

Abstract
While the opioid epidemic has garnered significant attention, the use of methamphetamines is growing worldwide independent of wealth or region. Following overdose and accidents, the leading cause of death in methamphetamine users is cardiovascular disease, due to significant effects of methamphetamine on vasoconstriction, pulmonary hypertension, atherosclerotic plaque formation, cardiac arrhythmias, and cardiomyopathy. In this review, we examine the current literature on methamphetamine-induced changes in cardiovascular health, discuss the potential mechanisms regulating these varied effects, and highlight our deficiencies in understanding how to treat methamphetamine-associated cardiovascular dysfunction.
Keywords: cardiovascular pathophysiology, catecholamine, drug abuse, vascular remodeling, cardiac dysfunction
Graphical Abstract
Introduction
Reports from a variety of sources suggest that the United States is currently experiencing an opioid epidemic initiated by the unanticipated proliferation of opioid prescriptions starting in the late 1990s, with the subsequent accelerated misuse of these drugs for nonmedical purposes.1-3 At the same time, however, methamphetamine use has also been increasing across the country, indicating that the use of this drug is developing into its own epidemic4. Methamphetamine, a highly potent amphetamine derivative, produces significant effects on physical, behavioral, cognitive, and psychiatric output.5, 6 Widely used for its ability to increase wakefulness and physical activity and decrease appetite, methamphetamine’s widespread misuse results from the intense euphoria the drug produces.7 These effects are largely due to the ability of methamphetamine to enhance monoamine (e.g. dopamine, noradrenaline) levels in the synaptic cleft. Epidemiological studies demonstrate that amphetamine-type stimulants are the most widely used illicit drug in the world after cannabis, with up to 51 million global users between the ages of 15 and 64.8, 9 Methamphetamine use is a growing worldwide phenomenon, with the consumption of the drug occurring independently of wealth, geographical location, and culture.
Methamphetamine (N-methyl-alpha-methylphenethylamine) is a cationic molecule and chiral compound based around a phenylethylamine core, obviously distinguishable from its amphetamine analogs by an additional methyl group (Figure 1A). This moiety makes methamphetamine highly lipophilic, thereby allowing it to increasingly penetrate the blood-brain barrier.5 Methamphetamine functions in neuronal tissue by promoting catecholamine (e.g. dopamine, norepinephrine) signaling through multiple mechanisms. Methamphetamine binds vesicular monoamine transporter-2 and accumulates in vesicles where it alters the pH resulting in catecholamine release into the cytosol (Figure 1B).10, 11 Additionally, methamphetamine inhibits the catecholamine catabolizing enzyme monoamine oxidase to stabilize cytosolic catecholamine levels. Interaction between methamphetamine and the dopamine transporter and norepinephrine transporter prevents catecholamine uptake and stimulates catecholamine release through exchange diffusion and modulation of receptor activity (Figure 1B).10, 11 While this results in acute increases in dopamine and norepinephrine signaling driving the methamphetamine-associated euphoria, chronic methamphetamine use induces neurotoxicity in dopaminergic axon terminals, associated with reduced dopamine production and reduced expression of the dopamine transporter.11 Additionally, methamphetamine induces neuronal cell death associated with endoplasmic reticulum stress, mitochondrial dysfunction, and enhanced reactive oxygen species (ROS) production.11
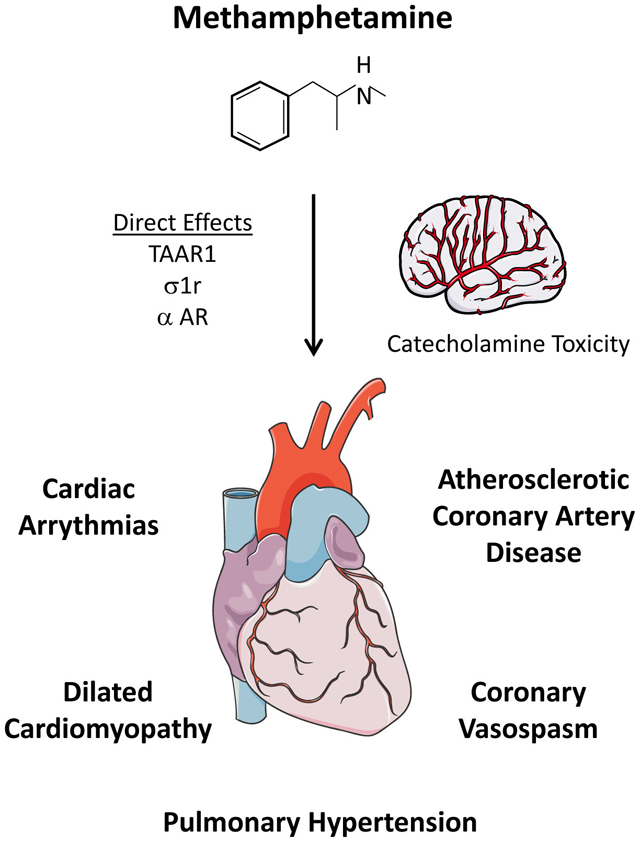
Figure 1. Methamphetamine effects and receptors.

