

Introduction
Consumption of high calorie/low nutrition (HCLN) foods, as well as increased levels of sedentary behavior (SB), have been associated with unhealthy levels of childhood weight gain and increased risk for obesity (Davison et al., 2001; Mitchell, J. A. et al., 2013; Prentice-Dunn et al., 2012). Over 18.4% of school-aged youth six to eleven are considered obese in the United States (Kumar et al., 2017), and are more likely than their normal weight peers to develop high cholesterol and blood pressure, prediabetes, bone and joint problems, asthma, and cancer later in life (Freedman et al., 2007; Must et al., 2006; Tanofsky-Kraff et al., 2011). Compared to their normal weight peers, overweight or obese children show significantly faster weight gain into adolescence and are more likely to be overweight or obese once reaching adulthood (Buscot et al., 2018; Field et al., 2005; Herman et al., 2009; McGinty et al., 2018; Singh et al., 2008).
Executive Function (EF) typically refers to a collection of inter-related processes that requires effortful, top-down control of action, attention, regulation of behavior and emotions, associated with neural systems involving the prefrontal cortex (Anderson, 2002; Müller et al., 2015; Zelazo et al., 2002). However, neural regions implicated in EF do not fully mature until late adolescence and into early adulthood (Ames et al., 2014; Casey et al., 1997; Gogtay et al., 2004), leaving children and adolescents vulnerable to engaging in behaviors that require effortful initiation or inhibition, including high calorie low/nutrition food intake and high levels of SB (Bechara et al., 2006; Francis et al., 2009; Guerrieri et al., 2008; Nederkoorn et al., 2006; Stacy, Ames, & Knowlton, 2004). Problems or deficits in inhibition have been found to increase the risk for unhealthy eating and increased SB in children in a number of investigations (Guerrieri et al., 2008; Nederkoorn et al., 2006). For example, a study by Francis and Sussman found that children with a compromised ability to inhibit behavior had higher weight and faster weight gain compared to children with higher levels of inhibition (Francis et al., 2009). Further, components of EF may play a role in the initiation of HCLN eating and sedentary behavior. Working memory capacity enables individuals to maintain attention and focus, and may work in concert with other executive processes such as inhibitory and emotional control (Riggs, N. et al., 2010). Put another way, working memory can guide attention toward or away from food-related cues in the environment, thus inhibiting or facilitating their behavior (Davidson et al., 2019; Higgs et al., 2018). Strong emotional impulses may also play a role in HCLN and SB, as negative mood states have shown to increase food intake among children and adolescents (Tice et al., 2001), as well as sedentary behavior (Aparicio et al., 2016; Isasi et al., 2013).
While past research has shown a relationship between EF, HCLN eating, and SB, to our knowledge, no study has examined if early patterns of EF can potentially predict long term patterns of obesity risk among children. Little is known about whether latent subgroups of EF exist in this population, and if these subgroups predict longitudinal patterns of unhealthy eating and sedentary behavior that may, in turn, represent greater or lesser risk for obesity. The current study applied a mixture model based on a latent transition analysis framework (Nylund-Gibson et al., 2014) to ascertain whether latent profiles (Gibson, 1959) of EF in early childhood predicted longitudinal profiles of HCLN eating and SB. It was hypothesized that low EF at baseline would predict an increased likelihood of engaging in long term HCLN eating and SB. Further model testing explored the influence of covariates on the relationship between EF and longitudinal patterns of HCLN eating and SB.
Method
The data included in this analysis were collected as part of a large, randomized controlled trial designed for the prevention of multiple health risk behaviors. Twenty-eight Southern California elementary schools in two large districts were matched on school-level demographic characteristics (e.g., ethnicity, socioeconomic status), and randomly assigned by pair within each district to an EF training program or a delayed intervention control group for obesity risk prevention (Sakuma et al., 2012). Participants were assessed at four measurement periods across three years, all receiving the same assessments. At baseline, 1,005 fourth grade students and their parents signed assent and active consent forms for participation in this study according to procedures approved by the university institutional review board. Of the 1,005, 296 were removed from the sample due to either moving out of the study area (n=249, 85%), declining assent at a follow-up assessment (n=18, 6%), or being absent on an assessment day (n=29, 10%). Thus, the final sample used in this analysis consisted of 709 fourth through sixth grade students, half of whom were female (50.1%), with a mean age 9.27 years (range eight to eleven years) (see Table 1). Participants that were removed from analysis did not differ greatly from the remaining population, with the exception that they were more likely to be Hispanic (33% vs. 26%; p<.05) and low SES (35% vs. 21%; p<.001).
Table 1.
Descriptive statistics for 709 students from 29 schools
| Grade, assessment, and variable | Statistics |
|---|---|
| 4th Grade: Initial Assessment | |
| Gender, n (%) | |
| Male | 354 (49.9%) |
| Female | 355 (50.1%) |
| Ethnicity, n (%) | |
| Hispanic | 182 (25.7%) |
| Non-Hispanic | 527 (74.3%) |
| Socioeconomic Status, n (%) | |
| Received a Free Lunch at School | 148 (20.9%) |
| Did Not Receive a Free Lunch at School | 561 (79.1%) |
| Intervention Assignment, n (%) | |
| Intervention | 377 (53.2%) |
| Control | 332 (46.8%) |
| Behavioral Rating Inventory of Executive Function, mean (SD) | |
| Emotion Regulation | 1.6 (0.4) |
| Inhibitory Control | 1.6 (0.4) |
| Working Memory | 1.7 (0.4) |
| Organization of Materials | 1.7 (0.4) |
| High Calorie/Low Nutrition Consumption, mean (SD) | 2.4 (1.0) |
| Sedentary Behavior, mean (SD) | 2.6 (1.3) |
| 4th Grade: 6-Month Follow-Up Assessment | |
| High Calorie/Low Nutrition Consumption, mean (SD) | 2.3 (0.9) |
| Sedentary Behavior, mean (SD) | 2.5 (1.2) |
| 5th Grade: 18-Month Follow-Up Assessment | |
| High Calorie/Low Nutrition Consumption, mean (SD) | 2.3 (0.9) |
| Sedentary Behavior, mean (SD) | 2.7 (1.2) |
| 6th Grade: 30-Month Follow-Up Assessment | |
| High Calorie/Low Nutrition Consumption, mean (SD) | 2.2 (0.9) |
| Sedentary Behavior, mean (SD) | 2.7 (1.2) |
Measures
High calorie/low nutrition.
Eating behavior was assessed using five items from the State and Local Youth Risk Behavior Survey (YRBSS, α= 0.80) which asked questions related to HCLN intake (Brener et al., 2013). Specifically, each item asked ‘How often to do you eat…’ and then listed a specific food or drink such as french-fries, potato chips, doughnuts, pastries, candy, or non-diet soda. Response option were 1= Less than once a week, 2= Once a week, 3= 2-3 times a week, 4= 4-6 times a week, 5= Once a day, and 6= 2 or more of these a day.
Sedentary behavior.
Population SB was assessed utilizing a previously validated three-item measure (α= 0.68), which assessed the number of hours spent playing video games, watching television, or using a computer outside of school (Hoelscher et al., 2003). Questions asked “On a regular school day, how many hours per day do you usually…” and listed “watch TV or video movies at home or away from school”, “spend on the computer at home or away from school”, and “spend playing video games that you sit down and play like PlayStation, Xbox, GameBoy, or arcade games”. The seven response options were 1= I don’t, 2= 1 hour, 3= 2 hours, 4= 3 hours, 5= 4 hours, 6= 5 hours, 7= 6 more hours.
Executive function.
