

Abstract
This study examines funding from the National Institutes of Health (NIH) to US dental institutions between 2005 and 2014 based on publicly available data from the NIH Research Portfolio Online Reporting Tools. Over the 10-y span, 56 US dental institutions received approximately $2.2 billion from 20 Institutes, Centers, and Offices at the NIH. The National Institute of Dental and Craniofacial Research (NIDCR) is the largest NIH supporter of dental institutions, having invested 70% of the NIH total, about $1.5 billion. The NIDCR is also the primary supporter of research training and career development, as it has invested $177 million, which represents 92% of the total NIH investment of $192 million. Over the past 10 y, about half of the NIDCR’s extramural award dollars have gone to dental schools, while the NIH has invested about 1%. There has been an approximately 10% net decrease in extramural dollars awarded to dental institutions over the past decade; however, given the year-to-year variability in support to dental institutions, it is unclear if this net decline reflects a long-term trend. In addition, there was an overall reduction in the extramural dollars awarded by the NIDCR and by the NIH. For example, from 2005 to 2014, the total NIDCR budget for extramural research decreased by roughly 4%, which represents a decrease of $20 million to dental institutions. After adjusting for inflation, the decline in funding to dental institutions from the NIDCR and NIH was approximately 30%. Although the NIDCR and NIH continue to invest in dental institutions, if the current decline were to continue, it could negatively affect the research conducted at dental institutions. Therefore, we discuss opportunities for dental institutions to increase NIDCR and NIH support and improve their capacity for research, research training, and career development.
Keywords: dental schools, dental research, dentistry, dental education, National Institute of Dental and Craniofacial Research, trends
Introduction
Continued investment in dental, oral, and craniofacial research is vital to improving the health of the public and to the future of the dental profession. A long-standing concern of dental researchers is ensuring that academic dental institutions play a role in the generation of new scientific knowledge (Gies 1926; Field 1995; Genco 1999; Bertolami 2002; Feinberg et al. 2015). A previous study reported on research funding from 2005 to 2009 (Lipton and Kinane 2011) to US dental schools from the National Institutes of Health (NIH) and the National Institute of Dental and Craniofacial Research (NIDCR), which is the federal government’s leading funder of dental, oral, and craniofacial research. This study stated that total NIH support to dental schools from Institutes, Centers, and Offices other than the NIDCR had increased annually, while NIDCR support to dental schools had decreased in nominal dollars and as a percentage of total NIDCR award dollars. The reported percentage of total NIDCR award dollars to dental schools declined from 50% in 2005 to 44% in 2009 and was cited as a worrisome trend in an accompanying perspective (Polverini 2011). The aim of the current study was to examine the total NIH and NIDCR funding to US dental institutions (dental schools plus 2 dental research institutions) over a longer period (2005 to 2014) and to ascertain if these downward trends were continuing.
Methods
The data set for this study was obtained from the NIH public resource on funded awards, called Research Portfolio Online Reporting Tools (RePORT; NIH 2015). The data set includes research, research training, and career development awards to institutions categorized by institution type. We selected “Schools of Dentistry” as defined by the NIH RePORT to capture dental institutions. A breakdown of how we calculated the number of NIDCR and NIH awards to dental institutions is presented in Appendix Table 1. The NIH RePORT funding numbers include the total direct and indirect costs for each award. All years associated with the funding data refer to US federal fiscal years. The final total number of awards to dental institutions was 5,990 from the NIH, of which 4,175 (70%) were from the NIDCR.
From 2005 to 2014, a total of 56 dental institutions received NIH awards, and 55 received NIDCR awards; these institutions compose the study population for the present data analysis. Nine US dental institutions from the American Dental Education Association’s (2015) list of current dental institutions did not receive any NIH awards during this period.
