

Abstract
Elevated proinflammatory cytokines and decreased antiinflammatory cytokines are important in the context of perinatal health, and immune dysregulation has been found among perinatal women with low socioeconomic status (SES). Data examining psychological factors that may contribute to cytokines in pregnancy are lacking. Of importance, these associations may be most evident among women with low SES. This study examined the moderating role of SES on associations among presence of meaning in life and repetitive negative thinking with cytokine levels among 67 pregnant women. A cumulative SES index was calculated using income, education, perceived social class, and receipt of governmental support. Measures included the Perseverative Thinking Questionnaire, Meaning in Life Questionnaire, and serum interleukin (IL)-6 as well as IL-4. Using PROCESS, moderation analyses showed significant interactions between psychological factors and SES in predicting serum cytokines. In the context of high SES only, greater repetitive negative thinking was associated with higher levels of the proinflammatory cytokine IL-6 (p = 0.056) while greater meaning in life was associated with higher levels of the antiinflammatory cytokine IL-4 (p = 0.02). Findings from this study suggest that the benefits of these psychological factors on cytokine levels may be most readily observable among women with greater economic stability. Identifying psychological factors that positively contribute to biological functioning in women experiencing heightened economic distress will be crucial in addressing SES-related disparities in perinatal health.
Keywords: Socioeconomic status (SES), interleukin(IL)-6, IL-4, repetitive negative thinking, meaning in life, pregnancy
Immune parameters have been shown to play a mediating role in the relationship between socioeconomic status (SES) and physical health outcomes (e.g., Chen & Miller, 2013; Matthews & Gallo, 2011). In the context of pregnancy, immune dysregulation has been associated with poor perinatal outcomes and these adverse outcomes have higher rates in women with low compared to high SES (Blumenshine, Egerter, Barclay, Cubbin, & Braveman, 2010; Coussons-Read et al., 2012; Silva et al., 2008). The Reserve Capacity Model provides a framework for understanding relationships among psychosocial factors, SES, and physical health (Gallo & Matthews, 2003; Matthews, Gallo, & Taylor, 2010). In fact, some data indicate that psychosocial factors may differently relate to immune parameters depending on SES (Gallo, de los Monteros, & Shivpuri, 2009; Matthews et al., 2010). The degree to which these findings generalize to clinically-relevant psychological factors warrants investigation.
Serum cytokines during pregnancy
Inflammation is particularly important for perinatal health. Longitudinal studies have demonstrated that pregnancy is characterized by healthy immune adaptation, including increases in serum levels of proinflammatory cytokines as well as increases in LPS-stimulated production of proinflammatory cytokines by peripheral blood mononuclear cells stimulated ex vivo (Christian & Porter, 2014; Coussons-Read et al., 2012; Gillespie, Porter, & Christian, 2016; Winkler et al., 2002). Despite healthy fluctuation of these cytokine levels in pregnancy, high levels of proinflammatory cytokines have been associated with poor birth and neonatal outcomes (Blair, Porter, Leblebicioglu, & Christian, 2015; Coussons-Read et al., 2012; Sorokin et al., 2010). In addition, low levels of antiinflammatory cytokines have been linked with pregnancy complications and poor birth outcomes (Chatterjee, Chiasson, Bounds, & Mitchell, 2014).
The current investigation focused on the proinflammatory cytokine IL-6 and the antiinflammatory cytokine IL-4. Widely studied in relation to psychosocial factors, IL-6 is responsive to psychosocial stress (Hänsel, Hong, Cámara, & von Känel, 2010; Segerstrom & Miller, 2004) and has been linked with preterm birth (Coussons-Read et al., 2012; Sorokin et al., 2010). In relation to pregnancy, IL-6 has been implicated in the production of prostaglandins which stimulate labor (Chatterjee et al., 2014; Wei, Fraser, & Luo, 2010). While data have largely emphasized the role of IL-6 found in maternal-fetal contexts like amniotic fluid (Wei et al., 2010), human studies have found associations among maternal serum levels of IL-6 and preterm birth (Coussons-Read et al., 2012; Sorokin et al., 2010). Data on antiinflammatory cytokines are less plentiful; however, lower levels of IL-4 have been observed in relation to stress (Hänsel et al., 2010) and associated with miscarriages as well as preeclampsia (Chatterjee et al., 2014). In pregnancy, IL-4 has been shown to play several important roles including promoting the development and function of the placenta as well as inhibiting the effects of proinflammatory cytokines (Chatterjee et al., 2014). Though the mechanisms require further testing, suppression of inflammatory responses is posited to be one pathway by which IL-4 is relevant for pregnancy complications and adverse birth outcomes (Chatterjee et al., 2014).
SES and serum cytokine levels
Despite important clinical implications, the relationship between SES and serum cytokine levels during pregnancy remains understudied. A substantial literature in non-pregnant adults has shown that low SES is associated with elevated proinflammatory cytokines, particularly IL-6 (Friedman & Herd, 2010; Gruenewald, Cohen, Matthews, Tracy, & Seeman, 2009; Koster et al., 2006; Loucks et al., 2010). Although limited, studies have examined the relationship between SES and biological functioning during the perinatal period. Data indicate that low SES or social resources are associated with hypothalamic-pituitary-adrenal (HPA) axis dysregulation (Bublitz, Vergara-Lopez, Treter, & Stroud, 2016; Jewell, Luecken, Gress-Smith, Crnic, & Gonzales, 2015; Thayer & Kuzawa, 2014), the system which modulates inflammatory responses (Silverman, Pearce, & Miller, 2003). Consistent with immune dysregulation, one would expect that low SES would be associated with elevated levels of proinflammatory cytokines and low levels of antiinflammatory cytokines in pregnancy.
SES, psychological factors, and serum cytokine levels
The Reserve Capacity Model provides a useful framework when considering associations among psychological factors, SES, and cytokine levels (Gallo & Matthews, 2003; Matthews et al., 2010). According to the model, individuals with low SES, compared to those with high SES, have fewer resilient resources available to use in response to stressful events. The model posits that individuals with low SES encounter a greater quantity of stressful events that require the use of resources, with few opportunities for these resources to be developed or replenished (see Gallo & Matthews, 2003 for a review of studies supporting these pathways). These psychosocial resources are often contextualized as (a) pathways by which people with low versus high SES have exacerbated health outcomes (i.e., mediate) or (b) buffers in the link between low SES and health (i.e., moderate; Gallo & Matthews, 2003; Matthews et al., 2010). It is also possible to consider SES as a moderator. In fact, data indicate that associations among psychosocial resources and biological functioning may be most evident among people with low versus high SES (Morozink, Friedman, Coe, & Ryff, 2010). The focus of the current investigation is on moderation, which will be described in greater detail below.
Consistent with the Reserve Capacity Model, greater resilient resources have buffered the effects of low SES on adverse physical health outcomes, including measures of self-rated health, functional limitations, and cardiovascular responses to acute stressors (for a review, see Gallo et al., 2009). Of note, the benefits of resilient resources may vary by SES. For example, Chen (2007) conducted an experimental study with 115 adolescents and found that an intervention of providing resources, as defined by informational support and perceived control over the task, buffered the effects of laboratory-induced stress on physiological responses among adolescents with low SES. Physiological responses did not differ in the intervention and no intervention groups for adolescents with high SES (Chen, 2007). Notably, existing studies examining psychosocial factors and health have largely defined these constructs using dispositional, self, ego, and interpersonal constructs; world views and cognitive factors have been recognized as important but received less attention (Dunkel Schetter & Dolbier, 2011). Of clinical relevance, these constructs are particularly modifiable in the context of therapeutic interventions and may be informative for future studies assessing SES-related disparities in perinatal health.
