

Abstract
Context
Although fatigue has been implicated in anterior cruciate ligament (ACL) injury, few researchers have examined the timing of injury across a competitive sport season or within a competitive session to gain insight into the potential effects of fatigue on the incidence of ACL injury.
Objective
To identify the time segments across a competitive season or within an individual competition associated with the greatest ACL injury incidence.
Design
Descriptive epidemiology study.
Methods
Data from the National Collegiate Athletic Association Injury Surveillance Program for 2004–2005 through 2015–2016 for basketball, lacrosse, and soccer were analyzed. Incidence rate ratios (IRRs) compared ACL injury rates by sport, sex, season segment, and competition period. Poisson regression was used to examine the associations between each of these categories and the incidence of ACL injury as well as interaction effects.
Results
During the early regular season, the incidence rate was elevated relative to the preseason (IRR = 1.86; 95% confidence interval [CI] = 1.27, 2.74), middle regular season (IRR = 1.48; 95% CI = 1.01, 2.15), late regular season (IRR = 1.56; 95% CI = 1.08, 2.27), and postseason (IRR = 2.20; 95% CI = 1.06, 4.56). A sport-by-season interaction indicated this effect was largely attributable to a higher incidence in the early season among lacrosse athletes. An interaction between season segment and competition period (P = .02) revealed a greater injury incidence before halftime in the early regular season (IRR = 0.38, 95% CI = 0.19, 0.76), but a greater incidence after halftime in the late regular season (IRR = 2.40, 95% CI = 1.15, 5.02). Fewer noncontact injuries occurred in soccer than in basketball or lacrosse.
Conclusions
The ACL injury incidence was higher in the early part of the regular season, particularly among lacrosse athletes. Although the injury incidences before and after halftime were similar, further analyses of player time and time of injury within each half are necessary. Coaches and practitioners should be cognizant of the elevated injury incidence during the early season among lacrosse athletes. Future authors should consider more specific analyses to further elucidate the potential role of fatigue development in exacerbating the incidence of ACL injury in collegiate athletes both within games and across the season.
Keywords: injury epidemiology, athletic injuries, knee injuries, basketball, lacrosse, soccer
Key Points
The anterior cruciate ligament (ACL) injury rate was highest during the earliest part of the collegiate regular season, an effect that was most prominent among lacrosse players.
The ACL injury incidence before halftime was greater during the early regular season but greater after halftime during the late regular season.
Future studies are needed to assess the role of appropriate season periodization in ACL injury and elucidate more precisely the timing of injuries during competitions.
Anterior cruciate ligament (ACL) injury presents a significant burden to athletes. This is especially true in the collegiate athletic environment because of limited time for recovery, the narrow schedule of competitions, and potential effects on athletic scholarships. The greater incidence of ACL injuries in female athletes compared with their male counterparts is well documented1,2 and has been attributed to multiple factors, including differences in hormonal profiles, joint laxity, neuromuscular activation, and anatomy. Much research has been conducted to examine the mechanisms and risk factors for ACL injury,3 and many intervention programs have been designed and implemented in the collegiate sports environment to reduce the risk associated with 1 or more of these factors.4 Despite these prevention efforts, the incidence rate of ACL injury has decreased only slightly in male athletes and has not shown any significant reduction in female athletes.5,6 It is therefore reasonable to conclude that further refinement of our injury-assessment and injury-prevention strategies is warranted, as well as additional identification of risk factors that will further inform our prevention strategies.
One such component that must be considered in the injury-risk equation is the effect of both acute and long-term physical exertion on the athlete. Strenuous, sustained physical exertion is known to result in diminished task performance and place an individual at a higher risk of injury. Although the effects of fatigue on biomechanics are variable,7 it is well accepted that fatigue affects lower limb kinematics and is likely context specific. From an acute standpoint, leg stiffness,8 knee abduction,9 knee internal rotation,9 knee kinetics,10 anterior tibial translation,11,12 and multivariate knee-joint biomechanics13 were each influenced by single sessions of fatiguing exercise because of reductions in both passive and active joint stabilization, and these factors tend to be more prominent in females than in males.9,13,14 The alterations in lower limb kinematics and kinetics associated with landing15–19 and cutting 19–21 tasks when fatigued are particularly problematic: these activities are high-risk maneuvers in relation to ACL injury and are prominent in sports such as basketball, lacrosse, and soccer. Although reduced passive stabilization (ie, increased joint laxity) and concomitant changes in biomechanics have been observed in the first 15 to 20 minutes of exercise,22 fatigue-related changes typically occur later in response to exercise that is high intensity or of longer duration. Fatigue- and laxity-related changes in biomechanics have been reported to be more pronounced in females (and compound one another),13 and these combined factors may place females at even greater risk later in a game or practice.
In addition to these acute exercise effects, more prolonged or long-term exertion over the course of a season may also play a role in compromising knee stability, leading to an increased incidence of ACL injury. Because fatigued athletes have demonstrated reduced isometric and concentric muscular activation,23,24 muscular strength,25 neuromuscular reflexive function,26 and neuromuscular excitability,27 they may be at a heightened risk of injury. Moreover, increasing evidence indicates that ACL failure may not be the result of a 1-time event but rather may result from cumulative loading over time,28,29 which could increase if dynamic stabilization is compromised because of fatigue.
This study represents a first step toward understanding the acute and long-term effects of exertion on the risk of ACL injury. Therefore, the purpose of our analysis was to determine whether a higher incidence of ACL injuries occurred among National Collegiate Athletic Association (NCAA) student-athletes during later periods in a season or competition compared with earlier periods. First, we hypothesized that the injury incidence would be elevated during the preseason and early-season segments and the late and postseason segments. Second, we proposed that ACL injuries would occur with greater frequency during the second half of a game or competition compared with the first, when athletes were presumably in a fatigued state. We also hypothesized that these acute and long-term effects would interact, such that the acute effects of fatigue would be exaggerated as the season progressed. Based on previous research that indicated biomechanics among females were affected to a greater degree after fatiguing exercise,14 we suggested that both the acute and long-term effects of fatigue would differentially affect the injury incidence in female athletes. It was unclear whether sport would interact with acute or chronic injury incidence and, thus, these analyses were primarily exploratory.