Items from the Behavioral Rating Inventory of Executive Function, Self-Report (BRIEF-SR) were used to assess EF in participants (Guy et al., 2004). The BRIEF was designed to measure EF in every-day situations among school-age children as young as fourth grade (Harris et al., 2016; Riggs et al., 2012). Specifically, BRIEF measures two broad areas of EF: behavioral regulation, the ability to shift, and modulate emotions and behavior via appropriate inhibitory control; and metacognition, the ability to cognitively self-manage tasks and monitor performance (Gioia et al., 2002). Due to time-constraints imposed by participating schools for in-class survey administration, 23 items from four clinical subscales of EF representing working memory, behavioral inhibition, emotional regulation, and organization of materials were selected as part of survey measures, which have been used in previous studies investigating the association between executive function and various health outcomes (Harris et al., 2016; Pentz et al., 2013; Pentz et al., 2015; Riggs et al., 2012; Warren et al., 2017). For each item, participants were asked “In the past month, how often has each of the following behaviors been a problem?”, with item response choices 1 = Never, 2 = Sometimes, 3 = Often. An example item for the working memory subscale is “I forget what I am doing in the middle of things”, inhibitory control is “I get out of control more than my friends”, emotional control is “I yell, scream, or cry for no reason” and organization of materials is “my desk/workspace is a mess”. Previous work using this same population found the abbreviated BRIEF-SR scale to demonstrate predictive validity when compared to the full scale (Riggs et al., 2010). Sub-scales and items were selected using the highest loading index items from a pilot study that demonstrated acceptable internal consistency (αs=0.63 to 0.74) when compared to full BRIEF scales (Riggs et al., 2010; Riggs et al., 2010).
Covariates.
Gender, ethnicity, and socioeconomic status were included as potential covariates based on prior research that has shown some differences in obesity risk among these variables (Singh et al. 2010). Dichotomous variables were created for gender (male vs. female), ethnicity (Hispanic vs. non-Hispanic), and socioeconomic status (received a free lunch at school vs. did not receive a free lunch at school). Intervention condition assignment was also included as a potential covariate as it may have influenced HLCN eating and SB.
Analysis Plan
Intra-class correlational analyses revealed that up to 3.7% of the variation in HCLN consumption and 7.5% of the variation in SB could be attributed to random effects at the school level. To adjust for similarities between students attending the same school, a clustering variable indicating the school each student attended was included in all statistical models. Standard errors robust to non-independence were estimated for each model. Full-information maximum likelihood was employed to account for missing data (Graham, 2009; Little et al., 2014), although no variable in the sample of 709 students had more than 2% of the data missing.
A latent profile analysis (LPA) was conducted to identify subgroups of similar students based on the means of the four subscales of EF that were measured at the baseline assessment (Lubke et al., 2005). To select the most plausible number of subgroups, a series of models were tested with between one and four profiles. Each model employed 5,000 random sets of starting values, 20 iterations at the initial stage, and 100 final stage optimizations. The best fitting model was selected (Collins et al., 2010; Nylund et al., 2007) by monitoring changes in Akaike’s Information Criterion (AIC; Akaike, 1987) and sample size adjusted Bayesian Information Criterion (SSA-BIC; (Sclove, 1987) with the goal of identifying the point at which the indices reached a minimum value or an “elbow” representing the last relatively large decrease (Collins et al., 2010; Nylund et al., 2007). The Lo-Mendell-Rubin test (LMR) and the bootstrap likelihood ratio test (BLRT) were also utilized to assess model fit (Lo et al., 2001; McCutcheon, 1987; McLachlan et al., 2000). With these tests, a statistically significant p value suggests that adding a latent profile improves model fit; a p value that is not statistically significant indicates that a more parsimonious model with fewer latent profiles will provide a better fit to the data. Once the number of subgroups in the LPA model was determined, the procedure was then replicated to perform a repeated measures latent profile analysis (RMLPA) using the means of the five-item measure of HCLN consumption and the mean of the three-item measure of SB. Responses from the initial assessment, as well as the 6-month, 18-month, and 30-month follow-up assessments, were used in the RMLPA model to identify longitudinal latent profiles.
After the final LPA and RMLPA models were selected, the three-step method (Asparouhov et al., 2014; Vermunt, 2017) was employed to regress the longitudinal latent profiles of HCLN consumption and SB on the initial latent profiles of EF (Nylund-Gibson et al., 2014). The first regression model was unconditional and determined the probability that students from a specific latent profile of EF would transition to a longitudinal latent profile of HCLN eating and SB. The second regression model integrated covariates (see Figure 1) to assess whether gender, ethnicity, socioeconomic status, and intervention condition changed the probability that a student from an EF latent profile would transition to a longitudinal HCLN/SB latent profile. All analysis was conducted using Mplus 8.2 software (Muthén et al., 2018).
Fig. 1.
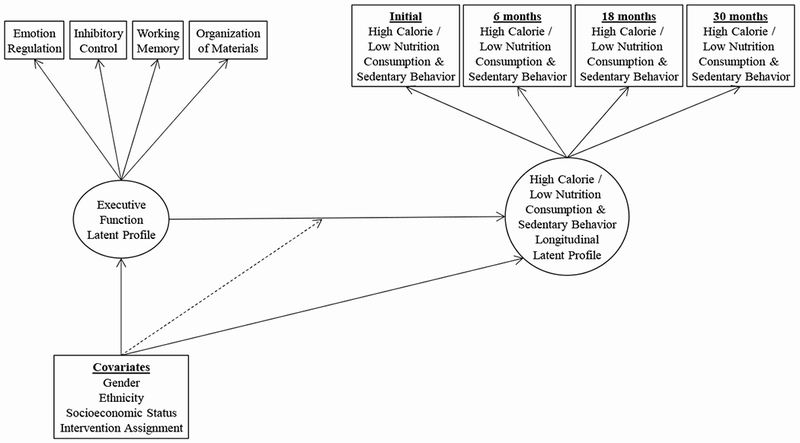
Visual depiction of model utilizing a latent transition framework.
Results
In the LPA of EF, AIC and SSA-BIC declined sharply in the first three models and tapered off in fourth model (see Table 2). The LMR and BLRT were statistically significant in the third model but not the fourth model, suggesting the model with three latent profiles (see Figure 2) provided the best fit the data. The first profile was labeled High EF and consisted of 35.2% of the sample. The EF subscale means within this latent subgroup ranged from 1.3 to 1.4, with lower scores representing higher levels of executive function. The second profile was labeled Medium EF, comprised 47.7% of the sample, and had subscale means that varied from 1.6 to 1.7. The third profile was labeled Low EF, made up of 17.1% of the sample, and had subscale means between 2.1 and 2.2.
Table 2.
Summary of information used to determine latent profiles.
| 1 Profile | 2 Profiles | 3 Profiles | 4 Profiles | |
|---|---|---|---|---|
| A. Executive Function | ||||
| AIC | 2914.599 | 2173.439 | 1987.441 | 1922.695 |
| SSA-BIC | 2925.708 | 2191.491 | 2012.436 | 1954.633 |
| LMR (p) | - | <.001 | .006 | .057 |
| BLRT (p) | - | <.001 | .007 | .061 |
| B. High Calorie/Low Nutrition Consumption and Sedentary Behavior | ||||
| AIC | 17032.512 | 15808.065 | 15406.562 | 15232.650 |
| SSA-BIC | 17054.730 | 15842.781 | 15453.775 | 15292.360 |
| LMR (p) | - | .006 | .115 | .326 |
| BLRT (p) | - | .006 | .119 | .331 |
Note: AIC = Akaike’s Information Criterion, SSA-BIC = Sample size adjusted Bayesian Information Criterion, LMR (p) = p value of Lo-Mendell-Rubin test, and BLRT (p) = p value of bootstrap likelihood ratio test.