One relevant world view indicator that is reflective of a psychological resource is meaning in life (Dunkel Schetter & Dolbier, 2011). A growing body of literature in non-pregnant adults has examined well-being indicators in relation to biological functioning (e.g., Ryff, 2014), with studies showing that greater eudaimonic well-being, including more purpose in life, is associated with lower levels of soluble IL-6 receptor as well as higher levels of interferon gamma (IFN-γ) and IL-10 (Hayney et al., 2003; Ryff, Singer, & Love, 2004). In line with the Reserve Capacity Model, some additional data support the hypothesis that the link between well-being and serum cytokine levels may be particularly meaningful among individuals with low SES. More specifically, in a study with 1,028 adults, greater purpose in life was associated with lower serum IL-6 levels only among individuals with lower education (Morozink et al., 2010).
Psychological risk factors may also contribute to cytokine levels. One relevant cognitive risk factor is repetitive negative thinking: a maladaptive thought pattern characterized by repetition, intrusiveness, and unproductiveness, encapsulating both rumination and worry (Ehring & Watkins, 2008; Ehring et al., 2011; McEvoy & Brans, 2012; McEvoy, Watson, Watkins, & Nathan, 2013; Watkins, 2008). Literature demonstrates that engagement in negative repetitive thought processes, such as rumination, is associated with neuroendocrine and immune dysregulation in non-pregnant adults, including elevated cortisol and C-reactive protein (CRP) levels as well as lower antibody responses (Segerstrom, Schipper, & Greenberg, 2008; Zoccola & Dickerson, 2012; Zoccola, Figueroa, Rabideau, Woody, & Benencia, 2014). Some data also indicate that repetitive negative thinking is important in the context of financial stress. In a sample of cancer caregivers, repetitive negative thinking served as one pathway by which financial stress was associated with depressive symptoms (Mitchell & Pössel, 2017). Collectively, these data with non-pregnant adults indicate that presence of meaning in life and repetitive negative thinking are psychological factors which may contribute to cytokine levels in pregnant women. Importantly, though, this relationship may be most evident among women experiencing economic distress.
The current study
The current study examined the moderating role of SES on associations among presence of meaning in life and repetitive negative thinking with serum cytokine levels in 67 pregnant women. First, we determined whether we could replicate associations between SES and serum cytokine levels in pregnant women. It was hypothesized that SES would be negatively associated with serum levels of proinflammatory cytokine IL-6 and positively associated with serum levels of the antiinflammatory cytokine IL-4. Second, we examined associations among meaning in life, repetitive negative thinking, and serum cytokine levels. It was expected that meaning in life would be negatively related to serum IL-6 and positively related to serum IL-4, whereas repetitive negative thinking would demonstrate contrasting associations. Finally, we examined interactions among psychological factors and SES in relation to serum cytokine levels. Consistent with the Reserve Capacity Model, it was expected that associations between these two psychological factors with serum cytokines would be most evident among women with low SES (see Figure 1).
Figure 1.
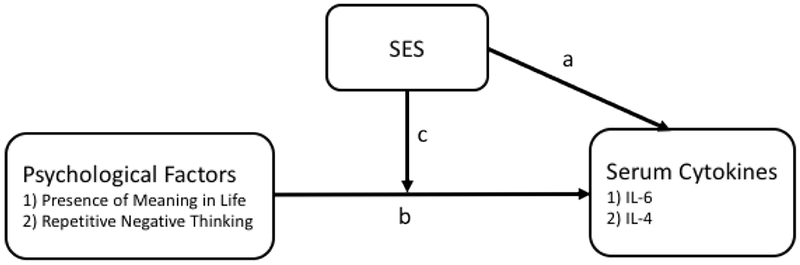
Proposed hypotheses in the current study.
SES = socioeconomic status; IL = interleukin.
Method
Study design.
The current study is a cross-sectional examination of psychological factors, SES, and serum cytokine levels among pregnant women who were part of a larger prospective study (Christian et al., 2017).
Participants.
Participants consisted of 69 pregnant women. Exclusion criteria included major immune conditions, such as cancer, greater than 30 weeks gestation, and reported weight and height consistent with a pre-pregnancy body mass index (BMI) < 18.5 or > 50. Women reporting acute illness, such as cold- or flu-like symptoms, or antibiotic use within seven days of a study visit were rescheduled. Two participants did not complete the second study visit and, therefore, did not have data on psychological factors of focus; thus, they were removed prior to analyses, resulting in a final sample of 67.
Study procedures.
Faculty, staff, and students at the Ohio State University (OSU) and OSU Wexner Medical Center (OSUWMC) were recruited for this study via advertisements placed in online campus newsletters. Patients from the OSUWMC Prenatal Clinic and women from the surrounding community of Columbus, Ohio were recruited in person at medical appointments and via advertisements displayed at medical offices and online. For the current study, data from two study visits were used. At the first study visit, research assistants reviewed study information and documentation with participants. Written informed consent and Health Insurance Portability and Accountability Act (HIPAA) authorizations were obtained at this time. Research nurses then collected blood samples into vacutainer tubes while participants were in a seated position and subsequently administered an influenza vaccination. Finally, participants completed items assessing demographics, SES, and health behaviors on paper. After 30 days, participants returned for a second study visit where they completed questionnaires assessing psychological factors on paper. Participants received modest compensation at the end of study visits. The study was approved by the OSU Biomedical Institutional Review Board.
Measures
Demographics.
Age, race, marital status, and number of births (parity) were collected by self-report at the first study visit. Pre-pregnancy BMI (kg/m2) was calculated utilizing self-reported pre-pregnancy weight and measured height at the first visit. Participants expected due date was obtained per medical record review. Gestational age at study visit was calculated by subtracting 280 days from the days left until their due date (date difference between expected due date and study visit date). Delivery routes were noted per medical record review. Presence or absence of pregnancy complications (i.e., gestational hypertension and preeclampsia) was obtained per medical record review and coded as a yes/no variable. Birth weight was obtained per medical record review; under 2,500g was classified as low birth weight. Gestational age at delivery was calculated by subtracting 280 days from the number of days the infant was delivered prior to the expected due date (date difference between expected due date and actual due date); under 37 weeks was classified as preterm birth. Singleton and multifetal pregnancies were determined per medical record review. Birth outcome data were unavailable for one woman due to delivery at an unexpected hospital.
Health behaviors.
Smoking, exercise, and prenatal vitamin use were assessed via self-report at the time of the first study visit. Smoking was defined as current or not current. Exercise was operationalized as the frequency with which a participant engaged in a vigorous activity long enough to build up a sweat. Prenatal vitamin use was assessed as never, 1-3 days per week, 4-6 days per week, or 7 days per week since pregnancy was known.
SES.
Annual household income, education, perceived social class, and receipt of women, infants, and children (WIC) support were assessed via self-report at the time of the first study visit. Annual household income was defined as less than $15,000, $15,000-$29,999, $30,000-$49,999, $50,000-$74,999, $75,000-$99,999, or $100,000 and above; highest completed education was captured as less than 7th grade, junior high, some high school, high school graduate, some college (2 year college or technical school), some college (4 year college), Associate’s or technical degree (2 year degree), Bachelor’s degree (4 year college), or some graduate school or higher. Participants were asked to indicate their current perceived social class from a classification system operationalized as lower class, working class, lower middle class, upper middle class, and higher class. Receipt of women, infants, and children (WIC) support was defined as yes/no. A cumulative SES index was calculated by summing the number of instances participants reported above the median on annual household income, education, and perceived social class as well as the absence of WIC support. This cumulative SES index was calculated to reflect all available SES data; this allowed for consideration of multiple facets of SES while performing the least number of statistical tests to assess study hypotheses. A cumulative SES index has been used in prior research (e.g., Beach, Dogan, Brody, & Philibert, 2014).
Presence of meaning in life.
