

Abstract
Purpose
Increased bone regeneration has been achieved through the use of stem cells in combination with graft material. However, the survival of transplanted stem cells remains a major concern. The purpose of this study was to evaluate the viability of transplanted mesenchymal stem cells (MSCs) at an early time point (24 hours) based on the type and form of the scaffold used, including type I collagen membrane and synthetic bone.
Methods
The stem cells were obtained from the periosteum of the otherwise healthy dental patients. Four symmetrical circular defects measuring 6 mm in diameter were made in New Zealand white rabbits using a trephine drill. The defects were grafted with 1) synthetic bone (β-tricalcium phosphate/hydroxyapatite [β-TCP/HA]) and 1×105 MSCs, 2) collagen membrane and 1×105 MSCs, 3) β-TCP/HA+collagen membrane and 1×105 MSCs, or 4) β-TCP/HA, a chipped collagen membrane and 1×105 MSCs. Cellular viability and the cell migration rate were analyzed.
Results
Cells were easily separated from the collagen membrane, but not from synthetic bone. The number of stem cells attached to synthetic bone in groups 1, 3, and 4 seemed to be similar. Cellular viability in group 2 was significantly higher than in the other groups (P<0.05). The cell migration rate was highest in group 2, but this difference was not statistically significant (P>0.05).
Conclusions
This study showed that stem cells can be applied when a membrane is used as a scaffold under no or minimal pressure. When space maintenance is needed, stem cells can be loaded onto synthetic bone with a chipped membrane to enhance the survival rate.
Keywords: Bone transplantation, Cell survival, Membranes, Stem cells, Tissue scaffolds
Graphical Abstract
INTRODUCTION
A variety of materials for bone reconstruction have been used to treat bone defects caused by various diseases or trauma [1]. Autogenous bone is recognized to be the gold standard as a graft material due to its osteogenic, osteoinductive, and osteoconductive properties [2]. The disadvantage of autogenous bone lies in its quick resorption after transplantation, lower space maintenance, and the need for an additional surgical procedure during harvest [3,4]. Conversely, synthetic bone functions well as a space maintainer and scaffold, but has no or limited osteogenic and osteoinductive ability [5].
Recently, several studies have explored the effects of mesenchymal stem cells, which have the capability to differentiate into bone, cartilage, and muscle, on bone regeneration [6,7]. The use of stem cells with a synthetic or xenogenic bone graft enhanced bone regeneration when compared with a bone graft alone, possibly due to the osteogenic and osteoinductive properties of stem cells [8,9]. Previous studies have shown that a combination of stem cells with bone graft material improved bone regeneration [10,11]. In addition, successful bone regeneration was achieved in participants with large bony defects by applying stem cells [12,13]. It cannot be overlooked that a significant amount of stem cells will migrate into bone defects over time [14]. It can be assumed that the adhesion of transplanted cells and/or migrated cells may vary depending on the type and nature of the scaffold [15]. Collagen, a component of the extracellular matrix of bone tissue, has been shown to promote osteogenic differentiation in stem cells and to enhance cell adhesion at the early stage of bone graft transplantation [16]. Moreover, cell adhesion and osteogenesis were found to be improved when collagen was applied in combination with hydroxyapatite [17]. The purpose of this study was to evaluate the viability of transplanted stem cells at an early time point (24 hours) based on the type and form of the scaffold used, including type I collagen membrane and synthetic bone.
MATERIALS AND METHODS
Obtaining the stem cells
Approximately 1 cm2 of periosteum was removed during surgical procedures, including tooth extraction and periodontal surgery, from otherwise healthy patients visiting the dental clinic of Uijeongbu St. Mary's Hospital. The participants did not have any systemic diseases. We obtained the approval of the Institutional Review Board at Uijeongbu St. Mary's Hospital's College of Medicine and the Catholic University of Korea (UC12TISI0046).
