

ABSTRACT
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastrointestinal tract. The most common location of GIST is the stomach; however, occurrences of GIST in the esophagus are also possible albeit rare. Although the current standard of care for gastric and intestinal GIST involves surgery and tyrosine kinase inhibitors, this case report focuses on the potential of treating esophageal GIST through a novel means of cryoablation therapy.
INTRODUCTION
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastrointestinal tract and may be asymptomatic until advanced stages. The standard of care for more common locations of GIST, such as the stomach and intestine, includes surgical resection and tyrosine kinase inhibitor therapy. However, esophageal GISTs are extremely rare and make up fewer than 5% of all GISTs.1 Because of such rarity, there is a lack of clear recommendations regarding optimal management.2 Because of the complicated blood supply found in the esophagus, surgical options are limited to esophagectomy or the relatively less invasive tumor enucleation.3 The debate to decide which surgical method should be performed for esophageal GISTs is still under scrutiny because some authors propose that enucleation of esophageal GISTs should be considered for smaller tumors (2–5 cm in size), whereas esophagectomy is recommended for GISTs above 9 cm in size.4,5 Given the complex esophageal anatomy and uncertainty in current recommendations, developing a noninvasive method to resolve esophageal GISTs would be optimal. Here, we present a case of an esophageal GIST successfully treated with cryoablation therapy.
CASE REPORT
A 69-year-old man with Barrett esophagus and esophageal adenocarcinoma (T1a disease) successfully treated with resection was found to have a 13 × 5 mm esophageal GIST originating from the muscularis propria layer at 37 cm on surveillance endoscopic ultrasound (EUS) and esophagogastroduodenoscopy (EGD) (Figure 1). The patient was deemed a poor surgical candidate because of a complicated postoperative course after esophageal resection as well as his multiple comorbidities, such as diabetes, coronary artery disease, and paroxysmal atrial fibrillation. Instead, endoscopic local treatment with a spray cryotherapy system (TruFreeze; CSA Medical Inc, Lexington, MA) was employed (Figure 2). At the initial treatment, the tumor was treated for 3 freeze-thaw cycles lasting 30 seconds each. On follow-up EGD/EUS, 3 months later, the GIST decreased in size to 10 × 2 mm. Cryotherapy was again performed with three 30-second cycles. The patient had some chest discomfort for 2 weeks after the second treatment session. On the subsequent EGD/EUS, 3 months later, the GIST was no longer visible (Figure 3). There was just a scar where the previous esophageal GIST had existed, and no residual lesion was identified on radial EUS. Biopsy from the scar had no evidence of GIST, dysplasia, or malignancy. We plan to continue endoscopic surveillance.
Figure 1.

(A) Endoscopic view and (B) EUS image of esophageal gastrointestinal tumor before treatment. EUS, endoscopic ultrasound.
Figure 2.
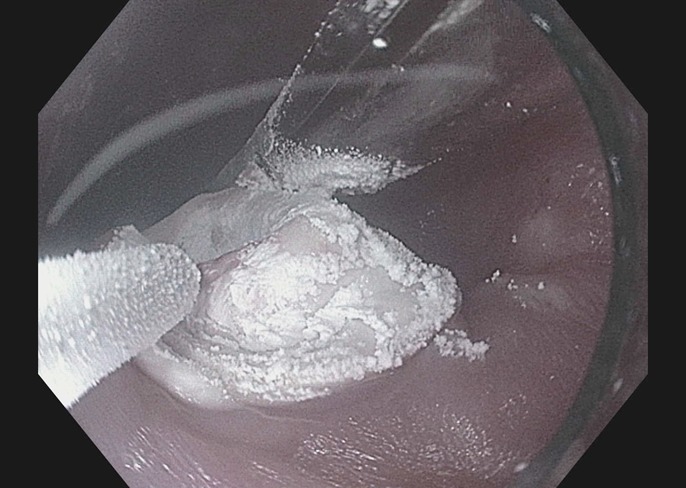
Cryotherapy being applied to esophageal GIST. GIST, gastrointestinal stromal tumor.
Figure 3.

