

Abstract
Quality improvement (QI) approaches have demonstrated a lot of promise in improving clinical care processes, both in high-resource and low-resource settings. However, most examples of QI initiatives in healthcare in low-income countries are clinic-based. The objective of this study was to demonstrate feasibility of applying QI methods in low-resource community settings by applying them to the problem of correct utilisation of long-lasting insecticidal nets (LLINs) in a rural community in Burundi. Correct utilisation of LLINs had been shown to be a cost-effective approach to malaria prevention. In Burundi, LLINs utilisation is low. The Model for Improvement, a well-known QI approach, was used to increase LLINs utilisation in a rural community in Burundi. In the baseline, LLINs ownership and weekly utilisation together with factors affecting LLINs non-use were documented for a period of 4 weeks before intervention. Improvement ideas were collaboratively developed by a quality improvement team (QIT) and tested using Plan-Do-Study-Act (PDSA) cycles. The first PDSA cycle consisted of the demonstration of how to mount LLINs, the second was an implementation of reminders done by household ‘watchdogs’, the third cycle consisted of conducting two community reminders every week and the last cycle was a combination of the last two PDSA cycles. The intervention lasted 4 weeks and data were collected weekly. LLINs utilisation was calculated each week and plotted on a run chart to demonstrate improvement trends. LLINs utilisation data were collected for another 3 weeks postintervention. Of 96 households, 83 (87%) households owned at least one LLIN. After intervention, the number of LLINs used increased from 32% to 75% (134% increase) and the number of persons (general population) sleeping under LLINs from 35% to 73% (108% increase). The number of children under 5 years sleeping under LLINs increased from 31% to 76% (145% increase) and the number of pregnant women who slept under LLINs from 43% to 73% (69% increase). Also, the averages of the number of nights in each week that the general population slept under LLINs increased from 2.13 to 5.11 (140% increase), children under 5 years from 1.68 to 4.78 (184% increase) and pregnant women from 1.56 to 4.47 (186% increase). Each of the 4 PDSA cycles led to a significant increase in outcome indicators and the trends appear to persist even after the implementation was complete. While it is impossible to draw generalisable conclusions from a small pilot study, QI approaches appear to be feasible to implement in low-resource community setting and have promise in producing results. More research at larger scale should be encouraged to validate our initial findings.
Keywords: LLINs utilization, Model for Improvement, Pregnant Women, Children under 5
Introduction
Problem description
Burundi is a malaria holo-endemic country with 6.6 million cases and 3000 deaths due to malaria each year.1 For more than a decade, long-lasting insecticidal nets (LLINs) have been provided free of charge through regular community mass distribution campaigns and targeted distribution for all pregnant women and mothers visiting healthcare settings for antenatal care, childhood immunisation or paediatric healthcare.2–5
However, mass distribution of LLINs has not necessarily led to reduced malaria incidence.6 Despite high LLINs ownership rates and coverage in many malaria endemic settings, LLINs misuse and non-use is reportedly high, which undermines efforts to control the disease.7–9 In Burundi for instance, with an average LLINs coverage of 46% in 2016, only 35% of LLINs were used.1 Most importantly, only 40% of children under 5 years and 44% of pregnant women in households with access to at least one LLIN reportedly slept under it the night before the 2016 Demographic and Health Survey interviews.1 In some cases, LLINs are used for other purposes (e.g. as fishing nets) resulting in the increase of malaria burden and its mortality rates and constitutes considerable wastage of scarce government resources in a low-income country.10 This paper describes the use of quality improvement (QI) methods to develop context appropriate solutions to address the low use of LLINs in Kayange community in north-western Burundi.
Available knowledge
LLINs use in Kayange mirrors the situation in the rest of the country. A 4-week baseline survey conducted prior to intervention showed that of 96 households in Kayange community, 83 (87%) households possessed at least one LLIN. However, only 40 households (42%) possessed at least one LLIN for every two people as recommended by the World Health Organization (WHO).11 A total of 210 LLINs were available in the community, and nearly one third of these were used in the month prior to intervention. 35% of community members, 31% of children under 5 years and 43% of pregnant women reported sleeping under LLINs. The average weekly number of nights that people including for pregnant women and children under 5 years reported sleeping under LLINs varied from 1 to 2 nights.
