

Abstract
Background:
Tongue cancer is the most common malignancy of the mouth. In recent decades, reported tongue cancer incidence and mortality rates have increased all over the world while survival has not improved that sometimes is related to mutation, especially in gene P53 (such R249, R248 mutations). Hence, this study aimed to identification of R249 mutation in P53 gene of tumor tissue in tongue cancer.
Methods:
In a cross-sectional study, 48 patients with squamous cell carcinoma (SCC) of tongue were selected, and mutation of R249 was investigated in sample of tumors. In addition, demographic data and medical history of patients were determined and registered in a collected data form. Finally added data were entered to computer and analyzed by SPSS software.
Results:
Polymerase-chain reaction test done on tissue samples from cancer patients showed that in a studied sample of 48 patients, 4 of them (8.3%) had R249 mutation. After selecting the codon 249 as a hotspot in oral cancer, forward and reverse primers for amplification of exon 7 were obtained from the articles.
Conclusions:
Considering the findings of our study, R249 mutation in P53 gene in patients with SCC is relatively high. Age and alcohol consumption were factors affecting incidence of the mutation. It is necessary to take an early treatment with a single lesion of tongue to prevent severe disease and prevent disease in patient's family with screening test and prevent cancer in future with gene therapy.
Keywords: Gene P53, mutation and R249, tongue squamous cell carcinoma
Introduction
After heart disease, cancer is the most common cause of death in the world, and unfortunately, the number of patients with malignant lesions is growing. This may be due to the development of detection methods, increasing life expectancy, and most importantly progresses in industries, technology, machine life, smoking, drugs and chemicals side effects and environmental pollution. Nowadays, head and neck cancer is the world's fifth most common cancer and it is more common in the Middle East.
Nearly, 485,000 new cases of oral cancer are diagnosed annually and more than 260,000 deaths due to this disease have been reported.[1] Close to 94% of oral cancers are in squamous cell carcinoma (SCC).[2] The global map of the prevalence of oral cancer is between 20 and 36.3 per 100,000 population.[3] The older, more likely to engage the oral floor and will be even worse to be pro-diagnosed.[4] According to most sources, the prevalence of cancer in men is higher than women's tongue. Other studies have shown that genetic mutations play a major role in the incidence of cancers of the mouth, especially the tongue SCC and in this regard, P53 gene mutation is more important. Carcinogens include genetic and environmental factors that are causing cancer cells by damaging and malfunction of the genome. Meanwhile, proto-oncogene genes alternations make cells out-of-control. The inhibiting activity of tumor suppressor genes, such as P53, leads to the removal of the natural growth, and tumor cells are formed and that would end up with the progress of this process that become tumor metastasis and cancer.[5] P53 protein by interrupting G1 phase of the cell cycle gives the opportunity to DNA repair factor to repair damaged DNA. However, if DNA damage is not repaired, these proteins accelerate the process of apoptosis and cell death. These proteins inhibit angiogenesis in tumor cells and prevent uncontrolled growth of cells. Certainly, P53 gene mutations and defects in the P53 protein cause cancer.[6,7,8] P53 gene is located on the short arm of the chromosome 17 and comprised 11 exons 10 introns. Exon 1 and a large part of exon 11 in P53 gene do not code in the mRNA, however, the hotspot region gene located on exons 8–5 and more than 90% of the mutations are happened on this region.[9,10,11] So far, several studies in different parts of the world in relation to the importance and the vital role of P53 gene mutations in development of different cancers have been done, and a wide range of frequency of these mutations (from zero to 70% of patients) is seen and that reflects the diversity, abundance, and the role of these gene mutations in causing the disease in different ethnic groups and populations, but several studies have been conducted on the expression of this gene in tongue cancer.[12] According to the statistics, during the last 10 years, the number of people who were suffering from tongue cancer and referred to the health centers and hospitals for treatment in the Isfahan province in Iran has increased.
