

Abstract
The aims of this study were to assess bone mass in children and adolescent soccer players and to evaluate the influence of both gender and pubertal status on bone mass. A total of 110 soccer players (75 males / 35 females; 12.73 ± 0.65 / 12.76 ± 0.59 years) participated in this cross-sectional study. They were divided into two groups according to their pubertal status. Bone and lean masses were measured with Dual-energy X-ray Absorptiometry. An independent t-test and an adjusted by subtotal lean and training experience multivariate analysis of covariance were used to analyse the differences in bone mass values between genders and maturity status. Female soccer players presented higher bone mass values than their male counterparts in most of the measured weight-bearing sites. Moreover, when stratifying by pubertal status, peripubertal and postpubertal females had higher subtotal body and lumbar spine bone mass than males. Comparing between pubertal status groups before adjustment, both male and female postpubertal players showed higher bone mass than their pubertal counterparts. After adjusting, these differences disappeared and, in fact results were inverted as bone mass at the femoral neck was higher in both male and female peripubertal soccer players than in postpubertal players. Bone mass seems to be more intensely stimulated by playing soccer in female than male players, particularly in the lumbar spine. The results of peripubertal players showing higher bone mass at the femoral neck after adjusting suggest that playing soccer during the peripubertal stage could be an effective activity to achieve optimal bone mass values.
Key words: soccer, sports, bone density, adolescent
Introduction
Osteoporosis is a disease characterised by low bone mineral density (BMD) and microarchitectural deterioration. According to the World Health Organization (WHO), this disease affects approximately 75 million people in the United States, Europe, and Japan (WHO, 2004). Moreover, the National Osteoporosis Foundation (NOF) reported that one in two women and one in four men over 50 years old would suffer a bone fracture due to osteoporosis. The interest in assessing bone mass during adolescence has increased as this period is an essential stage to reach appropriate bone development (Wallace and Ballard, 2002) and almost 90% of bone mass in adults is obtained during this period in life. Furthermore, genetics, nutrition, hormones, and mechanical factors (Cousins et al., 2010; Rizzoli et al., 2010) help to attain adequate values of bone mass at this stage and consequently, to prevent osteoporotic fractures during one’s elderly years. In addition, bone mass can also be altered by playing sport (Vicente-Rodriguez et al., 2003), but not all sports provoke the same osteogenic effect. Therefore, classification according to the influence of sports participation on bone health has been proposed: low-impact sports, such as swimming and cycling; odd-impact sports, such as soccer, basketball, and racquet games; or high-impact sports, such as volleyball and karate (Tenforde and Fredericson, 2011).
Focusing on soccer, this odd-impact sport has been defined by a combination of high-intensity actions such as running, changes of direction, starts, stops, jumps, and kicks, that have a positive effect on bone mass (Bangsbo, 1994). Moreover, it is most likely one of the most practised sports by children and adolescents worldwide. This fact has prompted research to focus studies on the effects of soccer on bones, reporting bone mass improvements after playing soccer in different periods of life, such as childhood (Vicente-Rodriguez et al., 2004), adolescence (Ferry et al., 2011; Lozano-Berges, 2018), and adulthood (Calbet et al., 2001). Nevertheless, neither Soderman et al. (2000) (females) nor Zouch et al. (2008) (males) found bone mineral content (BMC) and BMD differences between soccer players and a control group. On the other hand, a longitudinal study found that whole body, total hip, and lower limbs BMD values were higher in soccer players than controls after one year of playing soccer (Zouch et al., 2008). Therefore, the effects of playing soccer on bone mass are still fully unknown.
The period of life in which soccer is practised also seems important to bone mass acquisition, as stronger influences on bone mass were demonstrated in pubertal male (Nebigh et al., 2009; Zouch et al., 2014) and female (Soderman et al., 2000; Ubago-Guisado et al., 2015) soccer players than in their prepubertal counterparts when these players were compared with controls. However, only Zouch et al. (2014) directly evaluated differences between prepubertal and pubertal soccer players. On the other hand, only McCulloch et al. (1992) analysed differences between genders, showing no differences in BMC and BMD between male and female players.
