

Abstract
Previous research suggests that social relations are associated with age-related memory change. However, social relations are complex and multidimensional, and it is not yet clear which aspects (structure, quality) may be beneficial over time. Further, the strength and direction of associations may differ depending on relationship type (partner, children, other family, friends). Using longitudinal data from the Health and Retirement Study (n = 10,390; Mage = 69, SD = 9.53 at baseline), latent growth curve models tested which aspects of social relations predicted 6-year episodic memory trajectories. Both structure and quality of social relations were associated with initial memory level, such that being married/partnered, reporting more frequent contact with children and friends, reporting less support from family members other than partners and children, and reporting less strain across relationship types, were each independently associated with better initial memory. In contrast, only structure was associated with subsequent memory decline. Specifically, being married/partnered and reporting more frequent contact with friends were each independently associated with slower memory decline. No evidence of bidirectionality was found, as baseline memory did not predict subsequent changes in social relations. This longitudinal study helps to clarify which aspects of social relations are most likely to influence late-life episodic memory trajectories. Future intervention studies may focus on increasing social interactions with non-family members to minimize memory decline with age.
Keywords: episodic memory, social support, social strain, social network size, aging, longitudinal
A lack of disease-modifying treatments, recent clinical trial failures, and the rapid aging of the population have all contributed to increased interest in lifestyle factors relevant for dementia prevention (Livingston et al., 2017). Despite growing evidence that social relations are associated with risk of Alzheimer’s disease and related dementias (ADRD; Rafnsson, Orrell, d’Orsi, Hogervot & Steptoe, 2017; Amieva et al., 2010; Crooks, Lubben, Petitti, Little & Chiu, 2008; Fratiglioni, Wang, Ericsson, Maytan, & Winblad, 2000; Bassuk, Glass & Berkman, 1999), very little is known about the “active ingredients” of social relations that have the highest potential to modify ADRD risk. Social relations are complex and multidimensional (Antonucci, Ajrouch, & Birditt, 2014), and links between social relations and health outcomes are not clear (Antonucci, Birditt & Webster, 2010). Therefore, a more comprehensive investigation of how different aspects of social relations are associated with cognitive functioning is needed to inform future social interventions to minimize age-related cognitive decline and ADRD risk.
Theoretical Framework
An individual’s social resources are often embedded within the context of a social convoy (see Antonucci, 2001; Antonucci et al., 2014; Kahn & Antonucci, 1980). The convoy model of social relations details those factors influencing the development of social relations over the life course. Convoys represent an assembly of family and friends who surround the individual, serve to socialize and protect, as well as be available in times of need. Convoys are thought to be not only dynamic and lifelong, but also multidimensional. The convoy model was designed to encompass the multiple factors, both personal and situational, that influence the development of social relations, including social networks, support exchanges, and support quality (i.e., positive or negative; Antonucci et al., 2014). These factors both independently and interactively have been shown to influence health and well-being (Berkman, Glass, Brissette, & Seeman, 2000).
Multiple dimensions of social relations range from the general notion of a social tie (i.e., network structure) to quality of relations. Network structure includes the objective characteristics of the network, such as the number of people identified as close and important (i.e., size) and the frequency with which one has contact with network members (i.e., contact frequency). It also includes composition, usually defined by the type of the role relationships (e.g. spouse, child, other family members, friend). Relationship quality is distinct from structural network components, as quality of relations refers to an individual’s evaluation of a relationship as positive and/or negative. Positive relationships can be characterized by desired levels of social support. In contrast, negative relationships can be characterized by social strain (e.g., demands, conflicts).
The theoretical complexity of social relations necessitates a consideration of multiple facets of social relations, as each dimension may influence health in unique ways. We capitalize on the complexity detailed in the convoy model to examine different aspects of network structure and quality within a single model and explore their unique influences on cognitive health. This enhanced level of specificity will allow for the identification of what it is about social relationships that influences cognitive health contemporaneously and over time. In the following sections, we review the extant literature on associations between different aspects of social relations and cognitive functioning, as well as consider distinct mechanisms through which they may be associated with cognitive aging.
Structure of Social Relations and Cognitive Functioning
Many studies that have examined associations between social relations and cognitive outcomes among older adults have included only structural indicators of social relations: marital status, social network size, and/or contact frequency. These structural aspects of social relations have been linked to preserved cognitive functioning. For example, being married has been linked to better cognitive trajectories in studies with as many as 30 years of follow-up (Gow & Mortenson, 2016; van Gelder et al., 2006; Mousavi-Nasab, Kormi-Nouri, Sundström, & Nilsson, 2012). In a population-based sample of older adults followed for an average of 5 years, larger social network size (i.e., number of children, relatives and friends seen at least once a month) was associated with better initial cognition as well as slower rates of cognitive decline (Barnes, Mendes de Leon, Wilson, Bienias, & Evans, 2004). Yet, this latter study did not differentiate between network size and contact frequency, which represent two distinct dimensions of social relations, making it difficult to pinpoint the “active ingredient.”
Structural components of a social network, such as having a large social network or having high contact frequency with network members, may affect cognition through the cognitively stimulating nature of social interactions. Complex interpersonal communication engages various cognitive resources (e.g., attention, language, memory), and taking part in social interactions more frequently or with a greater number or variety of individuals provides more opportunities to exercise these cognitive processes. The theory of cognitive reserve articulates that intellectually challenging activities and experiences can help to maintain cognitive functioning in the face of aging and disease through the development of more efficient or alternative neural networks (Barulli & Stern, 2013). Examining multiple dimensions of network structure simultaneously will advance understanding of key mechanisms though which social structure operates to influence cognitive health.
Interestingly, when multiple aspects of social relations are included within the same model, relationship quality is more frequently linked to cognition than the number of social ties (i.e., Amieva et al., 2010; Gow, Corley, Starr & Deary, 2012; Holwerda et al., 2012; Seeman, Lusignolo, Albert & Berkman, 2001). These findings suggest that some of the predictive power of network structure, such as size, may actually be attributable to resources obtained through the social network, such as high-quality social support.
Quality of Social Relations and Cognitive Functioning
Prior work suggests that the quality of social relationships is an important protective resource for cognitive functioning. In the MacArthur Studies of Successful Aging, greater emotional support at baseline predicted better cognitive functioning 8 years later, controlling for baseline cognitive functioning (Seeman et al., 2001). Similarly, participants in the Midlife in the U.S. study (MIDUS) who reported more positive elements of support at baseline exhibited significantly better cognitive performance several years later, and increases in support over the study period were also associated with better performance (Seeman et al., 2011). The receipt of positive support may be beneficial for cognition through increased feelings of community and interconnectedness (Gleason, Iida, Shrout & Bolger, 2008), self-efficacy (Antonucci & Jackson, 1987), and conscientiousness (Hill, Payne, Jackson, Stine-Morrow & Roberts, 2014), which may benefit cognition in older adults by promoting healthy lifestyle behaviors (Lachman, Neupert & Agrigoroaei, 2011) and/or effortful strategies to compensate for age-related cognitive changes (de Frias, Dixon, & Bäckman, 2003; Miller & Gagne, 2005).
Social support, however, can have both beneficial and harmful effects on cognitive health (e.g., Zahodne, Watson, Seehra & Martinez, 2018). High levels of social support, though positive, may erode self-efficacy and increase dependency, leading to psychological distress and “excess disability” (Bolger & Amarel, 2007; Silverstein, Chen & Heller, 1996; Brody, 1971; Baltes, 1988), which suggests that more support is not always better. One experimental study investigating the deleterious effects of social support manipulated the support visibility by having confederates provide advice or reassurance directly to participants (i.e., visible support) or indirectly via a query to the experimenter that would be helpful to the participant but not perceived as support (i.e., invisible support) (Bolger & Amarel, 2007). Preliminary evidence indicated that visible support was deleterious, while invisible support was beneficial, in terms of participants’ distress over a public speaking assignment. Further, both effects were mediated by participants’ appraisal of whether the confederate viewed them as inefficacious. In general, damaging effects of social support are mostly likely to be seen when support is highly visible and/or excessive. Of note, the current study only considers visible support, as it relies on self-reports.
Not all aspects of social relationships are positive, and both positive and negative aspects of support may be found in the same relationship (Antonucci, 2001). Negative support quality corresponds to social strain (e.g., demands, conflicts) within relationships (Rook, 2001). Though older adults with higher fluid cognition evidence less negative reactivity to daily stressors, such as arguments with social partners (Stawski, Mogle & Sliwinski, 2013), negative social interactions may increase physiological (Kiecolt-Glaser et al., 1997), as well as emotional distress in later life (Newsom, Rook, Nishishiba, Sorkin & Mahan, 2005). Social strain may be viewed as a source of stress that hinders cognition (Seeman et al., 2011), yet there is some evidence to suggest that social strain is not always bad. For example, individuals with a chronic illness had lower mortality risk when spousal criticism and demands were higher (Birditt & Antonucci, 2008). When examining cognitive functioning, cross-sectional and longitudinal investigations have also linked greater social strain to better cognition in older adults (Seeman et al. 2001; Xu, Thomas, & Umberson, 2016). In some circumstance, social strain may reflect the extent to which social partners challenge one’s ways of thinking or behaving, which could help to foster interpersonal growth. Further, exposure to moderate stress and, in turn, slightly elevated cortisol levels have been linked to improved cognitive functioning (De Kloet, Oitzl, & Joëls, 1999).
Overall, mechanisms theorized to underlie links between relationship quality and cognition typically involve the stress response. Specifically, negative quality relationships characterized by social strain are thought to represent a stressor, while high positive quality relationships characterized by social support may be used as a coping resource to reduce perceived stress. Perceived stress is a known risk factor for cognitive impairment (Koyanagi et al., 2018), which likely reflects deleterious effects of chronically elevated glucocorticoids on brain structure, particularly in the hippocampus (de Souza-Talarico, Marin, Sindi & Lupien, 2011; Conrad & Bimonte-Nelson, 2010; Mehedi Hasan, Shaifur Rahman, Arif & Sobhani, 2012). However, mixed findings regarding whether social support and strain are beneficial or harmful leaves open the possibility that contextual factors, such as relationship type, may influence how relationship quality relates to cognitive functioning in later life.