Fig. 2.
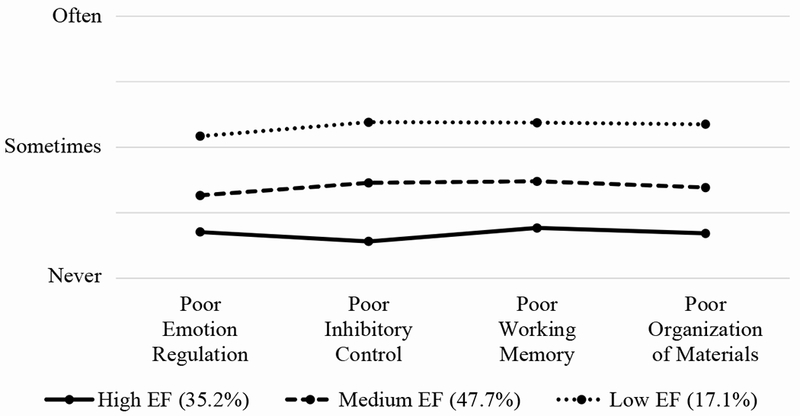
Visual depiction of latent profiles of executive function (EF) at the initial assessment.
In the RMLPA of HCLN consumption and SB, there was a sizable decrease in the AIC and SSA-BIC in the model with two longitudinal latent profiles and a modest decrease in the models with three and four longitudinal latent profiles. The LMR and BLRT were statistically significant in the model with two profiles but not three or four profiles. The model with two longitudinal latent profiles was therefore selected as the final model (see Figure 3). The first longitudinal profile consisted of 17.2% of the sample, and was labeled High HCLN/SB to reflect the higher levels of HCLN consumption and SB reported at each assessment period. The second longitudinal profile, which exhibited lower levels of HCLN consumption and SB at each assessment, was labeled Low HCLN/SB and constituted 82.8% of the sample.
Fig. 3.
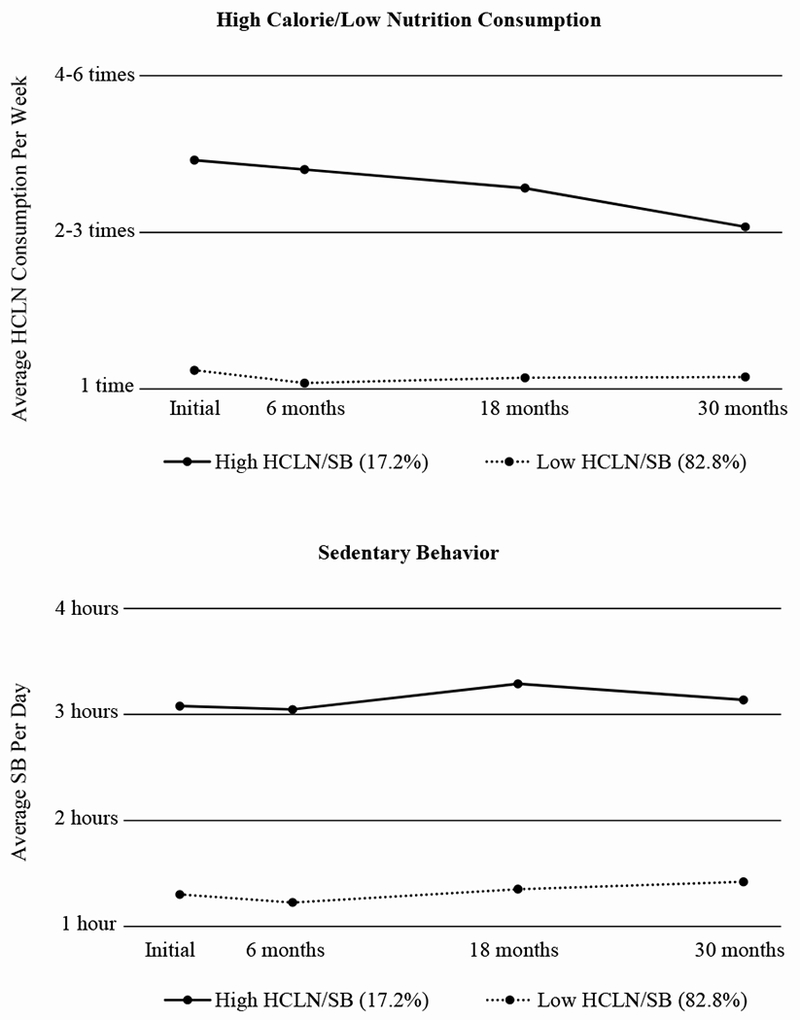
Visual depiction of longitudinal latent profiles of high calorie/low nutrition (HCLN) consumption and sedentary behavior (SB) across four assessment periods.
The three-step method was used to estimate the probability that students from each latent profile of EF would transition to the High HCLN/SB longitudinal profile. The unconditional regression model revealed that students in the Low EF latent profile had a 32% chance of transitioning to the High HCLN/SB longitudinal profile. Students in the Medium EF and High EF latent profiles had a 14% and 15% chance, respectively.
The regression model with covariates (see Table 3) indicated that students with low SES were less likely to be in the Medium EF latent profile compared to the Low EF latent profile (OR = 0.37, 95% CI = 0.19 to 0.71, p = .003). Socioeconomic status also increased the probability that a student in the High EF latent profile would transition to the High HCLN/SB longitudinal profile (OR = 4.55, 95% CI = 1.59 to 13.01, p = .005). The model also showed that males in the High EF latent profile had higher odds of transitioning to the High HCLN/SB longitudinal profile (OR = 2.74, 95% CI = 1.11 to 6.78, p = . 029), with even greater odds for males in the Low EF latent profile (OR = 11.88, 95% CI = 2.63 to 53.74, p = .001). Further, males were less likely to be in the High EF latent profile compared to the Low EF latent profile (OR = 0.60, 95% CI = 0.37 to 0.99, p = .045).
Table 3.
Odds ratios depicting the effect of covariates.
| Executive Function | Covariates | OR | [95% CI] | p |
|---|---|---|---|---|
| A. Effects of Covariates on Executive Function Latent Profile | ||||
| Low | Gender (Male) | Reference | ||
| Ethnicity (Hispanic) | ||||
| SES (Free Lunch) | ||||
| Intervention Assignment | ||||
| Medium | Gender (Male) | 0.72 | [0.43, 1.20] | .206 |
| Ethnicity (Hispanic) | 1.71 | [0.87, 3.37] | .118 | |
| SES (Free Lunch) | 0.37 | [0.19, 0.71] | .003 | |
| Intervention Assignment | 1.11 | [0.66, 1.87] | .681 | |
| High | Gender (Male) | 0.60 | [0.37, 0.99] | .045 |
| Ethnicity (Hispanic) | 1.72 | [0.92, 3.23] | .090 | |
| SES (Free Lunch) | 0.64 | [0.36, 1.15] | .135 | |
| Intervention Assignment | 1.99 | [1.20, 3.29] | .007 | |
| B. Effects of Covariates on Relationship Between Executive Function Latent Profile and High Calorie/Low Nutrition Consumption and Sedentary Behavior Latent Profile | ||||
| Low | Gender (Male) | 11.88 | [2.63, 53.74] | .001 |
| Ethnicity (Hispanic) | 1.14 | [0.23, 5.68] | .877 | |
| SES (Free Lunch) | 2.95 | [0.86, 10.08] | .084 | |
| Intervention Assignment | 0.72 | [0.24, 2.16] | .561 | |
| Medium | Gender (Male) | 2.28 | [0.97, 5.35] | .058 |
| Ethnicity (Hispanic) | 1.19 | [0.37, 3.8] | .767 | |
| SES (Free Lunch) | 1.61 | [0.41, 6.35] | .499 | |
| Intervention Assignment | 0.43 | [0.17, 1.1] | .078 | |
| High | Gender (Male) | 2.74 | [1.11, 6.78] | .029 |
| Ethnicity (Hispanic) | 1.36 | [0.46, 3.98] | .576 | |
| SES (Free Lunch) | 4.55 | [1.59, 13.01] | .005 | |
| Intervention Assignment | 1.86 | [0.66, 5.28] | .241 | |
Note: Depicts the odds of belonging to the high HCLN/SB longitudinal latent profile as compared to the low HCLN/SB longitudinal latent profile. SES = Socio-economic status.