METHODS
Analyses were based on 2 data sets (spanning 2004–2005 through 2008–2009 and 2009–2010 through 2015–2016) from the NCAA Injury Surveillance Program (ISP), a prospective injury-surveillance program managed by the Datalys Center for Sports Research and Prevention, Inc (Indianapolis, IN). Data were requested for both men's and women's sports with the highest ACL injury rates and for sports that were similar in athletic requirements between men and women: basketball, lacrosse, and soccer. The NCAA ISP data-collection protocol has been previously detailed.30 In brief, athletic trainers (ATs) at all participating NCAA institutions were asked to complete a detailed report on each injury or condition, including related circumstances, mechanism (eg, contact, noncontact), event type, and time in game and season. The ATs also documented exposure information for varsity-level practices (including team conditioning sessions) and competitions, including the activity type and number of athletes present. Injuries incurred during individual weight-lifting and conditioning sessions or off-season training were not included. We chose to analyze ACL injuries from all mechanisms because we were primarily concerned with the possible effect of exertional duration on injury. Considering that a key implication of fatigue on injury risk is a reduced ability to react to potential contact,12 fatigue would presumably increase the risk of both contact and noncontact injuries.
Although the 2 data sets were built using different data-collection methods,30 because of the severity and nature of ACL injuries, we determined that they could be combined to increase the sample size and robustness of the analyses. As such, although the 2009–2010 through 2015–2016 data included non–time-loss injuries, we analyzed only ACL injuries resulting in time loss of at least 24 hours of training or competition to allow for consistent injury definitions in the data sets. In the present analysis, ACL injury was defined as either a partial or complete tear of the ACL, regardless of whether the injury resulted in surgical intervention, as coded by the presiding AT.
Season segment was split into preseason, defined as all formal team practices and exhibition games conducted before the first regular season contest; regular season, defined as all practices and competitions from the first regular season competition through the last regular season competition; and postseason, defined as all practices and competitions after the last regular season competition through the last postseason competition. To further assess specific periods of the season, the regular season was split into thirds (early, middle, and late) based on average regular season length (days) for each division for each sport, and 5 segments were subsequently analyzed: preseason, the 3 segments in the regular season, and postseason. However, because injury and exposure dates were not available for the older data set, this more detailed analysis of season segment was limited to the more recent dataset (2009–2010 through 2015–2016). Session period was limited to games (injury incidence by time within practice was not recorded), and was split among before halftime and halftime or later. Notably, athlete-exposures (AEs) were recorded per competition and thus not individually coded by specific competition segment. Further breakdown of competition segments was not available.
Data were analyzed using SAS-Enterprise Guide software (version 7.1; SAS Institute Inc, Cary, NC). Injury rates per 10 000 AEs and 95% confidence intervals (CIs) were calculated. Incidence rate ratios (IRRs) compared ACL injury rates by sport, sex, mechanism of injury, season segment, and competition segment. Poisson regression of injury counts with AEs as the offset variable were used to examine the association between each category and ACL injury, as well as interactions of sport with season segment and competition segment; sex with season segment and competition segment; and season segment with competition segment. Sensitivity analyses that controlled for NCAA division and year were completed but not included in the results because the findings were consistent with the original analyses. All analyses were performed for all ACL injuries resulting in ≥24 hours of time lost, with additional analyses of only those reported as occurring from a noncontact mechanism. To determine the presence of a statistical interaction, the likelihood ratio χ2 value for the interaction term in the type 3 test of the Poisson regression was used. All significance tests were 2 sided, and P values < .05 were considered statistically significant.
RESULTS
From the combined data set (2004–2005 through 2015–2016), 529 ACL injuries resulting in at least 1 day of training or competition loss were reported, 320 (60%) of which were deemed noncontact injuries (Table 1). Females accounted for 357 ACL injuries (67%) and 222 noncontact injuries (69%). The injury rate was higher among females than males, both for all injuries (IRR = 2.18; 95% CI = 1.82, 2.61; P < .0001) and for noncontact injuries (IRR = 2.38; 95% CI = 1.87, 3.10; P < .0001). Among all ACL injuries, 264 (50%) were in basketball players (rate per 10 000 AEs = 1.34; 95% CI = 1.18, 1.52), 129 (24%) were in lacrosse athletes (rate per 10 000 AEs = 1.55; 95% CI = 1.31, 1.85), and 136 (26%; rate per 10 000 AEs = 0.75; 95% CI = 0.63, 0.89) were in soccer players (Table 1). There was no sex-by-sport interaction. When sex was controlled, the injury rate for soccer was lower than for basketball (IRR = 0.56; 95% CI = 0.46, 0.69; P < .0001) or lacrosse (IRR = 0.48; 95% CI = 0.38, 0.62; P < .0001) for all ACL injuries. A total of 172 noncontact injuries occurred in basketball (54%; rate per 10 000 AEs = 0.86; 95% CI = 0.73, 1.00), 91 in lacrosse (28%; rate per 10 000 AEs = 1.08; 95% CI = 0.87, 1.33), and 57 in soccer (18%; rate per 10 000 AEs = 0.31; 95% CI = 0.24, 0.40). The same trend held for noncontact ACL injuries: injury rates were again lower for soccer compared with basketball (IRR = 0.36; 95% CI = 0.27, 0.48; P < .0001) or lacrosse (IRR = 0.28; 95% CI = 0.20, 0.40; P < .0001).
Table 1.
All and Noncontact Anterior Cruciate Ligament Injuries by Sport and Sex
| Sport |
Males |
Females |
||||
| No. |
AEs |
Rate per 10 000 AEs (95% CI) |
No. |
AEs |
Rate per 10 000 AEs (95% CI) |
|
| All injuries | ||||||
| Basketball | 79 | 986 873 | 0.80 (0.62, 0.98) | 185 | 872 331 | 2.12 (1.82, 2.43) |
| Lacrosse | 59 | 457 123 | 1.29 (0.96, 1.62) | 70 | 349 310 | 2.00 (1.53, 2.47) |
| Soccer | 34 | 748 638 | 0.45 (0.30, 0.61) | 102 | 868 499 | 1.17 (0.95, 1.40) |
| All | 172 | 2 192 634 | 0.78 (0.67, 0.90) | 357 | 2 090 141 | 1.71 (1.53, 1.89) |
| Noncontact injuries | ||||||
| Basketball | 45 | 986 873 | 0.46 (0.32, 0.59) | 127 | 872 331 | 1.46 (1.20, 1.71) |
| Lacrosse | 41 | 457 123 | 0.90 (0.62, 1.17) | 50 | 349 310 | 1.43 (1.03, 1.83) |
| Soccer | 12 | 748 638 | 0.16 (0.07, 0.25) | 45 | 868 499 | 0.52 (0.37, 0.67) |
| All | 98 | 2 192 634 | 0.45 (0.36, 0.54) | 222 | 2 090 141 | 1.06 (0.92, 1.20) |
Abbreviations: AE, athlete-exposure; CI, confidence interval.