Relationship Type and Cognitive Functioning
Social resources may differentially affect cognitive functioning dependent on the relationship type. That is, whether the source of social resources is friends, family or a spouse may influence whether these social resources have beneficial or harmful effects on cognitive functioning in later life. Often, when examining the association between social resources and cognition, relationship type is not assessed, or composites across relationship types are constructed (i.e., Ertel, Glymour & Berkman, 2008; Fankhauser, Maercker, & Forstmeier, 2017; Haslam, Cruwys, Milne, Kan, & Haslam, 2016; Seeman et al., 2001; 2011). The nature of social relationships with a spouse, children, other family and friends, however, may differ in important ways and thus, may demonstrate distinct and independent associations with cognitive functioning in later life.
Convoys and close relationships usually include family members (i.e. spouse, parents, and children). Although these relations are often sources of positive assistance, they can also be the source of frustration, conflict, guilt, and/or ambivalence (Luescher & Pillemer, 1998). However, these negative aspects of family relationships may also promote good health outcomes in some contexts (Antonucci et al., 2010). Specifically, perceived conflict in certain relationships (e.g., the spousal relationship) may stem from arguments about health behaviors. Constantly being reminded to keep doctors’ appointments and eat healthy may be perceived as irksome but may also help to promote healthy engagement. This may be especially critical in the case of cognitive health outcomes.
In contrast to family relationships, which are more likely to be compulsory, friendships are more readily pruned over time, such that suboptimal friends do not remain in the network (English & Carstensen, 2014). Indeed, interacting with friends has been shown to yield a greater sense of immediate joy (Larson, Mannell & Zuzanek, 1986). Friendships have also been shown to require more active maintenance (e.g., shared activities, communication) (Roberts & Dunbar, 2011; Huxhold, Miche & Schuz, 2013), which has the added benefit of being cognitively stimulating. For example, older adults report that friendships are a strong motivator for engaging in leisure activities (Ball, Corr, Knight & Lewis, 2007), which have been associated with preserved cognitive functioning in later life (Jonaitis et al., 2013). Further, creating and maintaining friendships may enhance cognitive abilities due to the specific need to coordinate action with others (Brent et al., 2013). The unique functions of various relationship types provide rationale for examining their independent links with cognitive health.
Some evidence suggests that associations between cognition and social resources, such as network structure or quality, may vary depending on the relationship type (Frith & Loprinzi, 2017; La Fleur & Salthouse, 2017; Wang, He, & Dong, 2015). Yet, these were cross-sectional investigations. For example, an analysis of 1,874 older adults in the National Health and Nutrition Examination Survey found that the link between quality of social relations (i.e., social support) and cognition was significant only for the spousal relationship, while the link between social network structure (i.e., contact frequency) and cognition was significant only for friendships (Frith & Loprinzi, 2017). Another cross-sectional study of 2,613 older adults found that social contact with family members was associated with worse cognition, while social contact with friends was not associated with cognition (La Fleur & Salthouse, 2017). Finally, a study of 765 Chinese nonagenarians and centenarians found that being married and reporting a greater number of close friends were each independently associated with better cognition, but number of children and ties with neighbors were not (Wang et al., 2015). These cross-sectional investigations utilized concurrent assessments of social relations and cognition and may, therefore, be subject to reverse causation.
While few studies have investigated links between social resources and cognition across relationship type, even fewer have examined the longitudinal trajectory of cognition (i.e., slope). To our knowledge, only three studies have examined the link between social relations across relationship types and cognition longitudinally. Windsor and colleagues (Windsor, Gerstorf, Pearson, Ryan & Anstey, 2014) found that both greater support and greater strain from friends and family were independently linked to preserved cognitive functioning in later life. Support from a spouse was not linked to cognition, and findings regarding strain from a spouse were mixed. Of note, separate models were conducted for support and strain, so it is not clear whether their associations with cognition were independent of one another. Xu, Thomas and Umberson (2016) focused on the quality of social relations between spouses only and found that more frequent negative marital experiences were associated with a slower rate of cognitive decline in later life, while positive marital exchanges were not associated with cognitive trajectory. Béland and colleagues (Béland, Zunzunegui, Alvarado, Otero, & Del Ser, 2005) examined structural aspects of social relations and found that a greater number of familial ties and more social engagement with family predicted less cognitive decline up until age 80. A greater number of friendships was also linked to less decline in cognition, though only among women (Béland et al., 2005).
The above findings suggest that whether social exchanges are with friends, family, or a spouse, may differentially impact whether support or strain predict better or worse cognitive functioning in later life. Despite this initial evidence that the associations between social relations and cognition may vary by relationship type, few empirical studies have examined structural and quality aspects of social relations across relationship types within the same model. Further, scant work has examined whether these effects extend to longitudinal trajectories of cognitive functioning in later life.
The Present Study
Using data from 10,390 participants in the Health and Retirement Study, the current study aimed to clarify the relationship between social relations and cognitive aging by modeling independent associations between multiple aspects of social relations and 6-year trajectories of episodic memory, a cognitive domain that is highly sensitive to age-related cognitive decline and preclinical dementia. Social relations variables included structural dimensions (marital status; network size; frequency of contact with social network members) and quality (social support and strain from social network members), which may influence cognitive aging via mental stimulation and the stress response, respectively. We predicted that being married/partnered, larger social networks, and greater contact frequency with social network members would each be independently associated with better episodic memory trajectories due to the hypothesis that each dimension promotes greater mental stimulation. Given mixed findings of positive versus negative relationship quality on health, we test competing hypotheses to identify whether these related but separable aspects of relationship quality are beneficial or harmful for cognitive health. Finally, based on the very limited literature examining different relationship types that has produced mixed findings, we did not have a priori hypotheses regarding differential associations across relationship type (e.g., family versus friends).
Methods
Participants
Data were drawn from the Health and Retirement Study (HRS), a nationally representative sample of Americans over age 50 followed since 1992 (Sonnega & Weir, 2014). Details of the HRS longitudinal panel design, sampling, and all assessment instruments are available on the HRS website (http://hrsonline.isr.umich.edu). Participants in HRS are interviewed every two years. In 2006, the HRS initiated an enhanced face-to-face interview, which included a comprehensive psychosocial questionnaire that participants were asked to return by mail. A random one half of the sample was selected to participate in these procedures in 2006, and the other half was selected to participate in 2008. Response rates for the psychosocial questionnaire were 87.7% in 2006 and 83.7% in 2008.
Inclusion criteria for the current study were: (1) response to the psychosocial questionnaire at baseline (either 2006 or 2008); and (2) age 51 or older at baseline. In the current study, data from non-overlapping random halves of the HRS sample who completed the psychosocial questionnaire in 2006 or 2008 were combined to form a baseline time point. Biennial episodic memory data for these non-overlapping halves were similarly combined, resulting in four time points (i.e., 2006/2008, 2008/2010, 2010/2012, 2012/2014) in the combined sample of 10,390 individuals. Among these participants, 98.9% had available memory data at baseline. Across subsequent waves, 1,890 participants were lost to mortality. Among survivors, 9,230 had available memory data at time 2 (2008/2010), 8,464 had available memory data at time 3 (2010/2012), and 7,747 participants had available memory data at time 4 (2012/2014). On average, participants had 3.45 (SD = 0.97) time points of memory data. Baseline characteristics of the current sample are provided in Table 1. All participants provided written informed consent, and all study procedures were approved by the University of Michigan Institutional Review Board.
Table 1.
Sample characteristics at baseline
| Mean (SD) or % | |
|---|---|
| Age (years) | 68.58 (9.53) |
| Gender (% women) | 59.68 |
| Race/ethnicity (%) | |
| Non-Hispanic White | 78.89 |
| Non-Hispanic Black | 11.98 |
| Hispanic (any race) | 7.34 |
| Other | 1.78 |
| Education (years) | 12.72 (2.97) |
| 2006 baseline | 52.65 |
| Depressive symptoms (0-8) | 1.32 (1.87) |
| Self-rated health (1-5) | 2.79 (1.07) |
| Chronic diseases (0-7) | 2.01 (1.32) |
| Immediate recall (0-10) | 5.50 (1.59) |
| Delayed recall (0-10) | 4.41 (1.91) |
| Memory composite | 0.08 (0.89) |
| Social network structure | |
| Married/partnered (%) | 69.18 |
| Number of children (0-30) | 2.68 (2.60) |
| Number of other family (0-30) | 3.77 (4.30) |
| Number of friends (0-30) | 4.32 (4.42) |
| Contact frequency with children (1-6) | 4.01 (1.01) |
| Contact frequency with other family (1-6) | 3.38 (1.08) |
| Contact frequency with friends (1-6) | 3.75 (1.06) |
| Relationship quality | |
| Support from children (1-4) | 3.29 (0.71) |
| Support from other family (1-4) | 2.90 (0.86) |
| Support from friends (1-4) | 3.04 (0.75) |
| Support from spouse (1-4) | 3.47 (0.64) |
| Strain from children (1-4) | 1.70 (0.63) |
| Strain from other family (1-4) | 1.56 (0.61) |
| Strain from friends (1-4) | 1.40 (0.48) |
| Strain from spouse (1-4) | 1.97 (0.67) |
Measures
Memory
Episodic memory functioning was assessed every two years with a variant of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) list learning task (Ofstedal, Fisher & Herzog, 2005). Participants heard a list of 10 words and were asked to recall the words immediately and following a 5-minute delay. To improve reliability of the memory outcome in the current study, raw scores on immediate and delayed recall trials were combined into a z-score composite using means and standard deviations (SD) from the combined sample at baseline (i.e., either 2006 or 2008). Internal consistency of the memory outcome was good (α = .85), and baseline memory scores were normally distributed (skewness = −0.14, SE = 0.04; kurtosis = 0.05, SE = 0.05).
