

1. Introduction
Approximately 30% of older adults report balance impairments resulting in an increased fall risk that goes up with increasing age [1]. Balance impairment can result in dynamic instability while walking-i.e., diminished capacity to regulate the kinematics of the whole body center of mass (COM) with respect to the base of support (BOS) [2], which decreases older adults’ mobility, contributing to decreased community participation [3]. While reduced balance may relate with structural and functional declines in locomotor and balance control [4], other factors may also interact with the motor system and influence the observed decreased COM control [5]. For instance, psychosocial factors can acutely shape or modify how the motor system responds to static and dynamic tasks [6, 7]. Indeed, reduced balance confidence is associated with a deterioration in the performance of clinical tests of balance and mobility for elderly [8–10]. Thus, many factors can result in poor balance control and mobility limitations, which presents a critical concern for older adults [11] and understanding those factors can help to create targeted clinical interventions.
The control of the kinematics of the COM with respect to the BOS must be performed on a step-by-step basis [12, 13]. A measure of mechanical stability, the margin of stability (MOS), quantifies the distance from the extrapolated COM (i.e., the position and normalized velocity of the COM) to the boundary of the BOS [14, 15] on a step-by-step basis. Scaling speed can provide a challenge to controlling COM kinematics that is not observed at preferred walking speeds and can result in a decreased MOS [16]. As walking speed is systematically increased, step kinematic variability increases in young adults in both the mediolateral and sagittal planes [17], and at faster than preferred walking speeds, the extrapolated COM goes beyond the BOS, resulting in a negative MOS [16]. With aging, greater caution may be observed when performing gait related tasks that increase an individual’s risk of becoming unstable [12, 13].
Clinical measures of balance, i.e., self-selected walking speed, Berg Balance Scale, or Timed Up & Go Test, have been related to an individual’s balance confidence [9, 10, 18] whereby better balance performance is observed with higher balance confidence. If balance confidence is related to dynamic stability, then, as the task of walking becomes more challenging, reduced balance confidence may affect the willingness of individuals to attempt faster speeds. These self-imposed restrictions may relate to an actual decrement in controlling the COM when performing a challenging task or may just be the individual’s perception that COM control is worse, in which case the mechanics of gait will be similar to individuals with higher balance confidence. Thus, investigating the link between laboratory-based measures of dynamic stability while walking and balance confidence could inform different interventional approaches to improve balance and reduce fall risk.
Therefore, the purpose of this study is to investigate the relationship between dynamic stability and walking speed in a group of younger and older adults and the extent that dynamic stability measured in the lab setting is related to balance confidence. It was hypothesized that exposure to progressively faster speeds will result in decreased dynamic stability for older adults when compared to younger adults. We also hypothesized that balance confidence would relate to measures of stability while older adults attempted to walk at progressively faster speeds.
2. Materials and methods
2.1. Participants
Ten young adults (7 females) and 14 older adults (10 females) volunteered to participate in this study (Table 1). Participants were excluded from the study if they affirmed any neurological, musculoskeletal, or other injuries or disorders that would limit their functional mobility and if they required an assistive device to walk. Eligible participants provided written informed consent prior to participation. The study was approved by the Institutional Review Board at the University of Alabama at Birmingham, ethics approval number F160225004. Prior to testing, sociodemographic data, health-related information, comfortable and maximum walk speed and fall history (the number of falls in the past year) was collected.
Table 1.
Mean, standard deviation and 95% Confidence interval for mean of the young and older adults’ characteristics
| Characteristics | Young adults | Older adults | p-value |
|---|---|---|---|
| Age (years) | 27±4.18 [24.11, 30.09] |
69±3.57 [67.08, 71.20] |
<0.001*a |
| Height (m) | 1.72±0.10 [1.65, 1.79] |
1.70±0.09 [1.65, 1.75] |
0.658b |
| Weight (kg) | 69.11±9.44 [62.35, 75.87] |
76.62±14.31 [66.61, 82.50] |
0.380b |
| ABC score | 99±1 [97.63, 99.77] |
89±13 [81.19, 96.52] |
0.006*b |
| 5XStoS (sec) | 6.80±2.20 [5.22, 8.37] |
10.14±2.58 [8.65, 11.63] |
0.003*a |
| CWS (m/s) | 1.49±0.10 [1.42, 1.56] |
1.38±0.25 [1.24, 1.53] |
0.168a |
| MWS (m/s) | 2.46±0.65 [2.00, 2.93] |
1.76±0.33 [1.57, 1.95] |
0.007*b |
| Number of falls | 0(0) | 4(28.6%) | 0.064c |
ABC = the Activities-specific Balance Confidence Scale, 5XStoS = the 5-Time Sit-to-Stand, CWS = the Comfortable Walking Speed, MWS = the Maximum Walking Speed, years = years old, m = meter, kg = kilogram, sec = second.