To answer the first research question regarding the effects of long-term exertion on injury incidence, data were analyzed by season segment. As displayed in Table 2, for all ACL injuries in both sexes and all sports, a main effect for season segment was present (P = .005), such that injury rates were higher during the regular season relative to the preseason (IRR = 1.27; 95% CI = 1.04, 1.56), and were lower in the postseason compared with the regular season (IRR = 0.58; 95% CI = 0.36, 0.91). No interaction was evident between season segment and sex (P = .95). When we restricted the analysis to noncontact ACL injuries, patterns were similar (Table 2), with an overall main effect of season; however, the only statistically significant difference was that injury rates were lower during the postseason than the regular season (IRR = 0.51; 95% CI = 0.27, 0.95).
Table 2.
Comparison of All Anterior Cruciate Ligament Injuries by Season Segment and Sex
| Variable |
Preseason |
Regular Season |
Postseason |
Incidence Rate Ratio |
||||||||
| No. |
AEs |
Rate per 10 000 AEs (95% CI) |
No. |
AEs |
Rate per 10 000 AEs (95% CI) |
No. |
AEs |
Rate per 10 000 AEs (95% CI) |
Regular Season Versus Preseason |
Postseason Versus Preseason |
Postseason Versus Regular Season |
|
| All injuries | ||||||||||||
| Males | 39 | 584 216 | 0.67 (0.46, 0.88) | 127 | 1 476 792 | 0.86 (0.71, 1.01) | 6 | 131 626 | 0.46 (0.09, 0.82) | 1.29 (0.90, 1.84) | 0.68 (0.29, 1.61) | 0.53 (0.23, 1.20) |
| Females | 80 | 543 850 | 1.47 (1.15, 1.79) | 264 | 1 432 795 | 1.84 (1.62, 2.06) | 13 | 113 495 | 1.15 (0.52, 1.76) | 1.25 (0.98, 1.61) | 0.78 (0.43, 1.40) | 0.62 (0.36, 1.08) |
| All | 119 | 1 104 451 | 1.05 (0.87, 1.24) | 391 | 2 077 031 | 1.34 (1.21, 1.48) | 19 | 189 005 | 0.78 (0.43, 1.12) | 1.27 (1.04, 1.56)a | 0.73 (0.45, 1.19) | 0.58 (0.36, 0.91)a |
| Noncontact injuries | ||||||||||||
| Males | 23 | 584 216 | 0.39 (0.23, 0.55) | 72 | 1 476 792 | 0.49 (0.37, 0.60) | 3 | 131 626 | 0.23 (0.00, 0.49) | 1.24 (0.77, 1.98) | 0.58 (0.17, 1.93) | 0.47 (0.15, 1.48) |
| Females | 52 | 543 850 | 0.96 (0.70, 1.22) | 163 | 1 432 795 | 1.14 (0.96, 1.31) | 7 | 113 495 | 0.62 (0.16, 1.07) | 1.19 (0.87, 1.63) | 0.65 (0.29, 1.42) | 0.54 (0.25, 1.16) |
| All | 75 | 1 128 066 | 0.66 (0.51, 0.82) | 235 | 2 909 587 | 0.81 (0.70, 0.91) | 10 | 245 121 | 0.41 (0.16, 0.66) | 1.21 (0.94, 1.58) | 0.61 (0.32, 1.19) | 0.51 (0.27, 0.95)a |
Abbreviations: AE, athlete-exposure; CI, confidence interval.
P < .05.
When analyzing season segment by sport (Table 3), a significant interaction was observed (P = .0002; Figure). Injury rates were higher during the regular season than the preseason (IRR = 2.08; 95% CI = 1.35, 3.20; P < .001) and the postseason (IRR = 2.96; 95% CI = 1.09, 8.04; P < .001) in lacrosse. This segment effect pattern in lacrosse was observed when considering all injuries and only noncontact injuries (Table 3), though the P value for the sport-by-season segment interaction was no longer significant when the analysis was restricted to noncontact injuries (P = .11). No significant season segment effects were noted for basketball or soccer. No mechanism (contact versus noncontact)-by-season segment interaction was demonstrated (P = .51).
Table 3.
Comparison of All Anterior Cruciate Ligament Injuries by Season Segment and Sport
| Sport |
Preseason |
Regular Season |
Postseason |
Incidence Rate Ratio |
||||||||
| No. |
AEs |
Rate per 10 000 AEs (95% CI) |
No. |
AEs |
Rate per 10 000 AEs (95% CI) |
No. |
AEs |
Rate per 10 000 AEs (95% CI) |
Regular Season Versus Preseason |
Postseason Versus Preseason |
Regular Season Versus Postseason |
|
| All injuries | ||||||||||||
| Basketball | 62 | 437 920 | 1.42 (1.06, 1.77) | 190 | 1 334 615 | 1.42 (1.22, 1.63) | 12 | 86 669 | 1.38 (0.60, 2.17) | 1.01 (0.75, 1.34) | 0.98 (0.53, 1.81) | 1.03 (0.57, 1.84) |
| Lacrosse | 26 | 264 025 | 0.98 (0.61, 1.36) | 99 | 484 455 | 2.04 (1.64, 2.45) | 4 | 57 953 | 0.69 (0.01, 1.37) | 2.08 (1.35, 3.20)a | 0.70 (0.24, 2.01) | 2.96 (1.09, 8.04)a |
| Soccer | 31 | 426 121 | 0.73 (0.47, 0.98) | 102 | 1 090 517 | 0.94 (0.75, 1.12) | 3 | 100 499 | 0.30 (0.00, 0.64) | 1.29 (0.86, 1.92) | 0.41 (0.13, 1.34) | 3.13 (0.99, 9.88) |
| Noncontact injuries | ||||||||||||
| Basketball | 38 | 437 920 | 0.87 (0.59, 1.14) | 127 | 1 334 615 | 0.95 (0.79, 1.12) | 7 | 86 669 | 0.81 (0.21, 1.41) | 1.10 (0.76, 1.58) | 0.93 (0.42, 2.08) | 1.18 (0.55, 2.52) |
| Lacrosse | 20 | 264 025 | 0.76 (0.43, 1.09) | 69 | 484 455 | 1.42 (1.09, 1.76) | 2 | 57 953 | 0.35 (0.00, 0.82) | 1.88 (1.14, 2.09)a | 0.46 (0.11, 1.95) | 4.13 (1.01, 16.83)a |
| Soccer | 17 | 426 121 | 0.40 (0.23, 0.55) | 39 | 1090 517 | 0.36 (0.25, 0.47) | 1 | 100 499 | 0.10 (0.00, 0.29) | 0.90 (0.51, 1.58) | 0.25 (0.03, 1.87) | 3.59 (0.49, 26.16) |
Abbreviations: AE, athlete-exposure; CI, confidence interval.