A. Chemical structures of the catecholamines dopamine and norepinephrine, amphetamine, and methamphetamine. B. Effects of methamphetamine on catecholamine signaling. DAT, dopamine transporter; NET, norepinephrine transporter; VMAT2, vesicular monoamine transporter 2. C. Catecholamine-independent effects of methamphetamine. TAAR1, trace amino acid receptor 1; δ1r, sigma1 receptor; α2 AR, α2 adrenergic receptor.
While exposure of methamphetamine results in deleterious consequences to the neurological system, it also elicits a range of other adverse effects.12 Several clinical and postmortem studies clearly associate the use of methamphetamine with cardiovascular disease,13 and cardiovascular disease represents the second leading cause of death among methamphetamine abusers following only accidental overdose.14 Methamphetamine can have adverse and potentially fatal effects on arteries and blood vessels, including elevated blood pressure, acute vasospasm, and atherosclerotic cardiovascular disease. In addition, methamphetamine induces structural and electrical remodeling of cardiac tissue leading to arrhythmias and heart failure. However, the mechanisms surrounding these and other pathological responses of the cardiovascular system in methamphetamine abusers remains largely unknown. Methamphetamine may induce cardiovascular complications through catecholamine toxicity due to its high-affinity interactions with binding sites on the dopamine transporter (DAT, Ki = 0.46 μM) and norepinephrine transporter (NET, Ki = 0.11 μM).15 However, methamphetamine also interacts with moderate affinity to binding sites in other receptors present in the cardiovascular system, including the trace amino acid receptor 1 (TAAR1, EC50 ~1-3 μM), sigma (σ) receptor 1 (σ1r, Ki ~2 μM), and α2 adrenergic receptors (Ki ~1 μM) (Figure 1C).16-19 While originally thought to be a cell surface opioid receptor, the σ1 receptor primarily localizes to the endoplasmic reticulum and mitochondrial membrane, which may contribute to the effect of cytosolic methamphetamine signaling.20 Data collected from human methamphetamine users suggest that plasma methamphetamine concentrations average 2-3 μM, whereas concentrations can reach 17 μM in individuals arrested for erratic behavior and 87 μM in post-mortem samples from non-overdose patients.21-23 Therefore, the plasma methamphetamine levels in humans are sufficient to bind to and interact with all of the potential methamphetamine binding sites listed above.
In this review, we summarize the current literature on the effects of methamphetamine use on cardiovascular dysfunction, with a focus on vasoconstriction and pulmonary hypertension, atherosclerotic cardiovascular disease, cardiac arrhythmias, and cardiomyopathy. These studies highlight the importance of understanding methamphetamine-driven cardiovascular disease, and highlight the limitations of our current understanding of molecular mechanisms involved.
Methamphetamine-mediated vasoconstriction and pulmonary hypertension.
Methamphetamine administration in human subjects results in an acute, rapid increase in both heart rate and blood pressure.24 In mouse models, acute methamphetamine exposure induced vasoconstriction of pial arteries and intracerebral arteries,25, 26 and chronic methamphetamine exposure has been shown to promote vasoconstriction and persistent cerebral hypoperfusion driven by neurovascular damage and an imbalance of circulating vasoregulatory substances.27 Regulation of vascular tone and arterial blood pressure is maintained by neuronal stimulation and by circulating and endothelial-derived vasoactive substances.28 Endothelin, angiotensin II, and catecholamines promote vasoconstriction through G protein-coupled receptors that drive Gαq-dependent smooth muscle calcium influx. In contrast, circulating and endothelial-derived vasodilators (nitric oxide (NO), prostacyclin) reduce smooth muscle contraction by inhibiting either calcium influx or myosin phosphorylation. While the mechanisms of methamphetamine-induced vasoconstriction remain poorly described, current evidence suggests vasoconstriction by amphetamines and trace amines involves endothelial release of endothelin-125 or arterial TAAR1 signaling,29 whereas neuronal catecholamine signaling and adrenergic receptor signaling do not appear to be involved (Figure 2A).30 Consistent with methamphetamine-associated vasoconstriction, methamphetamine use is commonly associated with acute angina associated with vasospasm of the coronary arteries or coronary microvasculature, resulting in severely diminished blood flow to cardiac tissue. In one case report, methamphetamine induced coronary vasospasm resulting in myocardial infarction was found to be unresponsive to vasodilator therapy. Similarly, a small study of 20 methamphetamine users and 21 age-matched controls showed reduced nitroglycerine-mediated vasodilation in the methamphetamine users,31 suggesting that methamphetamine promotes smooth muscle dysfunction and reduced NO sensitivity.
Figure 2. Cardiovascular effects of methamphetamine use.