Statistically significant difference at p<0.05.
Comparison between groups by using the Independent t test.
Comparison between groups by using the Mann-Whitney U test.
Comparison between groups by using the Chi-square test
2.2. Procedure
All participants completed the 16-item Activities Specific Balance Confidence Scale [19]. This measure captures the self-assessed balance confidence of individuals performing tasks of daily living by rating their level of confidence in performing tasks without “losing their balance or becoming unsteady”. Scoring ranges from no confidence (0%) to completely confident (100%). Higher scores indicate greater balance confidence. The measure is reliable and valid and has been shown to predictive of fall status and incidence of future falls [20].
2.3. Experimental protocol
Individuals performed three 10-m overground walk trials timed with a stopwatch in each comfortable and maximum speeds to characterize our participant sample. For comfortable walking speed, individuals were instructed to “walk at a speed that feels the most comfortable” and for maximum speed individuals were instructed to “walk at the fastest speed you feel safe”. Prior to the start of the protocol, every participant was familiarized with walking on the treadmill by first walking at a very slow speed (0.4 m/s), and the speed was slowly increased once they confirmed they felt comfortable at that speed. The treadmill speed was increased until a walking speed of 1.0 m/s was achieved, and the participants affirmed they felt comfortable. In this study, we used a robotic system, the KineAssist (Figure 1), which is coupled with a split-belt instrumented treadmill. The device interfaces with individuals through a pelvic mechanism that allows 6-degrees of freedom of the pelvis to allow for relative transparency. This treadmill device was used for safety purposes to prevent individuals from falling to the treadmill surface if they lost their balance.
Figure 1.
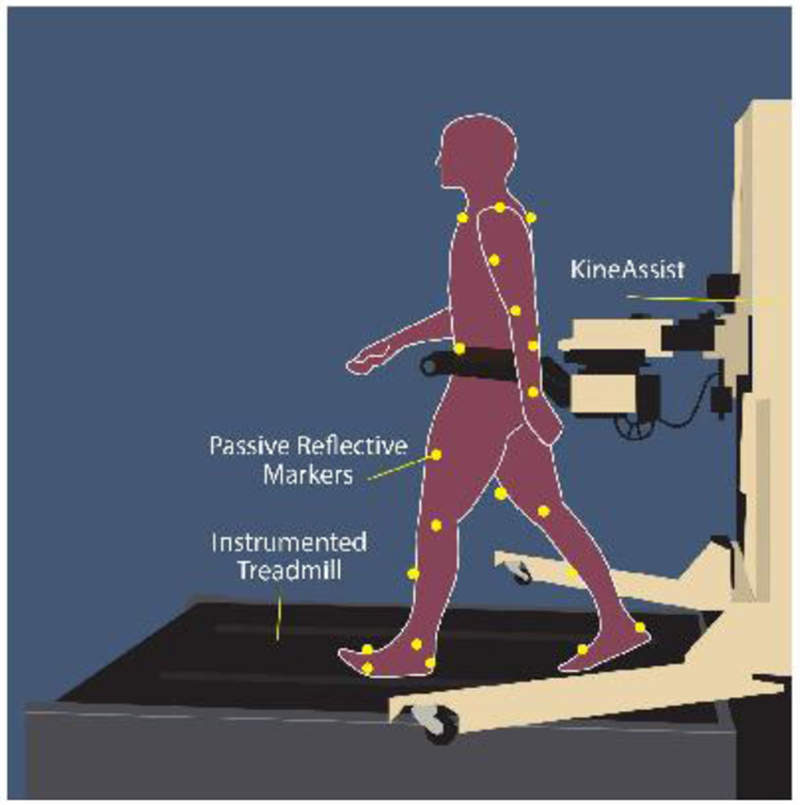
The experimental setup used for this experiment. The KineAssist which allows for six degrees of freedom at the pelvic interface creating relative transparency, was used to guard against falls during the experimental protocol.
