

Abstract
There are nearly 110 million cases of sexually transmitted infections (STI) in the United States. The Centers for Disease Control and Prevention estimates that annually there are more than 19.7 million new STI cases. Of those, more than half are accounted for by youth aged 15 to 24 years. Although some STIs are not considered to be life threatening, they can lead to severe health problems, risk of HIV infection or infertility if they are not properly treated. Some research has shown that parent-youth communication can reduce youth’s at-risk sexual behaviors. The following is a systematic review of the literature on parent-youth sexual communication and family-level interventions designed to reduce risky sexual behavior in youth.
Keywords: Minority health disparities, parent-youth sexual health communication, youth HIV prevention, youth risky sexual behaviors
Introduction
Prevalence of Sexually Transmitted Infections in Youth
Currently, there nearly 110 million cases of sexually transmitted infections (STI) in the United States (Centers for Disease Control and Prevention [CDC], 2014; Satterwhite, Torrone, Meites, Dunne, Mahajan, 2013). Annually, there are more than 19.7 million new STI cases, half of which are accounted for by youth ages 15 to 24 years (Satterwhite et al., 2013). Although some STIs are not considered to be life threatening they can lead to severe health problems or infertility if they are not properly treated (Satterwhite et al., 2013). Chlamydia, gonorrhea and syphilis are three of the most prevalent STIs contracted by youth. Minority females between ages 15 and 24, and minority males between 15 and 24 have higher rates of chlamydia, gonorrhea, and syphilis than their white counterparts (Satterwhite et al., 2013); these youth are also typically unaware of their positive STI status (CDC, 2015). This is significant because these STIs substantially increase the risk of HIV infections (CDC, 2014).
At-Risk Sexual Behaviors
A major factor contributing to African American youth STIs and early parenthood is at-risk sexual behaviors. These include having more than one sexual partner, changing sexual partners frequently, having oral, vaginal or anal sex without a condom, and using unreliable methods of birth control or using birth control inconsistently (CDC, 2012). Young and Vazsonyi (2011) found that more boys than girls reported engaging in at-risk sexual behaviors. In their study of 394 African American adolescents from the rural South, the youth reported having had more than 10 lifetime partners, 10.8% reported having been pregnant or having gotten someone pregnant, and 14.5% reported having received medical treatment for sexually transmitted diseases at least twice (Young & Vazsonyi, 2011). Moreover, the boys in their study engaged in sexual intercourse prior to 14 years of age, and about 25% of them reported having had more than one current sexual partner and using condoms occasionally or never.
Further, in a longitudinal study of at-risk sexual behaviors in public high school students, Fergus, Zimmerman and Caldwell (2007) found that African Americans in the ninth grade engaged in more at-risk sexual behaviors than Caucasians. Similarly, in a biannual study of the health behaviors of youth in public and private schools, the national Youth Risk Behavior Survey (YRBS) found that on average, young Black males than young white males had a higher prevalence for sexual behaviors: having sexual intercourse for the first time before they were 13 years old (13.9% vs. 3.9%); having intercourse with four or more persons during their lifetime (24.8% vs. 13.1%) and; having intercourse with at least one person during the 3 months prior to the conduct of the survey (41.3% vs. 32.4%) (CDC, 2012).
Additionally, among the 33.7% of currently sexually active students nationwide, 12.9% had not used any method to prevent pregnancy during their last sexual intercourse (Office of Adolescent Health [OAH], 2016. Overall, the prevalence of not having used any method to prevent pregnancy was higher among Black female (17.5%) than white female (11.7%) students and higher among Black male (9.9%) than white male (8.3%) students. Moreover, in 2016, the number of births (per 1,000 adolescent females) was higher among Black females than white females (43.9 births vs. 20.5 births) (OAH, 2016).
Given that youth have the highest rate of STI and HIV than any other group in the U.S. (CDC, 2014), there are numerous school-based programs that have been developed specifically for the sexual health educational needs of middle and high school students (DiIorio, McCarty, Resnicow, Lehr, & Denzmore, 2007b; Guilamo-Ramos, Jaccard, Dittus, Bouris, Gonzalez, Casillas, & Banspach, 2011). However, adolescents are still having unprotected sex regardless of abstinence-only and other sex education school-based programs (Bartlett, Holditch-Davis, & Belyea, 2007). Some researchers agree that one definite gap in HIV prevention has been the failure to involve parents in such programs (Byers, Sears, Sears, & Weaver, 2008; DiIorio et al., 2007b; Guilamo-Ramos et al., 2011). Excluding parents means they will not be informed about helpful information that their youth receive in school, thus they cannot reinforce important messages about risk prevention (DiIorio et al., 2007b). Moreover, parents were not adequately supported to talk with their youth about sexual health or protection against at-risk sexual behaviors that lead to STIs, HIV and early parenthood (DiIorio et al., 2007b).
Therefore, specific interventions at the family level can complement community efforts, which include the school and health systems to target youth (CDC, 2012). Though some researchers posit that family-level interventions are more advantageous than school-based because they allow parents to impart their family’s values about nonbiological topics such as sexual decision making (Jaccard, Dodge, & Dittus, 2002). Per Murry, Berkel, Chen, Brody, Gibbons, and Gerrard (2011), family-level interventions that target parenting are a promising strategy for youth, given the critical importance of the family’s role in their development. The researchers noted that this is especially true for African Americans, as their focus on family is emphasized in their traditional values (Murry et al. 2011). The role of family is also paramount with Latinos, as demonstrated in two randomized control trials of Mexican parents and Latino parents and adolescents on sexual health (Villarruel, Cherry, Cabriales, Ronis, & Zhou, 2008; Villarruel, Loveland-Cherry, & Ronis, 2010). These researchers used ecodevelopmental theory as a basis for their studies, which contends that one’s family is at the fundamental level, from which human development is influenced.
Some researchers agree that preadolescence is the most appropriate time for parents to communicate with their youth about preventing at-risk sexual behaviors because most preadolescents have not become sexually active (Guilamo-Ramos et al., 2011; Villarruel et al., 2010; Wyckoff, Miller, Forehand, Bau, Fasula, Long, & Armistead, 2008). This stage of childhood is especially important for prevention, because parents have been shown to have the most influence on adolescents’ decisions regarding sexual intercourse (Miller, Lin, Poulsen, Fasula, Wyckoff, Forehand, Long, & Armistead, 2011).
We selected self-efficacy as the theoretical underpinning for understanding the role of parent-youth communication to promote sexual health in youth. Bandura (1997) defined self-efficacy as the belief in one’s personal capability to organize and execute behaviors. People who have strong beliefs in their abilities are more likely to perform behaviors and more likely to be successful as a result (Bandura, 1997). Thus, parents who are confident in their ability to talk to their youth about sexuality issues are more likely to do so. The purpose of this systematic literature review is to provide an overview of the research on parent-youth sexual communication and family-level interventions designed to reduce at-risk sexual behaviors in youth.