Social relations
Social relations were assessed via a paper and pencil questionnaire that was left behind after the cognitive assessment and mailed back by participants (Schuster, Kessler & Aseltine, 1990; Turner, Frankel, & Levin, 1983). Unlike episodic memory, which was assessed every two years, social relations were assessed every four years. Baseline social relations were included in the primary analyses, while longitudinal social relations were included in subsequent analyses exploring potential reverse causation. Table 2 displays a correlation matrix for the social relations variables of interest at baseline.
Table 2.
Bivariate correlations among the variables of interest at baseline expressed as Pearson’s r unless otherwise noted
| Social network structure |
Relationship quality |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Marital statusa | Contact frequency |
Support |
Strain |
||||||||||
| Size | Children | Family | Friends | Spouse | Children | Family | Friends | Spouse | Children | Family | Friends | ||
| Social network structure | |||||||||||||
| Marital status | |||||||||||||
| Network size | −.02* | ||||||||||||
| Contact – children | .02 | .14** | |||||||||||
| Contact – family | −.04** | .20** | .44** | ||||||||||
| Contact – friends | −.06** | .14** | .36** | .32** | |||||||||
| Relationship quality | |||||||||||||
| Support – spouse | - | .08** | .07** | .03* | .06** | ||||||||
| Support – children | −.09** | .24** | .37** | .19** | .08** | .21** | |||||||
| Support – family | −.10** | .25** | .15** | .48** | .08** | .11** | .40** | ||||||
| Support – friends | −.11** | .17** | .12** | .14** | .39** | .09** | .25** | .29** | |||||
| Strain – spouse | - | −.06** | −.03* | −.02 | −.02* | −.50** | −.15** | −.09** | −.06** | ||||
| Strain – children | .02 | −.12** | −.09** | −.04** | −.02* | −.15** | −.40 | −.16** | −.05** | .36** | |||
| Strain – family | .00 | −.07** | −.04** | .01 | .01 | −.14** | −.21** | −.20** | −.02 | .29** | .51** | ||
| Strain – friends | −.02 | −.02 | −.06** | .01 | .03* | −.14** | −.15** | −.07** | −.09** | .27** | .40** | .47** | |
| Memory | .11** | −.06** | .14** | .05** | .20** | .05** | −.03** | −.05** | .09** | −.03* | .02* | .00 | −.04** |
Correlations expressed as Spearman’s rho
p < 0.05
p < 0.001
Structural aspects of social relations were assessed via marital status, social network size, and contact frequency. Marital status was queried with the question, “Do you have a husband, wife, or partner with whom you live?” and coded as 1=married/partnered, 0= not married/partnered. Social network size was assessed with three items querying how many children, other family (excluding spouse), and friends the participant would say he or she has “a close relationship with.” Total social network size was quantified as the sum of these three items, top-coded at 50 based on an examination of frequency distributions. The four-year correlation between social network size measured in 2006/2008 and 2010/2012 was r = 0.47. Contact frequency was assessed separately for children, other family (excluding spouse), and friends as the mean of three items querying how often participants “Meet up (include both arranged and chance meetings),” “Speak on the phone,” or “Write or email.” Items are rated on a 6-point scale ranging from 1=Three or more times a week to 6=Less than once a year or never. Items were reverse-coded so that higher scores correspond to greater contact frequency. Contact frequency for each relationship type (i.e., children, family [excluding spouses], friends) was averaged for the primary analysis. The four-year correlation between overall contact frequency measured in 2006/2008 and 2010/2012 was r = 0.58. In subsequent analyses, contact frequency with children, family, and friends were considered as independent variables.
Quality of social relations was assessed to examine positive and negative dimensions via social support and social strain, respectively. Social support was assessed separately for spouses, children, other family, and friends with three items (“How much do they really understand the way you feel about things?” (“How much can you rely on them if you have a serious problem?” and “How much can you open up to them if you need to talk about your worries?”). Items were rated on a 4-point scale ranging from 1=A lot to 4=Not at all. Items were reverse-coded so that higher scores correspond to greater support. For each relationship type (spouse, children, other family, friends), support was quantified as the mean of the three items. In the current sample, internal consistency for support variables ranged from α = 0.81 (spouse) to α = 0.86 (other family). Support was averaged across children, family (excluding spouse), and friends for the primary analysis. In subsequent analyses, support from spouse, children, family, and friends were considered as separate independent variables.
Social strain was assessed separately for spouse, children, other family, and friends with 4 items (“How often do they make too many demands on you?” “How often do they criticize you?” “How much do they let you down when you are counting on them?” and “How much do they get on your nerves?”). Items were rated on a 4-point scale ranging from 1=A lot to 4=Not at all. Items were reverse-coded so that higher scores correspond to greater social strain. For each relationship type (spouse, children, other family, friends), strain was quantified as the mean of the four items. In the current sample, internal consistency for strain variables ranged from α = 0.74 (friends) to α = 0.78 (spouse and other family). Strain was averaged across children, family (excluding spouse), and friends for the primary analysis. In subsequent analyses, strain from spouses, children, family, and friends were considered as separate independent variables.
Covariates
Baseline assessment wave (2006 or 2008) was included as a dichotomous variable, with 2006 as the reference category (0 = 2006; 1 = 2008). Age (in years) corresponded to age at the time of the baseline assessment wave (2006 or 2008). Gender was a dichotomous variable, with male as the reference category (0 = male; 1 = female). Self-reported race and ethnicity was dummy-coded into four categories: non-Hispanic White, non-Hispanic Black, Hispanic (of any race), and non-Hispanic other. The largest category, non-Hispanic White, was treated as the reference group. Education was self-reported years of education (0-17).
Sensitivity analyses additionally controlled for mental and physical health. Commonly used in epidemiological research, sensitivity analysis is a method to determine the robustness of results by examining the extent to which they are affected by changes in methods, models, unmeasured variables, or assumptions (Porta, 2008). Mental health was assessed with an 8-item version of the Center for Epidemiologic Studies – Depression Scale (CESD; Radi off, 1977) used in the HRS. Physical health was assessed with self-reported chronic health conditions and self-rated health. Chronic conditions were quantified as the sum of the presence/absence of hypertension, diabetes, cancer (excluding skin cancer), lung disease, heart disease, arthritis, and stroke. Self-rated health was assessed with the item, “Would you say your health is excellent, very good, good, fair, or poor?” Responses were coded on a scale of 1 (excellent) to 5 (poor), with higher scores corresponding to worse health.
Analytic Strategy
Descriptive statistics were computed in SPSS. Associations between social relations and episodic memory trajectories were examined using structural equation models (SEM) in Mplus version 8 (Muthén & Muthén, 2007). Trajectories of episodic memory functioning were estimated with a latent growth curve model using maximum likelihood estimation. Time was parameterized as years from baseline (2006 or 2008). Missing data were managed with full information maximum likelihood using all available data at each occasion. Models estimated the following latent variables: initial memory level (intercept) and subsequent rate of memory change over the six-year follow-up (linear slope).
Figure 1 provides a graphical depiction of the initial SEM. In this initial model, memory intercept and slope were regressed onto the structure and quality variables: marital status, total social network size, average contact frequency, average support, and average strain. Subsequently, a second model was run to clarify whether significant associations were unique to a specific relationship type (i.e., children, family [excluding spouse], or friends). A final model restricted to individuals who were married or partnered excluded marital status and additionally included support and strain from spouse/partner.
Figure 1.

Schematic of the initial structural equation model. For simplicity, covariates (i.e., year of baseline assessment, baseline age, gender, race, ethnicity, education) are not shown.
Model fit was evaluated with the following commonly-used indices: comparative fit index (CFI), Tucker-Lewis index (TLI), root-mean-square error of approximation (RMSEA), and standardized root-mean square residual (SRMR). CFI > 0.95, TLI > 0.95, RMSEA < 0.06, and SRMR < 0.05 were used as criteria for adequate model fit (Hu & Bentler, 1999).
Results
In a minimally adjusted model that included all covariates but none of the social predictors of interest, memory composite scores declined by 0.06 points per year. In other words, a 69-year-old, non-Hispanic white man with 12 years of education who first completed the psychosocial questionnaire in 2006 was estimated to decline 0.36 points on the memory composite over the 6-year follow-up period. In the paragraphs below, independent associations between averaged social relations variables across type (i.e., spouse, children, other family, friends) and memory trajectories are considered first. Next, this analysis is repeated to consider each significant social relations variable by relationship type.
Social Relations: Structure and Quality
Fit of the initial model was good: CFI = 0.99; TLI = 0.98; RMSEA = 0.02 (90% CI = 0.02-0.03); SRMR = 0.01. Results are shown in Table 3.
Table 3.
Standardized results from initial latent growth curve model (across relationship types)
| Initial memory level |
Rate of memory change |
|||||
|---|---|---|---|---|---|---|
| Estimate | 95% CI | p | Estimate | 95% CI | p | |
| Age | −.44 | −.46,−.43 | <.001 | −.42 | −.50,−.34 | <.001 |
| Education | .35 | .33, .36 | <.001 | .03 | −.03, .08 | .44 |
| Female | .20 | .19, .22 | <.001 | .01 | −.04, .06 | .77 |
| Black | −.17 | −.18,−.15 | <.001 | .14 | .09, .20 | <.001 |
| Hispanic | −.06 | −.18,−.04 | <.001 | .08 | .03, .14 | .010 |
| Other | −.06 | −.08,−.05 | <.001 | .01 | −.04, .06 | .69 |
| 2008 baseline | −.01 | −.03, .00 | 0.22 | .06 | .01, .11 | .05 |
| Social network structure | ||||||
| Married/partnered | .02 | .00, .04 | .04 | .08 | .02, .13 | .02 |
| Network size | .00 | −.02, .02 | .98 | −.03 | −.09, .02 | .30 |
| Contact frequency | .10 | .08, .12 | <.001 | .09 | .04, .15 | .01 |
| Quality | ||||||
| Support | −.03 | −.05,−.01 | .03 | −.03 | −.09, .02 | .34 |
| Strain | −.09 | −.10,−.07 | <.001 | −.02 | −.07, .04 | .59 |
Note. CI = Confidence interval.