After participants were acclimated to walking on the treadmill, they were asked to walk at a range of speed from 0.4 m/s to 2.0 m/s in 0.2 m/s increments with short rests between each walking speed. The top limit of 2.0 m/s is around the reported walk to run transition speed [21]. Faster walking trials were attempted until the participant chose not to walk at a faster speed, OR all speeds were attempted. Short breaks, from 2-5 minutes, were provided throughout the data collection and individuals had the option to sit if they desired to.
2.4. Data analysis
The trajectories of 34 passive reflective markers were recorded by an eight-camera motion capture system recording at 100 Hz (Qualysis, Goteborg, Sweden) to create a 12-segment ridgid body model [22]. The three-dimensional marker positions were tracked using commercial software (Qualysis Track Manager) and filtered with a Butterworth 6 Hz zero-lag low-pass filter. Maximum and minimum positions of heel and toe markers were used to identify heel strikes and toe offs, respectively, and estimates of COM position were quantified in Visual 3D (C motion Germantown, MD) and analyzed using custom Matlab software (MathWorks, Natick, MA).
For this investigation, we quantified dynamic stability on a step-by step basis using the margin of stability (MOS) [15]. The position and velocity of the COM were used to define the extrapolated COM (xCOM: Eq. 1). The velocity of the COM was normalized by the eigenfrequency, or natural frequency, of a non-inverted pendulum (ω0).
| (1) |
The MOS considers the distance between the xCOM and the border of BOS (Eq. 2 and 3). The anterior and medial border of the BOS was estimated with markers placed on the participants shoe over the middle phalangeal bone of the 1st toe and the proximal phalangeal of the 5th toe, respectively. This measure provides a spatial measure of stability whereby positive values of the MOS result from the xCOM being located within participants BOS. Negative MOS value represents the xCOM outsides an individual’s BOS and indicates an unstable step. MOSap (anterior-posterior) was quantified at heelstrike and MOSml (medial-lateral) was the minimum MOS, which occurs after heelstrike. The equation for MOS was as follow:
| (2) |
| (3) |
The MOSap were averaged for each speed and a regression relationship was created between MOSap and walking speed to assess the sensitivity of dynamic stability (i.e., the slope of the relationship). As individuals walk faster the MOSap decreases in value and will eventually cross zero [16]. We quantified the walking speed after MOSap crossed zero (i.e., zero crossing). As exploratory analysis we also quantified the COM position at footstrike defined as the location of the COM with respect to the BOS and related that to walking speed as well as the change in MOS variability with speed.
2.5. Statistical analyses
Descriptive statistics were computed for all variables and are reported with mean, standard deviation, 95% of confidence interval for mean and percentage to describe group proportions. For statistical analysis, data were analyzed with SPSS version 25 (IBM Corporation, Armonk, NY, United States). The distributions of the data were analyzed with a Shapiro Wilk test. Independent sample Student t test and the Mann-Whitney U test were performed to compare participant characteristics of both groups. The chi-square test was used to evaluate differences in falls between both groups. The Spearman rank correlation coefficient was used to examine the relationships between balance confidence and measures of stability while mixed linear regression analysis were used to assess the relationship of MOSap and walking speed. Two-tailed statistical significance was set to p<0.05.
3. Results
3.1. Age-related effects of speed
Age-related differences were detected in measures of gait and stability (Table 2). All younger adults attempted all possible speeds while some older adults chose to stop walking before 2.0 m/s. For older adults, 8 completed all speeds while 6 individuals stopped before 2.0 m/s (range, 1.0-1.8 m/s). Thus, the fastest speed attempted by older adults, on average, was 1.82±0.35 m/s (U(1)=40.00, Z= −2.310, p=0.021). The MOS variability of older adults was larger compared to young adults at the fastest speed achieved in the sagittal (U(1)=28.00, Z=2.459, p=0.013) and frontal plane (t(22)= −3.0, p=0.007). Older adults became unstable at a slower speed than younger adults. On average, younger adults MOS was negative at 1.60 ± 0.09 m/s whereas older adults MOS was negative at 1.23 ±0.27 m/s (U(1)=12.50, Z= −3.529, p<0.001), (Figure 2a). Older individuals walked with a reduced overground maximum walking speed (U(1)=24.00, Z=−2.695, p=0.007). There were no significant differences in the mean of MOS at fastest speed attempted and sensitivity of MOS between both groups (t(20.481)=1.208, p=0.241 and t(22)= −0.437, p=0.666, respectively) and overground comfortable walking speed (t(18.068)= −1.435, p=0.168).
