

Abstract
We report a nine-month-old Caucasian male with features seen in oculoauriculovertebral spectrum (OAVS) and frontonasal dysplasia sequence (FND) born to normal, non-consanguineous parents and review the literature. His malformations included a left pre-auricular skin tag, severely hypoplastic right pinna without an external canal, severely everted and hypoplastic left upper eyelid, bilateral cleft lip and palate, bifid broad nasal tip, ocular hypertelorism, micrognathia, hypoplastic mandible, an extra cervical rib on the left, hemivertebrae at T3–4, agenesis of the posterior corpus callosum with a midline lipoma, and an extra renal pelvis. This constellation of anomalies is consistent with the diagnosis of oculoauriculofrontonasal syndrome (OAFNS) which appears to be a distinct condition from either OAVS or FND but with overlapping features.
Keywords: frontonasal dysplasia sequence(FND), oculoauriculovertebral spectrum (OAVS), oculoauriculofrontonasal spectrum(OAFNS)
INTRODUCTION
Oculoauriculofrontonasal syndrome (OAFNS) is a rare disorder with features of both frontonasal dysplasia sequence (FND) and oculoauriculovertebral spectrum (OAVS). The term oculoauriculofrontonasal syndrome (OAFNS) was first coined by Carey and Yong in 1981. The constellation of findings seen in OAFNS was first reported by Gupta et al. in 1968. The spectrum was reviewed in 14 cases, including a report of a new patient, by Guion-Almeida and Lopes in 1997. Nine additional subjects have been reported [Cohen et al., 1971; Carey and Yong, 1981; Tenconi and Hall, 1983; Casey et al., 1996] with a combined total of 23 subjects in the literature. The etiology is unknown with one documented recurrence in a family (a brother and sister born to a diabetic mother) [Golabi et al., 1983]. Herein, we report a nine-month-old Caucasian male with features consistent with OAFNS, review the features typically associated with this rare disorder, and lend support that OAFNS is a separate entity from either FND or OAVS.
CLINICAL REPORT
Our subject was initially seen at nine days of age, due to multiple congenital anomalies. He was delivered by spontaneous vaginal delivery at 38 weeks of gestation to a healthy 39-year-old (G3P3) Caucasian mother. He has two older unaffected sibs. The three generation family history was unremarkable for similarly affected individuals, birth defects, mental retardation, miscarriages, or consanguinity. A chorionic villus sampling (CVS) was performed due to advanced maternal age, and a normal male karyotype (46,XY) was found. The pregnancy history was uncomplicated except for a cleft lip and possible cerebral mass identified by prenatal ultrasound. At birth, the patient was small for gestational age with a weight of 2.31 kg (≤ 3 percentile), a length of 48.5 cm (10 percentile) and a head circumference of 33 cm (3 percentile).
Multiple congenital anomalies noted at birth included bilateral cleft lip and palate, a left pre-auricular skin tag, severely hypoplastic right pinna without an external canal, severely everted and hypoplastic left upper eyelid, notched broad nasal tip, ocular hypertelorism, micrognathia, and a hypoplastic mandible (Fig. 1). A skeletal survey showed the micrognathia and an extra cervical rib on the left and hemivertebrae at T3–4. A head CT showed agenesis of the posterior corpus callosum with a midline lipoma and complex facial anomalies. An abdominal ultrasound revealed an extra renal pelvis on the left. An echocardiogram showed a small patent foramen ovale. An ABR indicated severe conductive hearing loss on the right. Given his anomalies, a high resolution chromosome analysis (550 band level) and FISH probe study for the 22q11 deletion were undertaken. The results were normal. At age nine months, the patient had significant feeding difficulties and a gastrostomy tube was placed. He was below the third percentile for height (64.5 cm), weight (5.38 kg), and head circumference (41.5 cm). His developmental milestones were normal.
Fig. 1.
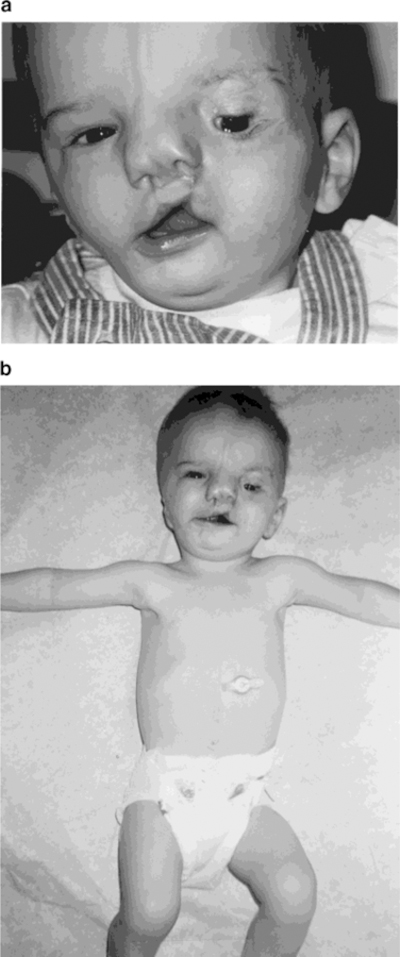
Facial (a) and frontal (b) views of our patient at nine months of age following plastic surgery.