Discussion
To our knowledge, this investigation is the first to identify latent profiles of EF in children and to use a latent transition analysis framework to determine the effect of these profiles on longitudinal HCLN consumption and SB. Executive control functions are a set of neuro-cognitive skills that allow an individual to problem solve, as well as engage in self-regulation and impulse control (Fishbein et al., 2009). Results showed support for the initial hypothesis, indicating that participants who had low EF at baseline assessment had a significantly higher probability of transitioning to a latent subgroup that regularly engaged in high HCLN consumption and frequent sedentary behavior. These results are in line with findings from prior investigations into the relationship between EF, eating, and physical activity (Ames et al., 2014; Ames et al., 2016; Francis et al., 2009; Goldschmidt et al., 2018; Nederkoorn et al., 2006; Riggs, N. et al., 2010; Riggs et al., 2003; Riggs et al., 2012; van Praag, 2009; Willoughby et al., 2018).
Several potential explanations tying into EF exist that may, in part, help explain these findings. First, it is possible that coming into contact with highly salient environmental or internal stimuli may trigger a pre-potent response to engage in a particular behavior. In other words, cues associated with an appetitive behavior can come to trigger a relatively automatic pattern of activation in memory, which may overwhelm regulatory control processes, thus allowing a behavioral response to occur without much thought or introspection (Stacy, Ames, & Leigh, 2004; Stacy et al., 2010; Wiers et al., 2007). Thus, executive control processes such as working memory capacity and behavioral inhibition become essential when facing relevant cues, potentially dampening or diminishing their influence (Friese et al., 2008; Hofmann et al., 2008; Hofmann et al., 2007; Houben, 2011; Houben et al., 2010; Nederkoorn et al., 2010). Second, it is possible that poor higher order organizational and intentional planning skills may lead to a diminished ability to organize healthy goals or appropriately weigh outcomes when executing decisions (Riggs et al., 2010; Riggs et al., 2012). Third, poor emotional regulation (i.e., the ability to cognitively control strong emotional impulses) may increase HCLN eating, as the relationship between negative mood states and increased food intake is well researched (Evers et al., 2010; Harrist et al., 2013; Tice et al., 2001). Unfortunately, executive control functions require greater cognitive resources that children may not be developmentally able to muster, and thus become easier to overwhelm (Grenard et al., 2008; Stacy et al., 2010). Investigations into neurodevelopment timelines have shown neural regions associated with executive control (i.e., frontal cortical regions) do not begin to fully mature until early adolescence (Gogtay et al., 2004). Taken together, these results may provide evidence that enhancing cognitive control directly or indirectly (Müller et al., 2015), or modifying environmental conditions to reduce EF demand (Allan et al., 2015), beginning early in childhood could be helpful in strengthening long term health behaviors. Several direct interventions already have attempted training various components of specific EF components among child and adolescent populations with promising results (Ames et al., 2016; Grenard et al., 2007; Houben, 2011; Houben et al., 2012; Houben et al., 2015; Pentz et al., 2016; Riggs et al., 2006; Verbeken et al., 2013). Further, several indirect interventions, which focus on more global self-regulatory enhancement compared to training specific EF components, have been shown to be effective in enhancing EF over time (Diamond, 2012; Diamond et al., 2011). For example, the Promoting Alternative Thinking Strategies (PATHS) emphasizes the integration of affect, behavior, and cognition, and has been shown to promote inhibitory control among seven-through nine-year olds (Greenberg et al., 1995; Riggs et al., 2006). Additionally, mindfulness training has shown support in enhancing the more controlled regulatory processes in children (Pentz et al., 2016; Zelazo et al., 2012). Nonetheless, future research could help clarify the long-term effect of EF training (both direct and indirect) on negative health behaviors.
The current study also investigated whether covariates changed the probability of transitioning to a longitudinal latent subgroup. Results indicated that being male significantly increased the probability that a student would engage in high levels of HCLN consumption and SB. While speculative, it is possible these results can be attributed to general differences in eating behavior between sexes. Specifically, investigations into childhood diet have shown a difference between the daily amount of sugar consumed by boys compared to girls (Ervin et al., 2012), and that after age nine, males preferred and consumed greater quantities of sweet foods than females of the same age (Cooke et al., 2007; Desor et al., 1975; Desor et al., 1987; Greene et al., 1975). Further investigation among children is needed to understand gender differences with respect to eating behavior and physical activity, and how these differences may be exacerbated by varying levels of neurocognitive functioning and development.
Students from a lower socioeconomic status also had a higher probability of transitioning into the high HCLN consumption and SB profile. For these students, it may be possible that high calorie snack foods are more readily available compared to healthy food alternatives such as fruit and vegetables (Powell et al., 2007). Further, children and adolescents from low income families may also live in environments where physical activity is more restricted (Hoyos Cillero et al., 2010; Jin et al., 2015). For example, an investigation into childhood SB in Southern California found that lower income children watched more hours of television per day, had less access to physical activity equipment, and were more likely to have restrictions on outdoor physical activity (Tandon et al., 2012). Based on these findings, it is plausible that various environment conditions, such as neighborhood disorganization and access to safe physical activity venues, can have an influence over child behavior.
Limitations and Strengths of the Current Study
There were several limitations to the present study. First, EF, HCLN consumption, and SB were only measured over a period of 30 months. It is possible that due to rapidly maturing neural structures (Gogtay et al., 2004), EF and HCLN/SB behaviors may change post-middle school. However, the stability of these outcomes in our sample, as well as past research showing childhood weight influences adolescent and adult weight, may provide evidence early EF can have a marked impact on future eating and physical activity behaviors. Future assessments conducted over a longer timeframe may provide additional insight into the influence that EF has on longitudinal behavioral patterns that begin in childhood. Univariate and multivariate growth curve models and growth mixture models may be particularly useful in identifying long-term trends associated with EF. Second, due to feasibility issues at study locations, laboratory-based measures of EF such as Self Ordered Pointing Task or Go-No/Go were not used. The BRIEF survey, used in their place, was designed to capture real-world behavioral manifestations of EF through measurement of day-to-day behavior (Gioia et al., 2002; Guy et al., 2004). Typically, this measure has been used when various participant or setting constraints prohibit the use of laboratory tasks. While some researchers argue that performance-based and rating measures of executive function assess different underlying mental constructs (Toplak et al., 2013), previous investigations have found the BRIEF adequately measures the components of EF under investigation in this study (Kenworthy et al., 2008; Mahone et al., 2002; Mangeot et al., 2002; Nadebaum et al., 2007). Nevertheless, future research should utilize more robust laboratory-based measures of EF to further clarify the relationship between EF and trajectories of SB/HCLN. Finally, the SB measure used in this study does not capture non-screen based sedentary behaviors (e.g., reading, doing homework). However, a strong link between high levels of screen time and obesity has been well documented (Mitchell, J.A. et al., 2013; Robinson et al., 2017), with large increases in usage first observed in children as they transition between elementary and middle school (Twenge et al., 2018). Regardless, future investigations into sedentary behavior could include non-screen behaviors to generate a more complete picture of child and adolescent health.