Research Questions
We explored the following research questions:
How does parent-youth communication impact sexual behaviors in pre-adolescent and adolescent youth?
What role do fathers have in promoting their youth’s sexual health?
Methods
Literature Search
The literature search was conducted using EndNote, a search tool/citation management software, and Proquest, an electronic database. Both EndNote and Proquest feature premier scholarly journals with a broad range of topics, including social research. The search used a combination of the following terms: fathers, parents, youth, sexual behaviors, sexually transmitted diseases or infections, HIV, communication, parent(ing) programs or interventions.
The search generated 200+ articles for EndNote and 16 for Proquest that were published in English between 2003 and 2013. The list of articles included quantitative or qualitative studies that focused on parent and youth communication about sexual health. A thesis was excluded from the review. The search yielded a few relevant studies from countries outside the United States; those were included in the review. However, we did not conduct a thorough search for international studies.
Inclusion/Exclusion Criteria
The criteria used to include and exclude articles were based on the suggestions from Littell, Corcoran, and Pillai (2008). Studies were eligible for inclusion if they pertained to parent and youth communication about sexual health and sexual behaviors to reduce or prevent STIs or early parenthood in youth. We planned to include studies on youth aged 18 years and younger; primarily youth in middle or high school.
Two practical screens were conducted separately by graduate research assistants #1 and #2 to ensure each article’s applicability to the study. Those articles not pertaining to the specific area of research were excluded from the lists, and the remaining were saved and tallied. Using the same search criteria as with the EndNote search, the first author and graduate research assistant #2 conducted additional, separate searches using Proquest in order to identify other articles not revealed in the EndNote search. These lists were then combined; duplicates were eliminated.
Quality Assessment
We assessed each quantitative study on its own methodological quality using several components adapted from the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies (National Collaborating Centre for Methods and Tools, 2008). This approach works well with analyzing studies in which there is a scarcity (e.g., father-youth dyads were not well represented in the body of literature) (Little et al., 2008). The components included: Selection bias, study design, based on the hierarchy of evidence, data collection tools, and analyses (see Appendix 1). Lower ratings indicate greater study quality.
Results
The full text of the selected articles was reviewed for 45 studies. Initially, 38 studies were selected for inclusion. However, the first author further excluded studies that pertained to: communication about sexuality and HPV vaccination; general information shared in parent-youth sexual health communication without reported association with sexual behaviors; parent factors (not specific to communication) on youth sexual behaviors; general youth risky behaviors, such as delinquent behavior; a conceptual basis for a HIV prevention program; protective and risk factors associated with sexual debut and risky sex; college students 19 years and older, without prior assessment as youth under 19 years old; HIV-positive study participants; and men who have sex with men. These were excluded because they did not pertain specifically to the variables of interest in the general population of youth. The Cochrane Library yielded one additional study not found using any of the above methods. Ultimately, a total of 23 studies were selected for inclusion in this review. Of the studies reviewed, there were 5 qualitative studies and 18 quantitative studies (see Table 1).
Table 1.
Study Methods and Findings
| Author & Year |
Design | Sample/Sample Size | Measure/ Data Collection |
Analysis | Main Findings | Quality Rating |
|---|---|---|---|---|---|---|
| Akers et al. (2010) | Cross-sectional interview | 53 African American families in Pennsylvania (68 parents, 57 adolescents) | 21 focus groups | Grounded theory approach to content analysis and constant comparison method | Contraceptive knowledge was low. Parents more often helped male adolescents get condoms than helping females get contraceptives. | N.A. |
| Bersamin et al. (2008) | One group pre, post-test | 887 adolescents who had never had sex. Latinos (12%), African Americans (5%), Asians (including Native American and Pacific Islander, 9%), European Americans (67%), multiple ethnicity (3%), 34 unknown ethnicities (4%) | Computer AssistedSelf Interviews (CASIs) administered in the home. α range = .67 - .78 | CFA; Logistic regressions | Greater communication with parents increased likelihood of youth initiating oral sex | 9 |
| Clawson & Reese-Weber (2003) | Cross-sectional survey | 214 youth ages 18–21.White (82.2%), AfricanAmerican (9.3%), Hispanic (5.6%), and Asian American(1.9%) | Measure of Family Sexual Communication Scale. Also, sexual risk communication variables from CDC scale. α range = .88 - .91. | Hierarchical regressions | Increase in sexual initiation, frequency of intercourse, number of sexual partners. Decrease in unprotected sex | 10 |
| DiIorio, Lehr, Wasserman, Eichler, Cherry, & Denzmore (2006a) | Cross-sectional interview | 14 African-American fathers of adolescent boys between the ages of 11 and 14 years | Focus group;open-ended and semi-structured questions | Content analysis | African-American fathers place a high value on fatherhood and accept their roles as sex educators of their male children | N.A. |
| DiIorio, McCarty, & Denzmore, (2006b) | Randomized controlled trial | 277 African American youth 11 and 14 years and their fathers, youth members of Boys & Girls Club of Atlanta | Sex-based communication measure consisting of16 sex-specific topics. α range = .83 −.97. | Mediation analyses | Effect of the intervention on father–son communication was mediated by differences in self-efficacy to talk about sex with son. Greater level sexual health communication and self-efficacy in intervention group than control group | 4 |
| Dilorio, McCarty, Resnicow, Lehr, & Denzmore (2007b) | Randomized controlled trial | 277 fathers and their 11- to 14-year-oldadolescent sons Most participants were African American (97%) | Composed of a list of sex-specifictopics measured sex-based communicationbetween fathers and sons. Participantsresponded on a 0-to-3 rating scale. α range = .89 - .97. | Independent-sample t-tests and Chi-square tests | Decrease in sexual initiation, sexual intent, frequency of intercourse, unprotected sex. Increase in abstinence | 4 |
| DiIorio, McCarty, Denzmore, & Landis, (2007a) | One group pre- post-follow-up | 425 African-American youth ages 12–15 | A 25-item scale (DiIorio et al., 1999) was used to measure communication about sex (yes, no). α range = .87 - .91. | Linear and logistic regression | Girls who talked more with their mothers about sexual topics were less likely to be involved in intimate sexual behaviors and to have initiated sexual intercourse than those who discussed few sex topics with their mothers. | 8 |
| Gillmore et al. (2011) | Secondary data analysis longitudinal ADD Health data. Cohort pre- post-follow-up | 10,131 participants; Wave 1 youth ages 13–19 in the U.S. and Wave 3 ages 19–27; African American (19.6%), Chinese American (1.6%), Mexican American (54.04%) and White (68.8%) | Parent–Child Communication About Sex. α range = .60 - .89. | Multinomial logisticregression | More frequent parent communication associated withincrease in frequency of intercourse. African American males greater condom use. | 8 |