The 10-item Meaning in Life (MLQ) scale was used to assess meaning in life at the second study visit (Steger, Frazier, Oishi, & Kaler, 2006). Each item is responded to on a 7-point Likert scale, ranging from 1 (absolutely untrue) to 7 (absolutely true). Items were summed to calculate two subscale scores: search for meaning in life and presence of meaning in life. In the current study, hypotheses and analyses focused on the presence of meaning in life. The MLQ has shown strong reliability and validity in adult samples (Steger et al., 2006). In this study sample, internal consistency for the presence of meaning in life subscale was α = .88.
Repetitive negative thinking.
The 15-item Perseverative Thinking Questionnaire (PTQ) was used to assess repetitive negative thinking at the second study visit (Ehring et al., 2011). Participants responded to each item utilizing a 5-point Likert scale, ranging from 0 (never) to 4 (almost always). Items were summed to calculate three subscale scores (i.e., core characteristics of repetitive negative thinking, unproductiveness of repetitive negative thinking, repetitive negative thinking capturing mental capacity) and a total score; the total score was used in the current study. The PTQ has demonstrated strong reliability in adult samples (Ehring et al., 2011). In this study sample, internal consistency for the PTQ total score was α = .96.
Blood parameters.
Samples were immediately centrifuged, aliquoted, and placed in −80°C freezer storage until analysis. Serum levels of IL-6 and IL-4 were assayed using multiplex V-Plex kits from Meso Scale Discovery (Meso Scale Discovery, 1601 Research Boulevard, Rockville, MD). The limit of detection was 0.06 pg/mL and 0.02 pg/mL for IL-6 and IL-4, respectively. Inter- and intra-assays coefficients of variation were 6.4% and 4.0% for IL-6 and 9.7% and 5.8% for IL-4. Cytokine values determined to be Not a Number (NaN), otherwise known as below fit curve range, on both runs by the MSD software were excluded from analyses (n = 7 for IL-6; n = 1 for IL-4); values that fit the curve but were below detection range were retained for analyses at the concentration reported by the software program (n = 37 for IL-4).
Statistical analyses.
All analyses were conducted in SPSS 24.0. Participants with NaN inflammatory values (n = 7 for IL-6; n = 1 for IL-4) or missing data (n = 1 for WIC status and n = 1 for medical conditions) were excluded from respective analyses. Serum IL-6 and IL-4 were log-transformed (base 10) to fit the normality assumption. Descriptive statistics were calculated for all participants. Differences on serum cytokine levels by pregnancy complications and adverse birth outcomes were examined by independent t-tests. Associations among SES indicators, psychological factors, and serum cytokine levels were conducted using Pearson’s and Spearman’s correlations. To examine interactions between psychological factors and SES on serum cytokine levels, moderation analyses were conducted using PROCESS (Hayes, 2013). Interactions were conducted with both cumulative SES and psychological factors as moderators to delineate relationships. To determine the point at which the moderators affected the direct relationship (e.g., psychological factors and serum cytokine levels or SES and serum cytokine levels), the increasingly popular Johnson-Neyman Technique was used unless otherwise specified (Bauer & Curran, 2005; Hayes, 2013). This approach identifies the exact value(s) of the moderator at which the conditional effect takes place (Hayes, 2013). All moderation analyses were adjusted for race, BMI, exercise, gestational age at visit, and medical conditions (i.e., presence or absence of preeclampsia and gestational hypertension), per findings in the literature (Chatterjee et al., 2014; Christian, Glaser, Porter, & Iams, 2013; Christian & Porter, 2014; Gillespie et al., 2016). Of note, while demographic information and immune data were captured at the first study visit, stable psychological factors (i.e., presence of meaning in life and repetitive negative thinking) were assessed 30 days later at the second study visit. Both of these psychological factors have been shown to have good stability over 30 days (Ehring et al., 2011; Steger et al., 2006).
Results
Sample characteristics.
Demographic, pregnancy, and health characteristics are detailed in Table 1 and key study variables are described in Table 2. Women were between six and 29 weeks gestation at the time of the study visit (M = 16.4, SD = 6.4). On average, women were 29.8 years old (SD = 5.3); 76.1% were White and 67.2% were married. In terms of cumulative SES, values were determined by summing the number of instances participants reported being above the median on income (i.e., $50,000 or higher), education (i.e., bachelor’s degree or higher), and perceived SES (i.e., lower middle class or higher) as well as the absence of WIC support, resulting in a range of 0 to 4: n = 10 at 0 (15.2%), n = 13 at 1 (19.7%), n = 4 at 2 (6.1%), n = 7 at 3 (10.6%), and n = 32 at 4 (48.5%) (Table 1).
Table 1.
Demographic, pregnancy, and health characteristics
| Age | 29.8 (5.3) |
| Race | |
| White1 | 51 (76.1%) |
| Black | 13 (19.4%) |
| Asian | 1 (1.5%) |
| Biracial/Multiracial | 2 (3.0%) |
| Marital Status | |
| Married | 45 (67.2%) |
| In a Relationship | 19 (28.4%) |
| Single | 3 (4.5%) |
| Parity (# of prev. births) | |
| 0 | 23 (34.3%) |
| 1 | 26 (44.8%) |
| 2 or more | 9 (15.5%) |
| Smoking Status | |
| Current | 7 (10.4%) |
| Not Current | 60 (89.6%) |
| Exercise | |
| Less than once per month | 14 (20.9%) |
| Once per month | 9 (13.4%) |
| 2-3 times per month | 10 (14.9%) |
| Once per week | 14 (20.9%) |
| More than once per week | 20 (29.9%) |
| Prenatal Vitamin Use | |
| Never | 4 (6.0%) |
| Some days (1-3 times per week) | 4 (6.0%) |
| Most days (4-6 times per week) | 11 (16.4%) |
| Every day (7 times per week) | 48 (71.6%) |
| BMI | 27.8 (7.9) |
| GA at Study Visit | 16.4 (6.4) |
| Delivery Route | |
| Spontaneous vaginal delivery | 38 (57.6%) |
| Obstetrical forceps delivery | 3 (4.5%) |
| Caesarean delivery | 25 (37.9%) |
| Multifetal Gestation | |
| Yes | 2 (3.0%) |
| No | 65 (97.0%) |
| Pregnancy Complications2 | |
| Yes | 7 (10.6%) |
| No | 59 (89.4%) |
| Adverse Birth Outcomes2 | |
| Yes | 9 (13.6%) |
| No | 57 (86.4%) |
Note. Data are reported in Mean (SD) or n (%).
Two white women endorsed Hispanic ethnicity.
Pregnancy complications include gestational hypertension and preeclampsia. Adverse birth outcomes include preterm birth and low birth weight. One woman was missing birth outcome data.
BMI = pre-pregnancy body mass index; GA = gestational age.
Table 2.
Key study variables
| Income | |
| Less than $15,000 | 11 (16.4%) |
| $15,000-$29,999 | 12 (17.9%) |
| $30,000-$49,999 | 7 (10.4%) |
| $50,000-$74,999 | 7 (10.4%) |
| $75,000-$99,999 | 12 (17.9%) |
| $100,000 and above | 18 (26.9%) |
| Education | |
| Less than 7th Grade | 0 (0%) |
| Junior High | 1 (1.5%) |
| Some High School | 5 (7.6%) |
| High School Graduate | 11 (16.7%) |
| Some College (2 year college/technical school) | 8 (12.1%) |
| Some College (4 year college) | 4 (6.1%) |
| Associate’s or Technical Degree | 2 (3.0%) |
| Bachelor’s Degree | 12 (18.2%) |
| Some Graduate School or More | 23 (34.8%) |
| Perceived SES | |
| Lower Class | 9 (13.4%) |
| Working Class | 11 (16.4%) |
| Lower Middle Class | 28 (41.8%) |
| Upper Middle Class | 19 (28.4%) |
| Higher Class | 0 (0%) |
| WIC Status1 | |
| Yes | 15 (22.7%) |
| No | 51 (77.3%) |
| Cumulative SES2 | |
| 0 | 10 (15.2%) |
| 1 | 13 (19.7%) |
| 2 | 4 (6.1%) |
| 3 | 7 (10.6%) |
| 4 | 32 (48.5%) |
| Repetitive Negative Thinking | 16.0 (11.5) |
| Presence of Meaning in Life | 28.8 (4.9) |
| Interleukin(IL)-63 | |
| Non-transformed | 0.565 (0.40) |
| Transformed | −0.379 (0.41) |
| Interleukin(IL)-43 | |
| Non-transformed | 0.015 (0.01) |
| Transformed | −1.94 (0.35) |
Note. Data are reported in Mean (SD) or n (%).