Awards classified as training and career development (herein referred to as “training” award dollars) included F awards (individual fellowships), K awards (individual career development awards), T awards (institutional training awards), and the T90/R90 awards (interdisciplinary research training awards). Research project grants were defined according to the NIH Data Book (NIH 2014). No research and development contracts were included in the data set.
NIDCR and NIH funding were obtained from the publicly available Congressional Justification of Budget Requests for each fiscal year. The total extramural award dollars were obtained from the sum of “total research grants” and “total research training” budget numbers, and the training dollars awarded are simply the “total research training” amount.
To quantify the variation in the percentage of extramural dollars awarded to dental institutions over time, we calculated the z score for each year by subtracting the individual value for each year (x) from the overall 10-y mean (μ), divided by the standard deviation of the mean (σ), using the following formula: (x – μ)/σ. Points that were >2 standard deviations outside the mean (z score >2) were significantly different and outside the normal distribution of the data set.
Results
To assess the breadth of funding to US dental institutions from the NIDCR and NIH, we examined the 56 dental institutions that received extramural award dollars from the NIH between fiscal years 2005 and 2014 (Table). In total, 55 (98.2%) of these institutions received some NIDCR support; 10 received all of their NIH funding from the NIDCR; and about half (n = 27) received >75% of their NIH support from the NIDCR. Over the past decade, the NIDCR invested $1,449.86 million in dental institutions, which is 69.9% of the NIH total of $2,117.41 million. NIDCR support was distributed across a range of dental institutions. Of the 65 US dental institutions listed by the American Dental Education Association in 2014, a total of 46 received funding from the NIDCR. Furthermore, of the NIDCR’s funding to dental institutions, the top quartile received 59.5%, and the top half received 85.4% (Appendix Fig. 1).
Table 1.
NIH and NIDCR Extramural Dollars Awarded to the 56 Assessed Dental Institutions: Fiscal Years 2005 to 2014.
| Organization | NIH |
NIDCR |
||||||
|---|---|---|---|---|---|---|---|---|
| Rank | $M | From NIDCR, % | $M | Rank | NIH R01 from NIDCR, % | NIH RPG from NIDCR, % | NIH Training from NIDCR, % | |
| University of California, San Francisco | 1 | 166.35 | 59.0 | 98.17 | 1 | 40.9 | 47.6 | 95.9 |
| University of Michigan at Ann Arbor | 2 | 124.43 | 78.3 | 97.39 | 2 | 76.8 | 78.0 | 92.4 |
| Forsyth Institute | 3 | 102.74 | 86.2 | 88.54 | 3 | 85.0 | 88.8 | 94.8 |
| University of North Carolina, Chapel Hill | 4 | 98.32 | 79.5 | 78.13 | 4 | 77.3 | 78.2 | 94.8 |
| University of California, Los Angeles | 5 | 93.07 | 77.1 | 71.78 | 6 | 71.7 | 75.4 | 97.5 |
| University of Florida | 6 | 91.30 | 72.4 | 66.08 | 9 | 71.7 | 70.3 | 69.4 |
| University of Maryland, Baltimore | 7 | 89.19 | 41.7 | 37.23 | 14 | 47.3 | 38.7 | 88.1 |
| New York University | 8 | 87.36 | 81.4 | 71.13 | 7 | 67.1 | 83.2 | 94.3 |