Overall, it has been shown that playing soccer may improve bone health in young males and females, although the effects of soccer according to pubertal status or gender still remain unclear. Therefore, the aims of this study were as follows: 1) to assess bone mass in a group of adolescent soccer players, and 2) to evaluate the influence of both gender and pubertal status on BMC and BMD. We hypothesized that female soccer players would exhibit higher bone mass than their male counterparts either in the peripubertal or postpubertal periods because females accumulate bone earlier than males.
Methods
Participants
Eight soccer clubs (all of them competed at the regional level for their age category) of Aragon (Spain) were invited to participate in this study. A total of 121 soccer players (81 males and 40 females) agreed to participate in the study. However, 11 players (6 males and 5 females) were not included because they did not participate in the measurements. Consequently, the final sample for the present study consisted of 110 soccer players (75 males and 35 females; mean age 12.73 ± 0.65 and 12.76 ± 0.59 years, respectively). Twenty female players (10 peripubertal and 10 postpubertal; mean age of 11.45 ± 1.19 years) had achieved the menarche (at the mean age of 11.45 ± 1.19 years) before the beginning of the present study.
Training experience ranged from 1 to 10 years in peripubertal males, from 2 to 9 years in postpubertal males, from 1 to 8 years in peripubertal females, and from 1 to 9 years in postpubertal females. Although the range of training experience was wide, no significant differences were found between peripubertal and postpubertal players either in males (χ2(10) = 12.48, p = 0.254) or females (χ2(7) = 6.95, p = 0.435). On the other hand, despite not following the same training program, training of all teams included in this study (both genders) lasted approximately 90 min, including a 5-min warm-up consisting of low-intensity running; 5-10 min of low-intensity games; 60 min of technical soccer exercises (e.g. passing, kicking, running, dribbling); and finally, 5-10 minutes of cool down exercises. All teams that participated in the present study played one match per week and trained two days per week, except one male team that trained 3 days per week (this team had 15 peripubertal and 3 postpubertal players).
The participants, their parents, and clubs were informed about the protocol of this study, its benefits, and risks. Written informed consent from parents and verbal assent from the participants were obtained. This study followed the declaration of Helsinki 1961 (revision of Fortaleza, 2013).
Measures
Anthropometric measurements
Body height was measured with a stadiometer to the nearest 0.1 cm (SECA 225, SECA, Hamburg, Germany) and body mass was evaluated using a medical scale to the nearest 0.1 kg (SECA, Hamburg, Germany) without shoes and with minimum clothing. The body mass index (BMI) was calculated according to the equation BMI (kg·m-2) = Body mass/Body height2.
Pubertal development
Pubertal status was self-determined according to the pubertal stages proposed by Tanner and Whitehouse (1976). Adolescents’ self-assessment of sexual maturation according to Tanner’s standard photographs has been found as a valid and reliable method (Duke et al., 1980).
Participants were classified into two groups: peripubertal (Tanner II and III) and postpubertal players (Tanner IV and V) to compare bone mass by sexual maturation.
Bone and lean mass measurements by Dual X-ray Absorptiometry (DXA)
Bone and lean masses were evaluated with DXA QDR-Explorer (paediatric version of the software QDR-Explorer, Hologic Corp. Software version 12.4, Bedford, Massachusetts, USA). DXA equipment was calibrated daily following the manufacturer’s guidelines. Whole body, non-dominant hip, and lumbar spine scans were performed in a supine position by the same technician who was fully trained to perform the scans. BMC (g) and lean mass (g) were obtained from the total and regional analyses of the whole body. The subregions evaluated in this study were the subtotal body and mean legs from the whole-body test; the hip and femoral neck from the hip test; and total lumbar spine from the lumbar spine test. The coefficients of variation of the DXA in our laboratory are published elsewhere (Garcia-Marco et al., 2012).
Procedures
The protocol of this study was approved by the Ethics Committee of Clinical Research from the Government of Aragon (CEICA, Spain) [C.I. PI13/0091]. The research was registered in the public database Clinicaltrials.gov [NCT02399553]. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement was used as a guideline for reporting observational studies (von Elm et al., 2007).
All participants were measured between November and December of 2013 in the Laboratory of Zaragoza, Spain. These participants had to be Caucasian, with at least one year of soccer training experience, between 11 and 14 years old, and free of medication that could affect bone mass.