| Guilamo-Ramos et al. (2007) | Cross-sectional survey | 668 inner-city middle school students and their mothers.132 African American, 264 Dominican, 158 Puerto Rican, the remainder were Haitian, or from a different Latino subgroup. | Self-administered questionnaires. α = .85; also α not tested for other scale items. | Logistic regression or ordinary least squares regression | Boys reported higher intentions, more positive expectancies, and lower levels of maternal communication. 25% of the adolescents indicated openness to engaging in sexual behaviors. The more the youth perceived their mother talked with him/her about sex topic, the more the youth expected to refrain from sex with respect to that topic. | 9 |
| Guilamos-Ramos et al. (2011) | Randomized clinical trial | 2,016 Latino and Black mother-adolescentdyads in New York City | Items structured to use a five-point agreement range. α not tested. | Logistic regression | FFT enhanced parenting practices. 79% of youth in the two FTT (parent-only groups) combined reported that their mothers had ever talked with them about not having sex, and 68% of youth in the MAD condition. FFT and MAD comparable in delaying initiation of sexual intercourse. | 5 |
| Hadley et al. (2009) | Cross-sectional survey | 485 Adolescents 13–18 years; had ever had sex; had been in mental health treatment within the past year African-Americans 65%, but 9% were Latinos | Included youth sexual activity items; Parent and youth Miller Sexual Communication Scale. α = .86; others did test α. | Logistic regression | Greater open communication by parent associated with decrease in unprotected vaginal or anal sex | 9 |
| Malcolm et al. (2013) | Cross-sectional survey | 171 Hispanic, Predominately male (73.1%) sexually active, problem behavior adolescents (mean age = 14.88 years) | Participants completed the assessment battery; taken from baseline assessments of two randomized clinical trials conducted. α range = .62 - .96. | Structuralequation modeling | Decrease in unprotected sex. Higher levels of parent–youth communication about sex directly and positively associated with condom use attitudes. Both condom attitudes and control beliefs directly and positively associated with condom use intentions. Increase in intentions to use condoms associated with an increase in condom use at last sexual intercourse. | 9 |
| Miller et al. (2011) | Randomized controlled trial | 1115 African American parent-preadolescentdyads | Data were taken from a CDC RCT. α range = .76 - .94. | Wilcoxon rank sum tests | Decrease in unprotected sex. Increase in abstinence | 4 |
| Murry et al. (2011) | Clustered-randomizedcontrolled trial | 332 families. African American mothersand their 11-year-old children at Wave 1 and follow-up at 17 years old at Wave 2;resided in nine rural counties in Georgia | Parent-Child Communication Scale, Racial Socialization Scale, three-item Black Pride scale, Risk Prototype Scale and several other measures. α range = .57 - .82 | Structural Equation Modeling | Fewer youth at age 17 years had ever had sex, and those who had become sexually active reported fewer sexual encounters, and greater likelihood of using condoms during sexual encounters. | 4 |
| Nielsen et al. (2013) | Cross-sectional interviews | 10 females from an undergraduatehealth sciences class at a large Midwestern university.Nine Caucasian, one “other” | Five-point Likert scale | Grounded Theory | Perceived good sexual educators themes: emotional closeness; comfort level during sexually specific conversations; degree of direct communication; humor; monitoring; belief that sexuality education for daughters is not solely a mother’s responsibility. | N.A. |
| O’Donnell et al. (2005) | Randomized controlled trial | 846 families-mothers, fathers, daughters, sons.(64% were black and 29% were Hispanic) 83% aged 10–11 years. Of the 674 parents at baseline, 92% were female; 88% were mothers/ mother figures. | Point rated scale items regarding pubertal changes, sexual abstinence, risk behaviors, and peer and media influences. α range = .68 −.96. | Multivariate logistic andlinear regression | Parents in intervention had more communication with youth about risk behaviors, had greater self-efficacy to discuss puberty and sexuality, and more likely to perceive influence over youths’ behaviors than controls. Youths in the intervention had higher family support, more family rules and fewer behavioral risks than controls. | 4 |
| Ohalete et al. (2010) | Cross-sectional ethnographicstudy | 19 African-American fathers | Tape-recorded individual interviews | Manifest and latent content analysis | Fathers reported talking with youth morality, sexuality, sexual health, early parenthood and relationships. Fathers began conversations before adolescence and felt it was equally important to have reproductive health communication with sons and daughters. Fathers more comfortable talking with sons than daughters. | N.A. |
| Villarruel et al. (2008) | Randomized controlled trial | 791 Mexican parents | 5–point Likert–typescales. α range = .59 - .94. | Generalizedestimation equation | Greater parent communication about sexual risk in intervention group than control group | 4 |
| Villarruel et al. (2010) | Randomized controlled trial | 130 parents and 130 Latino adolescents | 4- or 5-pointLikert-type scales. α range = .67 - .96. | Analysis of covariance | Parents in brief computer-based intervention had greater sexual communication and greater comfort discussing sex with youth. Youth of intervention parents had greater sexual communication | 4 |
| Wilson & Dalberth, & Koo (2010) | Cross-sectional interview | 131 Parents of youth aged 10–12. Blacks, whites, English-speaking Hispanics, and Spanish-speaking Hispanics | Focus group | Content analysis | Fathers are more likely than mothers to leave communication about sex to the other parent, but better suited to address certain topics (e.g., male puberty, but not menstruation). Fathers are less likely than mothers to advise delaying sex until marriage. | N.A. |
| Wilson & Koo (2010) | Randomized controlledexperiment | 829 fathers and 1,113 mothers of children aged 10 to 14. Predominantly white | Selected items from 8 measures of communication about sex. α not reported for any measures. | Chi-square test | Parents of daughters talked more about sexual topics, were more concerned about potential harmful consequences of sexual activity, and were more disapproving of their child having sex at an early age. | 6 |
| Wyckoff et al. (2008) | Secondary data analysis of Parents Matter! One group pre- post- follow-up | 135 African-American mothers, fathers, and their 9–12-year-old youth | 10-item measure of communication about risk factors for sexual activity, sexual communication, and sexual risk prevention. α not reported for any measures. α not reported for any measures. | Chi-square test | Abstinence was not discussed by majority of sons with either parent. Father-daughter dyads did not discuss abstinence, puberty, reproduction, and sex. Condoms were not discussed by majority of participants. Few preadolescents reported discussing HIV/ AIDS with their parents, though a majority of parents reported discussing the topic with their youth. | 9 |
| Yang et al. (2007) | One group pre- post- follow-up | 817 African-American adolescents andtheir parents | The Youth Health Risk Behavioral Inventory. α range = .73 - .95. | Logistic general estimating equation models | Parental monitoring had protective effects on risky behavior over two-years. Increase in abstinence in girls. Increase in sex for youth who perceived problem communication with parents. Sex remained stable for youth perceiving less problem communication with parents. | 8 |
Design and Sample
We systematically reviewed a variety of studies, which included five cross-sectional qualitative interviews (e.g., Akers, Schwarz, Borrero, & Corbie-Smith, 2010), cross-sectional surveys (e.g., Clawson & Reese-Weber, 2003), and randomized controlled trials (e.g., Guilamo-Ramos et al., 2011; Murry et al., 2011) concerning parent-youth sexual health communication. Study samples of parents consisted of both mothers and fathers, or solely fathers (e.g., DiIorio, McCarty, Resnicow, Lehr, & Denzmore, 2007b). The studies also included female and/or male youth. See Table 1 for details of extracted data.