| University of Alabama at Birmingham | 9 | 83.04 | 89.4 | 74.22 | 5 | 70.6 | 88.1 | 100.0 |
| University of Pennsylvania | 10 | 81.93 | 38.8 | 31.76 | 18 | 47.5 | 40.3 | 26.8 |
| Boston University Medical Campus | 11 | 79.71 | 65.2 | 51.95 | 10 | 54.1 | 54.7 | 92.9 |
| University of Southern California | 12 | 75.40 | 60.1 | 45.34 | 11 | 6.1 | 59.4 | 69.4 |
| University of Washington | 13 | 72.78 | 92.5 | 67.35 | 8 | 85.5 | 90.3 | 100.0 |
| Harvard University | 14 | 66.98 | 17.2 | 11.52 | 33 | 10.7 | 12.0 | 96.4 |
| University of Minnesota, Twin Cities | 15 | 55.55 | 63.1 | 35.08 | 15 | 47.1 | 57.3 | 88.0 |
| University of Connecticut School of Medicine/Dental Medicine | 16 | 53.15 | 58.9 | 31.31 | 19 | 46.9 | 49.0 | 100.0 |
| University of Louisville | 17 | 48.20 | 68.3 | 32.90 | 17 | 94.6 | 90.0 | 94.6 |
| University of Rochestera | 18 | 46.91 | 95.1 | 44.59 | 12 | 96.0 | 95.2 | 99.4 |
| University of Illinois at Chicago | 19 | 46.12 | 60.2 | 27.77 | 21 | 68.4 | 58.0 | 100.0 |
| University of Pittsburgh at Pittsburgh | 20 | 43.83 | 96.0 | 42.08 | 13 | 98.0 | 97.4 | 86.5 |
| University of Texas Health Science Center, San Antonio | 21 | 39.77 | 65.2 | 25.95 | 24 | 51.9 | 56.4 | 98.1 |
| Ohio State University | 22 | 37.32 | 48.4 | 18.08 | 26 | 31.9 | 36.5 | 99.4 |
| University of Missouri, Kansas City | 23 | 35.54 | 46.0 | 16.35 | 29 | 60.5 | 37.7 | 99.2 |
| University of Iowa | 24 | 33.61 | 100.0 | 33.61 | 16 | 100.0 | 100.0 | 100.0 |
| Medical University of South Carolina | 25 | 31.43 | 39.8 | 12.50 | 32 | 90.8 | 82.6 | 97.2 |
| State University of New York at Buffalo | 26 | 30.58 | 85.8 | 26.24 | 22 | 87.7 | 85.2 | 90.9 |
| Case Western Reserve University | 27 | 29.63 | 100.0 | 29.63 | 20 | 100.0 | 100.0 | 100.0 |
| University of Colorado Denver | 28 | 29.31 | 88.6 | 25.97 | 23 | 85.4 | 87.8 | 93.5 |
| University of Nebraska Medical Center | 29 | 26.99 | 19.5 | 5.27 | 41 | 62.8 | 56.7 | n/a |
| University of Kentucky | 30 | 24.66 | 17.8 | 4.38 | 42 | 100.0 | 93.7 | 100.0 |
| Texas A&M University Health Science Center | 31 | 20.72 | 93.4 | 19.35 | 25 | 96.5 | 94.8 | 100.0 |
| Columbia University Health Sciences | 32 | 20.47 | 63.2 | 12.95 | 30 | 54.9 | 60.5 | 100.0 |
| Rutgers Biomedical and Health Sciences School of Dental Medicine | 33 | 18.93 | 89.4 | 16.92 | 27 | 92.6 | 89.2 | 100.0 |
| State University New York, Stony Brook | 34 | 18.88 | 88.2 | 16.66 | 28 | 79.8 | 87.7 | 100.0 |
| Tufts University, Boston | 35 | 18.24 | 70.1 | 12.78 | 31 | 67.5 | 70.1 | n/a |
| University of Texas Health Science Center | 36 | 14.99 | 58.5 | 8.77 | 35 | 45.0 | 52.9 | 100.0 |
| Oregon Health and Science University | 37 | 14.29 | 37.6 | 5.38 | 40 | 24.9 | 35.5 | 100.0 |
| Virginia Commonwealth University | 38 | 11.98 | 82.3 | 9.85 | 34 | 88.9 | 84.0 | 71.3 |
| LSU Health Sciences Center | 39 | 9.16 | 71.6 | 6.56 | 38 | 73.8 | 75.2 | n/a |
| Georgia Health Sciences University | 40 | 8.90 | 88.2 | 7.85 | 36 | 90.1 | 87.2 | 100.0 |
| Indiana University-Purdue University at Indianapolis | 41 | 7.75 | 94.0 | 7.28 | 37 | 94.8 | 93.7 | 100.0 |
| University of Puerto Rico Medical Sciences | 42 | 6.08 | 100.0 | 6.08 | 39 | 100.0 | 100.0 | 100.0 |
| University of Oklahoma Health Sciences Center | 43 | 3.43 | 100.0 | 3.43 | 43 | 100.0 | 100.0 | n/a |