One woman was missing data regarding WIC status.
A cumulative SES index was calculated by summing the number of instances a participant reported above the median on income, education, and perceived social class as well as the absence of WIC support. One woman was missing data on cumulative SES.
Cytokine values determined to be Not a Number (NaN), otherwise known as below fit curve range, on both runs by the MSD software were excluded (n = 7 for IL-6; n = 1 for IL-4).
WIC = Women, Infants, and Children (WIC); SES = socioeconomic status.
In terms of pregnancy characteristics, three delivery routes were recorded in this sample: spontaneous vaginal delivery (n = 38, 56.7%), obstetrical forceps delivery (n = 3, 4.5%), and caesarean delivery (n = 25, 37.9%). Two women (3%) had multifetal gestation. Pregnancy complications of gestational hypertension or preeclampsia affected seven women (10.6%). Lower levels of IL-4 were found among the seven women who had gestational hypertension or preeclampsia (M = −2.28, SD = 0.46) versus those who did not have one of these conditions (M = −1.90, SD = 0.32) (t(63) = 2.79, p < 0.01). No significant differences emerged between women with pregnancy complications (M = −0.33, SD = 0.31) and those without (M = −0.39, SD = 0.43) on IL-6 levels (t(58) = −0.34, p = 0.73). Adverse birth outcomes of preterm birth or low birth weight occurred in nine women (13.6%). No significant differences were found among the nine women with adverse birth outcomes (M = −2.07, SD = 0.48) compared to those without (M = −1.92, SD = 0.33) on IL-4 levels (t(63) = 1.17, p = 0.25). Two women with adverse birth outcomes were excluded from analyses with IL-6 because of NaN values. No significant differences were found among the remaining seven women with adverse birth outcomes (M = −0.32, SD = 0.29) compared to those without (M = −0.39, SD = 0.43) on IL-6 levels (t(58) = −0.37, p = 0.71).
Relationships among key variables.
Correlations among distinct SES indicators, presence of meaning in life, repetitive negative thinking, serum cytokine levels, and other key study variables are detailed in Table 3. Although associations were in the expected direction, unexpectedly, no statistically significant relationships emerged between income (r = −0.18, p = 0.16), education (r = −0.14, p = 0.29), perceived SES (r = −0.23, p = 0.08), and WIC status (r = 0.11, p = 0.41) with IL-6. These findings were consistent with IL-4 as well: income (r = 0.21, p = 0.10), education (r = 0.15, p = 0.25), perceived SES (r = 0.16, p = 0.20), and WIC status (r = −0.04, p = 0.74). Consistent with hypotheses, presence of meaning in life was negatively associated with IL-6 (r = −0.26, p = 0.045) and a positive trend was observed in relation to IL-4 (r = 0.22, p = 0.07). As predicted, repetitive negative thinking was negatively associated with IL-4 (r = −0.24, p = 0.05); however, it was not linked with IL-6 (r = 0.07, p = 0.62).
Table 3.
Correlations among key study variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Income | --- | |||||||||||||
| 2 Education | 0.81*** | --- | ||||||||||||
| 3 Perceived SES | 0.75*** | 0.66*** | --- | |||||||||||
| 4 WIC Status | −0.62*** | −0.45*** | −0.45*** | --- | ||||||||||
| 5 Cumulative SES | 0.92*** | 0.82*** | 0.80*** | −0.74*** | --- | |||||||||
| 6 PTQ | −0.04 | 0.03 | 0.03 | −0.01 | −0.001 | --- | ||||||||
| 7 MLQ-P | 0.10 | 0.13 | 0.26* | −0.02 | 0.13 | −0.28* | --- | |||||||
| 8 BMI | −0.14 | −0.14 | −0.12 | −0.02 | −0.07 | 0.05 | 0.01 | --- | ||||||
| 9 Race | −0.52*** | −0.45*** | −0.41** | 0.40** | −0.53*** | −0.13 | 0.00 | 0.11 | --- | |||||
| 10 Exercise | 0.10 | 0.13 | 0.12 | −0.01 | 0.08 | −0.12 | 0.23 | −0.07 | −0.03 | --- | ||||
| 11 Days Pregnant | −0.03 | −0.11 | −0.13 | 0.04 | −0.12 | 0.04 | −0.14 | −0.09 | 0.07 | −0.11 | --- | |||
| 12 Pregnancy Complications | −0.04 | −0.13 | −0.02 | −0.05 | 0.07 | 0.22 | −0.15 | 0.07 | 0.04 | −0.03 | 0.01 | --- | ||
| 13 Adverse Birth Outcomes | −0.20 | −0.03 | −0,14 | 0.10 | −0.09 | −0.08 | 0.17 | 0.10 | 0.19 | 0.09 | −0.07 | 0.29* | --- | |
| 14 IL-6 | −0.18 | −0.14 | −0.23 | 0.11 | −0.18 | 0.07 | −0.26* | 0.44*** | 0.26* | −0.11 | 0.00 | 0.01 | 0.04 | --- |
| 15 IL-4 | 0.21 | 0.15 | 0.16 | −0.04 | 0.18 | −0.24* | 0.22 | −0.12 | −0.13 | 0.05 | −0.02 | −0.26* | −0.09 | −0.12 |
Note. Spearman’s correlations were used when WIC status, race, pregnancy complications, and adverse birth outcomes were included. WIC = Women, Infants, and Children (WIC); SES = socioeconomic status; PTQ = Negative Repetitive Thinking; MLQ-P = Presence of Meaning in Life; IL = interleukin. WIC status: 0 = not enrolled, 1 = enrolled; race: 0 = white, 1 = person of color; pregnancy complications: 0 = not present, 1 = present; adverse birth outcomes: 0 = not present, 1 = present; all other variables are coded as labeled in Table 1 or 2, in increasing order.
p ≤ 0.05
p < 0.001.
SES, presence of meaning in life, and serum cytokine levels.
Using the cumulative SES index, the interactions between presence of meaning in life and SES on serum cytokine levels were examined after controlling for race, BMI, exercise, gestational age at visit, and medical conditions. Consistent with hypotheses, the overall model with IL-4 was significant (F(8, 55) = 3.07, p < 0.01, R2 = 0.31), with a significant interaction term between presence of meaning in life and cumulative SES in predicting IL-4 (b = 0.01, t(55) = 2.22, p = 0.03, 95% Confidence Interval: [0.001, 0.024], ΔR2 = 0.06, ΔF = 4.94). Unexpectedly, follow-up analyses using the Johnson-Neyman Technique indicated that greater presence of meaning in life was associated with higher IL-4 levels only among women of high SES (significant at a cumulative SES index of = 3, b = 0.02, t(55) = 2.41, p = 0.02, 95% Confidence Interval: [0.004, 0.041]) (Figures 2 and 3).1 To fully delineate this relationship, this interaction was also examined using presence of meaning in life as a moderator. Results using the Johnson-Neyman Technique demonstrated that the greater SES was associated with higher IL-4 levels among women scoring ≥33 on the presence subscale of the Meaning in Life Questionnaire (b = 0.08, t(55) = 2.00, p = 0.05, 95% Confidence Interval: [0.000, 0.159]). No significant interaction was found between presence of meaning in life and SES in the model with IL-6 (b = 0.003, t(50) = 0.33, p = 0.75, 95% Confidence Interval: [−0.013, 0.018]).