The study of gene expression in a family practically has the property to help early diagnosis of tongue cancer along with other risk factors. Hence, it is necessary that the patients' family be informed about health risk of gene P53 and take an early and appropriate treatment with a single lesion (preventive property). In the near future, gene therapy will be used (preventive therapy) and it also will improve the prognosis of the patients (3th level preventive medicine). This gene is effective in over 50% of all malignancies in the body and mutations. In addition, the gene increases the risk of other synchronous malignancies. However, due to what mentioned and given that the study of P53 gene mutations in squamous cell tongues cancer has not been done in Iran so far, this study was carried out to identify mutation R249 in P53 gene in patients with tongue SCC.
Methods
This study is a cross-sectional study which was done between 2014 and 2015 at 2 big and overcrowded centers in Isfahan, Iran: Al-Zahra and Kashani hospitals. The study population consisted of patients with tongue SCC, and they were hospitalized or had surgery in the mentioned centers. Included criteria were SCC definitive diagnosis of tongue cancer, the availability of patient records, and pathology specimens of patients. An excluded criterion was the impossibility of identifying the R249 mutation of the P53 gene in samples for different reasons.
The sampling method for collection data was through census of patients who were treated and enrolled during the last 5 years between 2014 and 2015 in mentioned centers in Iran. The procedure was that after the acceptance of the proposal and coordination, initially, demographic data of patients with tongue SCC; who were hospitalized in teaching centers, were reviewed, and were reported in special form for the study purpose. To study gene mutations, R249 in P53, blocks belonging to these patients in the hospital pathology laboratory were examined, and positive cases were analyzed by RFLP polymerase-chain reaction (PCR) to determine R249 mutations in the gene.
After optimization of the concentration of MgCl2 and fusing temperature, PCR of all samples were performed, and the PCR product was seen as a dark band on agarose gel 2%, respectively. The data were collected and analyzed by SPSS version 23 (Merck, Germany), and statistical tests were done by t-student, Mann–Whitney, and Chi-square test.
Results
In this study, 48 patients who were diagnosed with tongue SCC were admitted between 2014 and 2015 at the Al-Zahra and Kashani hospitals. The average age of these patients was 60.3 ± 9.2 years with a range between 32 and 82 years old. 31 of patients (66.4%) were male and 17 patients (43.5%) were female. Demographic data are shown in the in two groups. More than two-thirds of patients (72.9%) were 50 years old and older and 66.4% of them were male. Other risk factors of cancer of the tongue, 52.1% of patients had a history of smoking, 6.3% had a history of alcohol, and 18.8% had underlying diseases such as hypertension, diabetes, hypothyroidism, and systemic lupus erythematosus.
Study of cancer patients based on the stage of disease showed that 4 patients (3.8%) were in Stage I, 22 patients (45.8%) were in Stage II, 19 patients (39.6%) were in Stage III, and 3 patients (6.3%) were in Stage IV. For the cell differentiation, 34 patients (70.8%) were with well differentiated, 11 cases (22.9%) held the distinction of average, and three patients (6.3%) has had differentiation. In addition, 12 patients (25%) had lymph node metastasis.
PCR test done on tissue samples of patients showed that in the 48 studied samples, 4 cases (8.3%) had R249 mutation. After selection, the codon 249 as a hotspot in oral cancer, forward and reverse primers for amplification of exon 7 were obtained from the articles. The junction of the primers in exon 7 and codon 249 is shown in Figure 1.
Figure 1.
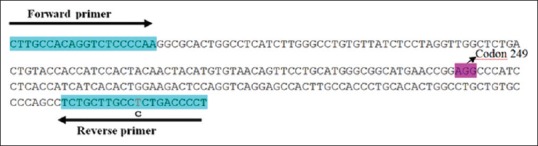
Junction of the primers in exon 7, codon 249
In Figures 2 and 3, PCR results of various examples can be seen on agarose gel.
Figure 2.