Initial memory
As shown, social network structure and quality were each independently associated with initial memory level. Specifically, being partnered, greater contact frequency, less support, and less strain with network members were each independently associated with higher initial memory. Younger age, higher education, female gender, and self-reported non-Hispanic white race were also associated with higher initial memory.
Rate of memory change
Only social network structure was independently associated with subsequent rate of memory change. Specifically, marital status (having a partner) and greater contact frequency were each independently associated with slower memory decline. Figure 2 depicts memory trajectories as a function of marital status, and Figure 3 depicts memory trajectories as a function of contact frequency. Older age and self-reported non-Hispanic white race were associated with faster memory decline.
Figure 2.

Model-estimated memory trajectories as a function of marital status. Level differences reflect the finding that being married/partnered was associated with higher initial memory. Non-parallel lines reflect the finding that being married/partnered was associated with slower subsequent rate of memory decline. Depicted intercepts and slopes control for all other variables in the model (i.e., age, gender, race, ethnicity, education, baseline year, social network size, contact frequency, social support, and social strain).
Figure 3.
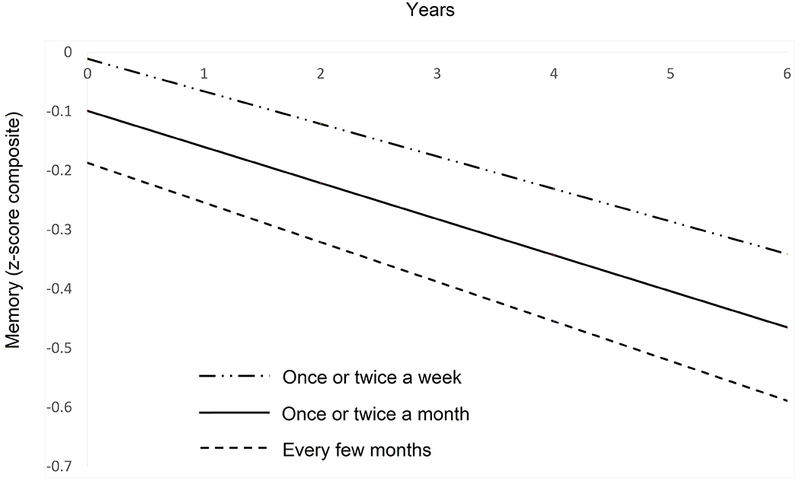
Model-estimated memory trajectories as a function of contact frequency with social network members other than spouses. Level differences reflect the finding that greater contact frequency was associated with higher initial memory. Non-parallel lines reflect the finding that greater contact frequency was associated with slower subsequent rate of memory decline. Depicted intercepts and slopes control for all other variables in the model (i.e., age, gender, race, ethnicity, education, baseline year, marital status, social network size, social support, and social strain).
Sensitivity analyses
We conducted a series of sensitivity analyses to determine whether results from our primary model changed when (1) variables were removed, (2) variables were added, or (3) independent (i.e., social relations) and dependent (i.e., episodic memory) variables were switched.
Examining individual social relations.
Many previous studies examining links between social relations and cognition have included only a single social variable, typically social network size or social support. In order to compare results from the current sample to this prior work, we also re-ran our initial model excluding all social variables except (1) social support or (2) social network size. In these separate models, both average support across relationship types (standardized estimate = 0.04; 95% CI: 0.02, 0.05; p < 0.001) and total social network size (standardized estimate = 0.0.02; 95% CI: 0.01, 0.04; p = 0.031) were positively associated with initial memory, though neither was significantly associated with subsequent memory change (both p’s > 0.69).
Considering mental and physical health.
Separate sensitivity analyses were conducted to determine the extent to which depressive symptoms or health status at baseline influenced the results. We did not include these additional covariates in the primary model because while they may represent potential confounders of associations between social relations and episodic memory, they may also represent potential mediators.
Among 10,324 participants with available data on the CESD, we re-ran the initial model controlling for baseline CESD. A higher level of depressive symptoms at baseline was associated with lower initial memory (standardized estimate = −0.12; 95% CI: −0.14, −0.10; p < 0.001), but not with subsequent memory change (standardized estimate = −0.04; 95% CI: −0.09, 0.01; p = 0.221). With regard to the social variables, the results of this model were identical to the primary model with one exception: being partnered was no longer significantly associated with higher initial memory (standardized estimate = 0.00; 95% CI: −0.02, 0.02; p = 0.845), but being partnered was still significantly associated with less subsequent memory decline (standardized estimate = 0.07; 95% CI: 0.01, 0.12; p = 0.048). When depressive symptoms were modeled as a time-varying covariate in a subset of 7,545 participants with available CESD data at all four time points, the longitudinal findings were identical. Specifically, being married (standardized estimate = 0.09; 95% CI: 0.03, 0.15; p = 0.017) and reporting more frequent contact with network members (standardized estimate = 0.12; 95% CI: 0.06, 0.19; p = 0.001) were each independently associated with less memory decline.
Among 10,351 participants with available data on physical health, we re-ran the initial model controlling for baseline chronic health conditions and self-rated health. Worse self-rated health was associated with lower initial memory (standardized estimate = −0.14; 95% CI: −0.16, −0.12; p < 0.001) and faster subsequent memory decline (standardized estimate = −0.08; 95% CI: −0.14, 0.02; p = 0.022). Number of chronic conditions was not associated with initial memory (standardized estimate = −0.01; 95% CI: −0.03, 0.01; p = 0.500) or memory change (standardized estimate = 0.03; 95% CI: −0.03, 0.08; p = 0.460) independent of self-rated health. With regard to the social variables, the results of this model were identical to the primary model with one exception: being partnered was no longer significantly associated with higher initial memory (standardized estimate = 0.01; 95% CI: −0.01, 0.03; p = 0.262), but being partnered was still significantly associated with less subsequent memory decline (standardized estimate = 0.07; 95% CI: 0.02, 0.13; p = 0.022). When physical health was modeled with time-varying covariates in a subset of 7,787 participants with available data on chronic conditions and self-rated health at all four time points, the longitudinal findings were identical. Specifically, being married (standardized estimate = 0.08; 95% CI: 0.02, 0.14; p = 0.019) and reporting more frequent contact with network members (standardized estimate = 0.12; 95% CI: 0.06, 0.18; p = 0.001) were each independently associated with less memory decline.
Longitudinal changes in social relations.
Finally, separate latent growth curve models were run to examine bi-directional effects. Specifically, we examined whether baseline memory performance predicted subsequent rates of change in the continuous social relations variables. Because the psychosocial questionnaire was administered every four years, eight years of data were available for the random half of the sample who first received the questionnaire in 2006, but only four years of data were available for the other half who first received the questionnaire in 2008. Therefore, the following time points of data were used: 2006/2008, 2010/2012, and 2014. Initial unconditional models revealed insufficient slope variance (i.e., non-significant individual differences) for social network size, precluding our ability to identify predictors of change in that variable.
Minimally adjusted models were run to characterize trajectories of change in each of the other social variables, controlling for age, sex, race, ethnicity, education, and baseline year (2006 or 2008). These models revealed that a 69-year-old, non-Hispanic white man with 12 years of education who first completed the psychosocial questionnaire in 2006 reported significant decreases in contact frequency (standardized slope estimate = −0.15; 95% CI: −0.22, −0.08; p = 0.001) and social strain (standardized slope estimate = −0.34; 95% CI: −0.43, −0.25; p = 0.004), accompanied by a significant increase in social support (standardized slope estimate = 0.17; 95% CI: 0.06, 0.28; p = 0.009). In subsequent models adding baseline memory as a predictor, there were no significant associations between baseline memory and subsequent rates of change in contact frequency (standardized estimate = 0.04; 95% CI: −0.01, 0.09; p = 0.143), social support (standardized estimate = −0.03; 95% CI: −0.10, 0.04; p = 0.502), or social strain (standardized estimate = −0.04; 95% CI: −0.09, 0.01; p = 0.195).
Examining Individual Relationship Types
Fit of a subsequent model replacing the averaged contact frequency, support, and strain variables with variables specific to each relationship type (i.e., children, other family [excluding spouse], and friends) fit well: CFI = 0.99; TLI = 0.98; RMSEA = 0.02 (90% CI = 0.02-0.02); SRMR = 0.01. Results are summarized in Table 4.
Table 4.
Standardized results from subsequent latent growth curve model: By relationship type
| Initial memory level |
Rate of memory change |
|||||
|---|---|---|---|---|---|---|
| Estimate | 95% CI | p | Estimate | 95% CI | p | |
| Age | −.43 | −.45,−.42 | <.001 | −.42 | −.50,−.34 | <.001 |
| Education | .33 | .32, .35 | <.001 | .02 | −.04, .08 | .59 |
| Female | .20 | .19, .22 | <.001 | .02 | −.04, .07 | .64 |
| Black | −.16 | −.18, −.14 | <.001 | .15 | .09, .20 | <.001 |
| Hispanic | .10 | −.08, −.04 | <.001 | .10 | .04, .15 | .01 |
| Other | .01 | −.08, −.04 | <.001 | .01 | −.04, .06 | .82 |
| 2008 baseline | .06 | −.03, .00 | .19 | .06 | .01, .11 | .07 |
| Social network structure | ||||||
| Married/partnered | .08 | .01, .04 | .03 | .08 | .02, .14 | .02 |
| Network size | −.00 | −.02, .02 | .77 | −.03 | −.09, .02 | .30 |
| Contact frequency – children | .05 | .03, .07 | <.001 | .08 | .01, .14 | .06 |
| Contact frequency – other family | −.01 | −.03, .01 | .43 | −.05 | −.11, .02 | .23 |
| Contact frequency – friends | .10 | .08, .12 | <.001 | .10 | .03, .16 | .01 |
| Quality | ||||||
| Support from children | .00 | −.02, .03 | .81 | −.00 | −.07, .07 | .98 |
| Support from other family | −.03 | −.05, −.01 | .02 | .03 | −.04, .09 | .54 |
| Support from friends | −.00 | −.02, .02 | .97 | −.06 | −.12, .00 | .09 |
| Strain from friends | −.04 | −.06, −.02 | .001 | .02 | −.04, .07 | .66 |
| Strain from children | −.03 | −.05, −.01 | .03 | −.04 | −.11, .02 | .30 |
| Strain from other family | −.04 | −.06, −.02 | .002 | .02 | −.05, .08 | .67 |
Note. CI = Confidence interval.