Figure 2.
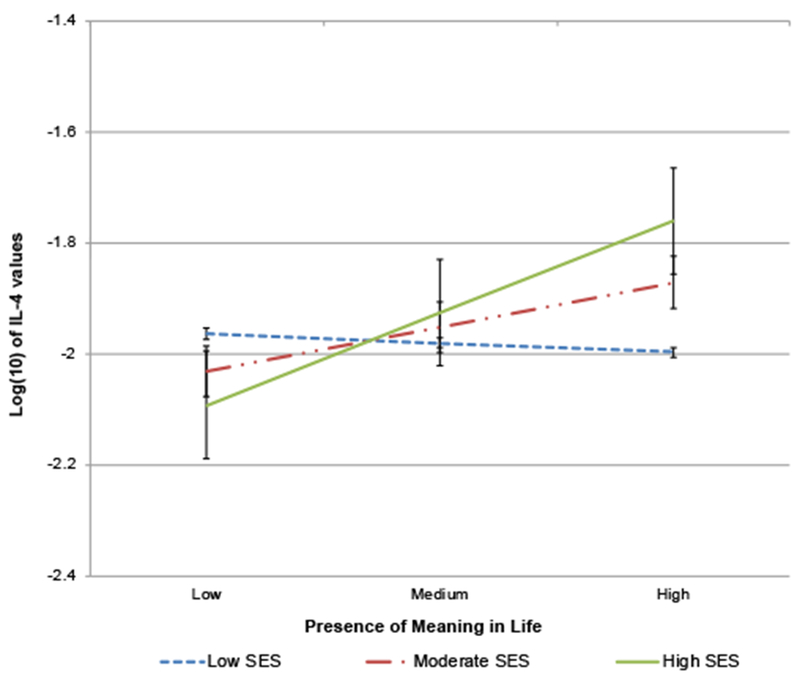
PROCESS results regarding interaction between presence of meaning in life and cumulative SES on IL-4 levels.
Low, moderate, and high SES lines are reflective of approximate cumulative SES values of 1, 2, and 4. Errors bars at ± 1 SE. SES = socioeconomic status; IL-4 = interleukin-4.
Figure 3.

PROCESS results regarding interaction between presence of meaning in life and cumulative SES on IL-4 levels.
SES = socioeconomic status; IL-4 = interleukin-4; CI = Confidence Interval.
SES, repetitive negative thinking, and serum cytokine levels.
Similarly, the cumulative SES index was used to assess the interactions between repetitive negative thinking and SES on serum cytokine levels after adjustment for race, BMI, exercise, gestational age at visit, and medical conditions. As expected, the overall model with IL-6 was significant (F(8,50) = 3.08, p < 0.01, R2 = 0.33); a significant interaction emerged between repetitive negative thinking and cumulative SES in predicting IL-6 (b = 0.01, t(50) = 2.24, p = 0.03, 95% Confidence Interval: [0.001, 0.012], ΔR2 = 0.07, ΔF = 5.00). Follow-up analyses demonstrated that, in contrast to hypotheses, greater repetitive negative thinking was associated with high levels of IL-6 only among women of high SES (trend observed at a maximum cumulative SES index of 4, b = 0.01, t(50) = 1.95, p = 0.056, 95% Confidence Interval: [−0.0004, 0.028]) (Figures 4 and 5).1 To fully delineate this relationship, this interaction was also examined with repetitive negative thinking as a moderator. Follow-up analyses conducted using the Johnson-Neyman Technique demonstrated that greater SES was associated with lower levels of IL-6 among women scoring ≤3 on the Perseverative Thinking Questionnaire (b = −0.097, t(50) = −2.01, p = 0.05, 95% Confidence Interval: [−0.195, 0.000]). No significant interaction was found between repetitive negative thinking and SES in the model with IL-4 (b = −0.002, t(55) = −0.95, p = 0.35, 95% Confidence Interval: [−0.007, 0.002]).
Figure 4.
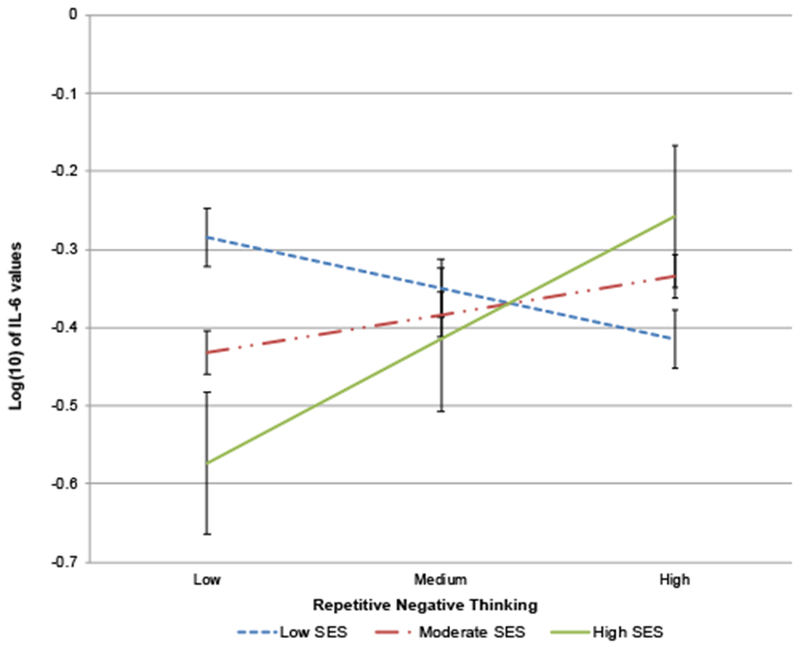
PROCESS results regarding interaction between repetitive negative thinking and cumulative SES on IL-6 levels.
Low, moderate, and high SES lines are reflective of approximate cumulative SES values of 1, 2, and 4. Errors bars at ± 1 SE. SES = socioeconomic status; IL-6 = interleukin-6.
Figure 5.
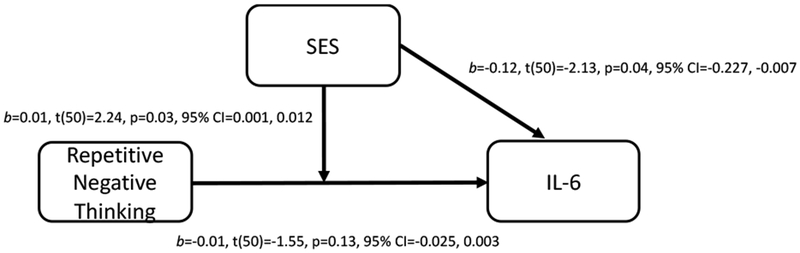
PROCESS results regarding interaction between repetitive negative thinking and cumulative SES on IL-6 levels.
SES = socioeconomic status; IL-6 = interleukin-6; CI = Confidence Interval.
Discussion
The current study demonstrated important interactions between presence of meaning in life and repetitive negative thinking with SES on serum cytokine levels during pregnancy. Of note, direct associations did not emerge among SES indicators with pro and antiinflammatory cytokines. However, the presence of meaning in life and repetitive negative thinking were directly related to serum cytokine levels. Specifically, lower meaning in life was associated with greater serum IL-6 levels while greater repetitive negative thinking was related to lower serum IL-4 levels. This is consistent with prior evidence showing lower eudaimonic well-being and greater rumination, a process embedded in repetitive negative thinking, are associated with neuroendocrine and immune dysregulation in non-pregnant adults (Hayney et al., 2003; Ryff et al., 2004; Segerstrom et al., 2008; Zoccola & Dickerson, 2012; Zoccola et al., 2014). Inconsistent with the Reserve Capacity Model, while greater meaning in life was associated with higher serum IL-4 levels, this effect only emerged among women with high, but not low, SES. Similarly, greater repetitive negative thinking was associated with higher levels of serum IL-6 but only among women with high compared to low SES.