Parent-Youth Sexual Health Communication Interventions
The intervention studies reviewed here typically were designed to enhance the frequency, depth or quality of the content (i.e., effectiveness) in parent-youth communication about sexual health. The sexual health content refers to accurate information about STIs, HIV, or early parenthood, for example, in order to increase parents’ and youth’s knowledge about sexual health risks and protection. There also were common elements that interventions encompassed that indicated their comprehensiveness. These included a focus on: the parent(s) (or parent figure[s]) and youth; early intervention at pre-adolescence; parental self-efficacy to talk about sex; parents’ expressing to youth their feelings and expectations about their not engaging in sex; knowledge of STIs, risks and protection as well as; racial or ethnic minorities’ attitudes, beliefs, and norms (e.g., regarding manhood and sex) that could lead to barriers with absorbing and applying knowledge.
To illustrate, Murry et al. (2011) implemented The Strong African American Families (SAAF) program, a family-focused, comprehensive communication intervention developed specifically for rural African Americans. The intervention entailed: regulated, communicative parenting; involved, vigilant parenting; racial socialization; sexuality communication, and; general communication. The main goal of their intervention was to understand and support the ways parents promoted youth’s sexual health and dissuaded at-risk sexual behaviors. They found increases in parent-youth communication about engaging in at-risk sexual behaviors.
Most interventions appear to foster some form of three major aspects of the above model programs: parent and youth intervention, self-efficacy or comfort in talking with youth about sex, and sexual health or STI knowledge. Mainly, the interventions included a self-efficacy component to enhance parents’ confidence so that they can talk with their youth to prevent their at-risk sexual behaviors. For example, in a randomized controlled study of 791 Mexican parents and their adolescents in the HIV risk reduction intervention group (intervention consisted of computer-based technology) reported more general communication, more sexual risk communication, and more comfort in communicating with their adolescents than parents in the waitlist control group (Villarruel et al., 2008).
There were usually more favorable outcomes for those parents who participated in such an intervention compared to those who were not in an intervention. Parents in the interventions possessed greater knowledge about sexual health topics, greater self-efficacy to communicate with their youth, and more frequent communication with their youth (DiIorio et al., 2006b; DiIorio et al., 2006a; Guilamo-Ramos et al., 2011; Miller et al., 2011; Wyckoff et al., 2008). For instance, in a randomized trial involving 277 fathers (includes father figures) (97% African-American) and their sons, Dilorio and her colleagues’ (2007b) tested the effect of the “R.E.A.L. Men Intervention” in preparing fathers to discuss STIs with their sons. Fathers were provided helpful information about communicating with adolescents, peer relationships, important sexuality topics for adolescents, and specific information about the transmission and prevention of HIV. The researchers found that fathers served as important educators of sex and HIV for their sons (Dilorio et al., 2007b). Moreover, fathers who participated in an intervention group reported significantly more discussions with their sons about sexuality than control group fathers (Dilorio et al., 2007b).
Youth’ s Sexual Health Outcomes
Sexual abstinence.
The majority of the studies designed to test the association between parent-youth communication and youth’s sexual health factors yielded findings indicating that better communication was associated with less at-risk sexual behaviors among youth (see Table 1 for the list of findings). Specifically, based on this review, enhanced parent-youth communication is related to an increase in sexual abstinence (DiIorio, McCarty, Denzmore, & Landis, 2007a; Dilorio et al., 2007b; Guilamo-Ramos, Jaccard, Dittus, Bouris, Holloway, & Casillas, 2007; Miller et al., 2011; Murry et al., 2011; O’Donnell et al., 2005; Yang et al., 2007).
Sexual initiation and frequency.
Parent-youth communication is also associated with a decrease in sexual initiation (Dilorio, Lehr, Wasserman, Eichler, Cherry, & Denzmore, 2006a; Dilorio et al., 2007a; Dilorio et al., 2007b; Guilamo-Ramos et al., 2011; Murry et al., 2011; O’Donnell et al., 2005). Additionally, our review shows that enhanced parent-youth communication is related to a decrease in the frequency of intercourse (Dilorio et al., 2007b; Guilamo-Ramos et al., 2011; Murry et al., 2011). However, in their pre-test post-test assessment of 817 African-American adolescents and their parents from 35 low-income urban communities, Yang et al. (2007) did not find a statistically significant association between boys’ perception of open communication with their parents and their engaging in sex.
Condom use.
Our review of the studies indicated that enhanced parent-youth communication is related to a decrease in unprotected sex (Clawson & Reese-Weber, 2003; Dilorio, et al., 2006a; Dilorio et al., 2007b; Hadley, Brown, Lescano, Kell, Spalding, Diclemente, & Donenberg, 2009; Malcolm, Huang, Cordova, Freitas, Arzon, Jimenez, & Prado, 2011; Miller et al., 2011; Murry et al., 2011). Of note, greater sexual communication between mothers and youth was shown to be significantly associated with decreased HIV risk, for up to three months, and increased protection from HIV (Kapungu, Baptiste, Holbeck, McBride, Robinson-Brown, Sturdivant et al., 2010).
Research indicated that family support, monitoring, and communication were associated with more consistent condom use by youth and fewer incidents of unprotected sex (Murry et al., 2011; Yang et al., 2007). Additionally, family functioning has been found to indirectly affect condom use through communication about contraception and sex (Malcolm et al., 2011). Adolescents who had discussions with their parents about using condoms were more likely to have used condoms in their most recent sexual encounters (Hadley, Brown, Lescano, Kell, Spalding, Diclemente, & Donenberg, 2009).