Statistical analysis
The sample size was calculated for whole body BMD by a bilateral Student’s t-test for two independent samples to obtain a power of 95% and to observe differences in comparison to a null hypothesis H0:μ1 = μ2. Taking into account that the confidence level was 95% and assuming that the means of male and female soccer players were 0.942 and 0.980, respectively, and the standard deviation of both groups was 0.037, 52 soccer players (26 males and 26 females) were needed. Sample size calculations were developed with G*Power 3.1 (Düsseldorf, Germany)
The Statistical Package for the Social Sciences (SPSS) version 22.0 for Mac OS X (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. All variables demonstrated normal distribution with the Kolmogorov-Smirnov test. Results were presented as means ± standard deviation (SD).
Two independent t-tests were performed in order to compare subject characteristics and bone mass variables between groups. A multivariate analysis of covariance (MANCOVA) was used to analyse differences in BMC and BMD variables between pubertal status and genders, using subtotal body lean mass, due to its influence on bone mass (Vicente-Rodriguez et al., 2008), and training experience as covariates. Effect size statistics using Cohen´s d and partial eta square were calculated. The effect size for Cohen´s d was considered small (0.2 – 0.5), medium (0.5 – 0.8) or large (>0.8); and the effect size n2p was estimated as small (0.01 – 0.06), medium (0.06 – 0.14) or large (>0.14). Statistical significance was set at p < 0.05.
Results
Characteristics of the participants by gender and pubertal status are showed in Table 1. Male peripubertal soccer players were lighter, smaller, trained more hours, and had a lower BMI and subtotal lean mass than male postpubertal players (p < 0.05, Cohen´s d ranged from 0.5 to 1.5). Female peripubertal soccer players presented lower subtotal lean mass than their postpubertal counterparts (p < 0.05, Cohen´s d 1.0). When male and female players within the same pubertal group were compared, differences were only found at the peripubertal stage as males were lighter, had a lower BMI, and had been playing soccer for more years than females (p < 0.05, Cohen´s d ranged from 0.5 to 1.0).
Table 1.
Subject characteristics of peripubertal and postpubertal male and female soccer players
| Peripubertal (Tanner II and III) | Postpubertal (Tanner IV and V) | |||
|---|---|---|---|---|
| Males (n = 53) | Females (n = 25) | Males (n = 22) | Females (n = 10) | |
| Age (year) | 12.66 (0.68) | 12.67 (0.58) | 12.87 (0.57) | 12.90 (0.61) |
| Body mass (kg) | 42.74 (7.79)*† | 47.63 (7.49) | 53.59 (11.06) | 53.70 (9.11) |
| Body height (cm) | 151.59 (7.61)† | 154.32 (6.45) | 161.31 (7.01) | 158.79 (7.40) |
| BMI (kg·m-2) | 18.53 (2.69)*† | 19.98 (2.75) | 20.49 (3.45) | 21.16 (2.11) |
| Training experience | 5.32 (2.23)* | 2.72 (2.30) | 4.82 (1.79) | 3.45 (3.08) |
| Training duration (h/week) | 4.17 (1.59)† | 3.58 (1.66) | 3.50 (1.06) | 3.05 (0.69) |
| Subtotal lean mass (kg) | 29.30 (4.81)† | 30.59 (4.01)† | 37.55 (6.09) | 35.41 (5.81) |
| Tanner status‡ | (18/35) | (12/13) | (18/4) | (8/2) |
Data are means (standard deviation). ‡ For peripubertal number of participants in Tanner 2 and 3, for postpubertal number of participants in Tanner 4 and 5; BMI: body mass index * p < 0.05 between genders; † p < 0.05 between pubertal status
Adjusted differences between genders
Comparisons of BMC and BMD for male and female soccer players without dividing by pubertal status are presented in Figure 1. Females demonstrated higher subtotal body and lumbar spine BMC and higher subtotal body, mean leg, lumbar spine, and femoral neck BMD than males (p < 0.05; ranged from 0.04 to 0.26; Figure 1).
Figure 1.