Table 2.
Mean, standard deviation and 95% Confidence interval for mean of the young and older adults’ gait parameters and measures of dynamic stability
| Variables | Young adults | Older adults | p-value |
|---|---|---|---|
| MOSfa at FSA (m) | −0.14±0.04 [−0.17, −0.11] |
−0.17±0.07 [−0.21, −0.13] |
0.241a |
| MOSfa variability at FSA (m) | 0.02±0.01 [0.12, 0.03] |
0.03±0.01 [0.02, 0.03] |
0.014*b |
| MOSml at FSA (m) | 0.12±0.02 [0.11, 0.13] |
0.13±0.03 [0.11, 0.14] |
0.598b |
| MOSml variability at FSA (m) | 0.01±0.01 [0.011, 0.017] |
0.02±0.01 [0.017, 0.024] |
0.007*a |
| Zero crossing fa (m) | 1.45±0.11 [1.38, 1.53] |
1.10±0.24 [0.96, 1.24] |
<0.001 *a |
| Sensitivity of MOS | −0.22±0.03 [−0.24, −0.20] |
−0.23±0.07 [−0.27, −0.19] |
0.666a |
| FSA (m/s) | 2.00±0 [2.00, 2.00] |
1.82±0.35 [1.56, 1.96] |
0.021 *b |
MOS = the Margin of Stability (fa = fore-aft direction and ml = medial-lateral direction), FSA = fast Speed Attempted, sec = second, and m/s = meter per second.
Statistically significant difference at p<0.05.
Comparison between groups by using the Independent t test.
Comparison between groups by using the Mann-Whitney U test.
Figure 2.
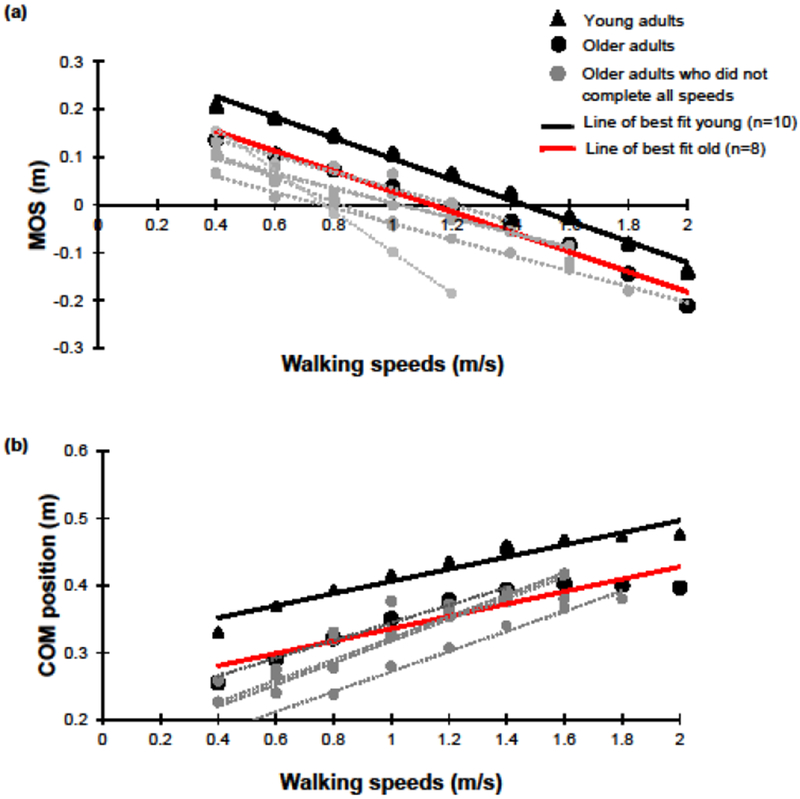
The relationship between walking speed and (a) margin of stability and (b) COM position among younger and older adults.
The distance between the COM position and the BOS at footstrike was smaller in the older adults compared with the young adults (Figure 2b). Following the mixed linear regression model analysis, the COM position did not show a significant interaction between effect of age and walking speeds (F(175.752)=0.111, p=0.739), but increasing walking speeds increased the COM position (F(175.752)=596.087, p<0.001) while older adults COM position was less than younger adults (F(35.984)=13.372, p=0.001).