Isolation and culture of stem cells derived from the periosteum were performed as follows. The periosteum was placed in sterile phosphate-buffered saline (PBS; Gibco BRL, Grand Island, NY, USA) containing 1% antibiotic and antimycotic (Gibco BRL). The periosteum was then washed with PBS (Gibco BRL) and cut into 1–2 mm2 fragments in sterile conditions. The tissues were digested with 0.06% collagenase type II (Invitrogen Corporation, Carlsbad, CA, USA) and incubated at 37°C in a humidified incubator (Forma Scientific Inc, Marietta, OH, USA) with 5% CO2 and 95% air for 4 hours. The periosteum-derived cells were filtered through a 70-μm cell strainer (BD Bioscience, Two Oak Park, Bedford, MA, USA), and centrifuged at 1,500 rpm for 5 minutes. The precipitates were suspended in Dulbecco's modified Eagle medium (Gibco BRL) containing 10% fetal bovine serum and 1% penicillin-streptomycin (Gibco BRL) and cultured in an incubator. Each day, the morphological characteristics of cells were observed under a microscope. When necessary, the culture medium was exchanged. Cells not attached to the culture dish were removed, and only the attached cells were cultured. Upon reaching 90% confluence, cells were subcultured with a coenzyme solution composed of trypsin (Gibco BRL) and ethylenediaminetetraacetic acid (EDTA; Gibco BRL). Stem cells were identified by the surface markers STRO-1 (R&D Systems, Minneapolis, MN, USA) and CD146 (R&D Systems) using a fluorescence-activated cell sorter (FACS, BD Biosciences, Bedford, MA, USA). Stem cells were subcultured several times to obtain a sufficient number of cells (Figure 1A). Fluorescent staining was performed to confirm the survival of transplanted stem cells (Figure 1B). In short, the viability of cell spheroids was qualitatively analyzed using a Live/Dead Viability/Cytotoxicity Kit for Mammalian Cells (Thermo Fisher Scientific, Waltham, MA, USA). The cells were washed and suspended in 10 mL of phosphate-buffered saline, followed by addition of 5 μL of 50 mM calcein acetoxymethyl ester solution and 20 μL of ethidium homodimer-1 for 20 minutes at room temperature.
Figure 1. Stem cells used for transplantation. (A) Cultured stem cells derived from the periosteum. (B) Periosteum-derived stem cells before transplantation. Fluorescent staining was performed before transplantation to confirm the survival of transplanted stem cells.

Animal experiments
New Zealand white rabbits weighing between 2.5 and 3.0 kg were used as experimental animals. All animal experiments were strictly carried out following the approval of the Ethics Committee for Animal Experiment of Uijeongbu St. Mary's Hospital, the Catholic University of Korea (UJA2017-05A).
General anesthesia was induced with tiletamine and zolazepam (15 mg/kg, Zoletil 50; Virbac Laboratories, Carros, France) and xylazine (5 mg/kg, Kepro BV, Deventer, Netherlands) intramuscularly and hair removal was performed. After disinfection with povidone-iodine (Sung Kwang Pharm, Seoul, Korea), local anesthesia was achieved with a 2% lidocaine solution containing epinephrine (Yuhan Co., Seoul, Korea).
A skin incision was made from the nasofrontal area to the external occipital area, and a periosteal flap was raised to expose the cranium. Four symmetrical circular defects 6 mm in diameter were made using a trephine drill (Figure 2A). The defects were grafted with 1) synthetic bone (β-tricalcium phosphate/hydroxyapatite [β-TCP/HA] with a particle size of 410–1,000 μm and a β-TCP-to-HA ratio of 7:3; Cowellmedi Co., Ltd, Seoul, Korea) and 1×105 MSCs, 2) a collagen membrane (type I collagen membrane, CollaTape®, Zimmer Dental Co., Carlsbad, CA, USA) and 1×105 MSCs, 3) β-TCP/HA+a collagen membrane and 1×105 MSCs, or 4) β-TCP/HA, a chipped collagen membrane, and 1×105 MSCs (Figure 2B). Efforts were made to apply the same amount of synthetic bone and/or collagen membrane in each group. The stem cells were incubated with the graft material for 1 hour before transplantation. The defects were then covered with a Teflon sheet (W.L. Gore & Associates Inc., Flagstaff, AZ, USA) and titanium screws (Figure 2C). The periosteum was released at its base, and the wound margins were reapproximated and closed with a non-absorbable suture (3-0 black silk; Ailee Co. Ltd, Busan, Korea).
