

Abstract
Distal tibiofibular syndesmosis injury (DTS) occurs frequently with ankle sprains. Current treatments pose several limitations including causing soft tissue irritation, bringing damage to fixation secondary to weight-bearing, and requiring follow-up surgeries. Here, we investigated the clinical effects of a new technique, titanium cable isotonic annular fixation, for the treatment of DTS injury. From January 2015 to June 2017, 36 patients with ankle fractures and DTS injuries had their fractures repaired with the titanium cable isotonic annular fixation system. Recovery was scored by the AOFAS ankle function score system. We also assessed the differences in ankle motion between healthy and operative joints, and recorded the complications. All patients recovered from surgery without any serious complications. We followed all the cases for 18-25 months with an average follow-up of 21.26±3.23 months. 12 months after the operation, X-ray images showed that the titanium cables were fixed in the correct position without any fracture or loosening. Additionally, no degeneration or traumatic arthritis was observed in the ankle joint. There were no incision or bone mineral density changes between the titanium fix and tibiofibular bones. Nearly all patients recovered well except for three who developed inflammation and infection. However, these three patients recovered following 1 week of intravenous antibiotics and local radiofrequency physiotherapy. According to the AOFAS scoring system, all patients achieved satisfactory recovery 12 months post operation. Our titanium cable isotonic annular fixation system has both the advantages of elastic and rigid fixations. It can restore isotonic strength of the distal tibiofibular joint, and its biomechanical performance approaches normal physiological function. After the operation, patients tolerated weight-bearing exercise and recovered joint mobility. Finally, there is no need to remove the distal tibiofibular implant after 12 weeks. Overall, it is a highly effective surgical method to treat DTS injury.
Keywords: Distal tibiofibular syndesmosis injury, ankle fracture, titanium cable, isotonic annular fixation
Introduction
The distal tibiofibular syndesmosis (DTS) is an important structure for maintaining the stability of the ankle joint, and 80% of the injuries to the DTS occur in ankle fractures [1,2]. Ankle fractures with DTS injury are most frequently caused by rotational force, especially by prepronation and pronation or postpronation and pronation (Lauge-Hansen classification), or type B and C (Danis-Weber classification) [3-5]. Ankle-point mismatch caused by the dissociation of distal tibiofibular syndesmosis changes the stress distribution of the tibial talus joint surface dramatically, which results in increased ankle joint load and walking pain [6]. Because of these complications, the dissociation of ankle joint fracture with DTS requires anatomical reduction and fixation to avoid unstable, long-term chronic pain and traumatic arthritis of the ankle joint [7]. Previously, tibiofibular bone fixation with distal tibiofibular screw was the most widely used method. It is simple, effective, and safe, however it poses several problems. This fixation method influences the motion; the screws are easily loose; distal tibiofibular connections are easily damaged; secondary surgeries are sometimes required; the fixation leads to limited tibiofibular joint micromotion; and a secondary extension of distal tibiofibular joint may present [8-11].
Recently, the button or annular fixation technique has been adopted for the elastic fixation of the DTS, which has shown promising results with fewer adverse effects [12,13]. The side effects can include loosening of the fixation, local soft tissue inflammation, and osteolysis [14-18]. In order to maintain the micro-dynamic function of the tibiofibular joint and the strength in the fixation, we fixed the DTS with a titanium cable isotonic annular fixation system. This isotonic fixation both reconstructed and improved the biomechanical strength of the syndesmosis while avoided the existing problems associated with screw and traditional elastic fixation methods. Here, we demonstrate the remarkable therapeutic effects of a titanium cable isotonic annular fixation system in the treatment of distal tibiofibular syndesmosis injury.
Materials and methods
Ethics statement
This study was approved by the Ethics Committee of Shenzhen People’s Hospital at Jinan University. All volunteers gave informed consent prior to participating in the study.
General information
Participants: Patient ages range from 18 to 60 years. Injuries occurred less than one week prior to treatment. Ankle fracture was accompanied by DTS separation in either the ankle orthotopic, ankle acupoint, or intraoperative external rotation stress positions. The criteria for DTS separation were inferior tibiofibular clear space (TFCS) in anteroposterior (AP) X-ray, 20° internal rotation clearance greater or less than 6 mm, 20° internal rotation less than 1.0 mm in AP X-ray, or medial clear space (MCS) greater than superior clear space (SCS) or greater than 5.0 mm in AP X-ray. Exclusion criteria included open fractures, fractures accompanied by vascular and nerve injury, and multiple injuries and pathological fractures. Summary: 36 cases including 20 women and 16 men; 19-56 years old (average 31.8 (35.3±14.6) years old); Causes of injury: 19 sports injuries, 11 motor vehicle injuries, 6 fall-related injuries; Fractures classified via Lauge-Hansen criteria: 22 cases of pronation and extraversion, 11 cases of supination and extraversion, 3 cases of pronation and abduction. Fractures classified via Danis-Weber criteria: 11 cases were type B, 17 were type C1, and 8 were type C2. The interval time from injury to operation was 7-14 days (10.2±2.6) (Table 1).
Table 1.
Patient statistics, injury mechanism, and fracture types
| Summary of patients’ information | |
|---|---|
| Number of patients | 36 |
| Gender | Male 16 (44.4%) |
| Female 20 (55.6%) | |
| Age | 35.3±14.6 Years (19~56) |
| Side | Right 22 (61.1%) |
| Left 14 (38.9%) | |
| Causes of injury | Sports injury 19 (52.8%) |
| Traffic accident 11 (30.6%) | |
| Fall from height 6 (16.6%) | |
| Classification | Lauge-Hansen type |
| Pronation-external rotation 22 (61.1%) | |
| Supination-external rotation 11 (30.6%) | |
| Pronation-abduction 3 (8.3%) | |
| Danis-Weber type | |
| Weber B 11 (30.6%) | |
| Weber C1 17 (47.2%) | |
| Weber C2 8 (22.2%) | |
| The time from injury to surgery | 7~14 (10.2±2.6) days |
Characteristic and principle of titanium cable isotonic annular fixation system
The titanium cable isotonic annular fixation system (Johnson & Johnson Medical Equipment, Shanghai) is essentially a modified Endobutton fixation with the titanium cable replacing the linear structure. It is easy to operate and cost effective. After reduction of the DTS, two parallel bone tunnels are built from the fibular side of the DTS. Through titanium cable and ring fixation and tightening, DTS isotonic strength is restored. This produces reliable strength and restored DTS physiologic function.
Preoperative preparation of patients
After admission, degrees of ankle swelling and soft tissue injury were evaluated. Temporary plaster fixation was performed on the affected limb, followed by elevation and bed rest to eliminate joint swelling.
Operative procedures
All patients were anesthetized with either combined spinal-epidural anesthesia or general anesthesia. They were placed in the supine position and fixed according to the fracture type: external ankle, posterior ankle, or medial malleolus. Cotton and external rotation stress tests were used to determine inferior DTS degree of injury. The cotton test is performed by fixing the distal tibia, medial malleolus, and lateral malleolus, then gently pulling the fibula outward using a pointed hook. If the movement is more than 3 mm, it indicates that the inferior tibiofibula is unstable and requires fixing. The external rotation stress test of the ankle joint was performed after ankle fracture fixation. If the tibiofibular space of X-ray film of the ankle acupoint was greater than >3 mm under fluoroscopy, it was considered unstable and DTS fixation was required. C-shaped forceps were used to temporarily reduce the DTS, and fluoroscopy was used to confirm the complete reduction. All patients with DTS fixations required closed reductions without ligament reconstruction. A 2.0 mm diameter drill was used 2-4 cm above the articular surface of the distal tibia, 25-30 degrees from posterior to anterior, through four cortical layers. The 1.0 mm titanium cable was then drilled from the fibula end to the medial tibia through four cortical channels of the DTS (Figure 1). The locker was then placed on the medial tibial margin and bandaged annularly. Throughout, dorsal extension of the ankle joint was maintained at 5-10 degrees, and the device tightened with 30-35 N of force. DTS joint fixation was confirmed by C-arm fluoroscopy and Hook experiments. Additionally, the end of locker was embedded in soft tissue to avoid irritation directly under the skin (Figure 2).
Figure 1.