| Nova Southeastern University | 44 | 3.30 | 100.0 | 3.30 | 44 | 100.0 | 100.0 | n/a |
| University of Mississippi Medical Center | 45 | 2.50 | 100.0 | 2.50 | 45 | 100.0 | 100.0 | n/a |
| University of Tennessee Health Science Center | 46 | 2.15 | 44.9 | 0.97 | 50 | 38.9 | 43.2 | n/a |
| Howard University | 47 | 2.06 | 52.7 | 1.09 | 48 | 100.0 | 100.0 | n/a |
| Temple University of the Commonwealth | 48 | 1.91 | 21.7 | 0.42 | 51 | 0.0 | 22.0 | n/a |
| Marquette University | 49 | 1.81 | 100.0 | 1.81 | 46 | 100.0 | 100.0 | n/a |
| Meharry Medical College | 50 | 1.51 | 100.0 | 1.51 | 47 | 100.0 | 100.0 | n/a |
| Creighton University | 51 | 1.41 | 69.8 | 0.98 | 49 | 100.0 | 68.4 | 100.0 |
| Loma Linda University | 52 | 0.66 | 36.3 | 0.24 | 54 | n/a | 36.4 | n/a |
| University of Nevada, Las Vegas | 53 | 0.36 | 100.0 | 0.36 | 52 | n/a | 100.0 | n/a |
| University of Utah | 54 | 0.34 | 100.0 | 0.34 | 53 | 100.0 | 100.0 | n/a |
| University of the Pacific, Stockton | 55 | 0.29 | 62.9 | 0.18 | 55 | n/a | 62.1 | n/a |
| West Virginia University | 56 | 0.07 | 0.0 | 0.00 | n/a | n/a | 0.0 | n/a |
| Total | 2,117.41 | 69.9 | 1,449.86 | |||||
Includes the percentage of NIH extramural dollars awarded by the NIDCR to each institution and the percentage of NIH extramural award dollars for selected award mechanisms awarded by the NIDCR. For dental institutions that merged during the years examined in this analysis, the data from the 2 institutions were combined for all years. The merged institutions include 1) Georgia Health Sciences University and Georgia Regents University and 2) Rutgers Biomedical and Health Sciences University and University of Medicine and Dentistry of New Jersey.
n/a, not applicable; NIDCR, National Institute of Dental and Craniofacial Research; NIH, National Institutes of Health; RPG, research project grant.
Data from the University of Rochester are limited to fiscal years 2008 to 2014 (NIH dental/oral and craniofacial spending category only).
To understand the types of NIDCR and NIH funding received by dental institutions, we next investigated the distribution of funding for 3 major award mechanisms: R01 grants, research project grants, and training awards (Table). The R01 award mechanism supports a discrete research project and is the gold standard of NIH awards. The NIDCR invested $764.92 million into R01 awards at dental institutions, which is 63.9% of the NIH total of $1,197.27 million (also see Appendix Table 2). About half (n = 27) of the institutions that received R01 funding from the NIDCR (52.9%) also received >75% of their total NIH funding for R01 awards from the NIDCR.
Training awards are essential to help the next generation of dentist scientists start to become independent researchers and to maintain a strong oral health research workforce. The NIDCR invested $176.95 million into training awards at dental institutions, which represents 91.9% of the NIH total of $192.49 million (also see Appendix Table 2). Of the 40 dental institutions that received training award dollars, 31 received >90% from the NIDCR (77.5% of all institutions), and 17 received 100% from the NIDCR (42.5% of all institutions).