A. Methamphetamine use is associated with acute vascular constriction and vasospasm, whereas chronic methamphetamine use drives endothelial damage and pulmonary hypertension in some patients. B. Enhanced atherosclerotic plaque formation following methamphetamine use correlates with enhanced inflammation due to endothelial activation and increased T cell and macrophage-driven proinflammatory signaling. C. Methamphetamine use drives cardiac structural (fibrosis, inflammation) and electrical remodeling, associated with QT prolongation and susceptibility to arrhythmias. D. Exposure to methamphetamine promotes mitochondrial dysfunction and dilated cardiomyopathy. These cardiotoxic properties appear to involve both catecholaminergic toxicity and direct toxicity.
While there are minimal reports concerning systemic, chronic hypertension in methamphetamine users, prolonged methamphetamine abuse can result in a marked increase in pulmonary hypertension.32, 33 Methamphetamine administered intravenously shows primary accumulation in the lung, where it is internalized and metabolized by pulmonary endothelial cells.34, 35 Endothelial exposure to methamphetamine resulted in enhanced ROS production and compensatory autophagy (Figure 2A).34, 36 Endothelial cells metabolize methamphetamine through carboxylesterase 1 (CES1), and a single nucleotide polymorphism in the CES1 predicted to reduce CES1 activity is associated with elevated ROS production, reduced endothelial autophagy, and enhanced endothelial apoptosis.34 Of particular interest, nearly all of the methamphetamine-associated pulmonary hypertension patients examined were heterozygous for this polymorphism.34
Multiple mechanisms may couple methamphetamine to induction of compensatory autophagy. While methamphetamine administration promotes dysfunction of amino acid and lipid metabolism triggering autophagy, methamphetamine also promotes dissociation of the Bcl-2/Beclin 1 complex, thereby limiting Bcl-2’s ability to inhibit autophagy.37, 38 This compensatory autophagy during methamphetamine consumption may be a potential protective mechanism against apoptotic cell death. In primary human brain microvascular endothelial cells and human umbilical vein endothelial cells, preventing autophagy following methamphetamine treatment enhanced endothelial apoptosis.39 Reduced compensatory autophagy upon CES depletion suggests that high levels of methamphetamine may hinder compensatory autophagy to promote endothelial cell death. However, additional studies are required to better define the pro-survival and pro-apoptotic functions of autophagy induction during methamphetamine-induced toxicity.
Methamphetamine in atherosclerotic cardiovascular disease.
The use of methamphetamine clearly increases the rate of coronary artery disease, with myocardial infarction often observed in very young patients with a history of methamphetamine abuse. A 1999 posthumous study of decedents from southern California demonstrated that methamphetamine users had an increase in minimal to severe atherosclerotic coronary artery disease (19%) compared to sex-aged matched controls (0.5%).40 Two posthumously studies from Australia also observed increased coronary artery disease severity among methamphetamine users in which 54% of patients had observed coronary artery disease and up to 10% had extremely severe coronary artery disease not observed in control cohorts.14, 41 Furthermore, chronic methamphetamine treatment of atherosclerosis-prone apolipoprotein E knockout mice increased atherosclerotic severity, providing direct evidence linking methamphetamine use to enhanced plaque formation.42, 43
Methamphetamine usage reduces traditional risk factors associated with atherosclerosis, such as elevated serum cholesterol and obesity, consistent with its known function as an appetite suppressor. However, atherosclerosis is a multifactorial disease involving local endothelial activation, intimal cholesterol deposition, leukocyte recruitment and dysfunction, and smooth muscle driven fibroproliferative remodeling.44 Methamphetamine can promote multiple aspects of endothelial activation, such as permeability and enhanced proinflammatory gene expression, in part due to enhanced ROS production (Figure 2B).45, 46 Analysis of mRNA from methamphetamine-treated mice demonstrates increased expression in pro-inflammatory markers of endothelial activation, such as intercellular adhesion molecule-1, vascular cell adhesion molecule-1, and monocyte chemotractant protein-1.42, 43 Additionally, methamphetamine can elicit pro-inflammatory responses from macrophages, as treatment of human derived-macrophages with methamphetamine elicits production of ROS, interleukin (IL)-6, and IL-1β, which are all known atherogenic factors,47 and plaques from methamphetamine-treated mice show increased pro-inflammatory T cell and macrophage levels (Figure 2B). Furthermore, methamphetamine directly alters mitochondria activity, leading to increased production of ROS and reactive nitrogen species that could potentiate atherogenic inflammation.48 While plaques from methamphetamine-treated mice show an increase in smooth muscle area, the elevated levels of interferon γ and reduced transforming growth factor β observed in these plaques would be predicted to promote smooth muscle apoptosis and reduce extracellular matrix deposition, consistent with the vulnerable plaque phenotype.42, 43 However, little is currently known about the regulation of vascular smooth muscle cell phenotype by methamphetamine exposure.