Initial memory
Contact frequency was significantly associated with initial memory level, but only for certain relationships. Specifically, greater contact frequency with children and friends were each independently associated with higher initial memory level. Associations involving the other structure variables (i.e., social network size, marital status) were similar to the initial model such that size was not associated with initial memory, and being married/partnered was associated with better initial memory. With regard to social support, only support from family members was significantly associated with memory level. Specifically, greater support from family members other than spouse and children was associated with lower initial memory level. With regard to strain, strain in all three relationship types were associated with memory level. Specifically, greater strain from children, other family (excluding spouse), and friends were each independently associated with lower initial memory level. Associations involving covariates were similar to the initial model.
Memory change
Contact frequency with friends was the only social relations variable associated with subsequent rate of memory change. Specifically, greater contact frequency with friends was associated with slower subsequent memory decline. Associations involving the other structure variables (i.e., social network size, marital status) were similar to the initial model. Similar to the initial model in which support and strain were each averaged across relationship types, neither support nor strain from individual relationships was significantly associated with memory change. Associations involving covariates were similar to the initial model.
Spousal Relationship Quality
The initial model was also run in a subset of participants who were married or partnered at baseline (N=7,142), replacing the marital status variable with two variables corresponding to support and strain from spouse. As shown in Table 5, neither spousal support nor spousal strain was significantly associated with initial memory or subsequent rate of memory change.
Table 5.
Standardized results from married subsample (N = 7,142).
| Initial memory level |
Rate of memory change |
|||||
|---|---|---|---|---|---|---|
| Estimate | 95% CI | p | Estimate | 95% CI | p | |
| Age | −.42 | −.44, −.40 | <.001 | −.41 | −.53, −29 | <.001 |
| Education | .34 | .31, .36 | <.001 | .03 | −.05, −.10 | .516 |
| Female | .21 | .19, .24 | <.001 | −.01 | −.08, .06 | .862 |
| Black | −.14 | −.16, −.12 | <.001 | .15 | .07, .23 | .001 |
| Hispanic | −.06 | −.08, −.04 | <.001 | .07 | −.01, .14 | .136 |
| Other | −.06 | −.08, −.04 | <.001 | −.01 | −.08, .05 | .721 |
| 2008 baseline | −.03 | −.05, −.01 | .033 | .13 | .05, .20 | .004 |
| Social network structure | ||||||
| Network size | −.01 | −.03, .02 | .615 | −.03 | −.10, .04 | .497 |
| Contact frequency | .10 | .08, .13 | <.001 | .14 | .06, .23 | .005 |
| Relationship quality | ||||||
| Support from spouse | .02 | −.00, .05 | .175 | −.02 | −.10, .07 | .725 |
| Strain from spouse | .00 | −.03, .03 | .988 | −.02 | −.11, .07 | .693 |
| Support from other relationships | −.03 | −.05, −.00 | .082 | −.04 | −.12, .04 | .373 |
| Strain from other relationships | −.09 | −.11, −07 | <.001 | −.03 | −.11, .05 | .533 |
We also examined whether spousal relationship quality was associated with memory trajectories in a model that excluded the other social relations variables. In this model, spousal strain was negatively associated with initial memory (standardized estimate = −0.04; 95% CI: −0.06, −0.02; p = 0.004) but was not associated with subsequent rates of memory change (standardized estimate = −0.04; 95% CI: −0.11, 0.04; p = 0.465). Spousal support was not significantly associated with initial memory (standardized estimate = 0.02; 95% CI: −0.01, 0.04; p = 0.255) or memory change (standardized estimate = −0.02; 95% CI: −0.10, 0.06; p = 0.721).
Due to the large correlation between spousal support and strain (see Table 2), a sensitivity analysis combined spousal support and strain into a single composite variable by reverse-coding strain and taking the mean. The resultant spousal relationship quality variable was not significantly associated with initial memory (standardized estimate = 0.02; 95% CI: −0.00, 0.04; p = 0.164) or memory change (standardized estimate = 0.00; 95% CI: −0.07, 0.08; p = 0.958). In a separate sensitivity analysis excluding all social relations variables other than spousal support and spousal strain, only one significant association emerged. Specifically, spousal strain was negatively associated with initial memory (standardized estimate = −0.04; 95% CI: −0.06, −0.02; p = 0.004).
Discussion
This longitudinal study enhances understanding of the complex links between social relations and late-life cognitive functioning by highlighting and examining the multidimensional nature of social relations. The present findings demonstrate that distinct aspects of social relations (i.e., structure and quality) are each independently associated with episodic memory functioning in a large nationally representative sample of older adults. While both the structure and quality of social relations were associated with initial memory level, only structural aspects of social relations (i.e., being married/partnered and reporting more frequent contact with friends) were independently associated with subsequent rates of episodic memory change. Importantly, while social relations at baseline predicted subsequent changes in memory, memory functioning at baseline did not predict subsequent changes in social relations.
These results are consistent with the convoy model of social relations, which posits that social relations are multidimensional and have far-reaching effects on health (Antonucci, 2001; Antonucci et al., 2014; Kahn & Antonucci, 1980). Social relations have been theorized to influence health through multiple behavioral pathways (Berkman et al., 2000). In the following paragraphs, we consider the ways in which different aspects of social relations (i.e., structure and quality) could influence late-life episodic memory. Specifically, it may be that structural aspects of social relations and quality of social relations influence cognitive aging via different mechanisms: mental stimulation versus stress regulation, respectively.
Mental Stimulation and Structural Aspects of Social Relations
In the current study, both being married/partnered and more frequent contact with network members were independently associated with not only higher memory level, but also slower subsequent memory decline. With regard to the size of these longitudinal effects, being married/partnered was equivalent to four to five years of aging, and a one-point increase on the six-point contact frequency scale (e.g., interacting with network members once or twice a month versus every few months) was equivalent to three years of aging. These effects may be meaningful, as microsimulation modeling has indicated that delaying the onset of dementia by only five years would yield a 41% reduction in the number of prevalent dementia cases (Zissimopoulos, Crimmins & St. Clair, 2014). That these associations were independent of social support and strain from these relationships may hint at underlying mechanisms, illustrating the advantage of considering multiple dimensions of social relations simultaneously. Both partnership and frequent social interaction may provide opportunities for beneficial mental stimulation.
Positive associations between being married and both episodic memory level and change are consistent with previous work in other datasets (Gow & Mortenson, 2016; van Gelder et al., 2006; Mousavi-Nasab et al., 2012). Being married may benefit late-life memory not only through pathways such as material resources (e.g., wealth) or assistance/pressure to follow health recommendations (Waite & Gallagher, 2002), but also through the mental stimulation that occurs when one is partnered. Marriage is often a relationship that requires communicating with and thinking about another person. The marital role, therefore, invites and perhaps requires heightened mental stimulation otherwise absent among those without a significant other.
In sensitivity analyses controlling for mental or physical health, the association between being partnered and better initial memory became non-significant. This pattern of results suggests that better mental and physical health may represent mechanisms by which being partnered could lead to better memory functioning (Waite & Gallagher, 2002). However, it is also possible that mental and physical health are confounders of the relationship between being partnered and initial memory functioning if individuals with poorer mental or physical health are less likely to establish or maintain romantic relationships. The fact that being partnered at baseline was still associated with better memory trajectories over time independent of baseline health strengthens our conclusion that there is a prospective association between being partnered and memory aging. It also suggests that better health may not be the primary mechanism by which being partnered influences subsequent memory trajectories. Living with a spouse or partner may be intrinsically cognitively stimulating, offering ongoing opportunities to engage in conversation and negotiate the needs of another person. Some of these benefits may not be unique to the marital relationship, as a longitudinal study in Finland, Italy, and the Netherlands showed that both married men and unmarried men who lived with others exhibited less cognitive decline than men who lived alone, and these results were not attributable to depressive symptoms or health behaviors (van Gelder, Tijhuis, Kalmijn, Giampaoli, Nissenen, & Kromhout, 2006). Mental stimulation, therefore, may be a primary mechanism through which contact with others benefits cognitive health.
More frequent contact with network members was also associated with better memory aging. Specifically, the cognitive benefits of greater social interaction may occur through conversational engagement. Conversation not only taps cognitive domains of attention, language, and memory, but also exposes individuals to new ideas and challenges them to navigate interpersonal situations. This mental stimulation may strengthen cognitive networks (e.g., “use it or lose it;” Hultsch et al., 1999), which could make these networks more robust to age-related pathology (i.e., cognitive reserve; Barulli & Stern, 2013). Social interaction may also provide opportunities for physical activity, and physical activity has been shown to improve brain health among older adults (Benedict et al., 2013).
This study extends previous findings by testing whether associations between contact frequency and memory trajectories are unique to particular social network members. That friendships may be particularly important for older adults’ health is consistent with previous research findings. For example, several studies have linked a greater proportion of friends within one’s social network to better emotional (Fiori, Antonucci & Cortina, 2006; Fuller-Iglesias, Webster, & Antonucci, 2015), health-related (Shiovitz-Ezra & Litwin, 2012) and cognitive (Li & Dong, 2017; Sharifian, Manly, Brickman & Zahodne, under revision) outcomes. Friendships are less likely than family relationships to be compulsory, particularly in late life. Indeed, individuals tend to prune suboptimal friends from their social networks as they age, whereas suboptimal family members may be harder to prune (English & Carstensen, 2014). Friendships have also been shown to require more active maintenance (e.g., shared activities, communication) than family relationships (Roberts & Dunbar, 2011; Huxhold et al., 2013), and it may be this active engagement that underlies the beneficial effects of interacting with friends.