Figure 2. Surgical procedure. (A) Bone defects were made in the rabbit calvarium. A circular defect with a diameter of 6 mm was formed in the skull. (B) The groups were designated as follows; group 1: β-TCP/HA+1×105 MSCs, group 2: type I collagen membrane+1×105 MSCs, group3: β-TCP/HA+type I collagen membrane+1×105 MSCs and group 4: β-TCP/HA+type I collagen chipped membrane+1×105 MSCs. (C) A Teflon sheet was applied and titanium screws were placed before suturing. The periosteum and scalp were replaced with non-absorbable sutures. (D) Harvesting of the grafted tissue was done at 24 hours after surgery.

β-TCP/HA: β-tricalcium phosphate/hydroxyapatite, MSCs: mesenchymal stem cells.
After surgery, all rabbits received subcutaneous injections of antibiotics (4 mg/kg gentamicin) and anti-inflammatory analgesics (1 mg/kg ketoprofen) once per day. An E-collar (Saf-T-Shield, EJAY International Inc., Glendora, CA, USA), was placed to prevent injuries to the surgical field and fresh vegetables, including cabbage, were supplied to promote the animals' recovery. The transplanted cells and scaffold were retrieved 24 hours later using various instruments, including curettes, and the remaining portion was retrieved by pipetting (Figure 2D).
Evaluation of the cellular experiments
The cells were retrieved through the following procedure. Tissues from the rabbit skulls were placed in a 1.5 mL tube and centrifuged. After removing the supernatant, the cells were washed with phosphate-buffered saline and then treated with collagenase type II (Gibco BRL) at 1 mg/mL for groups 2, 3, and 4, which contained collagen membranes. The cells were incubated for 30 minutes to 1 hour to dissolve the collagen. All tissues were centrifuged twice at 1,200 rpm for 5 minutes. The cells were then mixed with 9 mL of distilled water and 1 mL of ×10 PBS (Gibco BRL) for 15 seconds and then centrifuged at 1,700 rpm for 6 minutes to hemolyze the red blood cells. After removing the supernatant, 1 mL of PBS and 1 mL of trypan blue solution (T-8154, Merck KGaA, Darmstadt, Germany) were mixed. Next, the number of total cells, the number of live cells, and the ratio of live cells were analyzed using an automated cell counter (TC 20TM, Bio-Rad Laboratories, Berkeley, CA, USA). Before transplantation, the fluorescent-stained stem cells were observed with an inverted microscope (IX71; Olympus Co., Tokyo, Japan) and were photographed with a digital camera (DP70; Olympus Co.). A quantitative evaluation was performed by comparing and analyzing the measured values for each defect.
Statistical analysis
Data were presented as mean ± standard deviation. Statistical analysis was performed using SPSS version 12 for Windows (SPSS Inc., Chicago, IL, USA). The normality of the distribution of the data was tested, and one-way analysis of variance with the Tukey B post hoc test was used to evaluate between-group differences. The significance level of this study was set to P<0.05.