DISCUSSION
The features seen in our patient were consistent with the diagnosis of oculoauriculofrontonasal syndrome (OAFNS) which was initially described in the medical literature by Gupta et al. [1968]. Since that time, several labels have been used for this condition including Golabi-Gonzalez-Edwards (GGE) syndrome [Golabi et al., 1983], ophthalmofrontonasal dysplasia [Day, 1983], and OAFNS [Carey and Yong, 1981]. The earlier cases of OAFNS were in a brother and a sister born to a diabetic mother [Golabi et al., 1983]. The finding of affected siblings led the authors to suggest an autosomal recessive etiology, although there have been no further reported cases of affected siblings to confirm this hypothesis.
The various subjects described, like ours, have clinical findings reported in both the oculoauriculovertebral spectrum and frontonasal dysplasia sequence (Table I). Our subject demonstrates 15 of 16 major features seen in OAFNS. Eight of these 16 features are seen in the frontonasal dysplasia sequence, while 11 of the 16 features reported in oculoauriculovertebral spectrum were observed. Four of the 16 features overlap including cleft lip/cleft palate, accessory preauricular tags/pits, middle/inner ear anomaly with variable deafness, and agenesis of the corpus callosum.
TABLE I.
Physical Features Seen in Our Subject Consistent With Frontonasal Dysplasia Sequence, and Oculoauriculovertebral Spectrum
| Features/anomalies | Frontonasal dysplasia sequence | Oculoauriculovertebral spectrum | Our subject |
|---|---|---|---|
| Hypoplasia of malar, maxillary, and/or mandibular region | − | + | + |
| Hypoplasia of facial musculature | − | + | + |
| Upper eyelid coloboma | − | + | + |
| Epibulbar dermoids | − | + | − |
| Microtia | − | + | + |
| Hemivertebrae/hypoplasia of vertebra | − | + | + |
| Renal anomalies | − | + | + |
| Prenatal growth deficiency | − | + | + |
| Cleft lip/cleft palate | + | + | + |
| Notched broad nasal tip | + | − | + |
| Ocular hypertelorism | + | − | + |
| Low set ears | + | − | + |
| Accessory preauricular tags and/or pits | + | + | + |
| Middle/inner ear anomaly with variable deafness | + | + | + |
| Agenesis of corpus callosum | + | + | + |
| Lipoma in midbrain | + | − | + |
Frontonasal dysplasia sequence (FND) is a developmental field defect representing abnormal morphogenesis of the frontonasal eminence [Casey et al., 1996]. The pathogenesis is heterogeneous. It can be isolated, associated with other anomalies (tumor, encephalocele), or be part of a syndrome [Sedano and Gorlin, 1988].
Oculoauriculovertebral spectrum (OAVS) is a general title, which encompasses Goldenhar syndrome and hemifacial microsomia. This spectrum is a nonrandom association of anomalies in morphogenesis of the first and second branchial arches with occasional vertebral problems and ocular abnormalities [Gorlin et al., 1963; Tenconi and Hall, 1983; Cohen et al., 1989; Jones, 1997].
Our patient represents a new occurrence of OAFNS. His anomalies are consistent with the previously described clinical features in subjects reported with this disorder and summarized in Table II. Phenotypically, our patient has characteristics of both FND and OAVS as do other patients reported with OAFNS (Table I). These two disorders are classified as separate entities. FND is characterized by median facial abnormalities including ocular hypertelorism, widow’s peak, bifid nose, median cleft lip, and broad nasal root [Sedano and Gorlin, 1988; Jones, 1997]. Our subject has cleft lip and palate, a bifid nose, and ocular hypertelorism. Abnormalities described in OAVS include hypoplastic maxilla, hypoplastic mandible, microtia, preauricular skin tags, epibulbar dermoids, and vertebral defects [Tenconi and Hall, 1983; Rollnick et al., 1987; Cohen et al., 1989; Jones, 1997]. Our subject has preauricular skin tags, hypoplasia of maxillary and mandibular regions, microtia, and vertebral anomalies. He does not have epibulbar dermoids.