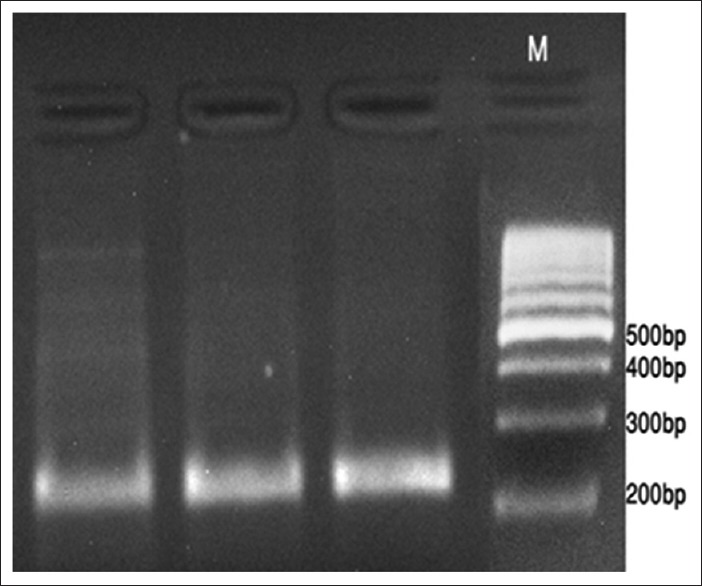
Polymerase-chain reaction product result are shown in AGAROSE 2% gel
Figure 3.
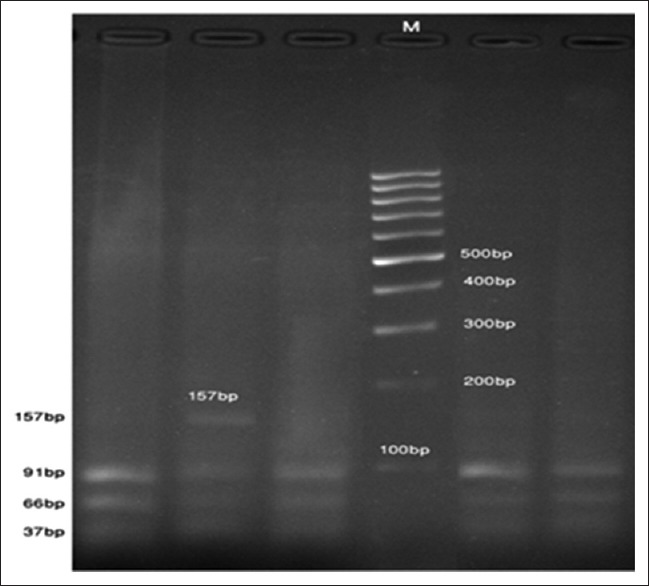
Results of polymerase-chain reaction product digestion on AGAROSE gel
Mutation is shown based on the demographic characteristics of the patients in this study. According to the results, patients who had R249 mutation had higher mean age. The percentage of people over 50-year-old in the group with the mutation was higher than that in the control group. In addition, the frequency of alcohol consumption was significantly higher in the group with the mutation. Finally, among other variables, the degree of cell differentiation in patients with mutation was significantly more favorable.
Discussion
Despite progress made in recent decades in cancer treatment, 5-year-survival of patients with this type of cancer still has remained unattainable. The studies show that at least 75% of patients with tongue cancer have two risk factors of cigarette and tobacco smoking along with p53 gene mutation which usually takes place in the region of R249. Based on the results of our study, 4 cases (3/8%) in 48 samples of tongue cancer, contained R249 mutation in the p53 gene compare with other mutations which did not contain R249. R249 is relatively high prevalence, and it can be one of the mutations that need to be taken into account confounding factors in the incidence of cancer of the tongue.