P < .05.
Figure.
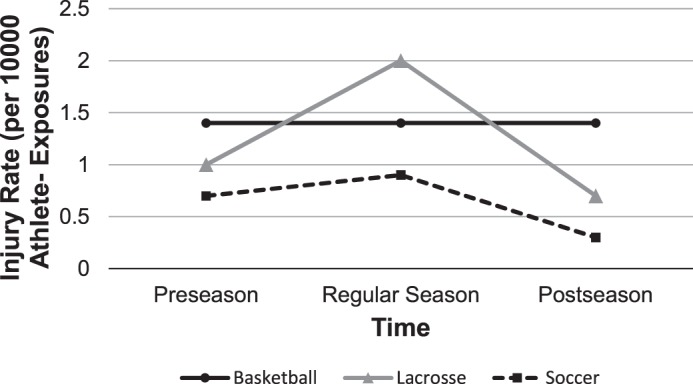
Interaction effect for anterior cruciate ligament injury incidence between season segment and sport.
To further answer the question of whether long-term exertion affected injury incidence, we used the 2009–2010 through 2015–2016 dataset to analyze specific season segments: preseason; early, middle, and late regular season; and postseason segments, collapsed across sex and sport. A significant effect of season segment (Table 4) occurred for all injuries (P = .01) and noncontact injuries only (P = .001). For all ACL injuries, the early regular season injury incidence was elevated relative to the preseason (IRR = 1.86; 95% CI = 1.27, 2.74), middle regular season (IRR = 1.48; 95% CI = 1.01, 2.15), late regular season (IRR = 1.56; 95% CI = 1.08, 2.27), and postseason (IRR = 2.20; 95% CI = 1.06, 4.56). No other differences between season segments were found. In a sensitivity analysis that involved removing lacrosse injuries from the data set, the results were similar. The direction of all effects was the same; however, the magnitude of the rate ratios was slightly attenuated, and the results were no longer significant (Supplemental Table 1 (143KB, pdf) , available online at http://dx.doi.org/10.4085/1062-6050-501-17.S1). Further sensitivity analyses restricted to practices only (Supplemental Table 2 (11.7KB, docx) ) showed a similar trend of elevated injury incidence in the early regular season relative to the middle (IRR = 1.93; 95% CI = 1.02, 3.64) and late regular season (IRR = 2.57; 95% CI = 1.28, 5.14) but not the preseason (IRR = 1.05; 95% CI = 0.65, 1.69) or postseason (IRR = 2.59; 95% CI = 0.79, 8.51).
Table 4.
Anterior Cruciate Ligament Injuries by Season Segmenta
| Variable |
Preseason |
Early Regular Season |
Middle Regular Season |
Late Regular Season |
Postseason |
| All injuries | |||||
| No. | 40 | 72 | 44 | 45 | 8 |
| AEs | 384 573 | 371 705 | 335 182 | 363 227 | 90 771 |
| Rate per 10 000 AEs (95% CI) | 1.04 (0.72, 1.36) | 1.94 (1.49, 2.38) | 1.31 (0.92, 1.70) | 1.24 (0.88, 1.60) | 0.88 (0.27, 1.49) |
| Noncontact | |||||
| No. | 22 | 45 | 20 | 21 | 2 |
| AEs | 384 573 | 371 705 | 335 182 | 363 227 | 90 771 |
| Rate per 10 000 AEs (95% CI) | 0.57 (0.33, 0.81) | 1.21 (0.86, 1.56) | 0.60 (0.34, 0.86) | 0.58 (0.33, 0.83) | 0.22 (0.00, 0.53) |
| All injuries IRR (95% CI) | |||||
| Versus preseason | 1.86 (1.27, 2.74)b | 1.26 (0.82, 1.94) | 1.19 (0.78, 1.82) | 0.85 (0.40, 1.81) | |
| Versus early regular season | – | 0.68 (0.47, 0.99)b | 0.64 (0.44, 0.93)b | 0.45 (0.22, 0.94)b | |
| Versus middle regular season | – | – | 0.94 (0.62, 1.43) | 0.67 (0.32, 1.43) | |
| Versus late regular season | – | – | – | 0.71 (0.34, 1.51) | |
| Noncontact IRR (95% CI) | |||||
| Versus preseason | 2.12 (1.27, 3.52)b | 1.04 (0.57, 1.91) | 1.01 (0.56, 1.84) | 0.39 (0.09, 1.64) | |
| Versus early regular season | – | 0.49 (0.29, 0.83)b | 0.48 (0.28, 0.80)b | 0.18 (0.04, 0.75)b | |
| Versus middle regular season | – | – | 0.97 (0.53, 1.79) | 0.37 (0.09, 1.58) | |
| Versus late regular season | – | – | – | 0.38 (0.09, 1.63) | |
Abbreviations: AE, athlete-exposure; CI, confidence interval; IRR, incidence rate ratio.
Analysis includes a subset of data restricted to 2009–2010 through 2015–2016.
P < .05.
When we analyzed noncontact ACL injuries only, the trend was the same as for all ACL injuries, with the early regular season incidence being elevated relative to the preseason (IRR = 2.12; 95% CI = 1.27, 3.52), middle regular season (IRR = 2.03; 95% CI = 1.20, 3.44), late regular season (IRR = 2.09; 95% CI = 1.25, 3.52), and postseason (IRR = 5.49; 95% CI = 1.33, 22.65). Similarly, for practices only, the early regular season injury incidence was increased relative to the middle regular season (IRR = 2.79; 95% CI = 1.19, 6.56) and late regular season (IRR = 3.41; 95% CI = 1.38, 8.44) but not the preseason (IRR = 1.38; 95% CI = 0.76, 2.51) or postseason (IRR = 2.82; 95% CI = 0.66, 12.01).