In the current study, there were no independent associations between social network size and memory level or change. Interestingly, many studies of the beneficial role of social relations in cognitive aging have operationalized social relations as number of social ties (e.g., Bennett, Schneider, Tang, Arnold & Wilson, 2006; Brenowitz, Kukull, Beresford, Monsell & Williams, 2014; Sörman, Rönnlund, Sundströrm, Norberg, & Nilsson, 2017). The current findings suggest that these previous findings may have been driven by other, more specific characteristics of the social network that correlate with network size. Indeed, in the current study, social network size was positively associated with memory in a model that excluded other aspects of social relations. However, social network size was also associated with nearly all of the other social variables examined in this study, and it was these variables that were independently associated with memory level and/or change. Thus, larger social networks may only be beneficial in cognitive aging to the extent that they provide older adults with more opportunities for social interaction. The mental stimulation inherent in social interaction may be one “active ingredient” of social relations that contributes to healthy cognitive aging.
Stress and Quality of Social Relations
Associations between quality of social relations and cognitive health were not evident over time. Cross-sectional associations between greater social strain and lower memory functioning in this study are consistent with a large body of research linking chronic stress to poorer memory in older adults (de Souza-Talarico et al., 2011; Sandi, 2007; Conrad & Bimonte-Nelson, 2010; Mehedi Hasan et al.,2012; Head, Sing, & Bugg, 2012). A commonly described mechanism by which stress negatively influences memory is via negative effects of glucocorticoids on hippocampal structure and function (de Souza-Talarico et al., 2011; Conrad & Bimonte-Nelson, 2010; Mehedi Hasan et al., 2012). In the current study, independent associations between greater reported strain in all relationship types and worse initial memory level suggest that the negative effects of interpersonal stress on memory may be at least additive. While the lack of association between strain and subsequent memory change leaves open the possibility that poorer memory functioning may lead to negative interactions with social network members, follow-up analyses did not reveal an association between baseline memory and subsequent changes in social strain. The lack of a prospective association between social strain and subsequent memory change may reflect the relatively young age of this older adult sample and the limited follow-up period. Both of these aspects may have restricted the observed variance in memory slope, thus limiting our ability to precisely estimate the association between social strain and memory change. Modeling additional follow-up occasions over a longer period as this cohort ages is likely to yield greater change, more precise estimates of change, as well as greater variability in change, which together could reveal additional associations between social strain and memory trajectories. Below, we consider the ways in which both social support and strain may be best understood through the lens of stress exposure and stress regulation.
In models that did not include any other social variables, social support averaged across relationship types was positively associated with initial memory, consistent with previous studies (Ellwardt, Aartsen, Deeg, & Steverink, 2013; Kats et al., 2016). However, social support averaged across relationship types was negatively associated with initial memory in models that included the other social relations variables of interest. This pattern of findings suggests that high levels of social support above and beyond what is expected based on other indicators of social network structure and quality (i.e., excessive support) may not be beneficial for cognitive functioning. It is possible that very high levels of social support can erode self-efficacy (Bolger & Amarel, 2007) and induce dependency (Baltes & Wahl, 1992; Baltes & Wahl, 1996), both of which may create stress and in turn, lead to poorer memory functioning.
It is also notable that zero-order correlations between social support and baseline memory differed by relationship type. Specifically, social support from spouse and friends was positively correlated with baseline memory, while social support from children and other family was negatively correlated with memory. These divergent correlations suggest that social resources obtained through different relationship types may have different causal bases or exert differential stress effects. It may also be the case that cognitive resources exert differential effects on the perception of social resources obtained through different relationship types.
The current findings leave open the possibility of reversed causation because the negative association between social support and initial memory level did not extend to longitudinal memory change. Specifically, one’s level of memory functioning, which may or may not reflect a change from a previous level, could affect support received from network members and/or one’s perception of that support. Memory dysfunction may lead to a mobilization of social support, particularly from relatives, which was the only relationship type for which social support was significantly associated with memory. However, follow-up analyses did not support an association between baseline memory and subsequent changes in social support.
The lack of a prospective association between social support and subsequent memory change is consistent with a recent study of 20-year cognitive change in 15,792 participants that found no association between social support and cognitive changes (Kats et al., 2016). Results contrast with another recent study that did find that emotional support was associated with less cognitive decline (Ellwardt et al., 2013). However, emotional support in the latter study was operationalized in terms of contact frequency rather than quality of support (i.e., “How often in the past year did you talk to [name] about your personal experiences and feelings?”). As discussed above, contact frequency was associated with less memory decline independent of other structural aspects and quality of social relations in the current study. Therefore, this latter study may provide additional support for the possibility that mental stimulation inherent in talking with social partners may be one “active ingredient” of social relations that contributes to healthy cognitive aging. In sum, it appears that quality of relationships have important cognitive effects cross-sectionally, suggesting stress effects via social relations have short-term impact, while the effects of social relations structure on memory aging extend across time.
Limitations and Strengths
Although the current study highlights the importance of specific social resources from different relationship types to explain individual differences in cognitive aging, there are some notable limitations. First, because the measures of social relations were added to the HRS in 2006, we were only able to examine episodic memory changes over a relatively short period of time (i.e., six years). Future studies should investigate longer-term changes in episodic memory functioning in later life. Second, only perceived social support measures were available in the current study. Prior research suggests that mixed findings regarding the protective or detrimental effects of social support may be dependent on whether actual support received or perceived social support is measured (Wethington & Kessler, 1986). Further, perceived social support in the current study focused predominantly on emotional aspects of support (i.e., do they understand you?), however, social support can also can take different forms. Therefore, future research should further investigate whether distinct types of social support (i.e., aid, affect or affirmation) and received social support differ in their associations with cognitive functioning in later life. Finally, the measures used to operationalize social relations in the HRS limited our ability to disentangle all aspects of social relations that may be important in memory aging. Specifically, these measures obscure potentially important aspects of individual relationships, as the items required participants to consider all of their individual network members within a category as a whole (e.g., all relatives, all friends). It may be that high levels of contact, support, or strain from an individual network member could have important consequences for memory aging.
Strengths of this study include its large, national sample of older adults. Another strength is the inclusion of multiple social relations variables in the same model, allowing us to preliminarily pinpoint potential elements of social interaction and relationships important for memory in later life. The longitudinal design also allowed for a demonstration of prospective associations, strengthening the interpretation that social variables are relevant for future memory aging. Specifically, the fact that both marital status and contact frequency predicted not only initial memory level, but also subsequent rate of memory change despite the relatively short follow-up period, lends important longitudinal support to the potential for these structural aspects of social relations to modify future dementia risk. Finally, sensitivity analyses revealed that the reported associations were largely robust to physical and mental health covariates and that baseline memory level did not lead to systematic changes in the structure or quality of social relations. The latter finding does not necessarily preclude the possibility of reciprocal influences between cognition and some aspects of the social network, as such influences may only be operable in subsets of individuals (e.g., those transitioning to dementia) or may operate on a different time scale than was examined in the current study. Social relations and cognition may also interact over time. These findings underscore the life span nature of both social relations and cognitive aging.
Conclusion
The results of the current study may help to refine theories of healthy aging and inform intervention development. Specifically, structural aspects of social relations, such as living with a partner or more frequent contact with network members, may be most beneficial for cognitive aging, which may reflect opportunities for mental stimulation. In contrast, the quality of social relations, such as the level of social strain, may influence cognition via brain and cognitive effects of stress. Taking a more comprehensive approach to characterizing social relations will allow for better understanding of their “active ingredients.” The convoy of social relations provides a useful framework for identifying various dimensions of social relations and the ways in which these dimensions may uniquely influence cognitive change. The current study suggests that programs or interventions aiming simply to expand older adults’ social networks may not be as effective as interventions that promote specific relationship types (e.g., friendships) or increase contact frequency. Future studies should examine longer periods of follow-up, test the efficacy and effectiveness of tailored social interventions to improve functioning across cognitive domains, and explore the psychological, behavioral, physiological, and neural mechanisms underlying the complex links between social relations and cognitive aging.
Acknowledgments
This work was supported by the National Institute on Aging of the National Institutes of Health under Award Numbers R00AG047963 and R01AG054520. The HRS (Health and Retirement Study) is sponsored by the National Institute on Aging (grant number NIA U01AG009740) and is conducted by the University of Michigan. The sponsor had no role in the current analyses or the preparation of this paper. The data appearing in this manuscript were previously disseminated through the 5th International Conference on Aging & Cognition in Zürich, Switzerland on April 24-26, 2019.