A review of the literature by Pulford et al (2011) identified discomfort due to hot weather, perceived low mosquito density, lack of knowledge about how to use LLINs and the inadequacy of LLINs as the predominant reasons associated with the non-use of LLINs.11 These reasons were also reflected in the Kayange baseline. 45.57% of households did not remember to hang LLINs up, 23.96% lacked knowledge for hanging LLINs, 14.84% blamed hot weather, while 4.96% claimed that LLINs are bad for health. When asked what else LLINs are used for, a majority (61%) did not provide a concrete answer, while others reported using LLINs for fishing (20%), night covering (5%), screens for windows (3%) and clothing (1%).
Rationale
Interventions to address LLINs non-utilisation have been dominated by general or targeted ‘educational programmes’.12 While community-tailored interventions seem to yield greater impact, general programmes have been found to be associated with lesser outcomes.12 13 In a community randomised trial by Soleimani Ahmadi et al 12 conducted in rural south-eastern settings of Iran, a community-targeted educational programme increased the proportion of households who used LLINs from 58.3% to 92.5% one month following intervention.12 On the other hand, malaria education interventions implemented through school students and religious leaders in Ethiopia did not achieve considerable impact, leading to the recommendation for educational programmes beyond the traditional messaging approach.13 Our intervention tested change ideas, collaboratively generated by a quality improvement team (QIT), in a small community in north-western Burundi using the QI methodology to assess whether ideas tailored to the local context were more effective. We also aimed to test the feasibility of applying QI methods to low-resource community settings.
Recently, there has been an increase in the use of QI approaches in healthcare in low-resource settings.14–16 The most common QI approaches include Six Sigma, Lean and the Model for Improvement (MFI).17 Each QI model has a different philosophy but overall, they have a common goal of improving process of care delivery or support.
In this study, we employed the MFI to test the possibility for improving LLINs use. The MFI consists of two main parts: a part that proposes changes that might result in improved outcomes and a part that systematically and iteratively tests these changes on a small scale in real life settings using the Plan-Do-Study-Act (PDSA) cycles.17 Each test cycle hypothesises a change, implements it on a small scale, studies whether it works, and based on the results, decides what to try in the next cycle.18 The model is shown in figure 1.
Figure 1.
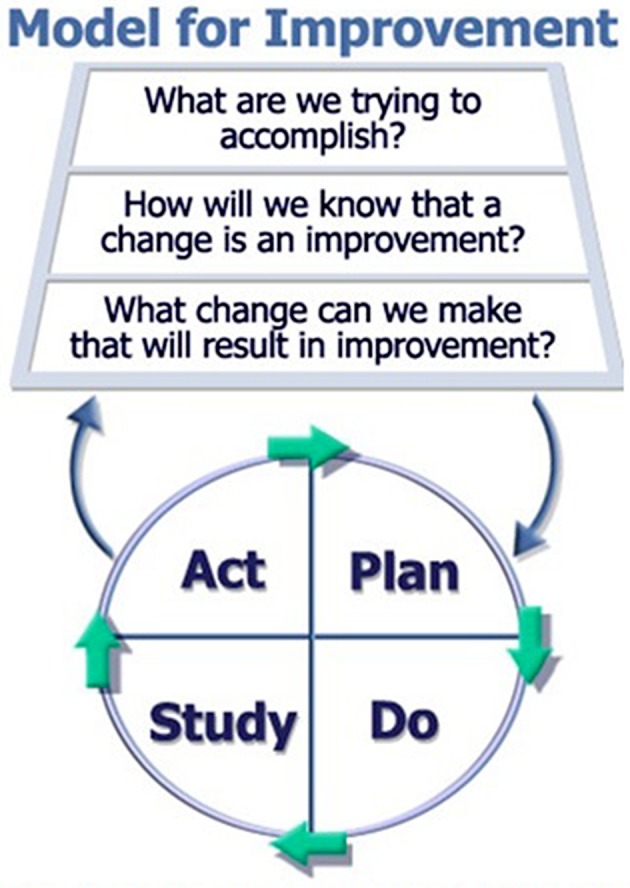
The Model for Improvement.