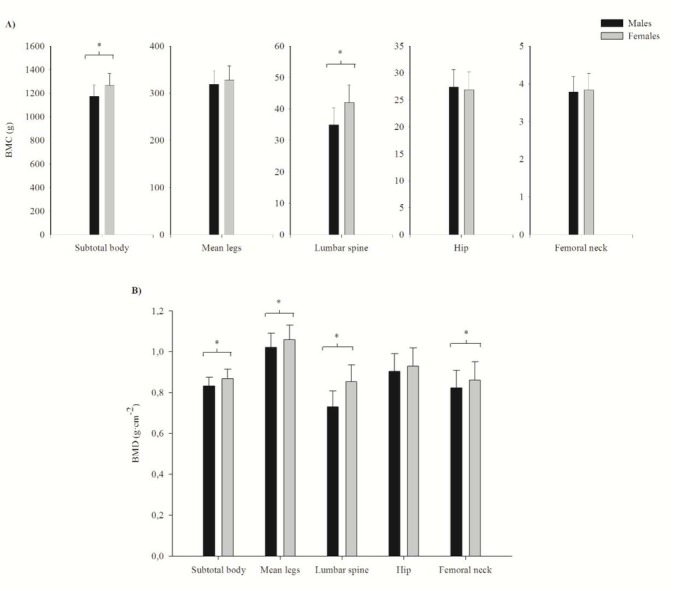
Adjusted bone mass values by DXA in adolescent soccer players without stratifying by pubertal status. (A) Bone mineral content (BMC) and (B) bone mineral density (BMD) differences between genders without taking into account the pubertal status. Data adjusted by subtotal lean mass and training experience. * p < 0.05 between genders.
Unadjusted bone mass differences between genders by pubertal groups
Higher lumbar spine BMC and BMD were found in female peripubertal and postpubertal players compared to their male counterparts (p < 0.05; Cohen´s d ranged from 0.88 to 1.65; Table 2). Female peripubertal participants also presented significantly higher subtotal body BMC and subtotal body, mean leg and femoral neck BMD values compared to their male counterparts (p < 0.05; Cohen´s d ranged from 0.46 to 0.70; Table 2).
Table 2.
Unadjusted BMC and BMD at different regions in peripubertal and postpubertal male and female soccer players.
| Peripubertal (Tanner II and III) | Postpubertal (Tanner IV and V) | ||||
|---|---|---|---|---|---|
| Males (n = 53) | Females (n = 25) | Males (n = 22) | Females (n = 10) | ||
| 1422.628 | |||||
| Subtotal body | 1091.847 (190.016)*† | 1214.832 (222.324)* | 1354.562 (257.965) | (288.962) | |
| BMC | Mean legs | 296.645 (53.691)* | 318.851 (57.287) | 370.917 (71.498) | 357.023 (70.785) |
| (g) | Lumbar spine | 32.444 (5.739)*† | 39.076 (8.938)* | 40.724 (7.822)† | 49.962 (8.855) |
| Hip | 25.860 (4.368)* | 25.874 (4.600) | 31.239 (6.226) | 29.104 (5.478) | |
| Femoral neck | 3.676 (0.470)* | 3.746 (0.658) | 4.052 (0.645) | 4.030 (0.668) | |
| Subtotal body | 0.813 (0.069)*† | 0.856 (0.068) | 0.881 (0.072) | 0.899 (0.075) | |
| BMD | Mean legs | 0.989 (0.097)*† | 1.056 (0.096) | 1.094 (0.109) | 1.077 (0.102) |
| Lumbar spine | 0.707 (0.076)*† | 0.818 (0.112)* | 0.781 (0.093)† | 0.947 (0.108) | |
| (g·cm-2) | Hip | 0.888 (0.091)* | 0.921 (0.113) | 0.939 (0.111) | 0.950 (0.111) |
| Femoral neck | 0.814 (0.088)† | 0.862 (0.120) | 0.844 (0.090) | 0.856 (0.113) | |
Data are means (standard deviation). BMC: bone mineral content; BMD: bone mineral density * p < 0.05 between pubertal status; † p < 0.05 between genders
Unadjusted bone mass differences between pubertal groups by gender
In females, postpubertal players showed higher subtotal body and lumbar spine BMC and lumbar spine BMD values when compared to peripubertal players (p < 0.05; Cohen´s d ranged from 0.81 to 1.22; Table 2). On the other hand, male postpubertal players showed higher BMC and BMD values at all sites except for femoral neck BMD when compared to peripubertal soccer players (p < 0.05; Cohen´s d ranged from 0.51 to 1.21; Table 2).