Conclusions
The results of this study help further our understanding of the interplay between executive control processes and eating/sedentary behavior among children and early adolescents. The population under investigation is at the early stages of setting long-term behaviors that put them at greater risk of developing negative health outcomes, such as becoming overweight or obese. Given these risks, a goal of future interventions might be to train individuals with lower EF across multiple domains (i.e., inhibition, working memory, etc.) over the long term to adopt alternative means of regulating behavior or engaging in appropriate decision-making. Indeed, a few interventions have demonstrated that adequate cognitive training has been key to reducing risky behaviors (Bickel et al., 2011; Fiore et al., 2000; Kalichman et al., 2000; Sussman et al., 2004), and two meta-analysis has shown that, at least over the short term, inhibition training shows small but significant effects in reducing negative health behaviors (Allom et al., 2016; Jones et al., 2016). Simultaneously, steps could be taken to enhance environmental conditions so that high levels of EF would not be required for children to make healthy decisions (Allan et al., 2015). Collectively, these two approaches may help reduce the probability that children will engage in unhealthy behaviors that become lifelong habits. Future research remains necessary to determine what, if any, long-term effects these efforts may have over health behaviors.
Supplementary Material
Research Highlights.
Diet and sedentary behavior are major factors in childhood and adult obesity.
Neurocognitive factors may highlight risk to developing obesity in childhood.
Executive function is linked to long-term habits of eating and sedentary behavior.
Acknowledgments
Role of Funding Source
This research was supported by grant T32CA009492, HD 052107 (NICHD, NIDA; Pentz, P.I.), and is registered at ClinicalTrials.gov (#). The NICHD and NIDA had no role in the design of the study, collection, analysis and interpretation of data, or in the writing of the report.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of Interest
None
References
- Akaike H (1987). Factor analysis and AIC. Psychometrika, 52, 317–332. doi: 10.1007/978-1-4612-1694-0_29 [DOI] [Google Scholar]
- Allan JL, Johnston M, & Campbell N (2015). Snack purchasing is healthier when the cognitive demands of choice are reduced: A randomized controlled trial. Health Psychology, 34(7), 750–755. doi: 10.1037/hea0000173 [DOI] [PubMed] [Google Scholar]
- Allom V, Mullan B, & Hagger M (2016). Does inhibitory control training improve health behaviour? A meta-analysis. Health Psychol Rev, 10(2), 168–186. doi: 10.1080/17437199.2015.1051078 [DOI] [PubMed] [Google Scholar]
- Ames SL, Kisbu-Sakarya Y, Reynolds KD, Boyle S, Cappelli C, Cox MG, … Stacy AW (2014). Inhibitory control effects in adolescent binge eating and consumption of sugar-sweetened beverages and snacks. Appetite, 81, 180–192. doi: 10.1016/j.appet.2014.06.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ames SL, Wurpts IC, Pike JR, MacKinnon DP, Reynolds KR, & Stacy AW (2016). Self-regulation interventions to reduce consumption of sugar-sweetened beverages in adolescents. Appetite, 105, 652–662. doi: 10.1016/j.appet.2016.06.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson P (2002). Assessment and development of executive function (EF) during childhood. Child Neuropsychol, 8(2), 71–82. doi: 10.1076/chin.8.2.71.8724 [DOI] [PubMed] [Google Scholar]
- Aparicio E, Canals J, Arija V, De Henauw S, & Michels N (2016). The role of emotion regulation in childhood obesity: implications for prevention and treatment. Nutr Res Rev, 29(1), 17–29. doi: 10.1017/S0954422415000153 [DOI] [PubMed] [Google Scholar]
- Asparouhov T, & Muthén B (2014). Auxiliary Variables in Mixture Modeling: Three-Step Approaches Using Mplus. Structural Equation Modeling: A Multidisciplinary Journal, 21(3), 329–341. doi: 10.1080/10705511.2014.915181 [DOI] [Google Scholar]
- Bechara A, Noël X, & Crone E (2006). Loss of willpower: Abnormal neural mechanisms of impulse control and decision making in addiction Handbook of implicit cognition and addiction (1 ed., pp. 215–232). Thousand Oaks: SAGE Publications. [Google Scholar]
- Bickel WK, Yi R, Landes RD, Hill PF, & Baxter C (2011). Remember the future: working memory training decreases delay discounting among stimulant addicts. Biol Psychiatry, 69(3), 260–265. doi: 10.1016/j.biopsych.2010.08.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brener ND, Kann L, Shanklin S, Kinchen S, Eaton DK, Hawkins J, & Flint K (2013). Methodology of the Youth Risk Behavior Surveillance System — 2013. Retrieved from [PubMed] [Google Scholar]
- Buscot MJ, Thomson RJ, Juonala M, Sabin MA, Burgner DP, Lehtimaki T, … Magnussen CG (2018). BMI Trajectories Associated With Resolution of Elevated Youth BMI and Incident Adult Obesity. Pediatrics, 141(1). doi: 10.1542/peds.2017-2003 [DOI] [PubMed] [Google Scholar]
- Casey BJ, Trainor RJ, Orendi JL, Schubert AB, Nystrom LE, Giedd JN, … Rapoport JL (1997). A Developmental Functional MRI Study of Prefrontal Activation during Performance of a Go-No-Go Task. J Cogn Neurosci, 9(6), 835–847. doi: 10.1162/jocn.1997.9.6.835 [DOI] [PubMed] [Google Scholar]
- Collins LM, & Lanza ST (2010). Latent class and latent transition analysis: With applications in the social, behavioral, and health sciences (Vol. 718): John Wiley & Sons. [Google Scholar]
- Cooke LJ, & Wardle J (2007). Age and gender differences in children’s food preferences. British Journal of Nutrition, 93(05). doi: 10.1079/bjn20051389 [DOI] [PubMed] [Google Scholar]
- Davidson TL, Jones S, Roy M, & Stevenson RJ (2019). The Cognitive Control of Eating and Body Weight: It’s More Than What You “Think”. Front Psychol, 10, 62. doi: 10.3389/fpsyg.2019.00062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davison KK, & Birch LL (2001). Childhood overweight: a contextual model and recommendations for future research. Obesity Reviews, 2(3), 159–171. doi: 10.1046/j.1467-789x.2001.00036.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desor J, Greene L, & Maller O (1975). Preferences for sweet and salty in 9- to 15-year-old and adult humans. Science, 190(4215), 686–687. doi: 10.1126/science.1188365 [DOI] [PubMed] [Google Scholar]
- Desor JA, & Beauchamp GK (1987). Longitudinal changes in sweet preferences in humans. Physiology & Behavior, 39(5), 639–641. doi: 10.1016/0031-9384(87)90166-1 [DOI] [PubMed] [Google Scholar]
- Diamond A (2012). Activities and Programs That Improve Children’s Executive Functions. Curr Dir Psychol Sci, 21(5), 335–341. doi: 10.1177/0963721412453722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diamond A, & Lee K (2011). Interventions shown to aid executive function development in children 4 to 12 years old. Science, 333(6045), 959–964. doi: 10.1126/science.1204529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ervin RB, Kit BK, Carroll MD, & Ogden CL (2012). Consumption of added sugar among U.S. children and adolescents, 2005-2008 NCHS data brief no 87. Hyattsville, MD: National Center for Health Statistics; 2012 (2156–5376 (Electronic) 2161–8313 (Linking)) Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/22797997 [Google Scholar]