Compared to older adults who completed all speeds, older adults who stopped earlier increased the variability of their MOSap between their penultimate speed and last speed attempted (0.014±0.012 and 0.001±0.009 m; (t(12)= −2.229, p=0.046). No difference was detected in variability of the MOS in medial-lateral direction from the penultimate speed to last speed attempted (0.006±0.003 and 0.003±0.007 m; t(12)= −1.016, p=0.330, Figure 3).
Figure 3.
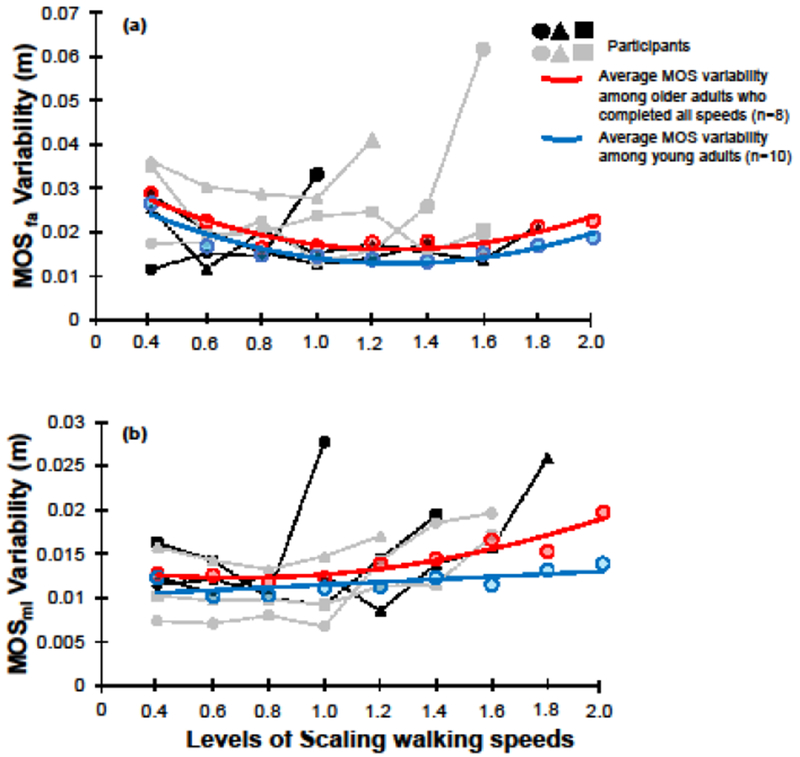
Variabilities of Margin of stability (MOS) among young adults (blue circles) and older adults who were not complete all walking speeds (a) in fore-aft direction (fa) (b) in medial-lateral direction (ml) relative with older adults who completed all speeds (red circles).
3.3. Balance confidence and walking performance in older adults
Balance confidence was correlated with measures of lab-based performance in older adults (Table 3). The ABC score correlated strongly with the fastest speed attempted (rho=0.85, p<0.001). A relationship was observed between the ABC score with the MOSap at the fastest speed attempted (rho= −0.62, p=0.004). The ABC score showed positive relationships with overground comfortable (rho=0.62, p=0.018) and maximum walking speed (rho=0.69, p=0.007) in older adults. However, no significant relationship was found between ABC score and sensitivity (rho=−0.02, p=0.93) for older adults and the ABC score did not correlate with the zero crossing (rho=0.38, p=0.18). Finally, a moderate relationship was found between the zero crossing and the fastest speed attempted (rho=0.60, p=0.022).
Table 3.
The relationships between ABC score and walking speeds at over ground among young and older adults
| ABC correlationa | ||
|---|---|---|
| Test | Young adults | Older adults |
| Sensitivity | −0.204, p=0.572 | −0.024, p=0.934 |
| CWS (m/s) | 0.355, p=0.314 | 0.619, p=0.018* |
| MWS (m/s) | −0.711, p=0.021* | 0.687, p=0.007* |
ABC = the Activities-specific Balance Confidence Scale, CWS = the Comfortable Walking Speed, MWS = the Maximum Walking Speed, sec = second, and m/s = meter per second.
Statistically significant relationship at p<0.05.