RESULTS
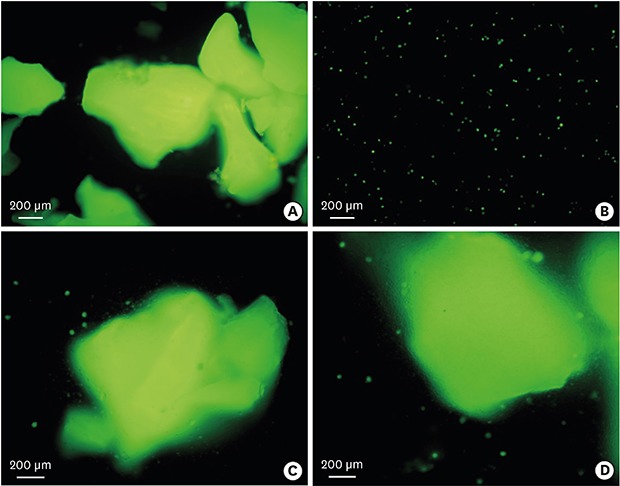
Cells were extracted from the collected tissues and the number of total cells and number of viable cells were measured. Cells were easily separated from the collagen membrane, but cells attached to the synthetic bone were not easily separated (Figure 3). The number of stem cells attached to the synthetic bone in groups 1, 3, and 4 seemed to be similar.
Figure 3. Fluorescent microscopic evaluation of the grafted tissue. (A) Group 1 (β-TCP/HA+MSCs): Viable MSCs were attached to β-TCP/HA. (B) Group 2 (collagen membrane+MSCs): The surviving MSCs that had been transplanted were easily separated from the collagen membrane. (C) Group 3 (β-TCP/HA+collagen membrane+MSCs). The surviving MSCs that had been transplanted were abundantly attached to the β-TCP/HA, and a small amount of MSCs were scattered around the β-TCP/HA. (D) Group 4 (β-TCP/HA+chipped collagen membrane+MSCs). The results were similar to those of group 3.

β-TCP/HA: β-tricalcium phosphate/hydroxyapatite, MSCs: mesenchymal stem cells.
Cellular viability in tissue
The percentage of viable cells in the tissues was calculated as follows: cellular viability=number of total viable cells/number of total cells collected [18]. In group 2, this percentage was significantly higher than in the other groups (Figure 4).
Figure 4. Cell viability in each group was calculated by dividing the number of harvested live cells by the total number of harvested cells on day 1.

a)A statistically significant difference was seen between group 2 and group 1 on day 1.
Cell migration rate
The rate of cell migration was calculated by dividing the number of total cells collected by the number of total cells transplanted [19]. The number of total cells reflected the sum of the number of transplanted cells that were not lost and the number of cells that migrated from neighboring areas. The cell migration rate was highest in group 2, but a statistically significant difference was not found (P>0.05) (Figure 5).
Figure 5. The cell migration rate was calculated by dividing the total number of harvested cells by the total number of grafted cells on day 1.

Cell survival rate
The cell survival rate was calculated by dividing the total number of viable cells collected by the number of surviving transplanted cells [20]. The values were highest in group 2 (P<0.05). However, there was no statistically significant difference among groups 1, 3, and 4 (P>0.05) (Figure 6).
Figure 6. The survival rate of cells was calculated by dividing the number of harvested live cells by the number of grafted live cells on day 1.

DISCUSSION
This study showed that the highest survival rate was found when the stem cells were applied to a membrane. When synthetic bone was used, utilizing a chipped membrane enhanced cell survival.
The survival of transplanted stem cells remains a major concern [21,22]. Human cord blood-derived stem cells were transplanted into a critically sized femoral defect with a combined collagen/β-TCP scaffold, and the transplanted cells were reported to survive for up to 4 weeks [23]. Amniotic fluid-derived stem cells were applied to a collagen/hydroxyapatite scaffold in sinus augmentation procedures, and survival of stem cells was observed 90 days after surgery [24]. An important consideration is that it was easy to separate cells from collagen scaffolds, but the cells attached to synthetic bone were not easily separated. However, a previous study suggested that the absolute value of viability of the transplanted cells may decrease significantly, even if their survival is maintained [25]. Unlike the stable environment of the laboratory, in vivo bone defects have the possibility of leakage or loss of transplanted cells due to active bleeding or blood circulation [26].