Adjusted bone mass differences between genders by pubertal groups
Female peripubertal and postpubertal soccer players had significantly higher BMC and BMD values at the subtotal body and lumbar spine than their male counterparts (p < 0.05; ranged from 0.09 to 0.60; Table 3). Moreover, female peripubertal players showed higher mean leg BMD compared to males (p < 0.05; 0.09; Table 3).
Table 3.
Adjusted BMC and BMD at different regions in peripubertal and postpubertal male and female soccer players.
| Peripubertal (Tanner II and III) | Postpubertal (Tanner IV and V) | ||||
|---|---|---|---|---|---|
| Males (n = 53) | Females (n = 25) | Males (n = 22) | Females (n = 10) | ||
| Subtotal body | 1181.782 (92.945)† | 1280.420 (106.065) | 1137.898 (102.415)† | 1258.660 (111.698) | |
| BMC | Mean legs | 321.126 (30.052) | 335.482 (28.420) | 311.939 (33.114) | 315.445 (29.928) |
| (g) | Lumbar spine | 34.712 (4.310)† | 40.855 (6.955) | 35.259 (4.751)† | 45.514 (7.324) |
| Hip | 27.507 (3.640) | 27.161 (2.655) | 27.272 (4.010) | 25.887 (2.795) | |
| Femoral neck | 3.844 (0.415) | 3.926 (0.365)* | 3.648 (0.460) | 3.581 (0.383) | |
| Subtotal body | 0.838 (0.044)† | 0.873 (0.045) | 0.820 (0.052)† | 0.857 (0.047) | |
| BMD | Mean legs | 1.025 (0.073)† | 1.077 (0.075) | 1.005 (0.075) | 1.026 (0.079) |
| (g·cm-2) | Lumbar spine | 0.730 (0.073)† | 0.836 (0.095) | 0.727 (0.080)† | 0.902 (0.101) |
| Hip | 0.912 (0.087) | 0.946 (0.080) | 0.880 (0.098) | 0.888 (0.085) | |
| Femoral neck | 0.837 (0.080)* | 0.888 (0.085)* | 0.789 (0.089) | 0.790 (0.092) | |
Data are means (standard deviation). BMC: bone mineral content; BMD: bone mineral density. Data adjusted by subtotal lean mass and the number of years training soccer. * p < 0.05 between genders pubertal status; † p < 0.05 between genders.
Adjusted bone mass differences between pubertal groups by gender
Adjusted BMC and BMD at the femoral neck were higher in peripubertal than postpubertal female soccer players (p < 0.05, were 0.15 and 0.20; Table 3). In males, peripubertal players demonstrated higher femoral neck BMD than postpubertal male players (p < 0.05, 0.057).
Discussion
The main findings of the present study were that subtotal body and lumbar spine BMC and BMD were significantly higher in female than in male adolescent soccer players, even considering the pubertal status of the participants. When bone comparisons between groups were not adjusted, both male and female postpubertal players showed greater BMC and BMD at several sites than their peripubertal counterparts. After adjusting by subtotal body lean mass and training experience, these BMC and BMD differences between pubertal groups disappeared and, in fact, both peripubertal male and female players showed higher femoral neck BMD than their postpubertal peers. Femoral neck BMC was also higher in peripubertal females than in postpubertal females after adjusting by the same covariates.
Previous studies in female (Ferry et al., 2011, 2013; Plaza-Carmona et al., 2013; Soderman et al., 2000) and male soccer players (Nebigh et al., 2009; Silva et al., 2011; Vicente-Rodriguez et al., 2003, 2004; Zouch et al., 2015) observed higher BMC and BMD values at most weight-bearing sites when compared to other athletes or controls; however, these differences were more significant in females. Although these studies showed the positive influence of playing soccer in both genders up to now, the only study that directly compared bone mass between male and female players reported no BMC and BMD differences between genders (McCulloch et al., 1992). In contrast, the current study established that females presented higher bone mass values at most weight-bearing sites when compared to males, even though peripubertal females had been playing soccer for fewer years than their male counterparts. Nevertheless, McCulloch et al. (1992) included participants who were 15.3 years old and in the present study, the mean age of participants was 12.7 years. It has been demonstrated that females accumulate BMC earlier than males: 26% of adult BMC is accumulated around the age of 12 in females (Theintz et al., 1992) and 14 in males (Bailey et al., 1999). Thus, these differences between studies could be justified by the fact that our males were younger and might not have attained their age of peak bone mass accumulation yet.