To address the second research question regarding the acute exertional effects on the incidence of ACL injury, injury rates by competition segment were analyzed across both sexes and all sports. No differences were observed between before halftime and halftime or later during competitions for all ACL injuries (IRR = 1.05; 95% CI = 0.83, 1.32; P = .68) or noncontact injuries (IRR = 1.01; 95% CI = 0.61, 1.95; P = .94). This finding was confirmed via subanalyses (Table 5), with no significant interactions between game segment and sex (P = .48) or game segment and sport (P = .74). Yet a significant interaction between competition segment and season period for all injuries (P = .02) was present: injuries were fewer after halftime compared with before halftime in the early regular season period (IRR = 0.38; 95% CI = 0.19, 0.76) but greater after halftime in the late regular season period (IRR = 2.40; 95% CI = 1.15, 5.02). The same interaction effect was evident for noncontact ACL injury (P = .03), although only the early regular season showed a reduced injury rate after halftime compared with before halftime (IRR = 0.31; 95% CI = 0.11, 0.85).
Table 5.
Anterior Cruciate Ligament Injury by Competition Period, Sport, Sex, and Season Segmenta
| Variable |
Before Halftime |
Halftime or Later |
Incidence Rate Ratio Versus Before Halftime (95% CI) |
||||
| No. |
AEs |
Rate per 10 000 AEs (95% CI) |
No. |
AEs |
Rate per 10 000 AEs (95% CI) |
||
| All injuries | |||||||
| Sport | |||||||
| Basketball | 72 | 400 589 | 1.80 (1.38, 2.21) | 76 | 400 589 | 1.90 (1.47, 2.32) | 1.06 (0.76, 1.46) |
| Lacrosse | 32 | 138 122 | 2.32 (1.51, 3.12) | 32 | 138 122 | 2.32 (1.51, 3.12) | 1.00 (0.61, 1.63) |
| Soccer | 38 | 373 576 | 1.02 (0.69, 1.34) | 41 | 373 576 | 1.10 (0.76, 1.43) | 1.08 (0.69, 1.68) |
| Sex | |||||||
| Males | 47 | 437 826 | 1.07 (0.77, 1.38) | 44 | 437 826 | 1.00 (0.71, 1.30) | 0.94 (0.62, 1.41) |
| Females | 95 | 474 461 | 2.00 (1.60, 2.40) | 105 | 474 461 | 2.21 (1.79, 2.63) | 1.11 (0.84, 1.46) |
| Season segment | |||||||
| Early regular seasonb | 29 | 108 645 | 2.67 (1.70, 3.64) | 11 | 108 645 | 1.01 (0.41, 1.61) | 0.38 (0.19, 0.76)c |
| Middle regular seasonb | 13 | 90 702 | 1.43 (0.65, 2.21) | 14 | 90 702 | 1.54 (0.73, 2.35) | 1.08 (0.51, 2.29) |
| Late regular seasonb | 10 | 106 679 | 0.94 (0.36, 1.52) | 24 | 106 679 | 2.25 (1.35, 3.15) | 2.40 (1.15, 5.02)c |
| Postseasonb | 3 | 20 176 | 1.49 (0.00, 3.17) | 2 | 20 176 | 0.99 (0.00, 2.37) | 0.67 (0.11, 3.99) |
| Noncontact | |||||||
| Sport | |||||||
| Basketball | 47 | 400 589 | 1.17 (0.84, 1.51) | 50 | 400 589 | 1.25 (0.90, 1.59) | 1.06 (0.71, 1.58) |
| Lacrosse | 23 | 138 122 | 1.67 (0.98, 2.35) | 19 | 138 122 | 1.38 (0.76, 1.99) | 0.83 (0.45, 1.52) |
| Soccer | 12 | 373 576 | 0.32 (0.14, 0.50) | 14 | 373 576 | 0.37 (0.18, 0.57) | 1.17 (0.54, 2.52) |
| Sex | |||||||
| Males | 22 | 437 826 | 0.50 (0.29, 0.71) | 24 | 437 826 | 0.55 (0.33, 0.77) | 1.09 (0.61, 1.95) |
| Females | 60 | 474 461 | 1.26 (0.94, 1.58) | 59 | 474 461 | 1.24 (0.93, 1.56) | 0.98 (0.69, 1.41) |
| Season segment | |||||||
| Early regular seasonb | 16 | 108 645 | 1.47 (0.75, 2.19) | 5 | 108 645 | 0.46 (0.06, 0.86) | 0.31 (0.11, 0.85)c |
| Middle regular seasonb | 6 | 90 702 | 0.66 (0.13, 1.19) | 7 | 90 702 | 0.77 (0.20, 1.34) | 1.17 (0.39, 3.47) |
| Late regular seasonb | 5 | 106 679 | 0.47 (0.06, 0.88) | 10 | 106 679 | 0.94 (0.36, 1.52) | 2.00 (0.68, 5.85) |
| Postseasonb | 0 | 20 176 | 0.00 | 0 | 20 176 | 0.00 | NA |
Abbreviations: AE, athlete-exposure; CI, confidence interval; NA, not available.
Restricted to competition injuries for which the segment that the injury occurred was recorded.
Season-by-competition interactions limited to the subset of data from 2009–2010 through 2015–2016.
P < .05.
DISCUSSION
The purpose of our study was to identify periods during the season or during competitions in which the ACL injury incidence was greatest for basketball, lacrosse, or soccer student-athletes. According to our hypothesis, based on the known effects of acute and long-term exertion on the musculoskeletal system, we believed that ACL injuries would be highest during either the early or late season (long-term fatigue development) and highest in the second half of competition relative to the first, when athletes were more likely to be acutely fatigued. These hypotheses were only partially supported by our analyses. The injury incidence was greatest in the early season segment and reduced late in the season, and although no difference occurred in injury incidence as a result of competition period alone, an interaction effect existed between season segment and competition period. These results also confirmed the well-established elevated incidence of ACL injury among females compared with males.31,32
We observed a season segment effect for all ACL injuries, but our results contrast with our original hypothesis that the injury incidence would be greater later in the season (ie, postseason). Instead, we noted the ACL injury rate was highest during the regular season. This may be a result of the regular season segment's posing a significantly greater load than that for which the athletes have been physically prepared. The reduced incidence of ACL injury during the postseason is a curious finding, as in the fatigue model, one would expect this period to produce the least favorable environment. However, these data may indicate that those athletes who were most vulnerable to ACL injury, through a combination of risk factors including fatigability, may have already sustained an ACL injury earlier in the season. Therefore, the regular season may have acted as a filter of sorts, resulting in the postseason segment's being populated by the more resilient athletes, thereby reducing injury incidence.