Collagen is known to be involved in the enhancement of adhesion, proliferation, and survival of stem cells [27]. It was shown that cell attachment ability in the early phase and osteogenic differentiation were significantly enhanced in collagen-grafted porous biphasic calcium phosphate (BCP) when compared with BCP alone [16]. Human mesenchymal stem cells were cultured in a three-dimensional collagen scaffold, and a large number of osteoblasts were identified after a 50-day culture period [28]. However, it should be considered that when compared with group 2, the cells from the other groups (groups 1, 3, and 4) were securely attached to the synthetic bone and not easily separated, and direct comparison between the groups may not be feasible. It can be assumed that a direct comparison between groups 1, 3, and 4 can be made because the same amount of synthetic bone was loaded and the number of attached cells was similar. Comparing groups 1, 3, and 4, in which synthetic bone was loaded, the cell viability, cell migration, and survival rates were increased by the addition of collagen membrane. Moreover, applying a chipped membrane enhanced the survival rate, but this finding did not reach statistical significance. Cells that do not adhere to the scaffold may die prematurely, and addition of collagen may decrease the loss of the transplanted cells and enhance their viability [29]. The transplanted cells may undergo differentiation into bone cells under the influence of the surrounding environment, and stem cells may have paracrine effects by producing various factors, including growth factors [30,31,32]. In this regard, higher cell viability and survival may have beneficial effects. In this study, the stem cells were incubated for 1 hour before transplantation to allow cells to adhere to the scaffold [33,34].
Various methods have been suggested to enhance functionality [22,35,36]. A previous report showed that three-dimensional stem cell spheroids exhibited greater resistance to apoptosis than dissociated stem cells in fibrin gels [37]. A self-assembling peptide nanofiber was applied to enhance the survival and osteogenic differentiation of peripheral blood mesenchymal stem cells in three-dimensional conditions [22]. A further study reported that fibrin gel properties were modified by supplementation with NaCl, which promoted the proangiogenic and osteogenic potential of stem cells [35]. An arginine-glycine-aspartic acid tripeptide (RGD)–modified alginate scaffold showed enhanced mesenchymal stem cell viability and osteogenic differentiation when compared with a non-modified scaffold [36]. Bone morphogenetic proteins (BMPs), including BMP-2, may be applied for bone regeneration because BMPs are capable of stimulating osteogenic differentiation during the healing period [38].
In conclusion, this study showed that stem cells could be applied to a membrane used as a scaffold under no or minimal pressure. When space maintenance is needed, stem cells can be loaded onto synthetic bone with a chipped membrane to enhance the survival rate.
ACKNOWLEDGEMENTS
The authors wish to acknowledge the financial support of The Catholic University of Korea Uijeongbu St. Mary's Hospital Clinical Research Laboratory Foundation in the program year of 2018.
Footnotes
- Conceptualization: Seung-Hwan Kang, Jun-Beom Park, InSoo Kim.
- Data curation:
- Formal analysis: Seung-Hwan Kang, Jun-Beom Park, InSoo Kim.
- Funding acquisition:
- Investigation: Seung-Hwan Kang, Jun-Beom Park, InSoo Kim, Won Lee, Heesung Kim.
- Methodology: Seung-Hwan Kang, Jun-Beom Park, InSoo Kim, Won Lee, Heesung Kim.
- Project administration:
- Resources:
- Software:
- Supervision:
- Validation:
- Visualization:
- Writing - original draft: Seung-Hwan Kang, Jun-Beom Park, InSoo Kim.