Our study embedded the MFI approach within a six-step process to develop context-specific locally appropriate change interventions. This involved setting an improvement aim, creating a QIT, establishing measures, identifying change ideas, performing tests, determining those that work and implementing them.
Methods
Study site
The study was conducted in Kayange community, Nyagatobe site, in north-western Burundi. In Burundi, administrative hierarchical levels are nation, province, commune, zone and hill. Kayange is a hill located at −3.2294° latitude and 29.4267° longitude in commune Rugazi, Province of Bubanza. The study site is shown in figure 2.
Figure 2.
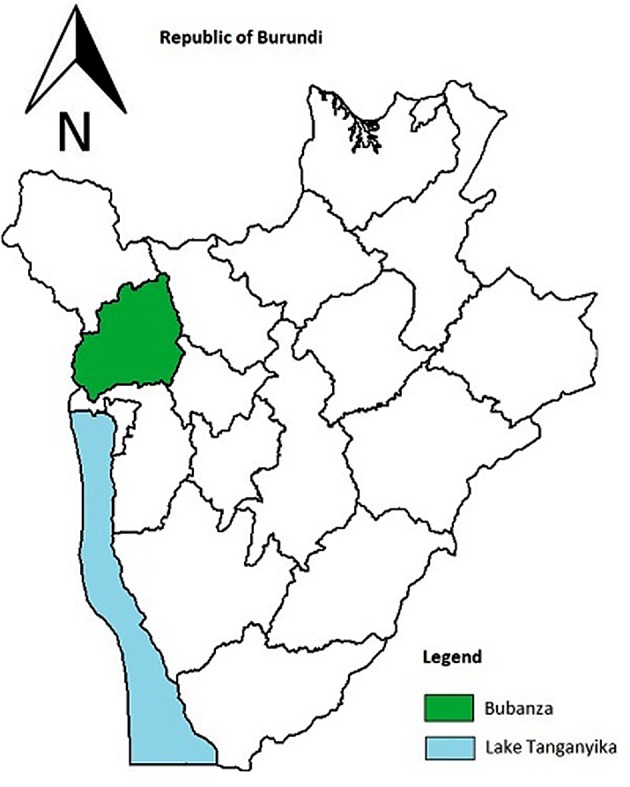
Study site.
Nyagatobe is a subcommunity of Kayange composed of 96 households. Baseline results showed that while 87% of households possessed at least one LLIN, this community only used 32% LLINs for malaria prevention. The community of Kayange had a population of 482 people of whom 110 (23%) were children below the age of 5 years and 23 (5%) were pregnant women. Approximately 65% of inhabitants have no formal education, 32% have primary education and 3% have attained secondary education. In this community, no one has reached tertiary education. It is an indigenous community and hence one of the poorest, least educated and disadvantaged population.
This setting has one of the highest malaria incidences in Burundi with 51.9% of new cases reported in 2017 (EPISTAT, MoH Burundi). Apart from belonging to the region at high malaria risk, selection of Kayange was by convenience, primarily based on accessibility and a smallness of the community with condensed households.
Improvement aims
The formal aim of the project is shown in box 1.
Box 1. Aim statement.
Over the next two months, 100% of LLINs possessed (n=210) in the study site will be correctly used, the number of people (including children under 5 years and pregnant women) who sleep under LLINs will increase by at least 30% from baseline and all those who sleep under LLINs will do so all nights of each week.