The 2011 article by Lipton and Kinane determined that the percentage of total NIDCR award dollars to dental schools had declined from 50% in 2005 to 44% in 2009; therefore, we wanted to do a similar analysis to extend these findings by examining NIDCR and NIH funding to dental institutions from 2005 to 2014 (Fig. 1A). The highest percentage of NIDCR extramural dollars awarded to dental institutions was in 2005 (52.0%), and the lowest percentage was observed in 2014 (47.1%). Across the 10-y period, the mean percentage of extramural award dollars from the NIDCR to dental institutions was 49.4%, and the median was 49.5%. To quantify the variation in extramural dollars awarded to dental institutions over time, we calculated the z score for each year. We found that the percentage of funding to dental institutions for each year did not fall outside 2 standard deviations of the overall mean for the 10-y period (SD, 1.7%; z score range, −1.4 to 1.6). This suggests that there was no statistically significant variation from the overall 10-y mean in the year-to-year funding to dental institutions; it also suggests that from 2005 to 2014, approximately 49% of the NIDCR’s extramural dollars were consistently awarded to dental institutions. The highest percentage of NIDCR extramural award dollars for training occurred in 2005 (7.4%), and the lowest percentage was awarded in 2012 (4.5%). Overall, the mean percentage of NIDCR’s extramural dollars devoted to training was 6.0%, and the median was 6.2%. The NIH extramural award percentage to dental institutions similarly declined from 1.1% in 2005 to 0.9% in 2014 (Appendix Fig. 2), and the mean and the median were both 1.0%.
Figure 1.

National Institute of Dental and Craniofacial Research (NIDCR) awards to dental institutions. (A) The percentage of NIDCR’s extramural dollars awarded to dental institutions from 2005 to 2014 (dark blue bars). The light blue bars represent the percentage of NIDCR’s extramural dollars awarded to dental institutions specifically for training. (B) The percentage of NIDCR’s total extramural dollars awarded to dental institutions (blue) as compared with medical institutions (green lines), nonmedical/dental academic institutions (orange), and other organizations (purple) in fiscal year 2014, broken down by extramural award dollars and extramural training award dollars.
The NIDCR aims to support the best oral health research across all institution types to ensure a diverse and innovative research portfolio. Therefore, we investigated the distribution of the NIDCR’s total extramural and training award dollars based on the NIH RePORT classification for institution type (Fig. 1B). In 2014, 45.6% of NIDCR’s total extramural award dollars and 73.7% of NIDCR’s extramural training award dollars went to dental institutions as compared to all other types of organizations. The remaining total extramural award dollars comprised 25.9% awarded to medical institutions, 12.1% to other nonmedical/nondental academic institutions, and 16.5% to other organizations, which included hospitals, research institutes, and small businesses. For training, the comparable investments were 15.4% for medical institutions, 7.0% to other nonmedical/nondental academic institutions, and 3.8% to other organizations.
To assess the trends in NIDCR and NIH support of dental institutions, we examined awarded extramural dollars from 2005 to 2014 while taking inflation into consideration using the Biomedical Research and Development Price Index (Fig. 2). Although there was variability from year to year, total NIH funding to dental institutions decreased from $215.77 million in 2005 to $195.35 million in 2014 (–9.5%). Total NIDCR funding to dental institutions also decreased, from $154.42 million in 2005 to $134.72 million in 2014 (–12.8%). Furthermore, when adjusted for inflation based on the Biomedical Research and Development Price Index (2014 constant dollars), the decline in total award dollars to dental institutions from 2005 to 2014 was 33.1% from the NIDCR and was 30.6% from the NIH. The percentage of total NIH extramural dollars awarded to dental institutions from the NIDCR was stable at about 70% across the 10-y period examined.
Figure 2.