References
- Amieva H, Stoykova R, Matharan F, Helmer C, Antonucci T, & Dartigues J (2010). What aspects of social network are protective for dementia? Not the quantity but the quality of social interactions is protective up to 15 years later. Psychosomatic Medicine, 72(9), 905–911. 10.1097/PSY.0b013e3181f5e121 [DOI] [PubMed] [Google Scholar]
- Antonucci TC (2001). Social relations: An examination of social networks, social support, and sense of control In Birren JE, & Schaie KW(Eds.). Handbook of the psychology of aging (5th ed.). (pp. 427–453). San Diego, US: Academic Press. [Google Scholar]
- Antonucci TC, Ajrouch KJ, & Birditt KS (2014). The convoy model: Explaining social relations from a multidisciplinary perspective. The Gerontologist, 54(1), 82–92. 10.1093/geront/gnt118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antonucci TC, Birditt KS, & Webster N (2010). Social relations and mortality: A more nuanced approach. Journal of Health Psychology, 15(5), 649–659. 10.1177/1359105310368189. [DOI] [PubMed] [Google Scholar]
- Antonucci TC, & Jackson JS (1987). Social support, interpersonal efficacy, and health: A life course perspective In Carstensen LL& Edelstein BA(Eds.), Pergamon general psychology series, Vol. 146. Handbook of clinical gerontology (pp. 291–311). Elmsford, NY, US: Pergamon Press. [Google Scholar]
- Ball V, Corr S, Knight J, & Lowis MJ (2007). An investigation into the leisure occupations of older adults. British Journal of Occupational Therapy, 70, 393–400. [Google Scholar]
- Baltes MM (1988). The etiology and maintenance of dependency in the elderly: Three phases of operant research. Behavior Therapy, 19, 301–319. 10.1016/S0005-7894(88)80004-2 [DOI] [Google Scholar]
- Baltes MM & Wahl H-W (1992). The dependency-support script in institutions: Generalization to community settings. Psychology and Aging, 7, 409–418. 10.1037/0882-7974.7.3.409 [DOI] [PubMed] [Google Scholar]
- Baltes MM, & Wahl H-W (1996). Patterns of communication in old age: The dependence support and independence-ignore script. Health Communication, 8, 217–231. 10.1207/s15327027hc0803_3 [DOI] [Google Scholar]
- Barnes LL, Mendes de Leon CF, Wilson RS, Bienias JL, & Evans DA (2004). Social resources and cognitive decline in a population of older African Americans and whites. Neurology, 63, 2322–2326. 10.1212/01.WNL.0000147473.04043.B3 [DOI] [PubMed] [Google Scholar]
- Barulli D, & Stern Y (2013). Efficiency, capacity, compensation, maintenance, plasticity: Emerging concepts in cognitive reserve. Trends in Cognitive Science, 17, 502–509. 10.1016/j.tics.2013.08.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bassuk SS, Glass TA, & Berkman LF (1999). Social disengagement and incident cognitive decline in community-dwelling elderly persons. Annals of Internal Medicine, 131(3), 165–173. [DOI] [PubMed] [Google Scholar]
- Béland F, Zunzunegui M, Alvarado B, Otero A, & de Ser T, (2005). Trajectories of cognitive decline and social relations. Journal of Gerontology: Psychological Sciences, 60, 320–330. 10.1093/geronb/60.6.P320 [DOI] [PubMed] [Google Scholar]
- Benedict C, Brooks SJ, Kullberg J, Nordenskjöld R, Burgos J, … Schiöth HB. (2013). Association between physical activity and brain health in older adults. Neurobiology of Aging, 34, 83–90. [DOI] [PubMed] [Google Scholar]
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS (2006). The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurology, 5, 406–412. 10.1016/S1474-4422(06)70417-3 [DOI] [PubMed] [Google Scholar]
- Berkman LF, Glass T, Brissette I, & Seeman TE (2000). From social integration to health: Durkheim in the new millennium. Social Science & Medicine, 51, 843–857. 10.1016/S0277-9536(00)00065-4 [DOI] [PubMed] [Google Scholar]
- Birditt K, & Antonucci TC (2008). Life sustaining irritations? Relationship quality ad mortality in the context of chronic illness. Social Science & Medicine, 67, 1291–1299. 10.1016/j.socscimed.2008.06.029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bolger N, & Amarel D (2007). Effects of social support visibility on adjustment to stress: experimental evidence. Journal of Personality and Social Psychology, 92, 458–475. 10.1037/0022-3514.92.3.458 [DOI] [PubMed] [Google Scholar]
- Brenowitz WK, Kukull WA, Beresford SAA, Monsell SE, & Williams EC (2014). Social relationships and risk of incident mild cognitive impairment in U.S. Alzheimer’s Disease Centers. Alzheimer’s Disease and Associated Disorders, 28, 253–260. 10.1097/WAD.0000000000000020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody E (1971) ‘Excess disabilities of mentally impaired aged: Impact of individualized treatment’, The Gerontologist, 25, 124–133. 10.1093/geront/11.2_Part_1.124 [DOI] [PubMed] [Google Scholar]
- Conrad CD & Bimonte-Nelson HA (2010). Impact of the hypothalamic-pituitary-adrenal/gonadal axes on trajectory of age-related cognitive decline. Progress in Brain Research, 182, 31–76. 10.1016/S0079-6123(10)82002-3 [DOI] [PubMed] [Google Scholar]
- Crooks VC, Lubben J, Petitti DB, Little D, & Chiu V (2008). Social network, cognitive function, and dementia incidence among elderly women. American Journal of Public Health, 98(1), 1221–1227. 10.2105/AJPH.2007.115923 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Frias CM, Dixon RA, & Bäckman L (2003). Use of memory compensation strategies is related to psychosocial and health indictors. Journal of Gerontology: Psychological Sciences, 58, 12–22. 10.1093/geronb/58.1.P12 [DOI] [PubMed] [Google Scholar]
- de Kloet ER, Oitzl MS, Joëls M (1999). Stress and cognition: Are corticosteroids good or bad guys? Trends in Neurosciences, 22, 422–426. 10.1016/S0166-2236(99)01438-1 [DOI] [PubMed] [Google Scholar]
- de Souza-Talarico JN, Marin MF, Sindi S, & Lupien SJ (2011). Effects of stress hormones on the brain and cognition: evidence from normal to pathological aging. Dementia & Neuropsychologia, 5, 8–16. 10.1590/S1980-57642011DN05010003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellwardt L, Aarsten M, Deeg D, & Steverink N (2013). Does loneliness mediate the relation between social support and cognitive functioning in later life? Social Sciences & Medicine, 98, 116–124. 10.1016/j.socscimed.2013.09.002 [DOI] [PubMed] [Google Scholar]
- English T, & Carstensen LL (2014). Selective narrowing of social networks across adulthood is associated with improved emotional experience in daily life. International Journal of Behavioral Development, 38(2), 195–202. 10.1177/0165025413515404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ertel KA, Glymour MM, & Berkman LF (2008). Effects of social integration on preserving memory function in a nationally representative US elderly population. American Journal of Public Health, 98, 1215–1220. 10.2105/AJPH.2007.113654 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fankhauser S, Maercker A, & Forstmeier S (2017). Social network and cognitive functioning in old age: Self-efficacy as a mediator? Zeitschriftfur Gerontologie und Geriatrie, 50, 123–131. 10.1007/s00391-016-1178-y [DOI] [PubMed] [Google Scholar]
- Fratiglioni L, Wang H, Ericsson K, Maytan M, & Winblad B (2000). Influence of social network on occurrence of dementia: A community-based longitudinal study. The Lancet, 355(9212), 1315–1319. 10.1016/S0140-6736(00)02113-9 [DOI] [PubMed] [Google Scholar]
- Frith E, & Loprinzi PD (2017). Soial support and cogntive function in older adults. Best Practices in Mental Health, 13, 41–49. [Google Scholar]
- Fiori KL, Antonucci TC, & Cortina KS (2006). Social network typologies and mental health among older adults. Journal of Gerontology: Psychological Sciences, 61B, 25–32. 10.1093/geronb/61.1.P25 [DOI] [PubMed] [Google Scholar]
- Fuller-Iglesias HR, Webster NJ, & Antonucci TC (2015). The complex nature of family support across the lifespan: Implications for psychological well-being. Developmental Psychology, 51, 277–288. 10.1037/a0038665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gleason EJ, Iida M, Shrout PE, & Bolger N (2008). Receiving support as a mixed blessing: Evidence for dual effects of support on psychological outcomes. Journal of Personality and Social Psychology, 94, 824–938. 10.1037/0022-3514.94.5.824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gow AJ, Corley J, Starr JM, & Deary IJ (2012). Reverse causation in activity-cognitive ability associations: The Lothian birth cohort 1936. Psychology and Aging, 27, 250–255. 10.1037/a0024144. [DOI] [PubMed] [Google Scholar]
- Gow AJ, & Mortensen EL (2016). Social resources and conitive ageing across 30 years: the Glostrup 1914 Cohort. Age and Ageing, 45, 480–486. 10.1093/ageing/afw070 [DOI] [PubMed] [Google Scholar]
- Haslam C, Cruwys T, Milne M, Kan CH, & Haslam SA (2016). Group ties protect cognitive health by promoting social identification and social support. Journal of Aging and Health, 28, 244–266. 10.1177/0898264315589578 [DOI] [PubMed] [Google Scholar]
- Head D, Singh T, & Bugg JM (2012). The moderating role of exercise on stres-related effects on the hippocampus and memory in later adulthood. Neuropsychology, 26, 133–143. 10.1037/a0027108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill PL, Payne BR, Jackson JJ, Stine-Morrow EA, & Roberts BW (2014). Perceived social support predicts increased conscientiousness during older adulthood. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 69, 543–547. doi: 10.1093/geronb/gbt024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holwerda TJ, Beekman AT, Deeg DJ, Stek ML, van Tilburg TG, Visser PJ, Schmand B, Jonker C, & Schoevers RA (2012). Increased risk mortality associated with social isolation in older men: Only when feeling lonely? results from the amsterdam study of the eldery (AMSTEL). Psychological Medicine, 42, 843–853. 10.1017/S0033291711001772 [DOI] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. [Google Scholar]
- Huxhold O, Miche M, & Shuz B (2013). Benefits of having friends in older ages: Differential effects of informal social activities on well-being in middle-aged and older adults. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 69, 366–375. 10.1093/geronb/gbt029 [DOI] [PubMed] [Google Scholar]
- Hultsch DF, Hertzog C, Small BJ, & Dixon RA (1999). Use it or lose it: Engaged lifestyle as a buffer of cognitive decline in aging? Psychology and Aging, 14, 245–263. 10.1037/0882-7974.14.2.245 [DOI] [PubMed] [Google Scholar]