Quality improvement team
We created a QIT composed of six members of whom two came from the community—a community health worker (CHW) and a community leader, one from the healthcare facility of Rugazi which is the nearest healthcare centre and another two members from local non-governmental organisations working on malaria prevention. These multidisciplinary team members were chosen because they are affected by the aim of the improvement and also had skills needed for implementing malaria control programmes. The principal investigator (PI) from the University of Burundi led that team. The QIT received a half-day training on the MFI provided by the PI. For the duration of the study, the QI team met each week to monitor the improvement measures described below and to identify a new change idea for testing. In addition, the CHW and the community leader were responsible for local mobilisation for community-level activities.
Improvement measures
In order to understand if tested change ideas were leading to improvement, we tracked the outcome indicator for each aim every week. Recognising that the use of nets could result in increased net wear and could be perceived as being detrimental to sleep by some community members, we also tracked data on one ‘balancing’ measure shown in table 1.
Table 1.
Outcome and balancing measures
| Aim | Outcome measure | Balancing measure |
| Increase correct use of LLINs | Per cent of households reporting LLINs use | Number of LLINs torn due to use |
| Increase people who sleep under LLINs | Average per cent of household members who sleep under LLINs | – |
| Average per cent of children under 5 who sleep under LLINs | – | |
| Average per cent of pregnant women who sleep under LLINs | – | |
| Increase the number or nights per week that people sleep under LLINs | Average weekly number of nights that all household members sleep under LLINs | – |
| Average weekly number of nights that children under 5 years sleep under LLINs | – | |
| Average weekly number of nights that pregnant women sleep under LLINs | – |
LLINs, long-lasting insecticidal nets.
Intervention development
Based on the baseline data and on the review of the literature on interventions to address low LLINs use, we developed a theory of change shown in figure 3. We established from the baseline that LLINs are available in the community, that they are of adequate quality and that it is feasible to hang them up in bedrooms. The main reasons for the non-use of the LLINs were related to skills and attitudes in the community. The two boxes to the right of the theory of change were targeted for the PDSA cycles.
Figure 3.

Theory of change. LLINs, long-lasting insecticidal nets; PDSA, Plan-Do-Study-Act.
As recommended by the MFI, we developed locally appropriate context-specific interventions by identifying change ideas and testing them through PDSA cycles. Each week’s data informed a change action. Change ideas were developed by the entire QIT but mostly tested by the PI who was assisted by one or two members of the team. Development of change ideas involved QIT participatory discussions during which members suggested bold ideas for change. Discussions lasted for approximately one to one and half hours. One idea was agreed on by members and retained for testing. In total, four change ideas were developed and tested using PDSA cycles as shown in table 2.
Table 2.
PDSA cycles
| Cycle | Change idea |
| 1 | LLIN hang-up demonstration |
| 2 | Household watchdogs |
| 3 | Weekly community reminders by the town crier |
| 4 | Combination of ideas 2 and 3 |
LLIN, long-lasting insecticidal net.
Description of cycles
Cycle 1: LLIN hang up demonstration
Community leaders were asked to invite all community members for the demonstration session. The demonstration was done first by the QIT and repeated by the community leader and by two randomly selected community members.
Cycle 2: household watchdogs
One adult in each household across Kayange community was named household watchdog by the QIT. Selection of household watchdogs was based on the member agreeing to volunteer for the role. The CHW and community leader visited each household to select watchdogs. During a gathering led by the PI, the CHW and the community leader, watchdogs were taught their responsibilities and approaches for checking and reminding household members to mount LLINs. Their role was to watch if any of the bedrooms did not have a mounted LLIN before sleeping. If they found such a bedroom, watchdogs were asked to kindly remind the persons who sleep on the bed to mount the net. Also, watchdogs were allowed to use the standard notice prepared and provided by the QIT that reads ‘muribuka kumanika umusegetera’ which means ‘please, you are kindly reminded to mount LLIN’ and hang it on the walls inside each bedroom.