One study indicated that although communication with parents helped to protect youth from engaging in at-risk sexual behaviors, the effects were not long-term (Gillmore, Chen, Haas, Kopak, & Robillard, 2011). Gilmore et al. reported that the effects faded as they transitioned to late adolescence and early adulthood. These researchers also found that Black males had greater condom use than other racial/ethnic groups in their study (Gilmore et al., 2011). We note that these results could be attributed to the age range of the sample. They were much older than the middle and high school aged youth in the majority of studies reviewed here; thus, it is likely that they have matured in their sexual decision making.
Other researchers have found parent-youth sexual health communication to be related to an increase in sexual initiation (Bersamin, Todd, Fisher, Hill, Grube, & Walker, 2008; Clawson & Reese-Weber, 2003; Yang et al., 2007), an increase in the number of sexual partners (Clawson & Reese-Weber, 2003), and an increase in the frequency of intercourse (Clawson & Reese-Weber, 2003; Gillmore et al., 2011). To explain these contradictory findings, researchers have speculated that perhaps parents began sexual health talks too late—only after they suspected their youth were already having sexual intercourse (Clawson & Reese-Weber, 2003; Gilmore et al., 2011). These samples were predominantly Caucasian (see Table 1), which was not representative of minorities who are most affected by sexually transmitted infections in the United States. Also, compared to most youth in the studies reviewed, the youth in the Clawson and Reese-Weber (2003) study were older, which we speculate might have also contributed to the differences in the results. Additionally, Yang et al. (2007) have attributed an increase in sex for the African American youth studied to perceived problem communication with their parents. Further, they report that sex among youth remained constant when they perceived less problem communication with their parents.
Communication Barriers
There were a number of barriers that prevented parents from educating their youth about sexual health related topics. For instance, some parents experience discomfort when talking with their youth about sex (Ohalete, Georges, & Doswell, 2010) and fathers, in particular, do not feel prepared to discuss factual information about puberty (Wilson, Dalberth, & Koo, 2010), do not discuss information about condoms as a means of prevention of STIs (Wyckoff et al., 2008), and communicate information that is not age-appropriate (DiIorio et al., 2006a) or suitable for their youth (DiIorio et al., 2006a; Dilorio et al., 2007b).
Parents’ sexual health knowledge and comfort with sexual topics can predict sexual communication between parents and their youth (Jerman & Constantine, 2010). Greater parental knowledge of sexual health, as well as comfort with sexual topics, have predicted more extensive sexual communication between parents and their youth (Jerman & Constantine, 2010). However, inconsistencies between mothers’ and adolescents’ reports about sexual communication have been marginally associated with decreased protection from sexual risks (Kapungu et al., 2010). According to Wyckoff et al. (2008), the majority of preadolescent youth in their study reported that their parents did not discuss condom use as a preventive measure against HIV, even though their parents reported that they had discussed HIV prevention with them (Wyckoff et al., 2008). It is critical to not only increase the frequency of parent-youth communication about sexual health, but also provide the needed knowledge and preparation to give accurate, adequate and appropriate information to youth to reduce sexual risk.
Fathers’ roles in communicating about sex, particularly with their adolescent sons, have not been as widely studied as mothers’ roles. But when compared to mothers, fathers encounter more barriers, including lower self-efficacy and lower confidence that discussing sex will result in positive outcomes (Wilson et. al., 2010). In a qualitative study in which 14 African American fathers were interviewed about their communications with their sons about sex and HIV prevention, one barrier identified was not knowing how to facilitate father-son sexual communication (DiIorio et al., 2006a). For instance, fathers felt that it was unnatural for males to communicate with each other males about sexual issues.
In a qualitative study, 16 focus groups were conducted in three U.S. cities with 131 parents of children aged 10–12 from various racial/ethnic backgrounds to elicit perspectives about fathers’ communications with their youth about sex (Wilson, Dalberth, & Koo, 2010). The researchers found that fathers felt they were more capable to discuss certain male-oriented topics such as male puberty, when compared to more female-specific topics such as menstruation. Moreover, these fathers specifically reported having difficulty communicating with their daughters about sex, and felt that sensitive topics were most appropriate for mothers to handle (Wilson et al., 2010). Ohalete et al. (2010) also found that 10 of the 18 African American fathers in their qualitative ethnographic study reported discomfort in communicating with their youth about sex. In some father-youth discussions about reproductive health and delaying sex to prevent HIV/AIDS, the conversations were not appropriate for the youth’s developmental age (Ohalete et al., 2010). Similarly, Wilson et al. (2010) reported that a father took pride in his teen-aged son who reported having had sex, because he felt that initiating sex was a rite of passage for males.
Gender has been shown to affect the sexual health information that is communicated and to whom. A large national online survey with 829 fathers and 1,113 mothers of youth aged 10 to 14 found that parent-youth communication about sexual topics depended on the gender of both the parent and the youth (Wilson & Koo, 2010), though the reasons for this were unknown. Gender biases do exist in regard to the type of information given to sons and daughters (Akers et al., 2010). African American fathers view their fatherhood role highly and they have a desire to inform their sons about sex more so than their daughters (DiIorio et al., 2006a; Wilson, Dalberth, & Koo, 2010). Thus, they tend to communicate about sexual topics less with daughters than with sons (Wilson & Koo, 2010; Wyckoff et al., 2008).
In a qualitative study of 53 black families (68 parents and 57 adolescents), Akers et al. (2010) found that mothers and fathers were more likely to inform their sons how to obtain condoms. However, they did not inform their daughters about obtaining contraception (Akers et al., 2010). Other research indicated that mothers’ parental messages for girls were more protective than for boys (Kapungu et al., 2010). In a study of 135 African-American mothers, fathers, and their preadolescent sons and daughters, Wyckoff et al. (2008) found that the majority of the parents and their youth reported communicating about most sexuality topics. However, fathers were less likely than mothers to communicate with their daughters (Wyckoff et al., 2008). Both mothers and fathers were equally likely to communicate with sons about sexuality, but, most of the sons did not receive information about abstinence from either of their parents (Wyckoff et al., 2008). Other research has found that mother-daughter communication about sex was more frequent than that between mothers and sons (Kapungu et al., 2010). In Kapungu et al.’s (2010) study, 162 African-American mother-adolescent dyads from impoverished urban neighborhoods with high HIV rates completed self-report measures of sex-related communication. They found that boys talked less than girls to their mothers, fathers, and peers about sex-related topics (Kapungu et al., 2010).