Methamphetamine and Cardiac Arrhythmias
A retrospective analysis of the United States National Inpatient Sample database involving more than 35 million patients and over 180,000 methamphetamine users demonstrated that methamphetamine users have a 27% increased risk of sudden cardiac death.49 Similarly, a review of the Australian National Coronial Information System data showed that 6.5% of all non-accidental deaths in methamphetamine users is due to sudden cardiac death.50 Most of these studies suffer from the bias of retrospective adjudication of deaths based on records and may offer only a glimpse of the actual problem. While there are isolated case reports of monomorphic ventricular tachycardia in methamphetamine users,51 there are no prospective observational studies or animal studies looking at the actual incidence of arrhythmias in methamphetamine users. However, there is now growing evidence that electrical and substrate changes induced by methamphetamine does induce prolonged QT changes in 12-lead electrocardiograms, suggesting an increased vulnerable period for initiation of and increased risk for ventricular arrhythmias (Figure 2C).52 The only animal study designed to assess the acute effect of methamphetamine on cardiac rhythm observed increased atrial and ventricular ectopic beats and sinus tachycardia in the 30 minutes following methamphetamine administration but no sustained ventricular arrhythmias.53
Methamphetamine use is associated with cardiac structural and cellular changes that are typically linked to cardiac arrhythmias (Figure 2C). Endomyocardial biopsies from the ventricles from patients with methamphetamine-associated cardiomyopathy showed increased markers of inflammation and fibrosis. Ventricular fibrosis in patients with methamphetamine-associated cardiomyopathy has been corroborated by cardiac MRI by other investigators.54 The extent of fibrosis directly correlated with duration of methamphetamine use and predicted recovery with discontinuation of the drug.55 In addition to structural remodeling described above, methamphetamine is also associated with cardiac electrical remodeling. Animal studies show decreased expression and activity of multiple potassium channels and voltage-gated calcium channels, which recovered significantly by week eight of withdrawing methamphetamine.56 In isolated ventricular myocytes, methamphetamine inhibited transient outward potassium current, inward rectifier potassium current and L-type calcium current in a dose dependent manner.57 In contrast, Sugimoto et al. found that methamphetamine treatment increases rat neonatal ventricular myocyte beating rates and calcium spark frequency in an L-type calcium channel-dependent manner.58 However, both studies highlight the ability of methamphetamine to directly affect cardiac myocyte function independent of catecholaminergic changes associated with the in vivo model.
Methamphetamine-associated cardiomyopathy.
Methamphetamine-related cardiomyopathy is associated with severe systolic dysfunction, left ventricular chamber dilation.55, 59 Clinical and autopsy reports obtained from long-term methamphetamine users showed indicators of cardiomyopathy, such as necrosis, fibrosis, hypertrophy, and enlargement of the heart.60 The degree of fibrosis predicts the functional recovery following cessation of methamphetamine use, whereas cardiac function did not improve in any of the patients that continued methamphetamine use.55 Methamphetamine use most commonly promotes dilated cardiomyopathy with an enlarged, dilated heart and severely diminished contractile function.61 In animal models, methamphetamine–administration induces cardiomyopathies with a disarray of cardiomyocytes, intracellular and extracellular edema, abnormally shaped mitochondria and nuclei, dilated T-tubules, myocyte degeneration, contraction band degeneration, and myofilament loss (Figure 2D).62 Methamphetamine-associated cardiotoxic effects have been reported following acute administration, chronic administration, and binge administration (i.e., frequent doses followed by a period of abstinence), suggesting both a rapid and sustained influence on myocardial function.
The molecular mechanisms of methamphetamine-associated cardiomyopathy are multifactorial, and possible etiologies are primarily based on cursory observations, such as excess catecholamine levels, ROS generation, mitochondrial dysfunction, metabolic dysregulation, coronary vasospasm, and myocardial ischemia.13 Studies showing that both short-term and longer-term methamphetamine exposure induce cellular damage and hypertrophy in isolated, cultured cardiomyocytes support a role for catecholamine-independent direct cardiotoxicity.57, 63, 64 However, the molecular targets and mechanisms driving the cellular effects of methamphetamine on the heart remain unknown.
Summary and Future Directions.
Methamphetamine use clearly induces a multifactoral dysfunction of the cardiovascular system, including both acute and chronic deleterious effects. Acute effects of methamphetamine often result in myocardial infarction driving users to the clinic. Methamphetamine use induces potent vasoconstriction that can result in severe vasospasm of the coronary arteries and microvasculature resulting in myocardial ischemia. In addition to vasospasm, methamphetamine users show significantly worsened atherosclerotic cardiovascular disease despite the reduction in several typical atherosclerotic risk factors. While currently poorly characterized, this pro-atherosclerotic effect may involve enhanced proinflammatory responses that contribute to plaque vulnerability, which may produce clinical manifestations in the context of methamphetamine-induced transient elevations in blood pressure. While there is minimal data suggesting that chronic methamphetamine use induces persistent hypertension, methamphetamine use significantly enhances susceptibility for pulmonary hypertension, especially in users with polymorphisms in the methamphetamine-degrading enzyme CES1. In the heart, methamphetamine promotes myocardial structural and electrical remodeling, which may promote cardiac arrhythmias. Ultimately, methamphetamine induces profound mitochondrial dysfunction and cardiac myocyte death driving dilated cardiomyopathy and heart failure.