When we analyzed the effect of season period on ACL injury incidence in greater detail, the elevated incidence during regular season was attributable to the early regular season segment, and this was largely observed in lacrosse athletes, although a similar nonsignificant pattern also occurred in soccer athletes. As a potential explanation for the increased injury incidence during the early regular season and subsequent decreased incidence in all other season segments, it is reasonable to suggest that the early season acts as a large, acute overload to the system relative to the long-term training history. Although we are unsure why this pattern of elevated early-season injury incidence would be lacrosse specific, one explanation may be the biomechanical requirements of the sport. As has previously been considered,33 lacrosse athletes are in a more at-risk position during play, with a more upright posture and extended knees (approximately 20° of knee flexion). The greater injury incidence during the early-season segment may also be due to factors such as more frequent substitutions during preseason competitions or a larger number of practices incorporating activities with a lower injury risk per AE (ie, technical or tactical training) during the preseason.
Exploratory post hoc sensitivity analyses restricted to injuries sustained during practices showed an elevated incidence in the early season relative to the middle and late season but not the preseason or postseason. The limited number of injuries sustained during practices makes interpretation of this analysis uncertain, yet this finding implicates early-season competitions as the primary factor driving the elevated injuries relative to the preseason. The increased injury incidence during competitions has been documented when considering both all-cause injuries1 and ACL injuries specifically,34 but our analysis suggests that preseason competitions may be distinct from regular season competitions in terms of the ACL injury incidence. We completed further post hoc analyses to assess the interaction between sex and season segment on injury rates and observed no significant interaction. This suggests that although females had an elevated incidence of ACL injury compared with males, the potential effects of fatigue on injury may be equally important for both sexes. However, because of the low injury counts in each category, this analysis was limited by sample size and, thus, definitive conclusions cannot be drawn regarding this interaction.
Many researchers have considered the role of acute fatigue in altered biomechanics and the subsequent injury risk. Nonetheless, we found no differences in ACL injury incidence between the first and second halves of competition. However, an interaction effect was present between competition segment and season period and may in fact point to an effect of fatigue during the early season. Theoretically, those individuals entering a competition in a fatigued state would have only a small amount of fatigue resistance remaining before they reach the threshold for an increased risk of injury. The increased incidence of injury before halftime in the early regular season was observed for both all injuries and noncontact injuries and further confirms this hypothesis. The increased incidence of injury after halftime in the late season points to a potential state of accumulated (long-term) fatigue and subsequent development of acute fatigue during a single competition. These possible explanations are, of course, speculative and require further exploration in future studies that specifically track athlete fatigue across the season and competitions.
The lack of difference among competition segments when considering either sex or sport suggests that acute exertion may not be a primary determinant of injury risk. Prior investigators35 reported that the soccer injury risk was higher in the last 15 minutes of each half and higher during the second half than the first. Our findings are limited to a comparison of the first and second halves of competition, as more detailed analyses within each half were not possible. In addition to fatigue development within a game, other factors may act to heighten the injury risk within a half. First, knee laxity is associated with higher-risk biomechanics and a greater risk of ACL injury (see review by Shultz et al3). During exercise, knee laxity is reported to increase more in females than in males, with these increases and subsequent changes in biomechanics occurring within 15 minutes of exercise22,36 and peaking at the end of the first and second halves of a simulated soccer match. Therefore, the lack of difference between competition segments may be due to greater knee laxity and fatigue toward the end of the period in both segments of play. Second, it is possible a number of the injuries observed affected substitutes, implicating an insufficient warm-up as opposed to fatigue development. Relatedly, an athlete who is sufficiently fatigued may be substituted for because of deficiencies in performance before the neuromuscular system is sufficiently compromised to elevate the injury risk. Anatomical factors associated with the ACL injury risk that do not change acutely as a consequence of exercise intensity or duration (eg, sex-related biomechanics, body mass index, posterior tibial slope, absolute joint laxity37–40) may also explain the lack of session segment effects. Unfortunately, we were unable to isolate a single factor or cluster of causative mechanisms in the present dataset.
Our analyses were subject to certain limitations. First, the NCAA ISP is a voluntary program with a convenience sample and may not represent all NCAA schools and teams. Second, these analyses combined 2 data sets that were collected using different methods; however, the analyses restricted to the 2009–2010 through 2015–2016 data showed similar injury rates by season as those observed in the combined data set, indicating that the 2 data sets were not largely dissimilar in terms of injury rates. Additionally, sensitivity analyses showed that controlling for year or data set did not substantially change the results (data not shown). Even so, a limitation was that our detailed analysis of in-season injury rates was conducted only on the 2009–2010 through 2015–2016 data set. Third, ACL injury is highly influenced by previous ACL injuries,41 including ACL reconstruction, for both the ipsilateral and contralateral limbs.42 Yet we did not distinguish participants based on the number or sequence of previous injuries. Fourth, AEs were reported only at the competition level, rather than the competition segment level. It is therefore unknown if more athletes participated in the first or second half of competitions, which could influence the injury rates. Lastly, the NCAA ISP does not gather information on training periodization or injuries occurring outside of the traditional season or in individual training sessions or captain's practices, so an overall picture of training load could not be examined. Even considering the hypothesized acute and long-term exertional effects, it is conceivable that coaches, strength and conditioning specialists, and ATs are aware of the variability in athlete preparation and physical loads across the season and regulate training loads to manage the increased injury risk.
Future researchers should expand on these findings by monitoring both the external loads imposed on athletes and their response to this training (the so-called internal load) and the association with injury incidence throughout the season. These findings should also be expanded to include other musculoskeletal injuries such as ankle injury, muscular tears, and tendinitis. In addition, our results should be confirmed in non-NCAA sports environments such as professional or Olympic training centers, as well as among high school athletes, who have vastly different training and competition structures.