Spearman rank correlation coefficients
4. Discussion
The purpose of this study was to investigate the relationship between dynamic stability and walking speed in a group of younger and older adults and the extent that dynamic stability measured in the lab setting is related to balance confidence. We hypothesized that exposure to progressively faster speeds would result in decreased dynamic stability for older adults when compared to younger adults. Our findings demonstrated decreased dynamic stability for both older adults and younger adults at faster walking speeds. Moreover, for older adults greater, MOS variability medio-laterally and anterior-posterior along with zero crossing occurring at a slower speed were found, explaining why some older adults chose to not attempt all speeds. However, we did not detect an age-related difference in the sensitivity of dynamic stability to increasing walking speed suggesting that increasing walking speed led to similar incremental decreases in dynamic stability. Thus, our hypothesis was mostly supported. Finally, we hypothesized that balance confidence would relate to measures of stability while older adults attempted to walk at progressively faster speeds. We found significant relationships between older adults’ balance confidence and some measures of lab-based dynamic stability (i.e., the fastest speed attempted, the MOSap among older adults, however the zero crossing was not correlated. Consequently, the second hypothesis was partially supported.
4.1. Effects of age and speed on dynamic stability
Age is an important factor that affects dynamic stability while walking at progressively faster speeds. In the current study, all younger adults and only 60% of older adults attempted all possible speeds. For older adults, the speed they stopped at was related to the speed at which they became unstable anterior-posterior (i.e. zero crossing). On average, the zero-crossing occurred at a much slower speed for older adults compared to younger adults. One possible explanation is a smaller established distance on a step-by-step basis between lead limb and the COM at foot strike (Figure 2) for older adults. The negative linear relationship between speed and MOSap we show has previously been described for younger adults walking at progressively faster speeds [16]. This may be a counterintuitive finding since a negative MOS is related to dynamic instability. The extrapolated COM represents the projected position of the COM, not the actual COM position, so as long as the foot is placed anterior to the COM the braking forces can be generated which allow a transition from one limb to the next (i.e., one inverted pendulum to the next). However, the more “unstable” the MOS (i.e., the more anterior the projection of the COM) the more challenging it would be to modify the walking pattern to avoid an undesirable step location or respond to an external disturbance. Indeed, older adults with faster walking speeds are at greater risk for falls in the community[23]. In the current investigation no loss of balance was reported during the walking trials, in part, because individuals could voluntarily not attempt a faster speed. While measures of average MOS at the fastest speed attempted in both anterior-posterior and medio-lateral directions failed to separate groups, increased step-to-step variability in MOS did. Differences in the variability of steady state gait variables have consistently showed an age-related difference [13, 24] and differentiated those at a higher fall risk [25]. In fact, it has been suggested that quantifying variability of stability may be more useful than mean MOS in assessing how individuals control walking stability [26].
4.2. Dynamic stability and balance confidence by older adults
Loss of balance confidence is common in community-dwelling older people and can affect up to 75% of older adults [27]. However in some cases, loss of balance confidence appears independent of experiencing falling [28] suggesting that this could relate to a perception of instability. In this investigation, older adults who reported lower balance confidence were less willing to attempt faster walking speeds, even though no falls occurred during the data collection. It’s possible that participants were responding to internal feedback about their gait control where they did not feel the could successfully complete a faster speed. In fact, most older adults who did not complete all walking speeds showed greater anterior-posterior MOS variability in the trial before choosing to stop the data collection (Figure 3). What cannot be determined however is whether the balance confidence affected stability (i.e., they could have walked faster but did not) or whether these individuals were physically unable to control their COM at faster speeds, and thus requires further study. The instrument used to assess balance confidence was based on self-recall and was a static measure (i.e., did not assess balance confidence of performing the task). It may be helpful to develop a more dynamic measure of balance confidence to try to relate changes in dynamic stability. It has recently been suggested that anxiety is also important to consider when assessing the psychological influence on balance [29]. Greater anxiety has been shown to relate to a decline in balance confidence [30]. In order to determine the relationship between psychological influences on control of gait, observed relationships with measures of dynamic stability should be investigated.