Study findings support the notion that world views and cognitive factors interact with SES to contribute to serum cytokine levels. Prior studies have largely focused on dispositional characteristics, emotional states (e.g., depression, anxiety, and hostility), health behaviors, or social support in models with SES and health in non-pregnant adults (Chen & Miller, 2013; Matthews & Gallo, 2011; Matthews et al., 2010). As described earlier, in a study of 1,028 non-pregnant adults, greater well-being, including more purpose in life, was associated with lower IL-6 levels among individuals with lower versus higher education levels (Morozink et al., 2010). However, in the current study, data suggest that associations among psychological factors and cytokine levels are more readily observable in the context of high compared to low SES.
Psychological factors and cytokine levels in women with low SES
Unmeasured constructs and study characteristics could explain the unexpected null findings in women with low SES. Other unassessed contributors to immune parameters associated with the hardships of low SES, such as those affecting basic needs (e.g., food and housing insecurity), health care access as well as services (e.g., illness frequency), and a sense of safety, may have played more meaningful roles than world views and cognitive factors. Indeed, data have shown that food insecurity and poor housing quality are linked with increased levels of CRP (Gowda, Hadley, & Aiello, 2012; Schmeer & Yoon, 2016). Although there is a lack of studies examining the distinct and combined contributions of physiological, safety, and psychological needs on immune parameters, it seems possible that, if not met, basic needs may play a more impactful role on an individual’s immune functioning.
In addition, women in this sample were predominately White. It is possible that biological dysregulation is exacerbated during pregnancy in the case of intersecting oppressed identities, such as income and racial/ethnicity, due to the unique experience of various stressors (e.g., discrimination). This is in line with theoretical models, including an extension of the Reserve Capacity Model, which outline how income and race/ethnicity interact to reflect “cumulative vulnerabilities” and result in poorer health outcomes (Myers, 2009). People of color are disproportionately represented in lower income brackets (Burton, Bonilla-Silva, Ray, Buckelew, & Hordge Freeman, 2010), and data have shown that African American women exhibit heighted inflammatory markers during pregnancy compared to White women (e.g., Gillespie et al., 2016). Thus, it is possible that interactions between psychological factors and SES may differ in samples that are more racially and ethnically diverse.
Nevertheless, consistent with the Reserve Capacity Model, literature has found that the presence of psychosocial resources, such as social support, meaning in life, perceived control, and maternal warmth during childhood, provides protective effects of low SES on biological functioning as well as physical health outcomes in children and adults (Chen & Miller, 2013; Gallo et al., 2009; Gallo & Matthews, 2003; Matthews et al., 2010). Thus, it is possible that associations among psychological factors and immune parameters may emerge in a larger cohort of women with lower SES. Given the SES-related disparities in perinatal health outcomes, studies examining clinically-relevant processes that may contribute to serum cytokine levels among pregnant women with low SES are warranted.
Psychological factors and cytokine levels in women with high SES
In the current study, greater engagement in repetitive negative thinking and a higher presence of meaning in life contributed to cytokine levels in women with high SES. Though literature primarily emphasizes the role of psychosocial resources on health in the context of low SES (Gallo et al., 2009; Gallo & Matthews, 2003; Matthews et al., 2010), there is no reason to suspect that these associations could not emerge in women with high SES. Further, these findings suggest that repetitive negative thinking and meaning in life may be worthy of investigation in future intervention studies.
Importantly, repetitive negative thinking and well-being play important roles in the context of psychological treatment. Repetitive negative thinking has been posited to serve as a mechanism by which mindfulness-based and cognitive therapies improve mental and physical health outcomes (Gu, Strauss, Bond, & Cavanagh, 2015; Keng, Smoski, & Robins, 2011). This assertion has been supported with data demonstrating that reductions in repetitive negative thinking result in enhanced mood (McEvoy, Erceg-Hurn, Anderson, Campbell, & Nathan, 2015). In addition, changes in well-being, including increased meaning in life, are often observed in psychotherapy (for a meta-analysis, see Weiss, Westerhof, & Bohlmeijer, 2016). Although a growing body of literature supports the effects of psychotherapeutic treatments on biological functioning (Black & Slavich, 2016; Bower & Irwin, 2016; Morgan, Irwin, Chung, & Wang, 2014), including neuroendocrine and immune dysregulation, studies examining the psychological mechanisms involved in these changes are lacking. Beyond direct effects of these psychological factors on the HPA axis (e.g., Zoccola & Dickerson, 2012), it is likely that they contribute to changes in biological functioning via changes in psychological distress (e.g., depressive symptoms) and health behaviors (e.g., sleep). Identifying key targets of psychological intervention and the pathways by which they can improve mental as well as physical functioning in perinatal women will be fruitful in approaching treatment from a precision medicine landscape.
Limitations
The current study has limitations. First, although more than 40% of women in this sample self-identified as lower middle class and/or reported an income below the median U.S. household income, according to the United States Census Bureau (Proctor, Semega, & Kollar, 2016), representation of women with lower SES was limited. A large body of literature with non-pregnant adults supports an association between SES and cytokines (Friedman & Herd, 2010; Gruenewald et al., 2009; Koster et al., 2006; Loucks et al., 2010). Importantly, other data have not observed differences between pregnant women with low versus high SES on proinflammatory cytokine levels or ratios (Corwin et al., 2013). Thus, it is possible that healthy immune adaptation during pregnancy may obfuscate relationships found among SES and cytokines in non-pregnant samples. Alternatively, these associations may emerge in a larger cohort or one with greater variability in all SES indicators, including education. Second, while neither the repetitive negative thinking measure nor the presence of meaning in life subscale have cut-off values, the averages observed in this sample are reflective of relatively low risk (i.e., on a scale of 0-60, mean PTQ is 16; on a scale of 5-35, mean MLQ-P is 29). Interactions may differ in samples with wider variability in these measures. Additionally, the psychological measures were administered 30 days after the demographic information and immune data were collected. While this temporal consideration could have affected the relationships reported, it is worth noting that both psychological measures have shown good test-retest reliability over 30 days (Ehring et al., 2011; Steger et al., 2006). Third and finally, the null findings observed could be a function of low power. Studies have shown small to medium effect sizes in direct associations and moderation models with psychosocial resources, SES, and health outcomes (e.g., Chen, 2007; Friedman & Herd, 2010; Morozink et al., 2010). This study was powered to detect medium to large effect sizes, and future studies should consider increasing sample sizes to detect smaller effects.
Future research
A cumulative SES index was used in the current study. This approach allowed for consideration of multiple facets of SES (e.g., income, perceived SES) while conducting the least number of statistical tests to assess study hypotheses. Studies indicate that SES indicators, including income, education, and perceived SES, may have differing and/or unique effects on health outcomes (Braveman et al., 2005; Tang, Rashid, Godley, & Ghali, 2016). Secondary analyses of the current study data indicate that the significant model with repetitive negative thinking and serum IL-6 was driven by income and education. The significant model with presence of meaning in life and serum IL-4 was largely driven by income, education, and WIC status (data not shown). Although a multitude of factors may contribute to the selection of which SES variables are included in a study, assessing the impact this decision may have on relationships with health outcomes will be important for future research.