- Evers C, Marijn Stok F, & de Ridder DT (2010). Feeding your feelings: emotion regulation strategies and emotional eating. Pers Soc Psychol Bull, 36(6), 792–804. doi: 10.1177/0146167210371383 [DOI] [PubMed] [Google Scholar]
- Field AE, Cook NR, & Gillman MW (2005). Weight status in childhood as a predictor of becoming overweight or hypertensive in early adulthood. Obes Res, 13(1), 163–169. doi: 10.1038/oby.2005.21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiore MC, Bailey WC, Cohen SJ, Dorfman SF, Goldstein MG, Gritz ER, & Wewers ME (2000). Treating tobacco dependence and use: Clinical practice guideline. Rockville, MD: US Department of Health and Human Services, Public Health Service. [Google Scholar]
- Fishbein D, & Tarter R (2009). Infusing neuroscience into the study and prevention of drug misuse and co-occurring aggressive behavior. Subst Use Misuse, 44(9-10), 1204–1235. doi: 10.1080/10826080902959975 [DOI] [PubMed] [Google Scholar]
- Francis LA, & Susman EJ (2009). Self-regulation and rapid weight gain in children from age 3 to 12 years. Arch Pediatr Adolesc Med, 163(4), 297–302. doi: 10.1001/archpediatrics.2008.579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman DS, Mei Z, Srinivasan SR, Berenson GS, & Dietz WH (2007). Cardiovascular risk factors and excess adiposity among overweight children and adolescents: the Bogalusa Heart Study. J Pediatr, 150(1), 12–17 e12. doi: 10.1016/j.jpeds.2006.08.042 [DOI] [PubMed] [Google Scholar]
- Friese M, Hofmann W, & Wanke M (2008). When impulses take over: moderated predictive validity of explicit and implicit attitude measures in predicting food choice and consumption behaviour. Br J Soc Psychol, 47(Pt 3), 397–419. doi: 10.1348/014466607X241540 [DOI] [PubMed] [Google Scholar]
- Gibson WA (1959). Three multivariate models: Factor analysis, latent structure analysis, and latent profile analysis. J Psychometrika, 24(3), 229–252. [Google Scholar]
- Gioia GA, Isquith PK, Retzlaff PD, & Espy KA (2002). Confirmatory factor analysis of the Behavior Rating Inventory of Executive Function (BRIEF) in a clinical sample. Child Neuropsychol, 8(4), 249–257. doi: 10.1076/chin.8.4.249.13513 [DOI] [PubMed] [Google Scholar]
- Gogtay N, Giedd JN, Lusk L, Hayashi KM, Greenstein D, Vaituzis AC, … Thompson PM (2004). Dynamic mapping of human cortical development during childhood through early adulthood. Proc Natl Acad Sci U S A, 707(21), 8174–8179. doi: 10.1073/pnas.0402680101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldschmidt AB, O’Brien S, Lavender JM, Pearson CM, Le Grange D, & Hunter SJ (2018). Executive functioning in a racially diverse sample of children who are overweight and at risk for eating disorders. Appetite, 724, 43–49. doi: 10.1016/j.appet.2017.03.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham JW (2009). Missing data analysis: making it work in the real world. Annu Rev Psychol, 60, 549–576. doi: 10.1146/annurev.psych.58.110405.085530 [DOI] [PubMed] [Google Scholar]
- Greenberg MT, Kusche C, Cook ET, & Quamma JP (1995). Promoting emotional competence in school-aged children: The effects of the PATHS curriculum. Emotions in Developmental Psychopathology(1). [Google Scholar]
- Greene LS, Desor J, & Maller O (1975). Heredity and experience: their relative importance in the development of taste preference in man. Journal of Comparative and Physiological Psychology, 89(3), 279. [DOI] [PubMed] [Google Scholar]
- Grenard JL, Ames SL, Wiers RW, Thush C, Stacy AW, & Sussman S (2007). Brief intervention for substance use among at-risk adolescents: a pilot study. J Adolesc Health, 40(2), 188–191. doi: 10.1016/j.jadohealth.2006.08.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grenard JL, Ames SL, Wiers RW, Thush C, Sussman S, & Stacy AW (2008). Working memory capacity moderates the predictive effects of drug-related associations on substance use. Psychol Addict Behav, 22(3), 426–432. doi: 10.1037/0893-164X.22.3.426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guerrieri R, Nederkoorn C, & Jansen A (2008). The interaction between impulsivity and a varied food environment: its influence on food intake and overweight. Int J Obes (Lond), 32(4), 708–714. doi: 10.1038/sj.ijo.0803770 [DOI] [PubMed] [Google Scholar]
- Guy SC, Gioia GA, & Isquith PK (2004). BRIEF-SR: Behavior rating inventory of executive function--self-report version: Professional manual: Psychological Assessment Resources. [Google Scholar]
- Harris MH, Gold DR, Rifas-Shiman SL, Melly SJ, Zanobetti A, Coull BA, … Oken E (2016). Prenatal and childhood traffic-related air pollution exposure and childhood executive function and behavior. Neurotoxicol Teratol, 57, 60–70. doi: 10.1016/j.ntt.2016.06.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrist AW, Hubbs-Tait L, Topham GL, Shriver LH, & Page MC (2013). Emotion regulation is related to children’s emotional and external eating. J Dev Behav Pediatr, 34(8), 557–565. doi: 10.1097/DBP.0b013e3182a5095f [DOI] [PubMed] [Google Scholar]
- Herman KM, Craig CL, Gauvin L, & Katzmarzyk PT (2009). Tracking of obesity and physical activity from childhood to adulthood: the Physical Activity Longitudinal Study. Int J Pediatr Obes, 4(4), 281–288. doi: 10.3109/17477160802596171 [DOI] [PubMed] [Google Scholar]
- Higgs S, & Spetter MS (2018). Cognitive Control of Eating: the Role of Memory in Appetite and Weight Gain. Curr Obes Rep, 7(1), 50–59. doi: 10.1007/s13679-018-0296-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoelscher DM, Day RS, Kelder SH, & Ward JL (2003). Reproducibility and validity of the secondary level School-Based Nutrition Monitoring student questionnaire. J Am Diet Assoc, 103(2), 186–194. doi: 10.1053/jada.2003.50031 [DOI] [PubMed] [Google Scholar]
- Hofmann W, Gschwendner T, Friese M, Wiers RW, & Schmitt M (2008). Working memory capacity and self-regulatory behavior: toward an individual differences perspective on behavior determination by automatic versus controlled processes. J Pers Soc Psychol, 95(4), 962–977. doi: 10.1037/a0012705 [DOI] [PubMed] [Google Scholar]
- Hofmann W, Rauch W, & Gawronski B (2007). And deplete us not into temptation: Automatic attitudes, dietary restraint, and self-regulatory resources as determinants of eating behavior. Journal of Experimental Social Psychology, 43(3), 497–504. doi: 10.1016/j.jesp.2006.05.004 [DOI] [Google Scholar]
- Houben K (2011). Overcoming the urge to splurge: influencing eating behavior by manipulating inhibitory control. J Behav Ther Exp Psychiatry, 42(3), 384–388. doi: 10.1016/j.jbtep.2011.02.008 [DOI] [PubMed] [Google Scholar]