Currently, many questions remain unanswered regarding methamphetamine mediated cardiovascular disease. While reduced mitochondrial function and enhanced oxidative stress represent common effects of methamphetamine use, specific reasons for these molecular changes underlying much of the cardiovascular complications are still unknown. More research is needed to identify critical molecular pathways and prognostic markers in order to evaluate and predict methamphetamine-induced pathological defects, along with environmental and genetic risk factors that contribute to methamphetamine-mediated cardiovascular events. While current clinical and animal studies provide compelling evidence of cardiovascular dysfunction, methamphetamine-associated cardiovascular complications remain an underappreciated clinical burden that requires systemic study to elucidate the prevalence of pathology and to define molecular mechanisms of disease progression.
Highlights.
Methamphetamine use is rising globally resulting in significant morbidity and mortality driven by a poorly understood increase in multiple forms of cardiovascular disease.
Methamphetamines may promote cardiovascular disease through catecholamine toxicity or through direct effects on cardiac and vascular tissue.
The use of methamphetamine is associated with pulmonary hypertension, particularly in patients showing specific polymorphisms in the methamphetamine catabolizing enzyme carboxylesterase 1.
Symptoms of myocardial infarction among methamphetamine users result from both acute coronary vasospasm and enhanced atherosclerotic plaque formation.
Remodeling of cardiac tissue following methamphetamine exposure promotes dilated cardiomyopathy and may enhance the susceptibility to cardiac arrhythmias.
Acknowledgments
Sources of Funding
This publication was supported by an Institutional Development Award (IDeA) from the National Institutes of General Medical Sciences of the NIH under grant number P20GM121307 to C.G.K and by NIH R01 HL098435, HL133497, and HL141155 to A.W.O, HL131844 to M.D.W., and HL122354 and HL145753 to M.S.B.
Abbreviations:
- CES1
carboxylesterase 1
- NO
nitric oxide
- ROS
reactive oxygen species
- TAAR1
trace amino acid receptor 1
- IL
interleukin
Footnotes
Disclosures
None
References
- 1.Guy GP Jr., Zhang K, Bohm MK, Losby J, Lewis B, Young R, Murphy LB, Dowell D. Vital signs: Changes in opioid prescribing in the united states, 2006-2015. MMWR Morb Mortal Wkly Rep. 2017;66:697–704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Maxwell JC. The prescription drug epidemic in the united states: A perfect storm. Drug Alcohol Rev. 2011;30:264–270 [DOI] [PubMed] [Google Scholar]
- 3.McHugh RK, Nielsen S, Weiss RD. Prescription drug abuse: From epidemiology to public policy. J Subst Abuse Treat. 2015;48:1–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ben-Yehuda O, Siecke N. Crystal methamphetamine: A drug and cardiovascular epidemic. JACC Heart Fail. 2018;6:219–221 [DOI] [PubMed] [Google Scholar]
- 5.Homer BD, Solomon TM, Moeller RW, Mascia A, DeRaleau L, Halkitis PN. Methamphetamine abuse and impairment of social functioning: A review of the underlying neurophysiological causes and behavioral implications. Psychol Bull. 2008;134:301–310 [DOI] [PubMed] [Google Scholar]
- 6.Meredith CW, Jaffe C, Ang-Lee K, Saxon AJ. Implications of chronic methamphetamine use: A literature review. Harv Rev Psychiatry. 2005;13:141–154 [DOI] [PubMed] [Google Scholar]
- 7.Panenka WJ, Procyshyn RM, Lecomte T, MacEwan GW, Flynn SW, Honer WG, Barr AM. Methamphetamine use: A comprehensive review of molecular, preclinical and clinical findings. Drug Alcohol Depend. 2013;129:167–179 [DOI] [PubMed] [Google Scholar]
- 8.McKetin R, Lubman DI, Baker AL, Dawe S, Ali RL. Dose-related psychotic symptoms in chronic methamphetamine users: Evidence from a prospective longitudinal study. JAMA Psychiatry. 2013;70:319–324 [DOI] [PubMed] [Google Scholar]