In addition, the current data focused on the proinflammatory cytokine IL-6 and anti-inflammatory cytokine IL-4 given their relationship to psychosocial stress and relevance for pregnancy (Chatterjee et al., 2014; Coussons-Read et al., 2012; Hänsel et al., 2010; Segerstrom et al., 2004). It may be useful to examine other cytokines in future studies. However, it is worth noting that secondary models conducted with TNF-α, IL-8, and IL-10 demonstrated no meaningful patterns (data not shown). While these findings could reflect the specific functions of cytokines IL-6 and IL-4, replication of this work is needed to make such conclusions, as cytokines are both pleiotropic (exerting multiple actions) and redundant (showing overlapping actions).
Conclusion
In sum, this study provides novel data on the roles of the presence of meaning in life and repetitive negative thinking on serum cytokine levels in pregnant women. These findings demonstrated that the association between psychological factors and serum cytokine levels emerged among women with high, but not low SES. In other words, psychological factors were not associated with serum IL-6 or IL-4 among pregnant women with low SES. However, among women with high SES, greater repetitive negative thinking was associated with higher serum levels of the proinflammatory cytokine IL-6 while greater presence of meaning in life was associated with higher serum levels of the antiinflammatory cytokine IL-4. These data provide insight into psychological processes that may contribute to favorable inflammatory profiles in perinatal women, though these associations may be more readily observable among women with greater financial stability. Additional data identifying other world views or cognitive factors that contribute to cytokine levels among women with low SES are warranted. Moreover, future examination of the role of these psychological processes in intervention studies with biological indicators would be informative. These studies will play a crucial role in the guidance of clinical care moving forward.
Acknowledgements:
We appreciate the contributions of our Clinical Research Assistants and students to data collection. We would like to thank our study participants and the staff at the OSU Clinical Research Center and Wexner Medical Center Prenatal Clinic.
Role of Funding Sources: This study was supported by the National Institutes of Health (R01 NR01366, LMC). The project described was supported by Award Number Grant UL1TR001070 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Footnotes
Given the limited variability in the cumulative SES variable, secondary analyses were conducted with cumulative SES defined as a dichotomous variable (i.e., cumulative SES of 0 to 3=0, cumulative SES of 4=1). Findings were consistent with those reported, with the exception that the p-value for the interaction between presence of meaning in life and SES on IL-4 levels went from p = 0.03 to p = 0.058. In addition, follow-up analyses of the association between repetitive negative thinking and IL-6 levels among high SES women went from p = 0.056 to p = 0.068.
Conflicts of Interest: The authors report no potential conflicts of interest.
References
- Bauer DJ, & Curran PJ (2005). Probing interactions in fixed and multilevel regression: Inferential and graphical techniques. Multivariate Behavioral Research, 40, 373–400. [DOI] [PubMed] [Google Scholar]
- Beach SRH, Dogan MV, Brody GH, & Philibert RA (2014). Differential impact of cumulative SES risk on methylation of protein–protein interaction pathways as a function of SLC6A4 genetic variation in African American young adults. Biological Psychology, 96, 28–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Black DS, & Slavich GM (2016). Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Annals of the New York Academy of Sciences, 1373, 13–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blair L, Porter K, Leblebicioglu B, & Christian L (2015). Poor sleep quality and associated inflammation predict preterm birth: Heightened risk among African Americans. Sleep, 38, 1259–1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blumenshine P, Egerter S, Barclay CJ, Cubbin C, & Braveman PA (2010). Socioeconomic disparities in adverse birth outcomes: a systematic review. American Journal of Preventive Medicine, 39, 263–272. [DOI] [PubMed] [Google Scholar]
- Bower JE, & Irwin MR (2016). Mind–body therapies and control of inflammatory biology: A descriptive review. Brain, Behavior, and Immunity, 51, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M, & Posner S (2005). Socioeconomic status in health research: One size does not fit all. JAMA, 294, 2879–2888. [DOI] [PubMed] [Google Scholar]
- Bublitz MH, Vergara-Lopez C, Treter MOR, & Stroud LR (2016). Association of lower socioeconomic position in pregnancy with lower diurnal cortisol production and lower birthweight in male infants. Clinical Therapeutics, 38, 265–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burton LM, Bonilla-Silva E, Ray V, Buckelew R, & Hordge Freeman E (2010). Critical race theories, colorism, and the decade’s research on families of color. Journal of Marriage and Family, 72, 440–459. [Google Scholar]
- Chatterjee P, Chiasson VL, Bounds KR, & Mitchell BM (2014). Regulation of the anti-inflammatory cytokines interleukin-4 and interleukin-10 during pregnancy. Frontiers in Immunology, 5, 124–130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen E (2007). Impact of socioeconomic status on physiological health in adolescents: An experimental manipulation of psychosocial factors. Psychosomatic Medicine, 69, 348–355. [DOI] [PubMed] [Google Scholar]
- Chen E, & Miller GE (2013). Socioeconomic status and health: Mediating and moderating factors. Annual Review of Clinical Psychology, 9, 723–749. [DOI] [PubMed] [Google Scholar]
- Christian LM (2012). Psychoneuroimmunology in pregnancy: Immune pathways linking stress with maternal health, adverse birth outcomes, and fetal development. Neuroscience & Biobehavioral Reviews, 36, 350–361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christian LM, Beverly C, Mitchell AM, Karlsson E, Porter K, Schultz-Cherry S, & Ramilo O (2017). Effects of prior influenza virus vaccination on maternal antibody responses and cord blood antibody titers. Vaccine, 35, 5283–5290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christian LM, Glaser R, Porter K, & Iams JD (2013). Stress-induced inflammatory responses in women: Effects of race and pregnancy. Psychosomatic Medicine, 75, 658–669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christian LM, & Porter K (2014). Longitudinal changes in serum proinflammatory markers across pregnancy and postpartum: Effects of maternal body mass index. Cytokine, 70, 134–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corwin EJ, Guo Y, Pajer K, Lowe N, McCarthy D, Schmiege S, … Stafford B (2013). Immune dysregulation and glucocorticoid resistance in minority and low income pregnant women. Psychoneuroendocrinology, 38, 1786–1796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coussons-Read ME, Lobel M, Carey JC, Kreither MO, D’Anna K, Argys L, … Cole S (2012). The occurrence of preterm delivery is linked to pregnancy-specific distress and elevated inflammatory markers across gestation. Brain, Behavior, and Immunity, 26, 650–659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunkel Schetter C, & Dolbier C (2011). Resilience in the context of chronic stress and health in adults. Social and Personality Psychology Compass, 5, 634–652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehring T, & Watkins E (2008). Repetitive negative thinking as a transdiagnostic process. International Journal of Cognitive Therapy, 1, 192–205. [Google Scholar]
- Ehring T, Zetsche U, Weidacker K, Wahl K, Schonfeld S, & Ehlers A (2011). The Perseverative Thinking Questionnaire (PTQ): Validation of a content-independent measure of repetitive negative thinking. Journal of Behavior Therapy and Experimental Psychiatry, 42, 225–232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman EM, & Herd P (2010). Income, education, and inflammation: Differential associations in a national probability sample (the MIDUS study). Psychosomatic Medicine, 72, 290–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gallo LC, de los Monteros KE, & Shivpuri S (2009). Socieconomic status and health: What is the role of reserve capacity? Current Directions in Psychological Science, 18, 269–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gallo LC, & Matthews KA (2003). Understanding the association between socioeconomic status and physical health: Do negative emotions play a role? Psychological Bulletin, 129, 10–51. [DOI] [PubMed] [Google Scholar]