4.3. Limitations
The present study has several limitations. Convenience sampling was used to select adults, 65-84 years old, who lived in the community for this pilot study. Thus, these results may not be generalizable to the older population as a whole. However, the results showed clear trends whereby decreased balance confidence is related to dynamic stability measured while walking. This investigation employed a rehabilitation robotic device that interfaced with participants via a pelvic harness, which may have influenced the results of this study. However, our data shows a similar negative linear trend between MOSap and speed as a previous study[16] and our MOS variability measures were of similar magnitude of other published studies [26, 31]. Thus, while we cannot rule out that device did not affect our participant’s responses, we can say that our data was similar to the extant literature. Also, cognitive function was not assessed for older participants. A link between balance and cognitive function has been discussed in the literature. Further, we are unable to separate whether balance confidence or inability to walk faster informed the participant’s choice to not attempt faster speeds. Our measure of balance confidence did not reflect how the individuals’ perception was modified by the task, thus an objective measure of balance confidence might provide a more mechanistic explanation of our present results providing the impetus for further study. Finally, the ceiling for the walking speed was set to 2.0m/s. This may not have been the maximum speed that some individuals would have attempted, however it is close to the speed that people transition to a run [21], thus this speed ensured that individuals could walk for all trials.
5. Conclusions
In summary, the current pilot study documents that older adults became unstable on a step by step basis at slower walking speeds than younger adults. Walking performance of older adults was related to their balance confidence suggesting an observable link between more cautious behavior and dynamic stability while walking. The findings of this study will help guide further research on the interaction between psychological aspects and capacity of mobility of older adults.
Highlights.
More variable stability step-by-step of older than younger adults at faster speeds
Balance confidence related with margin of stability among older adults
Lower balance confidence was indicative of slower treadmill walking speeds.
Acknowledgements
The authors would like to thank all participants for their involvement and participation in this research.
Funding: This work was supported by the Roybal Center for Research in Applied Gerontology [P30AG022838].
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of interest
CPH, JK none; DAB participates as a scientific consultant with the company HDT Global, the company that markets and sells the KineAssist device. He is a co-inventor who will potentially receive royalty payments.
References
- [1].Bergen G, Stevens MR, Burns ER. Falls and fall injuries among adults aged ≥ 65 years-United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65:993–8. [DOI] [PubMed] [Google Scholar]
- [2].Pai YC. Movement termination and stability in standing. Exerc Sport Sci Rev. 2003;31:19–25. [DOI] [PubMed] [Google Scholar]
- [3].Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH. Interventions for preventing falls in elderly people. Cochrane Database Syst Rev. 2003:CD000340. [DOI] [PubMed] [Google Scholar]
- [4].Granacher U, Muehlbauer T, Gruber M. A qualitative review of balance and strength performance in healthy older adults: impact for testing and training. J Aging Res. 2012;2012:708905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Ozdemir RA, Contreras-Vidal JL, Paloski WH. Cortical control of upright stance in elderly. Mech Ageing Dev. 2018;169:19–31. [DOI] [PubMed] [Google Scholar]
- [6].Bulea TC, Jonghyun K, Damiano DL, Stanley CJ, Hyung-Soon P. User-driven control increases cortical activity during treadmill walking: an EEG study. Conf Proc IEEE Eng Med Biol Soc. 2014;2014:2111–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Carpenter MG, Murnaghan CD, Inglis JT. Shifting the balance: evidence of an exploratory role for postural sway. Neuroscience. 2010;171:196–204. [DOI] [PubMed] [Google Scholar]
- [8].Lajoie Y, Gallagher SP. Predicting falls within the elderly community: comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparing fallers and non-fallers. Arch Gerontol Geriatr. 2004;38:11–26. [DOI] [PubMed] [Google Scholar]
- [9].Hatch J, Gill-Body KM, Portney LG. Determinants of balance confidence in community-dwelling elderly people. Phys Ther 2003;83:1072–9. [PubMed] [Google Scholar]