- 9.Wearne TA, Cornish JL. A comparison of methamphetamine-induced psychosis and schizophrenia: A review of positive, negative, and cognitive symptomatology. Front Psychiatry. 2018;9:491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Robertson SD, Matthies HJ, Galli A. A closer look at amphetamine-induced reverse transport and trafficking of the dopamine and norepinephrine transporters. Mol Neurobiol. 2009;39:73–80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fleckenstein AE, Volz TJ, Riddle EL, Gibb JW, Hanson GR. New insights into the mechanism of action of amphetamines. Annu Rev Pharmacol Toxicol. 2007;47:681–698 [DOI] [PubMed] [Google Scholar]
- 12.Rusyniak DE. Neurologic manifestations of chronic methamphetamine abuse. Neurologic Clinics. 2011;29:641–655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Won S, Hong RA, Shohet RV, Seto TB, Parikh NI. Methamphetamine-associated cardiomyopathy. Clin Cardiol. 2013;36:737–742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Darke S, Duflou J, Kaye S. Prevalence and nature of cardiovascular disease in methamphetamine-related death: A national study. Drug Alcohol Depend. 2017;179:174–179 [DOI] [PubMed] [Google Scholar]
- 15.Han DD, Gu HH. Comparison of the monoamine transporters from human and mouse in their sensitivities to psychostimulant drugs. BMC Pharmacol. 2006;6:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Reese EA, Bunzow JR, Arttamangkul S, Sonders MS, Grandy DK. Trace amine-associated receptor 1 displays species-dependent stereoselectivity for isomers of methamphetamine, amphetamine, and para-hydroxyamphetamine. J Pharmacol Exp Ther. 2007;321:178–186 [DOI] [PubMed] [Google Scholar]
- 17.Lewin AH, Miller GM, Gilmour B. Trace amine-associated receptor 1 is a stereoselective binding site for compounds in the amphetamine class. Bioorg Med Chem. 2011;19:7044–7048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nguyen EC, McCracken KA, Liu Y, Pouw B, Matsumoto RR. Involvement of sigma (sigma) receptors in the acute actions of methamphetamine: Receptor binding and behavioral studies. Neuropharmacology. 2005;49:638–645 [DOI] [PubMed] [Google Scholar]
- 19.U’Prichard DC, Greenberg DA, Snyder SH. Binding characteristics of a radiolabeled agonist and antagonist at central nervous system alpha noradrenergic receptors. Mol Pharmacol. 1977;13:454–473 [PubMed] [Google Scholar]
- 20.Sambo DO, Lin M, Owens A, et al. The sigma-1 receptor modulates methamphetamine dysregulation of dopamine neurotransmission. Nat Commun. 2017;8:2228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Logan BK, Fligner CL, Haddix T. Cause and manner of death in fatalities involving methamphetamine. J Forensic Sci. 1998;43:28–34 [PubMed] [Google Scholar]
- 22.Melega WP, Cho AK, Harvey D, Lacan G. Methamphetamine blood concentrations in human abusers: Application to pharmacokinetic modeling. Synapse. 2007;61:216–220 [DOI] [PubMed] [Google Scholar]
- 23.McIntyre IM, Nelson CL, Schaber B, Hamm CE. Antemortem and postmortem methamphetamine blood concentrations: Three case reports. J Anal Toxicol. 2013;37:386–389 [DOI] [PubMed] [Google Scholar]
- 24.Fleury G, De La Garza R 2nd, Mahoney JJ 3rd, Evans SE, Newton TF. Predictors of cardiovascular response to methamphetamine administration in methamphetamine-dependent individuals. Am J Addict. 2008;17:103–110 [DOI] [PubMed] [Google Scholar]
- 25.Seo JW, Jones SM, Hostetter TA, Iliff JJ, West GA. Methamphetamine induces the release of endothelin. J Neurosci Res. 2016;94:170–178 [DOI] [PubMed] [Google Scholar]
- 26.Polesskaya O, Silva J, Sanfilippo C, Desrosiers T, Sun A, Shen J, Feng C, Polesskiy A, Deane R, Zlokovic B, Kasischke K, Dewhurst S. Methamphetamine causes sustained depression in cerebral blood flow. Brain Res. 2011;1373:91–100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kousik SM, Graves SM, Napier TC, Zhao C, Carvey PM. Methamphetamine-induced vascular changes lead to striatal hypoxia and dopamine reduction. 2011;22:923–928 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Loh YC, Tan CS, Ch’ng YS, Yeap ZQ, Ng CH, Yam MF. Overview of the microenvironment of vasculature in vascular tone regulation. International Journal of Molecular Sciences. 2018;19:120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Fehler M, Broadley KJ, Ford WR, Kidd EJ. Identification of trace-amine-associated receptors (taar) in the rat aorta and their role in vasoconstriction by beta-phenylethylamine. Naunyn Schmiedebergs Arch Pharmacol. 2010;382:385–398 [DOI] [PubMed] [Google Scholar]