CONCLUSIONS
These findings suggest that the incidence of ACL injury was elevated during the regular season, particularly during the early regular season segment. Moreover, this increased incidence seemed to disproportionally affect lacrosse athletes. Total load management during both the preseason and early-season periods may assist in mediating this potential risk. Further investigation, including intervention studies of training loads as well as more precise analyses of exercise duration within a session, is needed to confirm these hypotheses and results. The effect of periodization on injury incidence should also be considered.
Supplementary Material
SUPPLEMENTAL MATERIAL
Supplemental Tables. All injuries (excluding lacrosse) by sex and season segment; Anterior cruciate ligament injury by specific segment restricted to practices only.
Found at DOI: http://dx.doi.org/10.4085/1062-6050-501-17.S1
REFERENCES
- 1.Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42(2):311–319. [PMC free article] [PubMed] [Google Scholar]
- 2.Prodromos CC, Han Y, Rogowski J, Joyce B, Shi K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury–reduction regimen. Arthroscopy. 2007;23(12):1320–1325. doi: 10.1016/j.arthro.2007.07.003. [DOI] [PubMed] [Google Scholar]
- 3.Shultz SJ, Schmitz RJ, Benjaminse A, Collins M, Ford K, Kulas AS. ACL Research Retreat VII: an update on anterior cruciate ligament injury risk factor identification, screening, and prevention: March 19–21, 2015; Greensboro, NC. J Athl Train. 2015;50(10):1076–1093. doi: 10.4085/1062-6050-50.10.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gagnier JJ, Morgenstern H, Chess L. Interventions designed to prevent anterior cruciate ligament injuries in adolescents and adults: a systematic review and meta-analysis. Am J Sports Med. 2013;41(8):1952–1962. doi: 10.1177/0363546512458227. [DOI] [PubMed] [Google Scholar]
- 5.Agel J, Rockwood T, Klossner D. Collegiate ACL injury rates across 15 sports: National Collegiate Athletic Association Injury Surveillance System data update (2004–2005 through 2012–2013) Clin J Sport Med. 2016;26(6):518–523. doi: 10.1097/JSM.0000000000000290. [DOI] [PubMed] [Google Scholar]
- 6.Sanders TL, Maradit Kremers H, Bryan AJ, et al. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med. 2016;44(6):1502–1507. doi: 10.1177/0363546516629944. [DOI] [PubMed] [Google Scholar]
- 7.Barber-Westin SD, Noyes FR. Effect of fatigue protocols on lower limb neuromuscular function and implications for anterior cruciate ligament injury prevention training: a systematic review. Am J Sports Med. 2017;45(14):3388–3396. doi: 10.1177/0363546517693846. [DOI] [PubMed] [Google Scholar]
- 8.Lehnert M. De Ste Croix M, Zaatar A, Hughes J, Varekova R, Lastovicka O. Muscular and neuromuscular control following soccer-specific exercise in male youth: changes in injury risk mechanisms. Scand J Med Sci Sports. 2017;27(9):975–982. doi: 10.1111/sms.12705. [DOI] [PubMed] [Google Scholar]
- 9.McLean SG, Fellin RE, Suedekum N, Calabrese G, Passerallo A, Joy S. Impact of fatigue on gender-based high-risk landing strategies. Med Sci Sports Exerc. 2007;39(3):502–514. doi: 10.1249/mss.0b013e3180d47f0. [DOI] [PubMed] [Google Scholar]
- 10.O'Connor KM, Johnson C, Benson LC. The effect of isolated hamstrings fatigue on landing and cutting mechanics. J Appl Biomech. 2015;31(4):211–220. doi: 10.1123/jab.2014-0098. [DOI] [PubMed] [Google Scholar]
- 11.Schmitz RJ, Kim H, Shultz SJ. Neuromuscular fatigue and tibiofemoral joint biomechanics when transitioning from non–weight bearing to weight bearing. J Athl Train. 2015;50(1):23–29. doi: 10.4085/1062-6050-49.3.79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wojtys EM, Wylie BB, Huston LJ. The effects of muscle fatigue on neuromuscular function and anterior tibial translation in healthy knees. Am J Sports Med. 1996;24(5):615–621. doi: 10.1177/036354659602400509. [DOI] [PubMed] [Google Scholar]
- 13.Shultz SJ, Schmitz RJ, Cone JR, et al. Changes in fatigue, multiplanar knee laxity, and landing biomechanics during intermittent exercise. J Athl Train. 2015;50(5):486–497. doi: 10.4085/1062-6050-49.5.08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kernozek TW, Torry MR, Iwasaki M. Gender differences in lower extremity landing mechanics caused by neuromuscular fatigue. Am J Sports Med. 2008;36(3):554–565. doi: 10.1177/0363546507308934. [DOI] [PubMed] [Google Scholar]
- 15.Borotikar BS, Newcomer R, Koppes R, McLean SG. Combined effects of fatigue and decision making on female lower limb landing postures: central and peripheral contributions to ACL injury risk. Clin Biomech (Bristol, Avon) 2008;23(1):81–92. doi: 10.1016/j.clinbiomech.2007.08.008. [DOI] [PubMed] [Google Scholar]
- 16.Dickin DC, Johann E, Wang H, Popp JK. Combined effects of drop height and fatigue on landing mechanics in active females. J Appl Biomech. 2015;31(4):237–243. doi: 10.1123/jab.2014-0190. [DOI] [PubMed] [Google Scholar]
- 17.Gehring D, Melnyk M, Gollhofer A. Gender and fatigue have influence on knee joint control strategies during landing. Clin Biomech (Bristol, Avon) 2009;24(1):82–87. doi: 10.1016/j.clinbiomech.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 18.McLean SG, Samorezov JE. Fatigue-induced ACL injury risk stems from a degradation in central control. Med Sci Sports Exerc. 2009;41(8):1661–1672. doi: 10.1249/MSS.0b013e31819ca07b. [DOI] [PubMed] [Google Scholar]
- 19.Qu X, Jiang J, Hu X. Effects of subsensory noise and fatigue on knee landing and cross-over cutting biomechanics in male athletes. J Appl Biomech. 2018;34(3):205–210. doi: 10.1123/jab.2017-0180. [DOI] [PubMed] [Google Scholar]
- 20.Collins JD, Almonroeder TG, Ebersole KT, O'Connor KM. The effects of fatigue and anticipation on the mechanics of the knee during cutting in female athletes. Clin Biomech (Bristol, Avon) 2016;35:62–67. doi: 10.1016/j.clinbiomech.2016.04.004. [DOI] [PubMed] [Google Scholar]
