

A 75-year-old man was brought to our emergency department by ambulance with abdominal pain and nausea. Clinical examination revealed acute abdomen with massive distension owing to a clinically irreducible left-sided indirect inguinal hernia (scrotal hernia). Sonography showed a primarily unclear large collection of fluid extending from the upper abdomen to the left scrotal compartment. On abdominal computed tomography this was found to be a massive gastric retention with displacement of the gastroduodenal junction into the hernia and constriction of the gastric antrum in the area of the hernial orifice. The patient’s symptoms were primarily relieved by insertion of a gastric tube and drainage of 5 L of fluid. Because of the extent of the hernia, the patient underwent exploratory laparotomy, repositioning of the hernial contents, and preperitoneal mesh repair according to Wantz/Stoppa with a 25 × 15 cm polyvinylidenefluoride (PVDF) mesh. After full recovery the patient was able to return home.
Translated from the original German by David Roseveare.
Cite this as: Junge K, Otto J, Oral H: A rare cause of gastric outlet stenosis—scrotal hernia.
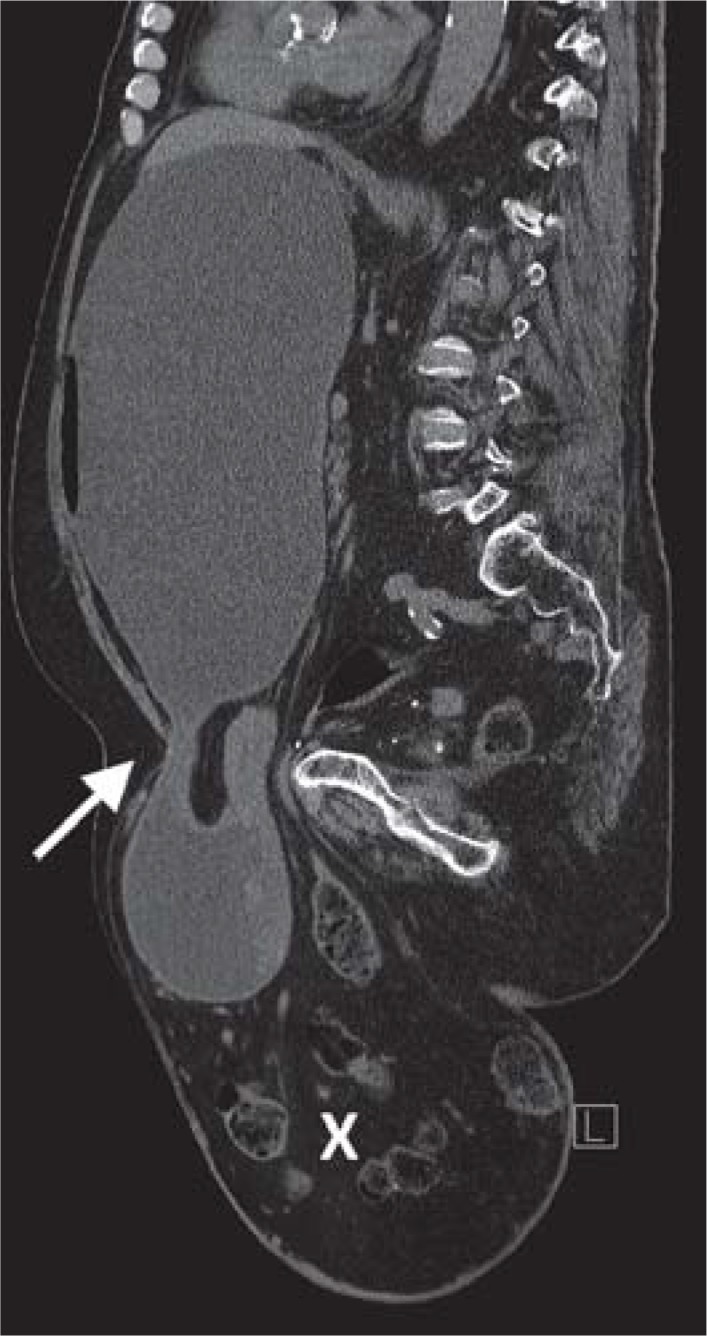
Computed tomography of the abdomen
Sagittal view, irreducible scrotal hernia: the gastroduodenal junction is inside the hernia and the stomach is distended due to antral stenosis (→). The hernial sac also contains further loops of intestine (X), and the fatty tissue has, typically, absorbed fluid.
Footnotes
Conflict of interest statement:
The authors declare that no conflict of interest exists