In this study, 48 patients with tongue SCC were studied, and the average age of these patients in study was 60.3 ± 9.2 years and 72.9% of them were male. According to most sources, the prevalence of tongue cancer in men is about the 1.5–2.4 times higher than that in women. In the study which was done by Delavarian in Mashhad, Iran, SCC was the most common malignancy in the mouth (73%). The ratio of male-to-female was 1–0.9, and the average age was 53.52 ± 17.66 years.[7] In another study in 2007 on 306 patients with oral cancers in Gilan province in Iran, the ratio of men to women was 1.55–1, and the average age of patients was 57.7 ± 15.65 years. The most common malignancies in cancer tongue patients were SCC with a frequency of 67%.[8] In a study conducted by Razmpa et al., different in two sexes was not significant.[9]
The results of studies conducted in America in 2011 show that over the past decade, the incidence and prevalence of SCC in both males and females has been raising between 3 and 5 years, and the survival rate of patients has been reduced with age and stage of disease, but it has not been significantly associated with patient gender.[5,6] In some studies, such famous Tze-Kiong Er and et al.'s study 68% of patients with tongue SCC had P53 mutation such R249, R248, and R247,…. The rate of R249 mutation was 0.02% in their study.[13]
According to the results of our study, PCR test showed 4 cases (8.3%) of the 48 studied samples were had R249 mutation. Previous studies have shown that genetic mutations play a major role in the incidence of cancers of the mouth, especially the tongue SCC.[14] So far, several studies in different parts of the world in relation to the importance and the vital role of P53 gene mutations in development of different kind of cancers have been done, and a wide range of frequency of these mutations (from 0% to 70% of patients) has been seen. These results reflect the diversity, abundance, and the role of these gene mutations in causing the disease in different ethnic groups and populations, and several studies have been conducted on the expression of P53 gene in tongue cancer.[15,16,17,18]
Based on the results of this study, 52.1% of patients had a history of smoking and 3.6% had alcohol consumption. Other studies have also mentioned that smoking and alcohol consumption are two important risk factors in the development of tongue cancer. In Iran, because of religious beliefs, alcohol consumption is not popular. However, the prevalence of alcohol consumption in patients who had R249 mutations in the P53 gene was significantly higher than that of society.[19]
On the other hand, based on the results of our study, samples with P53 gene mutations were in the region of R249 and they had more favorable degree of differentiation. Considering the findings of our study, R249 mutation in P53 gene in patients with SCC is relatively high. Age and alcohol consumption were the factors affecting the incidence of this mutation. Further studies are recommended. However, for prevention of tongue cancer and sever disease, it is important to start an early treatment with a single lesion of tongue to detect P53 gene[20] and also perform screening test on patient's family for early diagnosis and prevent cancer in future with gene therapy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Baily BJ. Otolatyngology, Head and neck surgery. 5th ed. Philadelphia: Elsevier Corp; 2014. pp. 156–60. [Google Scholar]
- 2.Harnschburger, Diagnostic Imaging Head and Neck. 2nd ed. USA: Mosby Elsevier Corp; 2011. p. 119. Epstein J, Van Der Waal I. Oral cancer. In: Greenberg MS, Glick M, editors. Burket's oral medicine, diagnosis and treatment. 11th ed. Hamilton: BC Decker; 2008. p. 153-89. [Google Scholar]
- 3.National Cancer Institute. Surveillance, Epidemiology, and End Results (SEER) [Last accessed 2011 Jan]. Available from: http://seer.cancer.gov/statistics .