- 21.Lucci S, Cortes N, Van Lunen B, Ringleb S, Onate J. Knee and hip sagittal and transverse plane changes after two fatigue protocols. J Sci Med Sport. 2011;14(5):453–459. doi: 10.1016/j.jsams.2011.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shultz SJ, Schmitz RJ, Cone JR, et al. Multiplanar knee laxity increases during a 90-min intermittent exercise protocol. Med Sci Sports Exerc. 2013;45(8):1553–1561. doi: 10.1249/MSS.0b013e31828cb94e. [DOI] [PubMed] [Google Scholar]
- 23.Koutedakis Y, Frischknecht R, Budgett R, Vrbova G, Sharp N. Impaired voluntary force production of quadriceps muscle in overtrained subjects. J Physiol. 1993;459:151P. [Google Scholar]
- 24.Koutedakis Y, Frischknecht R, Vrbová G, Sharp N, Budgett R. Maximal voluntary quadriceps strength patterns in Olympic overtrained athletes. Med Sci Sports Exerc. 1995;27(4):566–572. [PubMed] [Google Scholar]
- 25.Fry AC, Kraemer WJ, Ramsey LT. Pituitary-adrenal-gonadal responses to high-intensity resistance exercise overtraining. J Appl Physiol (1985) 1998;85(6):2352–2359. doi: 10.1152/jappl.1998.85.6.2352. [DOI] [PubMed] [Google Scholar]
- 26.Raglin JS, Koceja DM, Stager JM, Harms CA. Mood, neuromuscular function, and performance during training in female swimmers. Med Sci Sports Exerc. 1996;28(3):372–377. doi: 10.1097/00005768-199603000-00013. [DOI] [PubMed] [Google Scholar]
- 27.Lehmann M, Jakob E, Gastmann U, Steinacker JM, Keul J. Unaccustomed high mileage compared to intensity training-related neuromuscular excitability in distance runners. Eur J Appl Physiol Occup Physiol. 1995;70(5):457–461. doi: 10.1007/BF00618498. [DOI] [PubMed] [Google Scholar]
- 28.Lipps DB, Wojtys EM, Ashton-Miller JA. Anterior cruciate ligament fatigue failures in knees subjected to repeated simulated pivot landings. Am J Sports Med. 2013;41(5):1058–1066. doi: 10.1177/0363546513477836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Beaulieu ML, Wojtys EM, Ashton-Miller JA. Risk of anterior cruciate ligament fatigue failure is increased by limited internal femoral rotation during in vitro repeated pivot landings. Am J Sports Med. 2015;43(9):2233–2241. doi: 10.1177/0363546515589164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kerr ZY, Dompier TP, Snook EM, et al. National Collegiate Athletic Association Injury Surveillance System: review of methods for 2004–2005 through 2013–2014 data collection. J Athl Train. 2014;49(4):552–560. doi: 10.4085/1062-6050-49.3.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Agel J, Arendt EA, Bershadsky B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer: a 13-year review. Am J Sports Med. 2005;33(4):524–530. doi: 10.1177/0363546504269937. [DOI] [PubMed] [Google Scholar]
- 32.Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med. 1995;23(6):694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- 33.Braun HJ, Shultz R, Malone M, Leatherwood WE, Silder A, Dragoo JL. Differences in ACL biomechanical risk factors between field hockey and lacrosse female athletes. Knee Surg Sports Traumatol Arthrosc. 2015;23(4):1065–1070. doi: 10.1007/s00167-014-2873-0. [DOI] [PubMed] [Google Scholar]
- 34.Dragoo JL, Braun HJ, Durham JL, Chen MR, Harris AH. Incidence and risk factors for injuries to the anterior cruciate ligament in National Collegiate Athletic Association football: data from the 2004–2005 through 2008–2009 National Collegiate Athletic Association Injury Surveillance System. Am J Sports Med. 2012;40(5):990–995. doi: 10.1177/0363546512442336. [DOI] [PubMed] [Google Scholar]
- 35.Hawkins RD, Hulse MA, Wilkinson C, Hodson A, Gibson M. The association football medical research programme: an audit of injuries in professional football. Br J Sports Med. 2001;35(1):43–47. doi: 10.1136/bjsm.35.1.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Pollard CD, Braun B, Hamill J. Influence of gender, estrogen and exercise on anterior knee laxity. Clin Biomech (Bristol, Avon) 2006;21(10):1060–1066. doi: 10.1016/j.clinbiomech.2006.07.002. [DOI] [PubMed] [Google Scholar]
- 37.Bojicic KM, Beaulieu ML, Imaizumi Krieger DY, Ashton-Miller JA, Wojtys EM. Association between lateral posterior tibial slope, body mass index, and ACL injury risk. Orthop J Sports Med. 2017;5(2):2325967116688664. doi: 10.1177/2325967116688664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Uhorchak JM, Scoville CR, Williams GN, Arciero RA, Pierre PS, Taylor DC. Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 West Point cadets. Am J Sports Med. 2003;31(6):831–842. doi: 10.1177/03635465030310061801. [DOI] [PubMed] [Google Scholar]
- 39.Vacek PM, Slauterbeck JR, Tourville TW, et al. Multivariate analysis of the risk factors for first-time noncontact ACL injury in high school and college athletes: a prospective cohort study with a nested, matched case-control analysis. Am J Sports Med. 2016;44(6):1492–1501. doi: 10.1177/0363546516634682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Carson DW, Ford KR. Sex differences in knee abduction during landing: a systematic review. Sports Health. 2011;3(4):373–382. doi: 10.1177/1941738111410180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Orchard J, Seward H, McGivern J, Hood S. Intrinsic and extrinsic risk factors for anterior cruciate ligament injury in Australian footballers. Am J Sports Med. 2001;29(2):196–200. doi: 10.1177/03635465010290021301. [DOI] [PubMed] [Google Scholar]
- 42.Wright RW, Magnussen RA, Dunn WR, Spindler KP. Ipsilateral graft and contralateral ACL rupture at five years or more following ACL reconstruction: a systematic review. J Bone Joint Surg Am. 2011;93(12):1159–1165. doi: 10.2106/JBJS.J.00898. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.