Cycle 3: reminders by town criers
Before the third cycle, watchdogs were asked to stop household-level reminders and unhang notices in each bedroom. In Burundi, messages in rural communities are communicated by town-criers. In the evening, when all or the majority of community members are in their houses, town-criers circulate throughout the houses announcing the message. Town-criers use small drums to awake the attention of the community. Traditionally, when a small drum sounds during evening hours, the community pays attention to the message. The town-crier communicated the following message prepared and handed over by the QIT: ‘Dear community members of Kayange hill, Nyagatobe sub-hill, we are reminding you that malaria is a disease that is causing deaths to many people; especially pregnant women and children under 5 years. We therefore take the opportunity to remind you to sleep under LLINs’. The message, which was translated in Kirundi, was communicated between 07:00 and 21:00 hours two times a week for one week.
Cycle 4: combination of cycles 2 and 3
Both the town crier and the watchdogs were used and tested for another one week
Data collection
A semistructured paper-based interview questionnaire was used to collect data. Data included sections for sociodemographic characteristics of respondents, composition of household members, LLINs ownership, LLINs utilisation and drivers of LLINs non-utilisation (online supplementary appendix 1). The questionnaire was translated in Kirundi for better comprehension and data back-translated to English. Ten data collectors were identified from Kayange community and trained on data collection using the questionnaire. All households in Kayange were assigned a unique identification number and were equally divided among interviewers. Each interviewer was assigned between 8 and 10 households (n=96) and was required to collect data every week. Household visits were conducted on Saturdays during morning hours because in Burundi, people are more likely to be at home on weekends. During each day of data collection, the PI and one or two QIT members were present to oversee the data collection process. They visited each data collector for a period of 5–15 min during data collection for supervision. To reduce the risk of bias, individuals participating to the project (e.g. watchdogs) were not eligible to collect data. Other selection criteria were having completed primary education and availability.
bmjoq-2018-000540supp001.pdf (90.2KB, pdf)
Ethical considerations
Ethical clearance and approval for the research was granted by the Medical Health Research Ethics Committee (HREC) of the University of the Witwatersrand before the commencement of the research. Also, a local study authorisation was obtained from The Ministry of Interior and the Communal Administrator of Rugazi. Study participants were informed of the study and Informed Consent Forms (ICFs) were signed by participants. Data that were collected were used strictly for the purposes of this study and were password-protected. Also, confidentiality and anonymity were ensured by using serial numbers during data collection. Names and identifiable data of participants were not documented. Only the researcher and the supervisors had access to the datasets.
Results
Results from each PDSA cycle are presented in table 3. Improvements in LLINs utilisation have been presented using a run chart in figure 4.
Table 3.
Results from PDSA cycles
| Measurement | Baseline | Aim | Increase in outcome | |||
| PDSA 1 | PDSA 2 | PDSA 3 | PDSA 4 | |||
| Per cent LLINs used | 32.35% | 100% | 42.86% | 59.05% | 65.24% | 70.48% |
| People sleeping under LLINs | 35.48% | 44.82% | 43.36% | 58.09%* | 62.66%† | 68.88%† |
| Under 5 children sleeping under LLINs | 31.37% | 40.78% | 47.27%* | 59.08%† | 6636%† | 72.73%† |
| Pregnant women sleeping under LLINs | 43.48% | 56.52% | 47.83% | 56.53%* | 60.87%† | 69.57%† |
| Average number of weekly nights people slept under LLINs | 2.14 | 7 | 2.23 | 3.71 | 4.13 | 4.41 |
| Average number of weekly nights children under 5 slept under LLINs | 1.68 | 7 | 2.09 | 3.45 | 3.94 | 4.15 |
| Average number of weekly nights pregnant women slept under LLINs | 1.56 | 7 | 1.77 | 3.09 | 3.64 | 3.38 |
*Target aim is achieved.
†Improvement is sustained beyond target aim.
LLINs, long-lasting insecticidal nets; PDSA, Plan-Do-Study-Act.
Figure 4.

Run chart: LLINs utilisation in Kayange community. LLINs, long-lasting insecticidal nets; PDSA, Plan-Do-Study-Act.