Key Findings
Using the EPHPP Tool, we found the most rigorous studies were: (a) DiIorio, McCarty, & Denzmore, 2006b; (b) DiIorio et al, 2007b; (c) Guilamo-Ramos et al., 2011; (d) Miller et al., 2011; (e) Murry et al., 2011; (f) O’Donnell, Stueve, Agronick, Wilson-Simmons, Duran, & Jeanbaptiste, 2005 and; (g) Villarruel et al., 2008. Their quality scores ranged from 4 to 5. Additionally, these studies were conducted with participants who were representative of the target population. They all were either randomized controlled trials or a randomized clinical trial. They also included standardized measures, though the internal consistency for some scale items was not measured. Finally, the statistical methods were appropriate for the study design.
Noteworthy, was that the contradictory studies were amongst those with the lowest quality ratings: (a) Bersamin et al., 2008; (b) Clawson & Reese-Weber, 2003; (c) Gilmore et al., 2011) and; (d) Yang et al., 2007. Their scores ranged from 8 to 10, mainly due to their study design. The studies with the least quality were the cross-sectional or one-group pre-test post-test studies. See Table 1 for a complete listing of quality ratings.
Other Current Reviews
To our knowledge, there is one relatively recent review conducted prior to ours on the topic of youth sexual risk and parent-youth communication to reduce youth at-risk behavior (Commendador, 2010). Commendador’s review was conducted between 1980 and 2007 on parental (mainly mothers) and maternal influences on contraceptive decision making. She reported results from 35 research studies and 15 scholarly articles. The literature revealed there was an association between parental communication, parenting style, and adolescent sexual activity and contraception use. Additionally, she found that maternal communication was shown to delay sexual intercourse and increase contraceptive use, which had implications for mother-youth communication as an intervention to impact age at sexual initiation and contraception use. In our estimate, there were obvious gaps in the literature because of the lack of studies on the influences of paternal influences on their youth’s at-risk sexual behaviors. Commendador’s review differs from ours in that her main focus was on mothers and youth, thus little research on fathers and youth was included.
Discussion
Current research suggests that parents play a pivotal role in reducing at-risk sexual behaviors in adolescents and consequently, in decreased rates of STIs for their youth. The literature also suggests that sexual health conversations are needed before children become adolescents and become sexually active. Therefore, we explored the following: Research Question 1. How does parent-youth communication impact sexual behaviors in pre-adolescent and adolescent youth? Several researchers have found that parent-youth sexual health communication is associated with higher rates of sexual abstinence, condom use and intent to delay initiation of sexual intercourse, which can prevent infectious disease (DiIorio et al., 2007a; Guilamo-Ramos et al., 2007; Wyckoff, Miller, Forehand, Bau, Fasula, Long, & Armistead, 2008).
We found that there are several important components that must be included in intervention studies to increase parent-youth communication to prevent at-risk sexual behaviors. First, parents must receive interventions to enhance their confidence and capability to engage their sons and daughters in sexual health discussions. They also must receive accurate knowledge pertaining to sexual health risks and prevention to educate and guide their youth.
Research question 2: What role do fathers have in promoting their youth’s sexual health? The majority of the research on at-risk sexual behaviors in youth has examined the role of the mother; more research is needed with fathers (Coakley, Shears, & Randolph, 2014; Roberts, Coakley, Washington & Kelley, 2014). The father involvement literature shows that fathers contribute positively to numerous psychosocial and developmental outcomes in youth (Lamb, 2010; Palkovitz, 2002; Pleck, 2010; Roberts et al., 2014). However, there are significant gaps in the literature regarding fathers’ role in protecting their youth from sexual risk. As a result, we do not fully understand how fathers communicate and influence youth’s behaviors. It is important to undertake research that values the father’s role in the African American family and community. Although we feel strongly that fathers’ have an important role to protect youth from risk, we recognize that numerous fathers are not involved in their children’s lives. Therefore, we need to recognize that men, particularly male family members, can serve as important role models for African-American youth (Shears, Miller, McGee, Farinde, & Lewis, 2014; Wyckoff et al., 2008). As men adopt a protective role for children in their extended family, the father-youth and father figure-youth communication are equally important for reducing youth’s at-risk sexual behavior.
Based on the review, fathers experience barriers to communicating related to lower self-efficacy and lower confidence in their communication abilities (Wilson & Koo, 2010). Therefore, we recommend that intervention research be designed to support fathers to overcome barriers to communicating with both sons and daughters. Including daughters is important since research has shown that African-American fathers communicate about sexual topics less with daughters than with sons (Wyckoff, Miller, Forehand, Bau, Fasula, Long, & Armistead, 2008). Nielsen, Latty, and Angera (2013) studied fathers who were perceived as good sexual educators for their daughters and found several key themes among their successful fathers. Such themes included, emotional closeness with their daughters, active parenting, humor, and honesty about communicating about sexuality. Future research that include fathers and daughters could examine how those characteristics are associated with effective sexual communication between parents and youth.
Conclusion
Later childhood and early adolescence is a critical period when youth are vulnerable to engaging in at-risk sexual behaviors that could lead to STIs, HIV, and early parenthood. It is crucial to provide parents with the supports that enable them to intervene at this stage of their child’s life. Ideally, when parents are provided with the necessary tools to assist them in becoming better communicators with their youth regarding sexual activity, the effect of the parent on their youth’s sexual behavior may be revealed. Further, if fathers are properly equipped with accurate knowledge and skills, they could be an invaluable resource to reduce the incidence of infectious disease and early parenthood that have plagued youth. Additional research is needed to explore fathers’ perceptions of their role and impact on their youth’s at-risk sexual behaviors. Researchers should seek to understand specific factors that promote and inhibit fathers from talking with their youth about sexual health.
Figure 1.
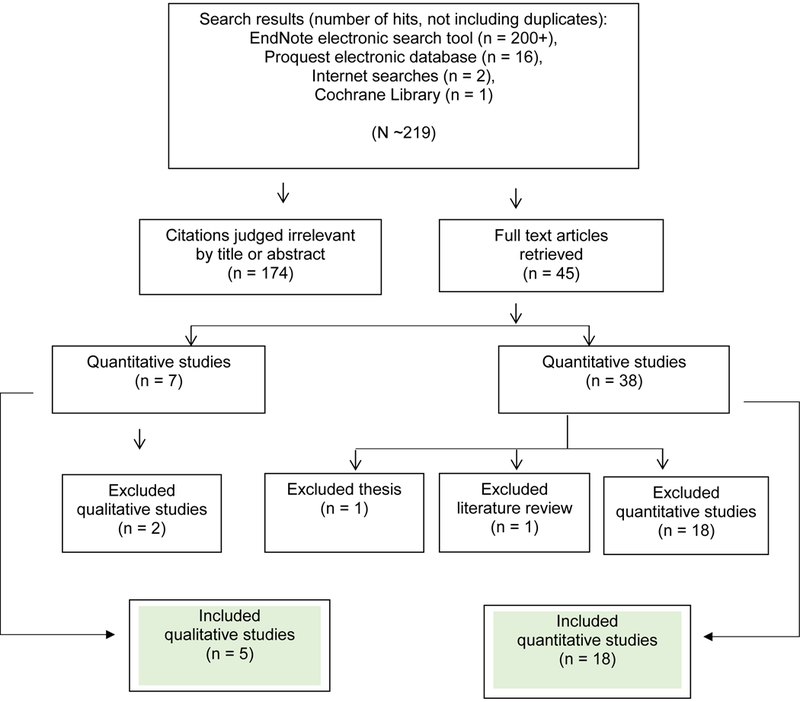
Literature Search Results
Appendix 1
QUALITY ASSESSMENT TOOL
SELECTION BIAS
Are the study participants likely to be representative of the target population?