Awards to US dental institutions during fiscal year 2005 to 2014 by National Institutes of Health (NIH; dark blue bars = actual dollars, light blue bars = adjusting for inflation in 2014 dollars with the Biomedical Research and Development Price Index) and National Institute of Dental and Craniofacial Research (NIDCR; dark green bars = actual dollars, light green bars = adjusting for inflation in 2014 dollars with the Biomedical Research and Development Price Index). The black line represents the percentage of NIH extramural dollars awarded to dental institutions by the NIDCR.
A total of 20 NIH Institutes, Centers, and Offices provided support to 56 dental institutions in 2014 (Fig. 3). NIDCR contributed $134.7 million (69.0%) of the total NIH investment of $195.3 million. The next-largest NIH funding Institutes, Centers, and Offices in 2014 were the National Institute of Arthritis and Musculoskeletal and Skin Diseases (5.9%), the National Institute of Allergy and Infectious Diseases (4.5%), and the National Institute of General Medical Sciences (3.8%).
Figure 3.
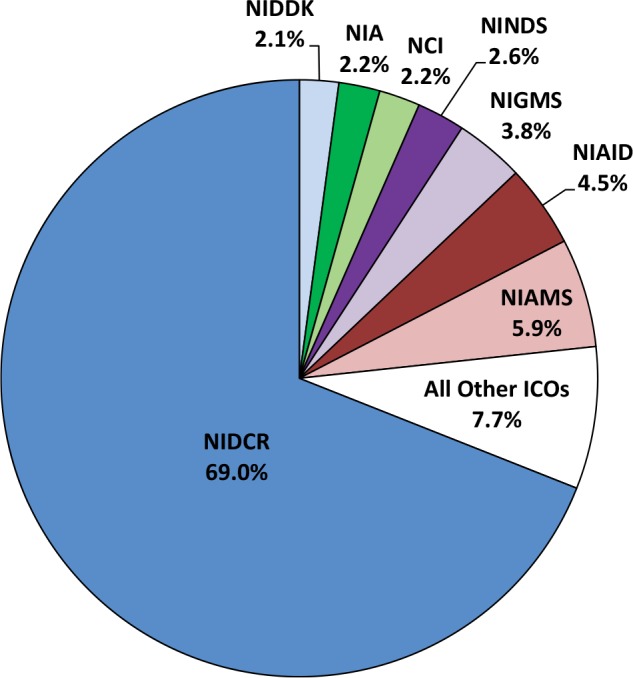
Awards to dental institutions for federal fiscal year 2014 by National Institutes of Health (NIH) Institutes, Centers, and Offices: National Institute of Dental and Craniofacial Research (NIDCR); National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); National Institute on Aging (NIA); National Cancer Institute (NCI); National Institute of Neurological Disorders and Stroke (NINDS); National Institute of General Medical Sciences (NIGMS); National Institute of Allergy and Infectious Diseases (NIAID); National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). All other institutes, centers, and offices: Fogarty International Center, the National Center for Complementary and Integrative Health (formerly the National Center for Complementary and Alternative Medicine), the National Eye Institute, the National Heart, Lung, and Blood Institute, the National Institute on Alcohol Abuse and Alcoholism, the National Institute of Biomedical Imaging and Bioengineering, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute on Drug Abuse, the National Institute on Deafness and Other Communication Disorders, the National Institute of Mental Health, the National Institute on Minority Health and Health Disparities, and the Office of the Director.
Discussion
A 2011 study by Lipton and Kinane reported that the total dollars awarded to US dental schools from the NIDCR had declined between 2005 and 2009. Therefore, we examined total NIDCR and NIH funding to US dental institutions over a longer period (2005 to 2014) to determine if there was a continuation of the reported trend.