TABLE II.
Comparison of Clinical Findings in Our Subject and Reported Subjects With Oculoauriculofrontonasal Syndrome
| Sex | Microtia/ear tags | Notched nasal tip/bifid nose | Epibulbar dermoids | Cleft lip/cleft palate | Mandibular hypoplasia | Facial asymmetry | Midbrain lipoma | Encephalocele | Vertebral defects | |
|---|---|---|---|---|---|---|---|---|---|---|
| Our subject | M | + | + | − | + | + | + | + | − | + |
| Gupta et al. [1968] | M | + | + | + | − | − | − | − | + | − |
| Fleischer-Peters [1969] | F | + | + | + | + | + | + | ? | − | − |
| Cohen et al. [1971] | M | + | + | − | ? | ? | − | ? | − | − |
| Tarateta et al. [1978] | F | + | − | + | + | + | − | − | + | ? |
| Carey and Yong [1981] | M | + | + | + | ? | ? | − | ? | − | − |
| M | + | + | + | − | + | + | − | − | − | |
| Castillo et al. [1983] | F | + | + | + | + | − | − | ? | − | ? |
| Fontaine et al. [1983] | F | + | + | + | − | + | + | ? | + | − |
| Golabi et al. [1983] | M | + | − | + | − | + | + | + | − | + |
| F | + | − | + | − | − | − | ? | − | − | |
| Tenconi and Hall [1983] | ? | + | + | + | ? | ? | − | − | + | − |
| ? | + | + | − | ? | ? | − | − | − | − | |
| ? | + | + | − | ? | ? | − | − | − | − | |
| Musarella and Young [1986] | F | + | + | + | − | + | + | + | − | − |
| Naidich et al. [1988] | F | + | + | + | + | − | − | ? | − | ? |
| M | + | + | + | + | − | − | + | − | ? | |
| Toriello et al. [1995] | M | + | + | + | + | − | − | − | − | ? |
| Guion-Almeida et al. [1996] | M | + | − | − | − | − | − | − | + | ? |
| F | + | − | − | + | + | + | − | + | ? | |
| Casey et al. [1996] | M | + | + | + | + | − | + | − | − | − |
| M | + | + | + | + | + | + | − | − | − | |
| F | + | + | + | + | − | + | − | − | − | |
| Guion-Almeida and Lopes [1997] | M | + | + | − | + | + | + | + | − | − |
| Total (percentage) | 12 M:9F | 24/24 (100%) | 19/24 (79%) | 17/24 (71%) | 12/19 (63%) | 10/19 (53%) | 11/24 (46%) | 5/17 (29%) | 6/24 (25%) | 2/17 (12%) |
OAFNS demonstrates variability in the overlap of features seen in FND and OAVS. Sixty-three percent of the reported OAFNS subjects had cleft lip and/or palate while 46% had facial asymmetry. Although many of the OAFNS characteristics are variable, all reported cases had microtia/ear tags. Therefore, microtia/ear tags can be considered a cardinal feature of this disorder. Notched nasal tip/bifid nose was seen in 79 percent of reported subjects. The other features seen in the reported OAFNS subjects in descending frequency were epibulbar dermoids (71%), cleft lip/cleft palate (63%), mandibular hypoplasia (53%), facial asymmetry (46%), midbrain lipoma (29%), encephalocele (25%), and vertebral defects (12%) (See Table II). An interesting variation of OAFNS, is the presence of vertebral defects seen in only two reported subjects but commonly seen in OAVS and less often in FND.
Our patient has findings seen in OAVS and others associated with FND. It has been suggested that OAFNS is a variation of either OAVS or FND. However, it appears that FND and OAVS are heterogeneous with different etiologies.
In summary, we conclude that OAFNS is the most appropriate diagnosis for our patient and that OAFNS is a distinct entity representing a discrete subset of patients. OAFNS as a distinct and separate condition from OAVS or FND is further supported by the reports of Casey et al. [1996] and Toriello et al. [1995]. Additional reports are needed, including molecular genetic studies, to identify a possible genetic cause of this rare condition to further distinguish it from OAVS and FND.
ACKNOWLEDGMENT
We thank Aliza Elrod for expert preparation of the manuscript.