To our knowledge, the only study that has compared bone mass between different pubertal status in male soccer players was performed by Zouch et al. (2014). They reported that soccer had a higher influence on bone mass in male pubertal than prepubertal players. Moreover, Nebigh et al. (2009) reinforced these results and suggested that these improvements in bone mass at weight-bearing sites were more marked during puberty than prepuberty in male players. On the other hand, in females, Soderman et al. (2000), Ubago-Guisado et al. (2015) and Plaza-Carmona et al. (2016) divided soccer players into pubertal groups and compared them separately with other athletes and controls of the same pubertal status. These authors reported that bone mass differences between female soccer players, other athletes, and controls were higher and more evident in athletes with higher pubertal status. The findings of the present study before adjustment, also reported higher BMC and BMD at most weight-bearing sites in postpubertal than peripubertal male and female soccer players (Table 2). However, when the data of the current study was adjusted by subtotal lean mass and training experience, these differences were in fact inverted, with higher femoral neck BMC and BMD appearing in peripubertal players than their postpubertal peers (Table 3). This suggests that peripubertal soccer players had strong bones in relation to their age and muscles. Bones are influenced by muscle contractions (Frost, 2003) therefore, adequate muscle tissue in the peripubertal stage could be an important factor to attain high BMC and BMD in these athletes. Yet, these differences between the peripubertal and the postpubertal stage might be influenced by the fact that peripubertal soccer players trained more hours per week than postpubertal ones.
Some limitations of this study should be recognised. First of all, the present study did not have a control group; therefore, further research evaluating the influence of gender and pubertal status between soccer players and controls could provide more information to better understand the effects of this sport during growth. Secondly, after calculating the sample size, 52 soccer players (26 males and 26 females) were needed to obtain a power of 95%. However, when the sample of 110 players was divided into four groups by gender and pubertal development, the number of subjects in some groups was lower than 26 participants, with the female postpubertal group presenting the lowest sample (n = 10). Therefore, the present findings of postpubertal females should be cautiously interpreted. Finally, the cross-sectional design of the current study (instead of longitudinal) does not allow one to obtain strong conclusions and to study bone development.
Conclusions
The current study provides evidence that female soccer players presented higher BMC and BMD at most of the weight-bearing sites than their male peers, being lumbar spine the site with the largest gender differences. Additionally, both male and female postpubertal players showed higher BMC and BMD than peripubertal players. Nonetheless, these results were inverted after adjusting by subtotal body lean mass and training experience which suggests that playing soccer during peripuberty may be one of the tools to reduce future osteoporotic problems in adulthood.
Acknowledgements
The authors would like to thank all the children, their parents, and soccer clubs (Real Zaragoza S.A.D.; Los Molinos U.D.; C.D. Marianistas; C.D. Transportes Alcaine and S.D. Ejea) that participated in the study for their understanding and dedication to the project.
This work was supported by the Spanish ‘Ministerio de Economía y Competitividad’ (Project DEP 2012-32724)’. GLB received a Grant FPU 2013 (FPU13/02111) from the ‘Ministerio de Educación, Cultura y Deporte’.