- Writing - review & editing: Seung-Hwan Kang, Jun-Beom Park, InSoo Kim, Won Lee, Heesung Kim.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
References
- 1.Wang W, Yeung KW. Bone grafts and biomaterials substitutes for bone defect repair: a review. Bioact Mater. 2017;2:224–247. doi: 10.1016/j.bioactmat.2017.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kubota T, Hasuike A, Ozawa Y, Yamamoto T, Tsunori K, Yamada Y, et al. Regenerative capacity of augmented bone in rat calvarial guided bone augmentation model. J Periodontal Implant Sci. 2017;47:77–85. doi: 10.5051/jpis.2017.47.2.77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fernández-Domínguez M, Ortega-Asensio V, Fuentes-Numancia E, Aragoneses JM, Barbu HM, Ramírez-Fernández MP, et al. Can the macrogeometry of dental implants influence guided bone regeneration in buccal bone defects? Histomorphometric and biomechanical analysis in beagle dogs. J Clin Med. 2019;8:8. doi: 10.3390/jcm8050618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ohta K, Tada M, Ninomiya Y, Kato H, Ishida F, Abekura H, et al. Application of interconnected porous hydroxyapatite ceramic block for onlay block bone grafting in implant treatment: a case report. Exp Ther Med. 2017;14:5564–5568. doi: 10.3892/etm.2017.5224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bertolai R, Catelani C, Aversa A, Rossi A, Giannini D, Bani D. Bone graft and mesenchimal stem cells: clinical observations and histological analysis. Clin Cases Miner Bone Metab. 2015;12:183–187. doi: 10.11138/ccmbm/2015.12.2.183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Park JB, Cho SH, Kim I, Lee W, Kang SH, Kim H. Evaluation of the bisphosphonate effect on stem cells derived from jaw bone and long bone rabbit models: a pilot study. Arch Oral Biol. 2018;85:178–182. doi: 10.1016/j.archoralbio.2017.10.024. [DOI] [PubMed] [Google Scholar]
- 7.Tae JY, Lee H, Lee H, Ko Y, Park JB. Osteogenic potential of cell spheroids composed of varying ratios of gingiva-derived and bone marrow stem cells using concave microwells. Exp Ther Med. 2018;16:2287–2294. doi: 10.3892/etm.2018.6462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Namli H, Erdogan Ö, Gönlüşen G, Kahraman OE, Aydin HM, Karabag S, et al. Vertical bone augmentation using bone marrow-derived stem cells: an in vivo study in the rabbit calvaria. Implant Dent. 2016;25:54–62. doi: 10.1097/ID.0000000000000334. [DOI] [PubMed] [Google Scholar]
- 9.Khadka A, Li J, Li Y, Gao Y, Zuo Y, Ma Y. Evaluation of hybrid porous biomimetic nano-hydroxyapatite/polyamide 6 and bone marrow-derived stem cell construct in repair of calvarial critical size defect. J Craniofac Surg. 2011;22:1852–1858. doi: 10.1097/SCS.0b013e31822e8274. [DOI] [PubMed] [Google Scholar]
- 10.Daei-Farshbaf N, Ardeshirylajimi A, Seyedjafari E, Piryaei A, Fadaei Fathabady F, Hedayati M, et al. Bioceramic-collagen scaffolds loaded with human adipose-tissue derived stem cells for bone tissue engineering. Mol Biol Rep. 2014;41:741–749. doi: 10.1007/s11033-013-2913-8. [DOI] [PubMed] [Google Scholar]
- 11.Yang P, Huang X, Wang C, Dang X, Wang K. Repair of bone defects using a new biomimetic construction fabricated by adipose-derived stem cells, collagen I, and porous beta-tricalcium phosphate scaffolds. Exp Biol Med (Maywood) 2013;238:1331–1343. doi: 10.1177/1535370213505827. [DOI] [PubMed] [Google Scholar]
- 12.Sándor GK, Tuovinen VJ, Wolff J, Patrikoski M, Jokinen J, Nieminen E, et al. Adipose stem cell tissue-engineered construct used to treat large anterior mandibular defect: a case report and review of the clinical application of good manufacturing practice-level adipose stem cells for bone regeneration. J Oral Maxillofac Surg. 2013;71:938–950. doi: 10.1016/j.joms.2012.11.014. [DOI] [PubMed] [Google Scholar]