REFERENCES
- Carey JC, Yong SL. 1981. Frontonasal dysplasia and the Goldenhar syndrome: the oculo-auriculo-frontonasal syndrome. 1981 conference on malformations and morphogenesis (March of Dimes), Dartmouth College, Hanover, New Hampshire. [Google Scholar]
- Casey HD, Braddock SR, Haskins RC, Carey JC, Morales L. 1996. Frontonasal malformation and the oculoauriculovertebral spectrum: the oculoauriculofrontonasal syndrome. Cleft Palate J 33:519–523. [DOI] [PubMed] [Google Scholar]
- Castillo S, Youlton R, Rojas J, Rivera L. 1983. Sindrome de fisura media del rostro. Rev Chil Ped 54:417–421. [PubMed] [Google Scholar]
- Cohen MM Jr, Sedano HO, Gorlin RJ, Jirasck JE. 1971. Frontonasal dysplasia (median cleft face syndrome): comments on etiology and pathogenesis. Birth Defects Orig Artic Ser 7(7):117–119. [PubMed] [Google Scholar]
- Cohen MM Jr, Rollnick BR, Kaye CI. 1989. Oculoauriculovertebral spectrum: an updated critique. Cleft Palate J 26:276–286. [PubMed] [Google Scholar]
- Day D 1983. Unique subpopulations in the diagnostic category of frontonasal dysplasia. Birth Defects Orig Artic Ser 19(5):182–183. [Google Scholar]
- Fleischer-Peters VA. 1969. Das Goldenhar syndrom und kiefemissbildungen. Dtsch Zahnarzlt Z 24:545–551. [PubMed] [Google Scholar]
- Fontaine G, Walbaum R, Poupard B, Bonte C, Ytheier H, Stevenard C. 1983. La dysplasie fronto-nasale (A propos de quatre observations). J Genet Hum 31:351–365. [PubMed] [Google Scholar]
- Golabi M, Gonzalez MC, Edwards MS. 1983. A new syndrome of oculoauriculovertebral dysplasia and midline craniofacial defect: the oculoauriculofrontonasal dysplasia. Two new cases in sibs. Birth Defects Orig Artic Ser 19:183–184.6228267 [Google Scholar]
- Gorlin RJ, Jue KL, Jacobsen U, Goldschmide B. 1963. Oculoauriculovertebral syndrome. J Pediatr 63:991–999. [DOI] [PubMed] [Google Scholar]
- Guion-Almeida ML, Lopes VL. 1997. Oculoauriculofrontonasal spectrum in an adult Brazilian male. Clin Dysmorph 6:251–255. [DOI] [PubMed] [Google Scholar]
- Guion-Almeida ML, Richieri-Costa A, Saavedra D, Cohen MM Jr. 1996. Frontonasal dysplasia: analysis of 21 cases and literature review. Int J Oral Maxillofac Surg 25:91–97. [DOI] [PubMed] [Google Scholar]
- Gupta JS, Gupta SD, Prashar SK. 1968. Oculo-auricular-cranial dysplasia. Br J Ophthalmol 52:346–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones KL. 1997. Smith’s recognizable patterns of human malformation Philadelphia: W.B. Saunders; p 642–645, 240–241. [Google Scholar]
- Musarella MA, Young ID. 1986. A patient with median cleft face anomaly and bilateral Goldenhar anomaly. Am J Med Genet 2:135–141. [DOI] [PubMed] [Google Scholar]
- Naidich TP, Osborn RE, Bauer B, Naidich MJ. 1988. Median cleft face syndrome: MR and CT data from 11 children. J Comp Assist Tomogr 12:57–64. [PubMed] [Google Scholar]
- Rollnick BR, Kaye CI, Nagatoshi K, Hauck W, Martin AO. 1987. Oculoauriculovertebral dysplasia and variants: phenotypic characteristics of 294 patients. Am J Med Genet 26:361–375. [DOI] [PubMed] [Google Scholar]
- Sedano HO, Gorlin RJ. 1988. Frontonasal malformation as a field defect and in syndromic associations. Oral Surg Oral Med Oral Pathol 65:704–710. [DOI] [PubMed] [Google Scholar]
- Tarateta A, Reboa E, Buffoni L. 1978. Median cleft face syndrome. Minerva Pediatr 30:53–60. [PubMed] [Google Scholar]
- Tenconi R, Hall BD. 1983. Hemifacial microsomia: phenotypic classification, clinical implications, and genetic aspects in treatment of hemifacial microsomia. In: Harvold EP, Vargervik K, Chierici G, editors. Treatment of hemifacial microsomia New York: Alan R Liss, Inc; p 39–49. [Google Scholar]
- Toriello HV, Higgins JV, Mann R. 1995. Oculoauriculofrontonasal syndrome: report of another case and review of differential diagnosis. Clin Dysmorphol 4:338–346. [DOI] [PubMed] [Google Scholar]