1 = Yes
2 = No
STUDY DESIGN
1 = Randomized controlled trial
2 = Controlled clinical trial
3 = Cohort analytic (two group pre- + post-test)
4 = Case-control
5 = Cohort (one group pre- + post-test)
6 = Other (e.g., cross-sectional survey)
7 = Can’t tell
DATA COLLECTION METHODS
Were the data collection tools reliable?
1 = Yes
2 = No
ANALYSES
Are the statistical methods appropriate for the study design?
1 = Yes
2 = No
References
- Akers AY, Schwarz EB, Borrero S, & Corbie-Smith G (2010). Family discussions about contraception and family planning: A qualitative exploration of black parent and adolescent perspectives. Perspectives on Sexual and Reproductive Health, 42(3), 160–167. doi: 10.1363/4216010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bandura A (1997). Self-efficacy: The exercise of control. New York, NY: Freeman. [Google Scholar]
- Bartlett TR, Holditch-Davis D, & Belyea M (2007). Problem behaviors in adolescents. Pediatric Nursing, 33(1), 13–36. [PubMed] [Google Scholar]
- Bersamin M, Todd M, Fisher DA, Hill DL, Grube JW, & Walker S (2008). Parenting practices and adolescent sexual behavior: A longitudinal study. Journal of Marriage and Family, 70(1), 97–112. doi: 10.1111/j.1741-3737.2007.00464.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Byers ES, Sears HA, & Weaver AD (2008). Parents’ reports of sexual communication with children in kindergarten to grade 8. Journal of Marriage and Family, 70, 86–96. doi: 10.1111/j.1741-3737.2007.00463.x [DOI] [Google Scholar]
- Centers for Disease Control and Prevention (CDC). (2012). Youth risk behavior surveillance United States 2011. Morbidity and Mortality Weekly Report, 61(4), 1–162. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC). (2015). HIV Surveillance Report, 2014; vol. 26 Retrieved from http://www.cdc.gov/hiv/library/reports/surveillance/ [Google Scholar]
- Centers for Disease Control and Prevention (CDC). (2014). HIV and AIDS among African American youth. Fact sheet. Retrieved from http://www.cdc.gov/nchhstp/newsroom/docs/CDC-Youth-AAs-508.pdf
- Clawson CL, & Reese-Weber M (2003). The amount and timing of parent-adolescent sexual communication as predictors of late adolescent sexual risk-taking behaviors. The Journal of Sex Research, 40(3), 256–265. Retrieved from http://search.proquest.com/docview/215280215?accountid=14604 [DOI] [PubMed] [Google Scholar]
- Coakley TM, Shears J, & Randolph SD (2014). Understanding key barriers to fathers’ case planning involvement.Child & Youth Services, 35(4), 343–364. doi: 10.1080/0145935X.2014.972550. [DOI] [Google Scholar]
- Commendador KA (2010). Parental influences on adolescent decision making and contraceptive use. Pediatric Nursing, 36(3), 147–170. [PubMed] [Google Scholar]
- DiIorio C, Lehr S, Wasserman JL, Eichler M, Cherry C, & Denzmore P (2006a). Fathers Are Important People: A Study of Father-Son Sexual Communication. Journal of HIV/AIDS Prevention in Children & Youth, 7(1), 55–72. doi: 10.1300/J499v07n01_04 [DOI] [Google Scholar]
- DiIorio C, McCarty F, & Denzmore P (2006b). An exploration of social cognitive theory mediators of father–son communication about sex. Journal of Pediatric Psychology 31(9), 917–927, 2006 doi: 10.1093/jpepsy/jsj101 [DOI] [PubMed] [Google Scholar]
- DiIorio C, McCarty F, Denzmore P, & Landis A (2007a). The moderating influence of mother-adolescent discussion on early and middle African-American adolescent sexual behavior. Research in Nursing & Health, 30(2), 193–202. Retrieved from http://onlinelibrary.wiley.com/journal/10.1002/(ISSN)1098-240X [DOI] [PubMed] [Google Scholar]
- Dilorio C, McCarty F, Resnicow K, Lehr S, & Denzmore P (2007b). REAL Men: A group-randomized trial of an HIV prevention intervention for adolescent boys. American Journal of Public Health, 97(6), 1084–1089. doi: 10.2105/ajph.2005.073411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fergus S, Zimmerman MA & Caldwell CH (2007). Growth trajectories of sexual risk behavior in adolescence and young adulthood. American Journal of Public Health, 97(6), 1096–1101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillmore MR, Chen AC, Haas SA, Kopak AM, & Robillard AG (2011). Do family and parenting factors in adolescence influence condom use in early adulthood in a multiethnic sample of young adults? Journal of Youth and Adolescence, 40(11), 1503–1518. doi: 10.1007/s10964-011-9631-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guilamo-Ramos V, Jaccard J, Dittus P, & Bouris A (2007). Adolescent expectancies, parent-adolescent communication and intentions to have sexual intercourse among inner-city, middle school youth. Annals of Behavioral Medicine, 34(1), 56–66. doi: 10.1080/08836610701495664 [DOI] [PubMed] [Google Scholar]
- Guilamo‐Ramos V, Jaccard J, Dittus P, Bouris A, Gonzalez B, Casillas E, & Banspach S (2011). A comparative study of interventions for delaying the initiation of sexual intercourse among Latino and Black youth. Perspectives on Sexual and Reproductive Health, 43(4), 247–254. doi: 10.1363/4324711 [DOI] [PubMed] [Google Scholar]
- Hadley W, Brown LK, Lescano CM, Kell H, Spalding K, Diclemente R, & Donenberg G (2009). Parent-adolescent sexual communication: Associations of condom use with condom discussions. AIDS and Behavior, 13(5), 997–1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaccard J, Dodge T, & Dittus P (2002). Parent adolescent communication about sex and birth control: A conceptual framework In Feldman SS & Rosenthal DA (Eds.), Talking sexuality: Parent-adolescent communication (pp. 9–41). San Francisco, CA: Jossey-Bass. [DOI] [PubMed] [Google Scholar]
- Jerman P, & Constantine NA (2010). Demographic and psychological predictors of parent-adolescent communication about sex: A representative statewide analysis. Journal of Youth and Adolescence, 39(10), 1164–74. Retrieved from http://search.proquest.com/docview/746772485?accountid=14604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kapungu CT, Baptiste D, Holmbeck G, McBride C, Robinson-Brown M, Sturdivant A, … Paikoff R (2010). Beyond the “birds and the bees”: Gender differences in sex-related communication among urban African-American adolescents. Family Process, 49(2), 251–264. doi: 10.1111/j.1545-5300.2010.01321.x. [DOI] [PubMed] [Google Scholar]