- 30.Broadley KJ, Fehler M, Ford WR, Kidd EJ. Functional evaluation of the receptors mediating vasoconstriction of rat aorta by trace amines and amphetamines. Eur J Pharmacol. 2013;715:370–380 [DOI] [PubMed] [Google Scholar]
- 31.Nabaei G, Oveisgharan S, Ghorbani A, Fatehi F. Impaired arterial smooth muscle cell vasodilatory function in methamphetamine users. J Neurol Sci. 2016;370:107–111 [DOI] [PubMed] [Google Scholar]
- 32.Schaiberger PH, Kennedy TC, Miller FC, Gal J, Petty TL. Pulmonary hypertension associated with long-term inhalation of “crank” methamphetamine. Chest. 1993;104:614–616 [DOI] [PubMed] [Google Scholar]
- 33.Chin KM, Channick RN, Rubin LJ. Is methamphetamine use associated with idiopathic pulmonary arterial hypertension? Chest. 2006;130:1657–1663 [DOI] [PubMed] [Google Scholar]
- 34.Orcholski ME, Khurshudyan A, Shamskhou EA, Yuan K, Chen IY, Kodani SD, Morisseau C, Hammock BD, Hong EM, Alexandrova L, Alastalo TP, Berry G, Zamanian RT, de Jesus Perez VA. Reduced carboxylesterase 1 is associated with endothelial injury in methamphetamine-induced pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol. 2017;313:L252–L266 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Volkow ND, Fowler JS, Wang GJ, Shumay E, Telang F, Thanos PK, Alexoff D. Distribution and pharmacokinetics of methamphetamine in the human body: Clinical implications. PLoS One. 2010;5:e15269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Chen PI, Cao A, Miyagawa K, Tojais NF, Hennigs JK, Li CG, Sweeney NM, Inglis AS, Wang L, Li D, Ye M, Feldman BJ, Rabinovitch M. Amphetamines promote mitochondrial dysfunction and DNA damage in pulmonary hypertension. JCI Insight. 2017;2:e90427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zheng T, Liu L, Shi J, Yu X, Xiao W, Sun R, Zhou Y, Aa J, Wang G. The metabolic impact of methamphetamine on the systemic metabolism of rats and potential markers of methamphetamine abuse. Mol Biosyst. 2014;10:1968–1977 [DOI] [PubMed] [Google Scholar]
- 38.Nopparat C, Porter JE, Ebadi M, Govitrapong P. The mechanism for the neuroprotective effect of melatonin against methamphetamine-induced autophagy. J Pineal Res. 2010;49:382–389 [DOI] [PubMed] [Google Scholar]
- 39.Ma J, Wan J, Meng J, Banerjee S, Ramakrishnan S, Roy S. Methamphetamine induces autophagy as a pro-survival response against apoptotic endothelial cell death through the kappa opioid receptor. Cell Death Dis. 2014;5:e1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Karch SB, Stephens BG, Ho CH. Methamphetamine-related deaths in san francisco: Demographic, pathologic, and toxicologic profiles. J Forensic Sci. 1999;44:359–368 [PubMed] [Google Scholar]
- 41.Kaye S, Darke S, Duflou J, McKetin R. Methamphetamine-related fatalities in australia: Demographics, circumstances, toxicology and major organ pathology. Addiction. 2008;103:1353–1360 [DOI] [PubMed] [Google Scholar]
- 42.Gao B, Li L, Zhu P, Zhang M, Hou L, Sun Y, Liu X, Peng X, Gu Y. Chronic administration of methamphetamine promotes atherosclerosis formation in apoe−/− knockout mice fed normal diet. Atherosclerosis. 2015;243:268–277 [DOI] [PubMed] [Google Scholar]
- 43.Zhu P, Li L, Gao B, Zhang M, Wang Y, Gu Y, Hu L. Impact of chronic methamphetamine treatment on the atherosclerosis formation in apoe−/− mice fed a high cholesterol diet. Oncotarget. 2017;8:55064–55072 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Vozenilek AE, Navratil AR, Green JM, Coleman DT, Blackburn CMR, Finney AC, Pearson BH, Chrast R, Finck BN, Klein RL, Orr AW, Woolard MD. Macrophage-associated lipin-1 enzymatic activity contributes to modified low-density lipoprotein-induced proinflammatory signaling and atherosclerosis. Arterioscler Thromb Vasc Biol. 2018;38:324–334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lee YW, Hennig B, Yao J, Toborek M. Methamphetamine induces ap-1 and nf-kappab binding and transactivation in human brain endothelial cells. J Neurosci Res. 2001;66:583–591 [DOI] [PubMed] [Google Scholar]
- 46.Ramirez SH, Potula R, Fan S, Eidem T, Papugani A, Reichenbach N, Dykstra H, Weksler BB, Romero IA, Couraud PO, Persidsky Y. Methamphetamine disrupts blood-brain barrier function by induction of oxidative stress in brain endothelial cells. J Cereb Blood Flow Metab. 2009;29:1933–1945 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hansson GK, Libby P, Schonbeck U, Yan ZQ. Innate and adaptive immunity in the pathogenesis of atherosclerosis. Circ Res. 2002;91:281–291 [DOI] [PubMed] [Google Scholar]