Discussion
The goal of this study was to demonstrate feasibility of applying QI methods in low-resource community settings. Results from the PDSA cycles supported our theory of change and improved LLINs utilisation for the entire community members and also for pregnant women and children under 5 years. This strongly demonstrates the potential for applying QI approaches in low-resources communities, provided adequate support is available. The PDSA cycles led to improved LLINs utilisation during the period of the study but we did not monitor sustainability of improvements. We created a multidisciplinary QIT, used a participatory discussion approach to identify change ideas, monitored implementation of change ideas using process and balancing measures, created an enabling environment by engaging community leaders and trained and supervised data collectors to reduce biases.
Overall, while the aim of increasing by greater than 30% from baseline the number of people sleeping under LLINs was more likely achievable, that of attaining regular LLINs use, which means achieving an increase of at least 227% from baseline, was too ambitious and could not be achieved. Total 30% increase was achieved after the second PDSA cycle. This can be partly explained by the Hawthorne effect because community members were aware that data collection is conducted every Saturday and were more likely to sleep under LLINs the nights preceding the visit.
Improvement was more significant after the two first PDSA cycles than it was after the two last ones. After the first PDSA cycle, the increase in the number of LLINs used and in the number of persons (including children under 5 years and pregnant women) who slept under LLINs was higher than the increase in the number of nights that they slept under LLINs. In other words, many people slept under LLINs but for only a few nights in a week. Without claiming the assertion, this may be explained by the fact that community members were initially excited, which excitement lost momentum day after day along the week. It is based on this finding that the QIT decided to implement a reminder change idea through household watchdogs.
The second PDSA cycle led to a considerable increase in both the number of persons who sleep under LLINs and the number of nights that they sleep under LLINs. The last two PDSA cycles led to a similar increase whose magnitude is smaller when compared with the first two achievements. This decelerated increase in LLINs utilisation over time could be an indication of a potential dropping trend when observed for a long period of time. Therefore, we cannot guarantee sustainability of achieved results.
Field experience has proved that community leaders play an essential role in community mobilisation and in achieving community participation. This was notably visible during the first PDSA cycle which required community gathering for LLINs mounting demonstration.
Successful implementation of the project was facilitated by a collaborative approach that brought together community leaders, CHW and local players involved in health and, specifically, in malaria interventions. Understanding the root causes of the problem and engaging a participatory discussion to identify change ideas were the key to success. Among the barriers to implementation include low level of literacy. This was addressed by translating all documents in Kirundi and by implementing simple and comprehensible change ideas.
Based on our experience, strong QI projects are possible provided that they are tailored and contextualised, conducted repetitively for a long period, supported by strong mechanisms to monitor the process and provided that they follow QI methodologies.
After the fourth PDSA cycle, weekly data were collected for another 3 weeks to observe the trends. Postintervention findings showed an increasing path for all indicators (e.g. figure 4). However, these results need a cautious treatment because of the unknown confounding effects and biases. Future rigorous researches may bring more light on the subject.
Moreover, our study was not immune to limitations. A small sample size and a close homogenous community are instances of such limitations. Bowing to contamination and social and cultural norms, it is more likely that such a community adopts similar behaviours and practices. Another shortcoming of the study lies in its inability to assess implementation process fidelity. Therefore, generalisation and replicability of implemented change packages cannot be recommended.
Conclusion
In conclusion, our study proved that QI models have potential for addressing community challenges in low-resources settings. While such programmes are labour intensive and need to be implemented with care, they are potential for achieving considerable impact and hence contributing to the achievement of the Sustainable Development Goals (SDGs) 2030. Based on our findings, we would call for more researches to pursue these kinds of projects, especially in the developing world.
bmjoq-2018-000540supp002.pdf (90.2KB, pdf)
Footnotes
Contributors: DH conceptualised, designed and implemented the project and drafted the manuscript. GiN supervised the conduct of the research and aided in writing the research protocol and the manuscript. GaN contributed in obtaining local study approval. JN and RR guided the methodological approach of Quality Improvement methodologies and, specifically, in the implementation of Plan-Do-Study-Act cycles.