- 4.Paul W Flint. Cumming's Otolaryngology, Head and neck surgery. 6th ed. Vol. 2. Philadelphia: Elsevier Corp; 2015. pp. 1319–21. [Google Scholar]
- 5.Wen CP, Tsai SP, Cheng TY, Chen CJ, Levy DT, Yang HJ, et al. Uncovering the relation between betel quid chewing and cigarette smoking in Taiwan. Tob Control. 2005;14(Suppl 1):16–22. doi: 10.1136/tc.2004.008003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Petersen PE. The World Oral Health Report 2003: Continuous Improvement of Oral in the 21st century-theapproach of the who global oral health rogram. Community Dent Oral Epideiol. 2003;31:3–23. doi: 10.1046/j..2003.com122.x. [DOI] [PubMed] [Google Scholar]
- 7.Sargeran K, Murtomaa H, Safavi SM, Vehkalahti M, Teronen O. Malignant oral tumours in Iran: Ten-year analysis on patient and tumour characteristics of 1042 patients in Tehran. J Craniofacial Surg. 2006;17:1230–3. doi: 10.1097/01.scs.0000246728.23483.ce. [DOI] [PubMed] [Google Scholar]
- 8.Saba NF, Goodman M, Ward K, Flowers C, Ramalingam S, Owonikoko T, et al. Gender and ethnic disparities in incidence and survival of squamous cell carcinoma of the oral tongue, base of tongue, and tonsils: A surveillance, epidemiology and end results program-based analysis. Oncol. 2011;81:12–20. doi: 10.1159/000330807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lodish H, Berk A, Kaiser CA, Krieger M, Bretscher A. Molecular cell biology. 6th ed. New York: WH Freeman and Company; 2007. pp. 1107–9. [Google Scholar]
- 10.He L, He X, Lim LP, de Stanchina E, Xuan Z, Liang Y, et al. A MicroRNA component of the P53 tumor suppressor network. Nature. 2007;447:1130–4. doi: 10.1038/nature05939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chang TC, Wentzel EA, Kent OA, Ramachandran K, Mullendore M, Lee KH, et al. Transactivation of miR-34a by P53 broadly influences gene expression and promotes apoptosis. Molec Cell. 2007;26:745–52. doi: 10.1016/j.molcel.2007.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Teodoro JG, Parker AE, Zhu X, Green MR. P53-mediated inhibition of angiogenesis through up-regulation of a collagen prolyl hydroxylase. Sci. 2006;313:968–71. doi: 10.1126/science.1126391. [DOI] [PubMed] [Google Scholar]
- 13.Er TK, Wang YY, Chen CC, Herreros-Villanueva M, Liu TC, Yuan SS, et al. Molecular characterization of oral squamous cell carcinoma using targeted next-generation sequencing. Oral Dis. 2015;21:872–8. doi: 10.1111/odi.12357. [DOI] [PubMed] [Google Scholar]
- 14.Benchimol S, Lamb P, Crawford LV, Sheer D, Shows TB, Bruns GA, et al. Transformation associated P53 protein is encoded by a gene on human chromosome 17. Somat Cell Mol Genet. 1985;11:505–10. doi: 10.1007/BF01534845. [DOI] [PubMed] [Google Scholar]
- 15.Isobe M, Emanuel BS, Givol D, Oren M, Croce CM. Localization of gene for human P53 tumor antigen to band 17p13. Nature. 1986;320:84–5. doi: 10.1038/320084a0. [DOI] [PubMed] [Google Scholar]
- 16.Miller C, Mohandas T, Wolf D, Prokocimer M, Rotter V, Koeffler HP. Human P53 gene localized to short arm of chromosome 17. Nature. 1986;319:783–4. doi: 10.1038/319783a0. [DOI] [PubMed] [Google Scholar]
- 17.Shiao YH, Rugge M, Correa P, Lehmann HP, Scheer WD. P53 alteration in gastric precancerous lesions. Am J Pathol. 1994;144:511–7. [PMC free article] [PubMed] [Google Scholar]
- 18.Luinetti O, Fiocca R, Villani L, Alberizzi P, Ranzani GN, Solcia E. Genetic pattern, histological structure, and cellular phenotype in early and advanced gastric cancers: Evidence for structure-related genetic subsets and for loss of glandular structure during progression of some tumors. Hum Pathol. 1998;29:702–9. doi: 10.1016/s0046-8177(98)90279-9. [DOI] [PubMed] [Google Scholar]
- 19.Uchino S, Noguchi M, Ochiai A, Saito T, Kobayashi M, Hirohashi S. P53 mutation in gastric cancer: A genetic model for carcinogenesis is common to gastric and colorectal cancer. Int J Cancer. 1993;54:759–64. doi: 10.1002/ijc.2910540509. [DOI] [PubMed] [Google Scholar]
- 20.Yamada Y, Yoshida T, Hayashi K, Sekiya T, Yokota J, Hirohashi S, et al. P53 gene mutations in gastric cancer metastases and in gastric cancer cell lines derived from metastases. Cancer Res. 1991;51:5800–5. [PubMed] [Google Scholar]