- Gillespie SL, Porter K, & Christian LM (2016). Adaptation of the inflammatory immune response across pregnancy and postpartum in Black and White women. Journal of Reproductive Immunology, 114, 27–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gowda C, Hadley C, & Aiello AE (2012). The association between food insecurity and inflammation in the U. S. adult population. American Journal of Public Health, 102, 1579–1586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gruenewald TL, Cohen S, Matthews KA, Tracy R, & Seeman TE (2009). Association of socioeconomic status with inflammation markers in black and white men and women in the Coronary Artery Risk Development in Young Adults (CARDIA) study. Social Science & Medicine, 69, 451–459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gu J, Strauss C, Bond R, & Cavanagh K (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1–12. [DOI] [PubMed] [Google Scholar]
- Hänsel A, Hong S, Cámara RJ, & Von Kaenel R (2010). Inflammation as a psychophysiological biomarker in chronic psychosocial stress. Neuroscience & Biobehavioral Reviews, 35, 115–121. [DOI] [PubMed] [Google Scholar]
- Hayes AF (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York City, NY: Guilford Press. [Google Scholar]
- Hayney MS, Love GD, Buck JM, Ryff CD, Singer B, & Muller D (2003). The association between psychosocial factors and vaccine-induced cytokine production. Vaccine, 21, 2428–2432. [DOI] [PubMed] [Google Scholar]
- Jewell SL, Luecken LJ, Gress-Smith J, Crnic KA, & Gonzales NA (2015). Economic stress and cortisol among postpartum low-income Mexican American women: Buffering influence of family support. Behavioral Medicine, 41, 138–144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keng S-L, Smoski MJ, & Robins CJ (2011). Effects of mindfulness on psychological health: A review of empirical studies. Clinical Psychology Review, 31, 1041–1056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koster A, Bosma H, Penninx BW, Newman AB, Harris TB, van Eijk JTM, … Rooks RN (2006). Association of inflammatory markers with socioeconomic status. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 61, 284–290. [DOI] [PubMed] [Google Scholar]
- Loucks EB, Pilote L, Lynch JW, Richard H, Almeida ND, Benjamin EJ, & Murabito JM (2010). Life course socioeconomic position is associated with inflammatory markers: the Framingham Offspring Study. Social Science & Medicine, 71, 187–195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews KA, & Gallo LC (2011). Psychological perspectives on pathways linking socioeconomic status and physical health. Annual Review of Psychology, 62, 501–530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews KA, Gallo LC, & Taylor SE (2010). Are psychosocial factors mediators of socioeconomic status and health connections? Annals of the New York Academy of Sciences, 1186, 146–173. [DOI] [PubMed] [Google Scholar]
- McEvoy PM, & Brans S (2012). Common versus unique variance across measures of worry and rumination: Predictive utility and mediational models for anxiety and depression. Cognitive Therapy and Research, 37, 183–196. [Google Scholar]
- McEvoy PM, Erceg-Hurn DM, Anderson RA, Campbell BNC, & Nathan PR (2015). Mechanisms of change during group metacognitive therapy for repetitive negative thinking in primary and non-primary generalized anxiety disorder. Journal of Anxiety Disorders, 35, 19–26. [DOI] [PubMed] [Google Scholar]
- McEvoy PM, Watson H, Watkins ER, & Nathan P (2013). The relationship between worry, rumination, and comorbidity: Evidence for repetitive negative thinking as a transdiagnostic construct. Journal of Affective Disorders, 151, 313–320. [DOI] [PubMed] [Google Scholar]
- Mitchell A, & Pössel P (2017). Repetitive negative thinking: The link between caregiver burden and depressive symptoms. Oncology Nursing Forum, 44, 210–216. [DOI] [PubMed] [Google Scholar]
- Morgan N, Irwin MR, Chung M, & Wang C (2014). The effects of mind-body therapies on the immune system: Meta-analysis. PloS One, 9, e100903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morozink JA, Friedman EM, Coe CL, & Ryff CD (2010). Socioeconomic and psychosocial predictors of interleukin-6 in the MIDUS national sample. Health Psychology, 29, 626–635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myers HF (2009). Ethnicity- and socio-economic status-related stresses in context: An integrative review and conceptual model. Journal of Behavioral Medicine, 32, 9–19. [DOI] [PubMed] [Google Scholar]
- Proctor BD, Semega JL, & Kollar MA (2016). Income and Poverty in the United States: 2015: Current Populations Reports (P60-256). Washington, DC: U.S. Government Printing Office. [Google Scholar]
- Ryff CD (2014). Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychotherapy and Psychosomatics, 83, 10–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryff CD, Singer BH, & Love GD (2004). Positive health: Connecting well-being with biology. Philosophical Transactions-Royal Society of London Series B: Biological Sciences, 359, 1383–1394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmeer KK, & Yoon AJ (2016). Home sweet home? Home physical environment and inflammation in children. Social Science Research, 60, 236–248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Segerstrom SC, & Miller GE (2004). Psychological stress and the human immune system: A meta-analytic study of 30 years of inquiry. Psychological Bulletin, 130, 601–630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Segerstrom SC, Schipper LJ, & Greenberg RN (2008). Caregiving, repetitive thought, and immune response to vaccination in older adults. Brain, Behavior, and Immunity, 22, 744–752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silva LM, Coolman M, Steegers EA, Jaddoe VW, Moll HA, Hofman A, … Raat H (2008). Low socioeconomic status is a risk factor for preeclampsia: The Generation R Study. Journal of Hypertension, 26, 1200–1208. [DOI] [PubMed] [Google Scholar]
- Silverman MN, Pearce BD, & Miller AH (2003). Cytokines and HPA axis regulation In Kronfol Z (Ed.), Cytokines and mental health (pp. 85–122). Norwell, MA: Kluwer. [Google Scholar]
- Sorokin Y, Romero R, Mele L, Wapner RJ, Iams JD, Dudley DJ, … Harper M (2010). Maternal serum interleukin-6, C-reactive protein, and matrix metalloproteinase-9 concentrations as risk factors for preterm birth< 32 weeks and adverse neonatal outcomes. American Journal of Perinatology, 27, 631–640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steger MF, Frazier P, Oishi S, & Kaler M (2006). The meaning in life questionnaire: Assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53, 80–93. [Google Scholar]
- Tang KL, Rashid R, Godley J, & Ghali WA (2016). Association between subjective social status and cardiovascular disease and cardiovascular risk factors: A systematic review and meta-analysis. BMJ Open, 6, e010137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thayer ZM, & Kuzawa CW (2014). Early origins of health disparities: Material deprivation predicts maternal evening cortisol in pregnancy and offspring cortisol reactivity in the first few weeks of life. American Journal of Human Biology, 26, 723–730. [DOI] [PubMed] [Google Scholar]
- Watkins ER (2008). Constructive and unconstructive repetitive thought. Psychological Bulletin, 134, 163–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wei SQ, Fraser W, & Luo ZC (2010). Inflammatory cytokines and spontaneous preterm birth in asymptomatic women: A systematic review. Obstetrics & Gynecology, 116, 393–401. [DOI] [PubMed] [Google Scholar]
- Weiss LA, Westerhof GJ, & Bohlmeijer ET (2016). Can we increase psychological well-being? The effects of interventions on psychological well-being: A meta-analysis of randomized controlled trials. PloS One, 11, e0158092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winkler G, Cseh K, Baranyi É, Melczer Z, Speer G, Hajós P, … Vargha P (2002). Tumor necrosis factor system in insulin resistance in gestational diabetes. Diabetes Research and Clinical Practice, 56, 93–99. [DOI] [PubMed] [Google Scholar]
- Zoccola PM, & Dickerson SS (2012). Assessing the relationship between rumination and cortisol: A review. The Journal of Psychosomatic Research, 73, 1–9. [DOI] [PubMed] [Google Scholar]
- Zoccola PM, Figueroa WS, Rabideau EM, Woody A, & Benencia F (2014). Differential effects of poststressor rumination and distraction on cortisol and C-reactive protein. Health Psychology, 33, 1606–1609. [DOI] [PubMed] [Google Scholar]