagnostic performance and predictive value of rheumatoid factor, anti-cyclic-citrullinated peptide antibodies and HLA-DRB1 locus genes in rheumatoid arthritis. Int Arch Med 2008;1:20–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Hamed R, Søren TP, Erik AK, et al. Diagnostic utility of musculoskeletal ultrasound in patients with suspected arthritis – a probabilistic approach. Arthritis Res Ther 2014;16:448–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Cimmino MA, Salvarani C, Macchioni P, et al. Extra-articular manifestations in 587 Italian patients with rheumatoid arthritis. Rheumatol Int 2000;19:213–7. [DOI] [PubMed] [Google Scholar]
- [26].Korkmaz C, Us T, Kasifoglu T, et al. Anti-cyclic citrullinated peptide (CCP) antibodies in patients with long-standing rheumatoid arthritis and their relationship with extra-articular manifestations. Clin Biochem 2006;39:961–5. [DOI] [PubMed] [Google Scholar]
- [27].Turesson C, McClelland RL, Christianson TJ, et al. Multiple extra-articular manifestations are associated with poor survival in patients with rheumatoid arthritis. Ann Rheum Dis 2006;65:1533–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Cojocaru M, Cojocaru IM, Silosi I, et al. Extra-articular manifestations in rheumatoid arthritis. Maedica (Buchar) 2010;5:286–91. [PMC free article] [PubMed] [Google Scholar]
- [29].Agrawal S, Misra R, Aggarwal A. Anemia in rheumatoid arthritis: high prevalence of iron-deficiency anemia in Indian patients. Rheumatol Int 2006;26:1091–5. [DOI] [PubMed] [Google Scholar]
- [30].Eker YO, Pamuk ON, Pamuk GE, et al. The Frequency of anti-CCP antibodies in patients with rheumatoid arthritis and psoriatic arthritis and their relationship with clinical features and parameters of angiogenesis: a comparative study. Eur J Rheumatol 2014;1:67–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Vela P. Extra-articular manifestations of rheumatoid arthritis, now. EMJ Rheumatol 2014;1:103–12. [Google Scholar]