NIDCR and NIH Support of Dental Institutions
The NIDCR is by far the largest supporter of dental institutions at NIH. Over the past 10 y, approximately 70% of the NIH’s extramural dollars awarded to dental institutions came from the NIDCR (Fig. 2) and remained relatively stable from 2005 to 2014. We also observed that from 2005 to 2014, on average, 49.4% of the NIDCR’s extramural dollars were awarded to dental institutions (Fig. 1). The NIDCR has been the sole NIH funding source for 10 of the 65 US dental institutions on the American Dental Education Association’s list (roughly 15%), while 9 US dental institutions received no NIH funding (approximately 14%). The NIDCR’s support is fairly well distributed across the dental institutions and is not highly concentrated at a small number of research-intensive institutions (Appendix Fig. 1). Although the NIDCR is the primary NIH supporter of dental institutions, in 2014, 30% of NIH support was from 19 other Institutes, Centers, and Offices, which reflects the diversity of research occurring at dental institutions (Fig. 3).
Between 2005 and 2014, there was a net decrease in award dollars to dental institutions from both the NIDCR and the NIH, −12.8% and −9.5%, respectively. However, the percentage of extramural dollars to dental institutions (vs. other types of institutions) has remained relatively stable, averaging approximately 49.4% across the 10-y period. In addition, although there have been fluctuations in support (the NIDCR saw a peak in funding in 2005 [52.0%] and a trough in 2014 [47.1%]), there is no significant variation from the 10-y mean in the year-to-year fluctuations, which suggests that the percentage of NIDCR funding to dental institutions over time has remained relatively stable. Therefore, the data suggest that this 10-y net decrease reflects a trough in the year-to-year fluctuations, rather than a long-term trend of reduced funding to dental institutions. Future analyses are warranted to determine if the current trough continues. Regardless of this finding, developing strategies to enhance research capacity at dental schools would be of value to the dental profession.
An additional factor in the NIDCR and NIH support of dental institutions was the decrease in total available extramural award dollars. From 2005 to 2014, the total NIDCR budget for extramural research decreased 3.6% (from $296.82 million to $286.19 million). This partially explains the NIDCR support to dental institutions decreasing from $154.42 million in 2005 to $134.72 million in 2014, which is −12.8% ($19.7 million). When adjusting for inflation, the decline in dental institution funding from the NIDCR and NIH was approximately 33% and 30%, respectively. It is promising that after a decade of minimal to no increase in the NIDCR and NIH budgets, the recent Consolidated Appropriations Act of 2016 (public law 114-113) includes an increase in support for biomedical research, with a 6.6% increase to the NIH and a 3.9% increase to the NIDCR.
NIDCR Support for Training at Dental Institutions
Since research training and career development are essential for the future of dental research, we examined the NIDCR’s investment in extramural training at dental institutions (Fig. 1A). Over the past 10 y, about 6.0% of the NIDCR’s extramural award dollars has gone to training at dental institutions. There was a decrease from 2005 (7.4%) to 2014 (4.8%), which mirrors the overall decrease in NIDCR funding support to dental institutions over the 10-y period examined.
Potential Opportunities for Dental Institutions
The goal of this study was to provide data on NIH and NIDCR support for US dental institutions that could guide future decision making related to oral health research and dental professional training. It is beyond the scope of this article to make specific recommendations to dental institutions; however, some potential opportunities will be briefly discussed. To start, the 2016 budget increase for the NIDCR and the NIH is an opportunity for more dental, oral, and craniofacial researchers to apply for research and training awards. Dental institutions that receive little or no NIDCR or NIH support should consider developing strategies to increase research activities and support from the NIDCR and from other Institutes, Centers, and Offices at the NIH. In addition, although this analysis did not examine the number of applications that are submitted by dental institutions to the NIH each year, data from the NIH Data Book suggest that research project grant applications submitted to the NIDCR have been flat over the past 10 y, while submissions to NIH have increased 1.2-fold. Therefore, increasing the number of high-quality applications should be a priority for all dental, oral, and craniofacial researchers and dental institutions.