References
- Bailey DA, McKay HA, Mirwald RL, Crocker PR, Faulkner RA. A six-year longitudinal study of the relationship of physical activity to bone mineral accrual in growing children: the university of Saskatchewan bone mineral accrual study. J Bone Miner Res. 1999;59:1672. doi: 10.1359/jbmr.1999.14.10.1672. –. [DOI] [PubMed] [Google Scholar]
- Bangsbo J. The physiology of soccer with special reference to intense intermittent exercise. Acta Physiol Scand Suppl. 1994;619:1. –. [PubMed] [Google Scholar]
- Calbet JA, Dorado C, Diaz-Herrera P, Rodriguez-Rodriguez LP. High femoral bone mineral content and density in male football (soccer) players. Med Sci Sports Exerc. 2001;33:1682. doi: 10.1097/00005768-200110000-00011. –. [DOI] [PubMed] [Google Scholar]
- Cousins JM, Petit MA, Paudel ML, Taylor BC, Hughes JM, Cauley JA, Zmuda JM, Cawthon PM, Ensrud KE. Osteoporotic Fractures in Men Study Group. Muscle power and physical activity are associated with bone strength in older men: The osteoporotic fractures in men study. Bone. 2010;47:205. doi: 10.1016/j.bone.2010.05.003. –. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duke PM, Litt IF, Gross RT. Adolescents' self-assessment of sexual maturation. Pediatrics. 1980;66:918. –. [PubMed] [Google Scholar]
- Ferry B, Duclos M, Burt L, Therre P, Le Gall F, Jaffre C, Courteix D. Bone geometry and strength adaptations to physical constraints inherent in different sports: comparison between elite female soccer players and swimmers. J Bone Miner Metab. 2011;29:342. doi: 10.1007/s00774-010-0226-8. –. [DOI] [PubMed] [Google Scholar]
- Ferry B, Lespessailles E, Rochcongar P, Duclos M, Courteix D. Bone health during late adolescence: effects of an 8-month training program on bone geometry in female athletes. Joint Bone Spine. 2013;80:57. doi: 10.1016/j.jbspin.2012.01.006. –. [DOI] [PubMed] [Google Scholar]
- Frost HM. Bone's mechanostat: a 2003 update. Anat Rec A Discov Mol Cell Evol Biol. 2003;275:1081. doi: 10.1002/ar.a.10119. –. [DOI] [PubMed] [Google Scholar]
- Gracia-Marco L, Ortega FB, Jimenez-Pavon D, Rodríguez G, Castillo MJ, Vicente-Rodríguez G, Moreno LA. Adiposity and bone health in Spanish adolescents. The HELENA study. Osteoporos Int. 2012;23:937. doi: 10.1007/s00198-011-1649-3. –. [DOI] [PubMed] [Google Scholar]
- Lozano-Berges G, Matute-Llorente A, González-Agüero A, Gómez-Bruton A, Gómez-Cabello A, Vicente-Rodríguez G, Casajús JA. Soccer helps build strong bones during growth: a systematic review and meta-analysis. Eur J Pediatr. 2018;177:295. doi: 10.1007/s00431-017-3060-3. –. [DOI] [PubMed] [Google Scholar]
- McCulloch RG, Bailey DA, Whalen RL, Houston CS, Faulkner RA, Craven BR. Bone Density and Bone Mineral Content of Adolescent Soccer Athletes and Competitive Swimmers. Pediatr Exerc Sci. 1992;4:319. –. [Google Scholar]
- Nebigh A, Rebai H, Elloumi M, Bahlous A, Zouch M, Zaouali M, Alexandre C, Sellami S, Tabka Z. Bone mineral density of young boy soccer players at different pubertal stages: relationships with hormonal concentration. Joint Bone Spine. 2009;76:63. doi: 10.1016/j.jbspin.2008.03.002. –. [DOI] [PubMed] [Google Scholar]
- National Osteoporosis Foundation. What is Osteoporosis and What Causes it? https://www.nof.org/patients/what-is-osteoporosis/; Available at. accessed on 12.11.2017.