- Jonaitis E, La Rue A, Mueller KD, Koscik RL, Hermann B, & Sager MA (2013). Cognitive activities and cognitive performance in middle-aged adults at risk for Alzheimer’s disease. Psychology and Aging, 28, 1004–1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahn RL & Antonucci TC (1980). Convoys over the life course: Attachment, roles, and social support In Baltes PBand Grim OG(Eds.) Lifespan Development and Behavior (3rd ed) (pp. 253–286). New York City, New York: US: Elsevier Academic Press. [Google Scholar]
- Kats M, Patel MD, Palta P, Meyer ML, Gross AL, Whitsel EA, Knopman D, Alonso A, Mosley TH, & Heiss G, (2016). Social support and cognition in a community-based cohort: The atherosclerosis risk in communities (ARIC) study. Age and Ageing, 45, 475–480. 10.1093/ageing/afw060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, Glaser R, Cacioppo JT, MacCallum RC, Snydersmith M, Kim C, Malarkey WB (1997). Martial conflict in older adults: Endocrinological and immunological correlates. Psychosomatic Medicine, 59, 339–349. 10.1097/00006842-199707000-00001 [DOI] [PubMed] [Google Scholar]
- Koyanagi A, Oh H, Vancampfort D, Carvalho AF, Veronese N, Stubbs B, & Lara E (2018). Perceived stress and mild cognitive impairment among 32,715 community-dwelling older adults across six low- and middle-income countries. Gerontology. doi: 10.1159/000492177. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- La Fleur C, & Salthouse TA (2017). Which aspects of social support are associated with which cognitive abilities for which people? The Journals of Gerontology: Psychological Sciences, 72, 1006–1016. 10.1093/geronb/gbv119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lachman ME, Neupert SD, & Agrigoroaei S (2011). The relevance of control beliefs for health and aging In Schaie KW& Willis SL(Eds)., The handbooks of aging consisting of three vols. Handbook of the psychology of aging (pp.175–190). Sand Diego, CA US: Elsevier Academic Press. [Google Scholar]
- Larson R, Mannell R, & Zuzanek J (1986). Daily well-being of older adults with friends and family. Psychology and Aging, 1, 117–126. 10.1037//0882-7974.1.2.117 [DOI] [PubMed] [Google Scholar]
- Li M, & Dong X (2017). Is social network a protective factor for cognitive impairment in US Chinese older adults? Findings from the pine study. Gerontology. 10.1159/000485616 [DOI] [PubMed] [Google Scholar]
- Livingston G, Sommerlad A, Orgeta V, Costafreda SG, Huntley J, … & Mukadam N. (2017). Dementia prevention, intervention, and care. Lancet, 390, 2673–2674. 10.1016/S0140-6736(17)31363-6 [DOI] [PubMed] [Google Scholar]
- Luescher K, Pillemer K (1998). Intergenerational ambivalence: A new approach to the study of parent-child relations in later life. Journal of Marriage and the Family, 60, 413–425. 10.2307/35858 [DOI] [Google Scholar]
- Mehedi Hasan KM, Rahman S, Arif KMT, & Sobhani ME (2012). Psychological stress and aging: role of glucocorticoids (GCs). Age, 34, 1421–1433. 10.1007/s11357-011-9319-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller LMS, & Gagne DD (2005). Effects of age and control beliefs on resource allocation during reading. Aging, Neuropsychology, and Cognition, 12, 129–148. 10.1080/13825580590925161 [DOI] [Google Scholar]
- Mousavi-Nasab SM, Kormi-Nouri R, Sundstrom A, & Nilsson LG (2012). The effects of marital status on episodic and semantic memory in healthy middle-aged and old individuals. Scandinavian Journal of Psychology, 53, 1–8. 10.1111/j.1467-9450.2011.00926.x [DOI] [PubMed] [Google Scholar]
- Muthén LK., & Muthén BO. (2007). Mplus User’s Guide (Sixth Edition). Los Angeles, CA: Muthen & Muthen. [Google Scholar]
- Newsom JT, Rook KS, Nishishiba M, Sorkin DH, & Mahan TL (2005). Understanding the relative importance of positive and negative social exchanges: Examining specific domains and appraisals. Journal of Gerontology: Psychological Sciences, 60B, 304–312. 10.1093/geronb/60.6.P304 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ofstedal MB, Fisher GG, & Herzog AR (2005). Documentation of cognitive functioning measures in the Health and Retirement Study. HRS Documentation Report DR-006. Retrieved from https://hrs.isr.umich.edu/sites/default/files/biblio/dr-006.pdf
- Porta M(ed). (2008). A Dictionary of Epidemiology. Oxford University Press, New York, NY. [Google Scholar]
- Radloff LS. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurements, 1, 385–401. [Google Scholar]
- Rafnsson SB, Orrell M, d’Orsi E, Hogervorst E, & Steptoe A (2017). Loneliness, Social Integration, and Incident Dementia Over 6 Years: Prospective Findings from the English Longitudinal Study of Ageing. Journals of Gerontology: Social Sciences. 10.1093/geronb/gbx087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rook KS, (2001). Emotional health and positive versus negative social exchanges: A daily diary analysis, Applied Developmental Science, 5, 86–97. 10.1207/S1532480XADS0502_4 [DOI] [Google Scholar]
- Roberts SGB & Dunbar RIM (2011). Communication in social networks: Effects of kinship, network size, and emotional closeness. Personal Relationships, 18, 439–452. 10.1111/j.1475-6811.2010.01310.x [DOI] [Google Scholar]
- Sandi C (2007). Memory impairments associated with stress and aging In Bermúdez-Rattoni F(ed). Neural Plasticity and Memory: From Genes to Brain Imaging. Boca Raton (FL): CRC Press/Taylor & Francis, ch. 12. [PubMed] [Google Scholar]
- Schuster TL, Kessler RC, & Aseltine RH Jr. (1990). Supportive interactions, negative interactions, and depressed mood. American Journal of Community Psychology, 18, 423–438. 10.1007/BF00938116 [DOI] [PubMed] [Google Scholar]
- Seeman TE, Lusignolo TM, Albert M, & Berkman L (2001). Social relationships, social support, and patterns of cognitive aging in healthy, high-functioning older adults: MacArthur studies of successful aging. Health Psychology, 20, 243–255. 10.1037/0278-6133.20.4.243 [DOI] [PubMed] [Google Scholar]
- Seeman TE, Miller-Martinez DM, Merkin SS, Lachman ME, Tun PA, & Karlamangla AS (2011). Histories of social engagement and adult cognition: Midlife in the U.S. study. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences, 66B, 141–152. 10.1093/geronb/gbq091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharifian N, Manly JJ, Brickman AM, & Zahodne LB (submitted) Social network characteristics and cognitive functioning in ethnically diverse older adults: The role of network size and composition. Manuscript submitted for publication. [DOI] [PMC free article] [PubMed]
- Shiovitz-Ezra S, & Litwin H (2012). Social network type and health-related behaviors: Evidence from an American national survey. Social Science & Medicine, 75, 901–904. 10.1016/j.socsci.med.2012.04.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silverstein M, Chen X, & Heller K (1996). Too much of a good thing? Intergenerational social support and the psychological well-being of older parents. Journal of Marriage and Family, 58, 970–982. 10.2307/353984 [DOI] [Google Scholar]
- Sonnega A, Weir DR .(2014). The health and retirement study: a public data resource for research on aging. Open Health Data, 2, e7 10.5334/0hd.am [DOI] [Google Scholar]
- Sörman D, Rönnlund M, Sundström A, Norberg M, & Nilsson LG (2017). Social network size and cognitive functioning in middle-aged adults: cross-sectional and longitudinal associations. Journal of Adult Development, 24, 77–88. 10.1007/sl0804-016-9248-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stawski RS, Mogle JA, & Sliwinski MJ (2013). Associations among fluid and crystallized cognition and daily stress processes in older adults. Psychology and Aging, 28, 57–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turner RJ, Frankel G, & Levin DM (1983). Social support: Conceptualization, measurement, and implications for mental health In Greenley JR& Simmons RG(Eds.), Research in Community andMental Health (pp. 67–111). Greenwich: JAI Press. [Google Scholar]
- Van Achterberg T, Huisman-de Waal GGJ, Ketelaar NABM, Oostendorp RA, Jacobs JE, & Wollersheim HCH (2011). How to promote healthy behaviours in patients? An overview of evidence for behaviour change techniques. Health Promotion International, 26, 148–162. 10.1093/heapro/daq050 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Gelder BM, Tijhuis M, Kalmijn S, Giampaoli S, Nissinen A, & Kromout D (2006). Marital status and living situation during a 5-year period are associated with a subsequent 10-year cognitive decline in older men: the FINE Study. Journal of Gerontology: Social Sciences, 61, P213–P219. 10.1093/geronb/61.4.P213 [DOI] [PubMed] [Google Scholar]
- Waite L, & Gallagher M (2002). The case for marriage: Why married people are happier, healthier and better off financially. New York, NY: Broadway Books. [Google Scholar]
- Wang B, He P, & Dong B (2015). Associations between social networks, social contacts, and cognitive function among Chinese nonagenarians/centenarians. Archives of Gerontology and Geriatrics, 60, 522–527. 10.1016/j.archger.2015.01.002 [DOI] [PubMed] [Google Scholar]
- Windsor TD, Gerstorf D, Pearson E, Ryan L, & Anstey KJ (2014). Positive and negative social exchanges and cognitive aging in young-old adults: Differential associations across family, friend, and spouse domains. Psychology and Aging, 29, 28–43. 10.1037/a0035256 [DOI] [PubMed] [Google Scholar]
- Wethington E, & Kessler RC (1986). Perceived support, received support, and adjustment to stressful life events. Journal of Health and Social Behavior, 27, 78–89. doi: 10.2307/2136504 [DOI] [PubMed] [Google Scholar]
- Xu M, Thomas PA, & Umbersson D (2016). Marital quality and cognitive limitations in late life. Journal of Gerontology Series B: Psychological Sciences and Social Sciences, 71, 165–176. 10.1093/geronb/gbv014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zahodne LB, Watson CW-M, Seehra S, & Martinez M (2018). Positive psychosocial factors and cognition in ethnically diverse older adults. Journal of the International Neuropsychological Society, 24, 294–304. 10.1017/S1355617717000935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zissimopoulos J, Crimmins E, & St. Clair P (2014). The value of delaying Alzheimer’s disease onset. Forum for Health Economics and Policy, 18, 25–39. [DOI] [PMC free article] [PubMed] [Google Scholar]