- 13.Zamiri B, Shahidi S, Eslaminejad MB, Khoshzaban A, Gholami M, Bahramnejad E, et al. Reconstruction of human mandibular continuity defects with allogenic scaffold and autologous marrow mesenchymal stem cells. J Craniofac Surg. 2013;24:1292–1297. doi: 10.1097/SCS.0b013e318294288a. [DOI] [PubMed] [Google Scholar]
- 14.Kim SJ, Kim MR, Oh JS, Han I, Shin SW. Effects of polycaprolactone-tricalcium phosphate, recombinant human bone morphogenetic protein-2 and dog mesenchymal stem cells on bone formation: pilot study in dogs. Yonsei Med J. 2009;50:825–831. doi: 10.3349/ymj.2009.50.6.825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wu H, Liu GH, Wu Q, Yu B. Repairing rabbit radial defects by combining bone marrow stroma stem cells with bone scaffold material comprising a core-cladding structure. Genet Mol Res. 2015;14:11933–11943. doi: 10.4238/2015.October.5.7. [DOI] [PubMed] [Google Scholar]
- 16.Yang DJ, Jeon JH, Lee SY, An HW, Park KO, Park KB, et al. Effects of collagen grafting on cell behaviors in BCP scaffold with interconnected pore structure. Biomater Res. 2016;20:3. doi: 10.1186/s40824-016-0049-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Villa MM, Wang L, Rowe DW, Wei M. Effects of cell-attachment and extracellular matrix on bone formation in vivo in collagen-hydroxyapatite scaffolds. PLoS One. 2014;9:e109568. doi: 10.1371/journal.pone.0109568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Koury MJ, Bondurant MC. Maintenance by erythropoietin of viability and maturation of murine erythroid precursor cells. J Cell Physiol. 1988;137:65–74. doi: 10.1002/jcp.1041370108. [DOI] [PubMed] [Google Scholar]
- 19.Piltti KM, Avakian SN, Funes GM, Hu A, Uchida N, Anderson AJ, et al. Transplantation dose alters the dynamics of human neural stem cell engraftment, proliferation and migration after spinal cord injury. Stem Cell Res (Amst) 2015;15:341–353. doi: 10.1016/j.scr.2015.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zhang H, Chen H, Wang W, Wei Y, Hu S. Cell survival and redistribution after transplantation into damaged myocardium. J Cell Mol Med. 2010;14:1078–1082. doi: 10.1111/j.1582-4934.2010.01076.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Alfotawei R, Naudi KB, Lappin D, Barbenel J, Di Silvio L, Hunter K, et al. The use of TriCalcium Phosphate (TCP) and stem cells for the regeneration of osteoperiosteal critical-size mandibular bony defects, an in vitro and preclinical study. J Craniomaxillofac Surg. 2014;42:863–869. doi: 10.1016/j.jcms.2013.12.006. [DOI] [PubMed] [Google Scholar]
- 22.Wu G, Pan M, Wang X, Wen J, Cao S, Li Z, et al. Osteogenesis of peripheral blood mesenchymal stem cells in self assembling peptide nanofiber for healing critical size calvarial bony defect. Sci Rep. 2015;5:16681. doi: 10.1038/srep16681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jäger M, Degistirici O, Knipper A, Fischer J, Sager M, Krauspe R. Bone healing and migration of cord blood-derived stem cells into a critical size femoral defect after xenotransplantation. J Bone Miner Res. 2007;22:1224–1233. doi: 10.1359/jbmr.070414. [DOI] [PubMed] [Google Scholar]
- 24.Berardinelli P, Valbonetti L, Muttini A, Martelli A, Peli R, Zizzari V, et al. Role of amniotic fluid mesenchymal cells engineered on MgHA/collagen-based scaffold allotransplanted on an experimental animal study of sinus augmentation. Clin Oral Investig. 2013;17:1661–1675. doi: 10.1007/s00784-012-0857-3. [DOI] [PubMed] [Google Scholar]