(A) Endoscopic view and (B) EUS image of esophageal gastrointestinal tumor after treatment. EUS, endoscopic ultrasound.
DISCUSSION
Regardless of the size or location, all GISTs have been found to harbor malignant potential.6 It is thus imperative that intervention takes place whenever possible. Esophagectomy is the primary definitive treatment for large esophageal GISTs, although surgery involves significant morbidity.
Our case study demonstrates the potential for cryoablation therapy to resolve esophageal GISTs without invasive surgical intervention. Cryoablation therapy was successful in our patient because there was no longer a visible lesion at the location of the GIST on repeat endoscopy. The procedure was well-tolerated by the patient, and no adverse effects were noted during the procedure or on follow-up. Cryoablation therapy has shown to be effective in achieving local control of Barrett esophagus as well as in treatment of esophageal cancer for both palliation and curative intent.7,8 In fact, in a recent multicenter study, patients with esophageal adenocarcinoma who failed or were not deemed candidates for conventional therapy had endoscopic cryotherapy performed with biopsy-proven local tumor eradication. Pathological examination showed slightly less than 80% of patients with T1a esophageal cancer had complete response to cryoablation.9 Cryotherapy is generally a safe procedure and is associated with low rates of serious adverse events.7,9 More research is needed to better characterize the efficacy and safety profiles of cryoablation therapy with regard to definitive management of esophageal GISTs.
DISCLOSURES
Author contributions: D. Mai wrote and edited the manuscript, and is the article guarantor. A. Yu, DP Lee, and J. Samarasena wrote and edited the manuscript. R. Hashimoto, EJ Torralba, E. Tran, and N. El-Hage Chehade wrote the manuscript.
Financial disclosure: J. Samarasena is a consultant for CSA Medical Inc, Lexington, MA, USA. All other authors have no financial conflicts.
Informed consent was obtained for this case report.
REFERENCES
- 1.Rubin BP, Heinrich MC, Corless CL. Gastrointestinal stromal tumor. Lancet. 2007(9574):1731. [DOI] [PubMed] [Google Scholar]
- 2.Neofytou K, Costa Neves M, Giakoustidis A, Benson C, Mudan S. Effective downsizing of a large oesophageal gastrointestinal stromal tumour with neoadjuvant imatinib enabling an uncomplicated and without tumour rupture laparoscopic-assisted Ivor-Lewis oesophagectomy. Case Rep Oncol Med. 2015;2015:165736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee HJ, Park SI, Kim DK, Kim YH. Surgical resection of esophageal gastrointestinal stromal tumors. Ann Thorac Surg. 2009;87:1569–71. [DOI] [PubMed] [Google Scholar]
- 4.Coccolini F, Catena F, Ansaloni L, Lazzareschi D, Pinna AD. Esophagogastric junction gastrointestinal stromal tumor: Resection vs enucleation. World J Gastroenterol. 2010;16(35):4374–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hihara J, Mukaida H, Hirabayashi N. Gastrointestinal stromal tumor of the esophagus: Current issues of diagnosis, surgery and drug therapy. Transl Gastroenterol Hepatol. 2018;3:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Hum Pathol. 2002;33(5):459–65. [DOI] [PubMed] [Google Scholar]
- 7.Greenwald BD, Dumot JA, Abrams JA, et al. Original article: Endoscopic spray cryotherapy for esophageal cancer: Safety and efficacy. Gastrointest Endosc. 2010;71:686–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kachaamy T, Prakash R, Kundranda M, et al. Liquid nitrogen spray cryotherapy for dysphagia palliation in patients with inoperable esophageal cancer. Gastrointest Endosc. 2018;88(3):447–55. [DOI] [PubMed] [Google Scholar]
- 9.Tsai FC, Ghorbani S, Greenwald BD, et al. Safety and efficacy of endoscopic spray cryotherapy for early stages of esophageal cancer. Dis Esophagus. 2017;30(11):1–7. [DOI] [PubMed] [Google Scholar]