- 48.Potula R, Hawkins BJ, Cenna JM, Fan S, Dykstra H, Ramirez SH, Morsey B, Brodie MR, Persidsky Y. Methamphetamine causes mitrochondrial oxidative damage in human t lymphocytes leading to functional impairment. J Immunol. 2010;185:2867–2876 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Parekh JD, Jani V, Patel U, Aggarwal G, Thandra A, Arora R. Methamphetamine use is associated with increased risk of stroke and sudden cardiac death: Analysis of the nationwide inpatient sample database. JACC Cardiovasc. Interv. 2018;11:S29 [Google Scholar]
- 50.Darke S, Kaye S, Duflou J. Rates, characteristics and circumstances of methamphetamine-related death in australia: A national 7-year study. Addiction. 2017;112:2191–2201 [DOI] [PubMed] [Google Scholar]
- 51.Li J, Li J, Chen Y, Xu Y, Li W, Chen Y, Cui K. Methamphetamine use associated with monomorphic ventricular tachycardia. J Addict Med. 2014;8:470–473 [DOI] [PubMed] [Google Scholar]
- 52.Haning W, Goebert D. Electrocardiographic abnormalities in methamphetamine abusers. Addiction. 2007;102 Suppl 1:70–75 [DOI] [PubMed] [Google Scholar]
- 53.Dawes DM, Ho JD, Cole JB, Reardon RF, Lundin EJ, Terwey KS, Falvey DG, Miner JR. Effect of an electronic control device exposure on a methamphetamine-intoxicated animal model. Acad Emerg Med. 2010;17:436–443 [DOI] [PubMed] [Google Scholar]
- 54.Pujol-Lopez M, Ortega-Paz L, Flores-Umanzor EJ, Perea RJ, Bosch X. Cardiac magnetic resonance as an alternative to endomyocardial biopsy to predict recoverability of left ventricular function in methamphetamine- associated cardiomyopathy. JACC Heart Fail. 2017;5:853–854 [DOI] [PubMed] [Google Scholar]
- 55.Schurer S, Klingel K, Sandri M, Majunke N, Besler C, Kandolf R, Lurz P, Luck M, Hertel P, Schuler G, Linke A, Mangner N. Clinical characteristics, histopathological features, and clinical outcome of methamphetamine-associated cardiomyopathy. JACC Heart Fail. 2017;5:435–445 [DOI] [PubMed] [Google Scholar]
- 56.Qu YH, Leung KP, Qiao DF, Li DR, Liu C, Yue X, Wang HJ. Remodeling of ion channel expression may contribute to electrophysiological consequences caused by methamphetamine in vitro and in vivo. Biochem Biophys Res Commun. 2014;443:441–446 [DOI] [PubMed] [Google Scholar]
- 57.Liang R, Zhou Y, Wu F, Zhou C, Zhao X, Zhang M, Tian X, Zhu B. Effect of methamphetamine on potassium and l-type calcium currents in rat ventricular myocytes. Toxicol Mech Methods. 2010;20:458–465 [DOI] [PubMed] [Google Scholar]
- 58.Sugimoto K, Okamura K, Tanaka H, Takashima S, Ochi H, Yamamoto T, Matoba R. Methamphetamine directly accelerates beating rate in cardiomyocytes by increasing ca(2+) entry via l-type ca(2+) channel. Biochem Biophys Res Commun. 2009;390:1214–1220 [DOI] [PubMed] [Google Scholar]
- 59.Richards JR, Harms BN, Kelly A, Turnipseed SD. Methamphetamine use and heart failure: Prevalence, risk factors, and predictors. Am J Emerg Med. 2018;36:1423–1428 [DOI] [PubMed] [Google Scholar]
- 60.Zhao SX, Kwong C, Swaminathan A, Gohil A, Crawford MH. Clinical characteristics and outcome of methamphetamine-associated pulmonary arterial hypertension and dilated cardiomyopathy. JACC Heart Fail. 2018;6:209–218 [DOI] [PubMed] [Google Scholar]
- 61.Wijetunga M, Seto T, Lindsay J, Schatz I. Crystal methamphetamine-associated cardiomyopathy: Tip of the iceberg? J Toxicol Clin Toxicol. 2003;41:981–986 [DOI] [PubMed] [Google Scholar]
- 62.He SY, Matoba R, Fujitani N, Sodesaki K, Onishi S. Cardiac muscle lesions associated with chronic administration of methamphetamine in rats. Am J Forensic Med Pathol. 1996;17:155–162 [DOI] [PubMed] [Google Scholar]
- 63.Maeno Y, Iwasa M, Inoue H, Koyama H, Matoba R, Nagao M. Direct effects of methamphetamine on hypertrophy and microtubules in cultured adult rat ventricular myocytes. Forensic Sci Int. 2000;113:239–243 [DOI] [PubMed] [Google Scholar]
- 64.Turdi S, Schamber RM, Roe ND, Chew HG Jr., Culver B, Ren J. Acute methamphetamine exposure inhibits cardiac contractile function. Toxicol Lett. 2009;189:152–158 [DOI] [PMC free article] [PubMed] [Google Scholar]