Funding: This work was funded by TDR, the Special Programme for Research and Training in Tropical Diseases, which is hosted at the WHO and cosponsored by UNICEF, UNDP, the World Bank and WHO. TDR grant number: WHO/TDR/RCS/B40299.
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Burundi. Troisième Enquête Démographique et de Santé au Burundi (EDSB-III) - Rapport de synthèse. 2017. [Google Scholar]
- 2. World Health Organization World malaria report 2015 World Health Organization; 2016. [Google Scholar]
- 3. Beier JC, Keating J, Githure JI, et al. . Integrated vector management for malaria control. Malar J 2008;7 Suppl 1:S4 10.1186/1475-2875-7-S1-S4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Burundi. Malaria control: strategic plan. 2008. [Google Scholar]
- 5. Falisse J-B, Ndayishimiye J, Kamenyero V, et al. . Performance-Based financing in the context of selective free health-care: an evaluation of its effects on the use of primary health-care services in Burundi using routine data. Health Policy Plan 2015;30:1251–60. 10.1093/heapol/czu132 [DOI] [PubMed] [Google Scholar]
- 6. Bennett A, Smith SJ, Yambasu S, et al. . Household possession and use of insecticide-treated mosquito nets in Sierra Leone 6 months after a national mass-distribution campaign. PLoS One 2012;7:e37927 10.1371/journal.pone.0037927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ahmed SM, Zerihun A. Possession and usage of insecticidal bed nets among the people of Uganda: is brac Uganda health programme pursuing a pro-poor path? PLoS One 2010;5:e12660 10.1371/journal.pone.0012660 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Matovu F, Goodman C, Wiseman V, et al. . How equitable is bed net ownership and utilisation in Tanzania? A practical application of the principles of horizontal and vertical equity. Malar J 2009;8:109 10.1186/1475-2875-8-109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Minakawa N, Dida GO, Sonye GO, et al. . Unforeseen misuses of bed nets in fishing villages along lake Victoria. Malar J 2008;7:165 10.1186/1475-2875-7-165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Fantom NJ, Serajuddin U. The world bank's classification of countries by income, 2016. [Google Scholar]
- 11. WHO WHO recommendations for achieving universal coverage with long–lasting insecticidal nets in malaria control. Geneva: World Health Organization, 2013. [Google Scholar]
- 12. Soleimani Ahmadi M, Vatandoost H, Shaeghi M, et al. . Effects of educational intervention on long-lasting insecticidal nets use in a malarious area, Southeast Iran. Acta Med Iran 2012;50:279-87. [PubMed] [Google Scholar]
- 13. Birhanu Z, Abebe L, Sudhakar M, et al. . Access to and use gaps of insecticide-treated nets among communities in Jimma zone, southwestern Ethiopia: baseline results from malaria education interventions. BMC Public Health 2015;15:1304 10.1186/s12889-015-2677-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Bisognano M, Cherouny PH, Gullo S. Applying a science-based method to improve perinatal care: the Institute for healthcare improvement perinatal improvement community. Obstet Gynecol 2014;124:810–4. 10.1097/AOG.0000000000000474 [DOI] [PubMed] [Google Scholar]
- 15. Jencks SF, Wilensky GR. The health care quality improvement initiative. A new approach to quality assurance in Medicare. JAMA 1992;268:900–3. [PubMed] [Google Scholar]
- 16. Twum-Danso NA, Dasoberi IN, Amenga-Etego IA, et al. . Using quality improvement methods to test and scale up a new national policy on early post-natal care in Ghana. Health Policy Plan 2014;29:622–32. 10.1093/heapol/czt048 [DOI] [PubMed] [Google Scholar]
- 17. Hughes RG. Tools and strategies for quality improvement and patient safety 2008. [PubMed]
- 18. IHI Institute for Healthcare Improvement. “The Model for Improvement", 2016. Available: http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx [Accessed 25 July 2016].
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjoq-2018-000540supp001.pdf (90.2KB, pdf)
bmjoq-2018-000540supp002.pdf (90.2KB, pdf)