- [10].Marchetti GF, Whitney SL, Redfern MS, Furman JM. Factors associated with balance confidence in older adults with health conditions affecting the balance and vestibular system. Arch Phys Med Rehabil. 2011;92:1884–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].McMullan II, McDonough SM, Tully MA, Cupples M, Casson K, Bunting BP. The association between balance and free-living physical activity in an older community-dwelling adult population: a systematic review and meta-analysis. BMC Public Health. 2018;18:431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Hurt CP, Grabiner MD. Age-related differences in the maintenance of frontal plane dynamic stability while stepping to targets. J Biomech. 2015;48:592–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Hurt CP, Rosenblatt NJ, Crenshaw JR, Grabiner MD. Variation in trunk kinematics influences variation in step width during treadmill walking by older and younger adults. Gait Posture. 2010;31:461–4. [DOI] [PubMed] [Google Scholar]
- [14].Hak L, Houdijk H, Beek PJ, van Dieën JH. Steps to take to enhance gait stability: the effect of stride frequency, stride length, and walking speed on local dynamic stability and margins of stability. PLoS One. 2013;8:e82842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Hof A, Gazendam MG, Sinke WE. The condition for dynamic stability. J Biomech. 2005;38:1–8. [DOI] [PubMed] [Google Scholar]
- [16].Süptitz F, Karamanidis K, Moreno Catalá M, Brüggemann GP. Symmetry and reproducibility of the components of dynamic stability in young adults at different walking velocities on the treadmill. J Electromyogr Kinesiol. 2012;22:301–7. [DOI] [PubMed] [Google Scholar]
- [17].Rumble DD, Hurt CP, Brown DA. Step-by-step variability of swing phase trajectory area during steady state walking at a range of speeds. PLoS One. 2018;13:e0191247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Myers AM, Powell LE, Maki BE, Holliday PJ, Brawley LR, Sherk W. Psychological indicators of balance confidence: relationship to actual and perceived abilities. J Gerontol A Biol Sci Med Sci 1996;51:M37–43. [DOI] [PubMed] [Google Scholar]
- [19].Powell LE, Myers AM. The Activities-specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci. 1995;50A:M28–34. [DOI] [PubMed] [Google Scholar]
- [20].Cleary KK, Skornyakov E. Reliability and internal consistency of the activities-specific balance confidence scale. Phys Occup Ther. 2014;32:58–67. [Google Scholar]
- [21].Hreljac A Preferred and energetically optimal gait transition speeds in human locomotion. Med Sci Sports Exerc. 1993;25:1158–62. [PubMed] [Google Scholar]
- [22].Winter DA. Biomechanics and Motor Control of Human Movement. Fourth Edition ed Waterloo, Ontario, Canada: John Wiley & Sons, Inc; 2009. [Google Scholar]
- [23].Quach L, Galica AM, Jones RN, Procter-Gray E, Manor B, Hannan MT, et al. The nonlinear relationship between gait speed and falls: the Maintenance of Balance, Independent Living, Intellect, and Zest in the Elderly of Boston Study. J Am Geriatr Soc. 2011;59:1069–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Owings TM, Grabiner MD. Step width variability, but not step length variability or step time variability, discriminates gait of healthy young and older adults during treadmill locomotion. J Biomech. 2004;37:935–8. [DOI] [PubMed] [Google Scholar]
- [25].Brach JS, Berlin JE, VanSwearingen JM, Newman AB, Studenski SA. Too much or too little step width variability is associated with a fall history in older persons who walk at or near normal gait speed. J Neuroeng Rehabil. 2005;2:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].McAndrew Young PM, Wilken JM, Dingwell JB. Dynamic margins of stability during human walking in destabilizing environments. J Biomech. 2012;455:1053–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Büla CJ, Monod S, Hoskovec C, Rochat S. Interventions aiming at balance confidence improvement in older adults: an updated review. Gerontology. 2011;57:276–86. [DOI] [PubMed] [Google Scholar]
- [28].Rochat S, Büla CJ, Martin E, Seematter-Bagnoud L, Karmaniola A, Aminian K, et al. What is the relationship between fear of falling and gait in well-functioning older persons aged 65 to 70 years? Arch Phys Med Rehabil. 2010;91:879–84. [DOI] [PubMed] [Google Scholar]
- [29].Payette MC, Bélanger C, Léveillé V, Grenier S. Fall-Related Psychological Concerns and Anxiety among Community-Dwelling Older Adults: Systematic Review and Meta-Analysis. PLoS One. 2016;11:e0152848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Hull SL, Kneebone II, Farquharson L. Anxiety, depression, and fall-related psychological concerns in community-dwelling older people. Am J Geriatr Psychiatry. 2013;21:1287–91. [DOI] [PubMed] [Google Scholar]
- [31].McAndrew Young PM, Dingwell JB. Voluntary changes in step width and step length during human walking affect dynamic margins of stability. Gait Posture. 2012;36:219–24. [DOI] [PMC free article] [PubMed] [Google Scholar]