- Houben K, Havermans RC, Nederkoorn C, & Jansen A (2012). Beer a no-go: learning to stop responding to alcohol cues reduces alcohol intake via reduced affective associations rather than increased response inhibition. Addiction, 107(7), 1280–1287. doi: 10.1111/j.1360-0443.2012.03827.x [DOI] [PubMed] [Google Scholar]
- Houben K, & Jansen A (2015). Chocolate equals stop. Chocolate-specific inhibition training reduces chocolate intake and go associations with chocolate. Appetite, 87, 318–323. doi: 10.1016/j.appet.2015.01.005 [DOI] [PubMed] [Google Scholar]
- Houben K, Roefs A, & Jansen A (2010). Guilty pleasures. Implicit preferences for high calorie food in restrained eating. Appetite, 55(1), 18–24. doi: 10.1016/j.appet.2010.03.003 [DOI] [PubMed] [Google Scholar]
- Hoyos Cillero I, & Jago R (2010). Systematic review of correlates of screen-viewing among young children. PrevMed, 51(1), 3–10. doi: 10.1016/j.ypmed.2010.04.012 [DOI] [PubMed] [Google Scholar]
- Isasi CR, Ostrovsky NW, & Wills TA (2013). The association of emotion regulation with lifestyle behaviors in inner-city adolescents. Eat Behav, 14(4), 518–521. doi: 10.1016/j.eatbeh.2013.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jin Y, & Jones-Smith JC (2015). Associations between family income and children’s physical fitness and obesity in California, 2010-2012. Prev Chronic Dis, 12, E17. doi: 10.5888/pcd12.140392 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones A, Di Lemma LC, Robinson E, Christiansen P, Nolan S, Tudur-Smith C, & Field M (2016). Inhibitory control training for appetitive behaviour change: A meta-analytic investigation of mechanisms of action and moderators of effectiveness. Appetite, 97, 16–28. doi: 10.1016/j.appet.2015.11.013 [DOI] [PubMed] [Google Scholar]
- Kalichman SC, Benotsch E, Suarez T, Catz S, Miller J, & Rompa D (2000). Health literacy and health-related knowledge among persons living with HIV/AIDS. American Journal of Preventive Medicine, 18(4), 325–331. [DOI] [PubMed] [Google Scholar]
- Kenworthy L, Yerys BE, Anthony LG, & Wallace GL (2008). Understanding executive control in autism spectrum disorders in the lab and in the real world. Neuropsychol Rev, 18(4), 320–338. doi: 10.1007/s11065-008-9077-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumar S, & Kelly AS (2017). Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin Proc, 92(2), 251–265. doi: 10.1016/j.mayocp.2016.09.017 [DOI] [PubMed] [Google Scholar]
- Little R, & Rubin DB (2014). Statistical analysis with missing data: John Wiley & Sons. [Google Scholar]
- Lo Y, Mendell NR, & Rubin DB (2001). Testing the number of components in a normal mixture. Biometrika, 88(3), 767–778. [Google Scholar]
- Lubke GH, & Muthen B (2005). Investigating population heterogeneity with factor mixture models. Psychol Methods, 10(1), 21–39. doi: 10.1037/1082-989X.10.1.21 [DOI] [PubMed] [Google Scholar]
- Mahone EM, Cirino PT, Cutting LE, Cerrone PM, Hagelthorn KM, Hiemenz JR, … Denckla MB (2002). Validity of the behavior rating inventory of executive function in children with ADHD and/or Tourette syndrome. Archives of Clinical Neuropsychology, 17(1), 643–662. doi: 10.1093/arclin/17.7.643 [DOI] [PubMed] [Google Scholar]
- Mangeot S, Armstrong K, Colvin AN, Yeates KO, & Taylor HG (2002). Long-term executive function deficits in children with traumatic brain injuries: assessment using the Behavior Rating Inventory of Executive Function (BRIEF). Child Neuropsychol, 5(4), 271–284. doi: 10.1076/chin.8.4.271.13503 [DOI] [PubMed] [Google Scholar]
- McCutcheon AL (1987). Latent class analysis: Sage. [Google Scholar]
- McGinty SM, Osganian SK, Feldman HA, Milliren CE, Field AE, & Richmond TK (2018). BMI Trajectories from Birth to Young Adulthood. Obesity (Silver Spring), 26(6), 1043–1049. doi: 10.1002/oby.22176 [DOI] [PubMed] [Google Scholar]
- McLachlan GJ, & Peel D (2000). Finite Mixture Models (1994/01/01 ed). New York, NY: John Wiley & Sons, Inc. [Google Scholar]
- Mitchell JA, Pate RR, Beets MW, & Nader PR (2013). Time spent in sedentary behavior and changes in childhood BMI: a longitudinal study from ages 9 to 15 years. Int J Obes (Lond), 37(1), 54–60. doi: 10.1038/ijo.2012.41 [DOI] [PubMed] [Google Scholar]
- Mitchell JA, Rodriguez D, Schmitz KH, & Audrain-McGovern J (2013). Greater screen time is associated with adolescent obesity: a longitudinal study of the BMI distribution from ages 14 to 18. 21(3), 572–575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Müller U, & Kerns K (2015). The development of executive function. Handbook of child psychology and developmental science, 7, 571–623. [Google Scholar]
- Must A, & Anderson SE (2006). Body mass index in children and adolescents: considerations for population-based applications. Int J Obes (Lond), 30(4), 590–594. doi: 10.1038/sj.ijo.0803300 [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2018). Mplus software (Version 8). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Nadebaum C, Anderson V, & Catroppa C (2007). Executive function outcomes following traumatic brain injury in young children: a five year follow-up. Dev Neuropsychol, 32(2), 703–728. doi: 10.1080/87565640701376086 [DOI] [PubMed] [Google Scholar]
- Nederkoorn C, Braet C, Van Eijs Y, Tanghe A, & Jansen A (2006). Why obese children cannot resist food: the role of impulsivity. Eat Behav, 7(4), 315–322. doi: 10.1016/j.eatbeh.2005.11.005 [DOI] [PubMed] [Google Scholar]
- Nederkoorn C, Houben K, Hofmann W, Roefs A, & Jansen A (2010). Control yourself or just eat what you like? Weight gain over a year is predicted by an interactive effect of response inhibition and implicit preference for snack foods. Health Psychol, 29(4), 389–393. doi: 10.1037/a0019921 [DOI] [PubMed] [Google Scholar]
- Nylund KL, Asparouhov T, & Muthén BO (2007). Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569. doi: 10.1080/10705510701575396 [DOI] [Google Scholar]
- Nylund-Gibson K, Grimm R, Quirk M, & Furlong M (2014). A Latent Transition Mixture Model Using the Three-Step Specification. Structural Equation Modeling: A Multidisciplinary Journal, 21(3), 439–454. doi: 10.1080/10705511.2014.915375 [DOI] [Google Scholar]
- Pentz MA, & Riggs NR (2013). Longitudinal relationships of executive cognitive function and parent influence to child substance use and physical activity. Prev Sci, 14(3), 229–237. doi: 10.1007/s11121-012-0312-3 [DOI] [PubMed] [Google Scholar]
- Pentz MA, Riggs NR, & Warren CM (2016). Improving substance use prevention efforts with executive function training. Drug Alcohol Depend, 163 Suppl 1, S54–59. doi: 10.1016/j.drugalcdep.2016.03.001 [DOI] [PubMed] [Google Scholar]
- Pentz MA, Shin H, Riggs N, Unger JB, Collison KL, & Chou CP (2015). Parent, peer, and executive function relationships to early adolescent e-cigarette use: a substance use pathway? Addict Behav, 42, 73–78. doi: 10.1016/j.addbeh.2014.10.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Powell LM, Slater S, Mirtcheva D, Bao Y, & Chaloupka FJ (2007). Food store availability and neighborhood characteristics in the United States. Prev Med, 44(3), 189–195. doi: 10.1016/j.ypmed.2006.08.008 [DOI] [PubMed] [Google Scholar]