Differences with the Lipton and Kinane Study
The data presented were not intended to recapitulate the data reported in the Lipton and Kinane study but rather to provide a comprehensive follow-up to the 2011 study to examine funding to US dental institutions over a broader time frame (10 y). Accordingly, there are several differences between the current study and the Lipton and Kinane study. The 2011 study found that NIDCR funding to dental schools declined from 50% in 2005 to 44% in 2009 (a difference of 6%), whereas we observed a decrease of 2.2% (52.0% to 49.8%). Possible reasons for this discrepancy include 1) using publicly available NIH RePORT award data for schools of dentistry, 2) obtaining annual extramural research and training award dollars from the public Congressional Justification of Budget Requests, and 3) performing no manual curation of the data set. We chose this approach to allow the community to reproduce the data set and to allow future standardized analyses. In addition, to ensure that our study was comprehensive, we included 2 additional dental research institutions: the Forsyth Institute and the University of Rochester (see Table). Although both are postgraduate dental institutions, they were included in the data set because they are important components of training the next generation of dental researchers and they receive a significant amount of NIDCR and NIH support. Furthermore, many trainees from these 2 institutions populate the research faculty in dental schools across the country.
Limitations of the Data Analysis
As stated above, the data set was derived from publicly available information on NIH RePORT, and the institution type classification was directly dependent on information entered by the submitting institution; therefore, it is possible that there are classification errors in the type of institution. Additionally, each award and the associated dollars are attributed to only 1 institution, which does not fully capture the distribution of funds to other associated institutions—a common feature of many awards. For example, the University of Alabama at Birmingham has been ranked first for the past 3 y largely due to funding of the National Dental Practice-Based Research Network, which in turn supports a number of other dental institutions not captured in this analysis. Also not included here is support from other sources beyond the NIH, including other federal agencies, state and local governments, private industry, research foundations, and sources of funding within universities.
Author Contributions
C.L. Ferland, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; M. O’Hayre, W.M. Knosp, C.H. Fox, D.J. Horsford, contributed to conception, design, and data interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplementary Material
Footnotes
A supplemental appendix to this article is published electronically only at http://jdr.sagepub.com/supplemental.
The authors received no financial support and declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
- American Dental Education Association. 2015. U.S. and Canadian dental schools [accessed 2016 Jul 20]. http://www.adea.org/dental_education_pathways/aadsas/Pages/PDS.aspx.
- Bertolami CN. 2002. The role and importance of research and scholarship in dental education and practice. J Dent Educ. 66(8):918–924. [PubMed] [Google Scholar]
- Feinberg F, Garcia LT, Polverini PJ, Fox CH, Valachovic RW. 2015. The vital role of research in preserving the oral health of the public and dental profession. J Am Dent Assoc. 146(6):355–356. [DOI] [PubMed] [Google Scholar]
- Field MJ, editor. 1995. Dental education at the crossroads: challenges and change. Washington (DC): National Academies of Medicine. [PubMed] [Google Scholar]
- Genco R. 1999. Building partnerships and interdisciplinary collaborations in oral health research. In: AADS 75th Anniversary Summit Conference. Washington (DC): American Dental Education Association. [Google Scholar]
- Gies WJ. 1926. Dental education in the United States and Canada: a report to the Carnegie Foundation for the advancement of teaching. J Am Coll Dent. 79(2):32–49. [PubMed] [Google Scholar]
- Lipton JA, Kinane DF. 2011. Total NIH support to US dental schools, 2005–2009. J Dent Res. 90(3):283–288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institutes of Health. 2014. NIH data book [accessed 2016 Jul 20]. http://report.nih.gov/nihdatabook/index.aspx.
- National Institutes of Health. 2015. Research portfolio online reporting tools (RePORT) [accessed 2016 Jul 20]. https://report.nih.gov/.
- Polverini PJ. 2011. Shaping the future of the dental profession through research and discovery. J Dent Res. 90(3):281–282. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.