- Lamb ME (2010). The role of the father in child development (5th ed.). Hoboken, NJ: John Wiley & Sons. [Google Scholar]
- Littell JH, Corcoran J, & Pillai V (2008). Systematic reviews and meta-analysis. Oxford University Press, Inc. [Google Scholar]
- Malcolm S, Huang S, Cordova D, Freitas D, Arzon M, Jimenez GL & Prado G (2013). Predicting condom use attitudes, norms, and control beliefs in hispanic problem behavior youth: The effects of family functioning and parent-adolescent communication about sex on condom use. Health Education and Behavior, 40(4), 384 Retrieved from http://search.proquest.com/docview/1412668494?accountid=14604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller KS, Lin CY, Poulsen MN, Fasula A, Wyckoff SC, Forehand R Long N, & Armistead L (2011). Enhancing HIV communication between parents and children: Efficacy of the Parents Matter! Program. AIDS Education and Prevention, 23(6), 550–563. doi: 10.1521/aeap.2011.23.6.550 [DOI] [PubMed] [Google Scholar]
- Murry VM, Berkel C, Chen Y-F, Brody GH, Gibbons FX, & Gerrard M (2011). Intervention induced changes on parenting practices, youth self-pride and sexual norms to reduce HIV-related behaviors among rural African American youths. Journal of Youth and Adolescence, 40(9), 1147–1163. doi: 10.1007/s10964-011-9642-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Collaborating Centre for Methods and Tools (2008). Quality assessment tool for quantitative studies. (Updated 13 April, 2010). Hamilton, ON: McMaster University; Retrieved from http://www.nccmt.ca/resources/search/14. [Google Scholar]
- Nielsen SK, Latty CR, & Angera JJ (2013). Factors that contribute to fathers being perceived as good or poor sexuality educators for their daughters. Fathering, 11(1), 52–70. [Google Scholar]
- Office of Adolescent Health (OAH). (2016). Trends in teen pregnancy and childbearing. Retrieved from https://www.hhs.gov/ash/oah/adolescent-health-topics/reproductive-health/teen-pregnancy/trends.html
- O’Donnell L, Stueve A, Agronick G, Wilson-Simmons R, Duran R, & Jeanbaptiste V (2005). Saving sex for later: An evaluation of a parent education intervention. Perspectives on Sexual and Reproductive Health, 37(4), 166–173. [DOI] [PubMed] [Google Scholar]
- Ohalete N, Georges J, & Doswell W (2010). Tales From the “Hood:” Placing reproductive health communication between African American fathers and children in context. Association of Black Nursing Faculty in Higher Education Journal, 21(1), 14–20. [PubMed] [Google Scholar]
- Palkovitz R (2002). Involved fathering and child development: Advancing our understanding of good fathering In Tamis-LeMonda CS & Cabrera N (Eds.), Handbook of father involvement: Multidisciplinary perspectives (pp. 119–140). Mahwah, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Pleck JH (2010). Paternal involvement: Revised conceptualization and theoretical linkages with child outcomes In Lamb ME (Ed.), The role of fathers in child development (5th ed, pp. 58–93). Hoboken, NJ: John Wiley & Sons. [Google Scholar]
- Roberts JD, Coakley TM, Washington T, & Kelley A (2014). Fathers’ perspectives on supports and barriers that affect their fatherhood role. SAGE Open. doi: 10.1177/2158244014521818 [DOI] [Google Scholar]
- Satterwhite CL, Torrone E, Meites E, Dunne EF, Mahajan R, Ocfemia MC, … Weinstock H (2013). Sexually transmitted infections among U.S. women and men: Prevalence and incidence estimates, 2008. Sexually Transmitted Diseases, 40(3), 187–193. doi: 10.1097/OLQ.0b013e318286bb53 [DOI] [PubMed] [Google Scholar]
- Shears J, Miller C, McGee M, Farinde A, & Lewis C (2014). Fathers’ presence as a mediator of teacher’s gender effect on self-concept in young African-American males. NHSA Dialog 17(2), 58–67. [Google Scholar]
- Villarruel AM, Cherry CL, Cabriales EG, Ronis DL, Zhou Y (2008). A parent-adolescent intervention to increase sexual risk communication: Results of a randomized controlled trial. AIDS Education and Prevention, 20(5), 371–383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Villarruel AM, Loveland-Cherry CJ, & Ronis DL (2010). Testing the efficacy of a computer-based parent-adolescent sexual communication intervention for Latino parents. Family Relations, 59(5), 533–543. doi: 10.1111/j.1741-3729.2010.00621.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson EK, Dalberth BT, & Koo HP (2010). “We’re the heroes!”: Fathers’ perspectives on their role in protecting their preteenage children from sexual risk. Perspectives on Sexual & Reproductive Health, 42(2), 117–124. doi: 10.1363/4211710 [DOI] [PubMed] [Google Scholar]
- Wilson EK, & Koo HP (2010). Mothers, fathers, sons, and daughters: Gender differences in factors associated with parent-child communication about sexual topics. Reproductive Health, 7, 31. doi: 10.1186/1742-4755-7-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wyckoff SC, Miller KS, Forehand R, Bau JJ, Fasula A, Long N, & Armistead L (2008). Patterns of sexuality communication between preadolescents and their mothers and fathers. Journal of Child and Family Studies, 17(5), 649–662. doi: 10.1007/s10826-007-9179-5 [DOI] [Google Scholar]
- Yang H, Stanton B, Li X, Cottrel L, Galbraith J, & Kaljee L (2007). Dynamic association between parental monitoring and communication and adolescent risk involvement among African-American adolescents. Journal of the National Medical Association, 99(5), 517–524. [PMC free article] [PubMed] [Google Scholar]
- Young MA, & Vazsonyi AT (2011). Parents, peers, and risky sexual behaviors in rural African American adolescents. The Journal of Genetic Psychology: Research and Theory on Human Development, 172(1), 84–93. doi: 10.1080/00221325.2010.506373 [DOI] [PubMed] [Google Scholar]