- 25.Robey TE, Saiget MK, Reinecke H, Murry CE. Systems approaches to preventing transplanted cell death in cardiac repair. J Mol Cell Cardiol. 2008;45:567–581. doi: 10.1016/j.yjmcc.2008.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Amini AR, Laurencin CT, Nukavarapu SP. Bone tissue engineering: recent advances and challenges. Crit Rev Biomed Eng. 2012;40:363–408. doi: 10.1615/critrevbiomedeng.v40.i5.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Somaiah C, Kumar A, Mawrie D, Sharma A, Patil SD, Bhattacharyya J, et al. Collagen promotes higher adhesion, survival and proliferation of mesenchymal stem cells. PLoS One. 2015;10:e0145068. doi: 10.1371/journal.pone.0145068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Neuss S, Stainforth R, Salber J, Schenck P, Bovi M, Knüchel R, et al. Long-term survival and bipotent terminal differentiation of human mesenchymal stem cells (hMSC) in combination with a commercially available three-dimensional collagen scaffold. Cell Transplant. 2008;17:977–986. doi: 10.3727/096368908786576462. [DOI] [PubMed] [Google Scholar]
- 29.Tiwari S, Patil R, Bahadur P. Polysaccharide based scaffolds for soft tissue engineering applications. Polymers (Basel) 2018;11:11. doi: 10.3390/polym11010001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Linero I, Chaparro O. Paracrine effect of mesenchymal stem cells derived from human adipose tissue in bone regeneration. PLoS One. 2014;9:e107001. doi: 10.1371/journal.pone.0107001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Deb A. How stem cells turn into bone and fat. N Engl J Med. 2019;380:2268–2270. doi: 10.1056/NEJMcibr1905165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Robey PG. Cell sources for bone regeneration: the good, the bad, and the ugly (but promising) Tissue Eng Part B Rev. 2011;17:423–430. doi: 10.1089/ten.teb.2011.0199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lawrence LM, Cottrill A, Valluri A, Marenzi G, Denning KL, Valluri J, et al. Minimally manipulative method for the expansion of human bone marrow mesenchymal stem cells to treat osseous defects. Int J Mol Sci. 2019;20:20. doi: 10.3390/ijms20030612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dow J, Simkhovich BZ, Kedes L, Kloner RA. Washout of transplanted cells from the heart: a potential new hurdle for cell transplantation therapy. Cardiovasc Res. 2005;67:301–307. doi: 10.1016/j.cardiores.2005.04.011. [DOI] [PubMed] [Google Scholar]
- 35.Murphy KC, Hughbanks ML, Binder BY, Vissers CB, Leach JK. Engineered fibrin gels for parallel stimulation of mesenchymal stem cell proangiogenic and osteogenic potential. Ann Biomed Eng. 2015;43:2010–2021. doi: 10.1007/s10439-014-1227-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Moshaverinia A, Chen C, Xu X, Akiyama K, Ansari S, Zadeh HH, et al. Bone regeneration potential of stem cells derived from periodontal ligament or gingival tissue sources encapsulated in RGD-modified alginate scaffold. Tissue Eng Part A. 2014;20:611–621. doi: 10.1089/ten.tea.2013.0229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Murphy KC, Fang SY, Leach JK. Human mesenchymal stem cell spheroids in fibrin hydrogels exhibit improved cell survival and potential for bone healing. Cell Tissue Res. 2014;357:91–99. doi: 10.1007/s00441-014-1830-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Scarfì S. Use of bone morphogenetic proteins in mesenchymal stem cell stimulation of cartilage and bone repair. World J Stem Cells. 2016;8:1–12. doi: 10.4252/wjsc.v8.i1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]