- Prentice-Dunn H, & Prentice-Dunn S (2012). Physical activity, sedentary behavior, and childhood obesity: a review of cross-sectional studies. Psychol Health Med, 17(3), 255–273. doi: 10.1080/13548506.2011.608806 [DOI] [PubMed] [Google Scholar]
- Riggs N, Chou CP, Spruijt-Metz D, & Pentz MA (2010). Executive cognitive function as a correlate and predictor of child food intake and physical activity. Child Neuropsychol, 16(3), 279–292. doi: 10.1080/09297041003601488 [DOI] [PubMed] [Google Scholar]
- Riggs NR, Blair CB, & Greenberg MT (2003). Concurrent and 2-year longitudinal relations between executive function and the behavior of 1st and 2nd grade children. Child Neuropsychol, 9(4), 267–276. doi: 10.1076/chin.9.4.267.23513 [DOI] [PubMed] [Google Scholar]
- Riggs NR, Greenberg MT, Kusche CA, & Pentz MA (2006). The mediational role of neurocognition in the behavioral outcomes of a social-emotional prevention program in elementary school students: effects of the PATHS Curriculum. Prev Sci, 7(1), 91–102. doi: 10.1007/s11121-005-0022-1 [DOI] [PubMed] [Google Scholar]
- Riggs NR, Spruijt-Metz D, Chou CP, & Pentz MA (2012). Relationships between executive cognitive function and lifetime substance use and obesity-related behaviors in fourth grade youth. Child Neuropsychol, 15(1), 1–11. doi: 10.1080/09297049.2011.555759 [DOI] [PubMed] [Google Scholar]
- Riggs NR, Spruijt-Metz D, Sakuma KL, Chou CP, & Pentz MA (2010). Executive cognitive function and food intake in children. J Nutr Educ Behav, 42(6), 398–403. doi: 10.1016/j.jneb.2009.11.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson TN, Banda JA, Hale L, Lu AS, Fleming-Milici F, Calvert SL, & Wartella E (2017). Screen Media Exposure and Obesity in Children and Adolescents. Pediatrics, 140(Suppl 2), S97–S101. doi: 10.1542/peds.2016-1758K [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sakuma KL, Riggs NR, & Pentz MA (2012). Translating evidence based violence and drug use prevention to obesity prevention: development and construction of the pathways program. Health Educ Res, 27(2), 343–358. doi: 10.1093/her/cyr095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sclove SL (1987). Application of model-selection criteria to some problems in multivariate analysis. Psychometrika, 52(3), 333–343. doi: 10.1007/bf02294360 [DOI] [Google Scholar]
- Singh AS, Mulder C, Twisk JW, van Mechelen W, & Chinapaw MJ (2008). Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev, 9(5), 474–488. doi: 10.1111/j.1467-789X.2008.00475.x [DOI] [PubMed] [Google Scholar]
- Stacy AW, Ames SL, & Knowlton BJ (2004). Neurologically Plausible Distinctions in Cognition Relevant to Drug Use Etiology and Prevention. Substance Use & Misuse, 39(10-12), 1571–1623. doi: 10.1081/lsum-200033204 [DOI] [PubMed] [Google Scholar]
- Stacy AW, Ames SL, & Leigh BC (2004). An implicit cognition assessment approach to relapse, secondary prevention, and media effects. Cognitive and Behavioral Practice, 11(2), 139–149. [Google Scholar]
- Stacy AW, & Wiers RW (2010). Implicit cognition and addiction: a tool for explaining paradoxical behavior. Annu Rev Clin Psychol, 6(1), 551–575. doi: 10.1146/annurev.clinpsy.121208.131444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sussman S, Earleywine M, Wills T, Cody C, Biglan T, Dent CW, & Newcomb MD (2004). The motivation, skills, and decision-making model of “Drug Abuse” 1 prevention. Subst Use Misuse, 39(10–12), 1971–2016. [DOI] [PubMed] [Google Scholar]
- Tandon PS, Zhou C, Sallis JF, Cain KL, Frank LD, & Saelens BE (2012). Home environment relationships with children’s physical activity, sedentary time, and screen time by socioeconomic status. Int J Behav Nutr Phys Act, 9, 88. doi: 10.1186/1479-5868-9-88 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanofsky-Kraff M, Shomaker LB, Olsen C, Roza CA, Wolkoff LE, Columbo KM, … Yanovski JA (2011). A prospective study of pediatric loss of control eating and psychological outcomes. J Abnorm Psychol, 120(1), 108–118. doi: 10.1037/a0021406 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tice DM, Bratslavsky E, & Baumeister RF (2001). Emotional distress regulation takes precedence over impulse control: If you feel bad, do it! Journal of Personality and Social Psychology, 80(1), 53–67. doi: 10.1037/0022-3514.80.1.53 [DOI] [PubMed] [Google Scholar]
- Toplak ME, West RF, & Stanovich KE (2013). Practitioner review: do performance-based measures and ratings of executive function assess the same construct? J Child Psychol Psychiatry, 54(2), 131–143. doi: 10.1111/jcpp.12001 [DOI] [PubMed] [Google Scholar]
- Twenge JM, Martin GN, & Campbell WK (2018). Decreases in psychological well-being among American adolescents after 2012 and links to screen time during the rise of smartphone technology. [DOI] [PubMed] [Google Scholar]
- van Praag H (2009). Exercise and the brain: something to chew on. Trends Neurosci, 32(5), 283–290. doi: 10.1016/j.tins.2008.12.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verbeken S, Braet C, Goossens L, & van der Oord S (2013). Executive function training with game elements for obese children: A novel treatment to enhance self-regulatory abilities for weight-control. Behaviour research and therapy, 51(6), 290–299. doi: 10.1016/j.brat.2013.02.006 [DOI] [PubMed] [Google Scholar]
- Vermunt JK (2017). Latent Class Modeling with Covariates: Two Improved Three-Step Approaches. Political Analysis, 18(04), 450–469. doi: 10.1093/pan/mpq025 [DOI] [Google Scholar]
- Warren CM, Riggs NR, & Pentz MA (2017). Longitudinal relationships of sleep and inhibitory control deficits to early adolescent cigarette and alcohol use. J Adolesc, 57, 31–41. doi : 10.1016/j.adolescence.2017.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiers RW, Bartholow BD, van den Wildenberg E, Thush C, Engels RC, Sher KJ, … Stacy AW (2007). Automatic and controlled processes and the development of addictive behaviors in adolescents: a review and a model. Pharmacol Biochem Behav, 86(2), 263–283. doi: 10.1016/j.pbb.2006.09.021 [DOI] [PubMed] [Google Scholar]
- Willoughby MT, Wylie AC, & Catellier DJ (2018). Testing the association between physical activity and executive function skills in early childhood. Early Childhood Research Quarterly, 44, 82–89. doi: 10.1016/j.ecresq.2018.03.004 [DOI] [Google Scholar]
- Zelazo P, & Müller U (2002). Executive functioning in typical and atypical children In Goswami U (Ed.), Blackwell Handbook of childhood cognitive development (2nd ed., pp. 574–603). [Google Scholar]
- Zelazo PD, & Lyons KE (2012). The Potential Benefits of Mindfulness Training in Early Childhood: A Developmental Social Cognitive Neuroscience Perspective. Child Development Perspectives, 6(2), 154–160. doi: 10.1111/j.1750-8606.2012.00241.x [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.