- Plaza-Carmona M, Ubago-Guisado E, Sánchez-Sánchez J, Felipe JL, Fernández-Luna A, García-Unanue J, Burillo P, Gallardo L. Body composition and physical fitness in prepubertal girls swimmers and soccer players. JSHR. 2013;5:251. –. [Google Scholar]
- Plaza-Carmona M, Vicente-Rodriguez G, Gomez-Cabello A, Martin-Garcia M, Sanchez-Sanchez J, Gallardo L, Ara I. Higher bone mass in prepubertal and peripubertal female footballers. Eur J Sport Sci. 2016;16:877. doi: 10.1080/17461391.2016.1144794. –. [DOI] [PubMed] [Google Scholar]
- Rizzoli R, Bianchi ML, Garabedian M, McKay HA, Moreno LA. Maximizing bone mineral mass gain during growth for the prevention of fractures in the adolescents and the elderly. Bone. 2010;46:294. doi: 10.1016/j.bone.2009.10.005. –. [DOI] [PubMed] [Google Scholar]
- Silva CC, Goldberg TB, Teixeira AS, Dalmas JC. The impact of different types of physical activity on total and regional bone mineral density in young Brazilian athletes. J Sports Sci. 2011;29:227. doi: 10.1080/02640414.2010.529456. –. [DOI] [PubMed] [Google Scholar]
- Soderman K, Bergstrom E, Lorentzon R, Alfredson H. Bone mass and muscle strength in young female soccer players. Calcif Tissue Int. 2000;67:297. doi: 10.1007/s002230001149. –. [DOI] [PubMed] [Google Scholar]
- Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child. 1976;51:170. doi: 10.1136/adc.51.3.170. –. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tenforde AS, Fredericson M. Influence of sports participation on bone health in the young athlete: a review of the literature. Pm R. 2011;3:861. doi: 10.1016/j.pmrj.2011.05.019. –. [DOI] [PubMed] [Google Scholar]
- Theintz G, Buchs B, Rizzoli R, Slosman D, Clavien H, Sizonenko PC, Bonjour JP. Longitudinal monitoring of bone mass accumulation in healthy adolescents: evidence for a marked reduction after 16 years of age at the levels of lumbar spine and femoral neck in female subjects. J Clin Endocrinol Metab. 1992;75:1060. doi: 10.1210/jcem.75.4.1400871. –. [DOI] [PubMed] [Google Scholar]
- Ubago-Guisado E, Gomez-Cabello A, Sanchez-Sanchez J, Garcia-Unanue J, Gallardo L. Influence of different sports on bone mass in growing girls. J Sports Sci. 2015;33:1710. doi: 10.1080/02640414.2015.1004639. –. [DOI] [PubMed] [Google Scholar]
- Vicente-Rodriguez G, Ara I, Perez-Gomez J, Serrano-Sanchez JA, Dorado C, Calbet JA. High femoral bone mineral density accretion in prepubertal soccer players. Med Sci Sports Exerc. 2004;36:1789. doi: 10.1249/01.mss.0000142311.75866.d7. –. [DOI] [PubMed] [Google Scholar]
- Vicente-Rodriguez G, Jimenez-Ramirez J, Ara I, Serrano-Sanchez JA, Dorado C, Calbet JA. Enhanced bone mass and physical fitness in prepubescent footballers. Bone. 2003;33:853. doi: 10.1016/j.bone.2003.08.003. –. [DOI] [PubMed] [Google Scholar]
- Vicente-Rodriguez G, Urzanqui A, Mesana MI, Ortega FB, Ruiz JR, Ezquerra J, Casajus JA, Blay G, Blay VA, Gonzalez-Gross M, Moreno LA. AVENA Zaragoza Study Group. Physical fitness effect on bone mass is mediated by the independent association between lean mass and bone mass through adolescence: a cross-sectional study. J Bone Miner Metab. 2008;26:288. doi: 10.1007/s00774-007-0818-0. –. [DOI] [PubMed] [Google Scholar]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. Strobe Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4:e296. doi: 10.1371/journal.pmed.0040296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace LS, Ballard JE. Lifetime physical activity and calcium intake related to bone density in young women. J Womens Health Gend Based Med. 2002;11:389. doi: 10.1089/152460902317586029. –. [DOI] [PubMed] [Google Scholar]
- World Health Organization. WHO Scientific group on the asssessment of osteoporosis at primary health care level. Summary Metting Report. 2004. http://www.who.int/chp/topics/Osteoporosis.pdf; Available at. accessed on 10.11.2017.
- Zouch M, Jaffre C, Thomas T, Frere D, Courteix D, Vico L, Alexandre C. Long-term soccer practice increases bone mineral content gain in prepubescent boys. Joint Bone Spine. 2008;75:41. doi: 10.1016/j.jbspin.2006.12.008. –. [DOI] [PubMed] [Google Scholar]
- Zouch M, Vico L, Frere D, Tabka Z, Alexandre C. Young male soccer players exhibit additional bone mineral acquisition during the peripubertal period: 1-year longitudinal study. Eur J Pediatr. 2014;173:53. doi: 10.1007/s00431-013-2115-3. –. [DOI] [PubMed] [Google Scholar]
- Zouch M, Zribi A, Alexandre C, Chaari H, Frere D, Tabka Z, Vico L. Soccer increases bone mass in prepubescent boys during growth: a 3-yr longitudinal study. J Clin Densitom. 2015;18:179. doi: 10.1016/j.jocd.2014.10.004. –. [DOI] [PubMed] [Google Scholar]