Two kirschner wires during intra-operative X-ray show the fixed position and direction of the titanium cable.
Figure 2.

Surgical procedure of tibiofibular syndesmosis fixation with titanium cable. A. Determining the location and direction of titanium cable placement under fluoroscopy, and then creating the bone channel according to the location and direction of titanium cable placement. B. Titanium cable was inserted from the fibular side. C. Maintaining the ankle joint in the functional position, then tighting the titanium cable isotonic annular fixation at the tibial side. D. The condition of the titanium cable isotonic annular fixing device after tightened.
Post-operative management
All patients were administered first generation cephalosporin antibiotics to prevent infection 30 minutes before operation, non-steroidal anti-inflammatory and analgesic drugs (NSAIDs) with ice compress for 48 hours after operation to relieve swelling, low molecular weight heparin sodium subcutaneously to prevent venous thrombosis, and non-weight-bearing ankle extension and flexion exercises 24 hours after operation. Gradual weight-bearing exercises and X-rays 12 weeks after operation showed complete fracture healing and enabled clearance for bearing weight.
Follow-up and efficacy evaluation
All patients underwent ankle orthopaedic and ankle acupoint X-ray films at 1, 3, 6, and 12 months after operation, and were evaluated both clinically and radiographically. MCS, SCS and TFCS were measured 1 cm above the tibial talus joint on AP X-rays of the ankle joint to evaluate DTS integrity. Ankle function was evaluated 1, 3, 6, and 12 months after operation via American Orthopaedic Foot and Ankle Society (AOFAS) scores [19,20], and ankle flexion and extension exercises. Ankle flexion and extension evaluations were compared with the healthy side to assess functional recovery.
Statistical analysis
The data were analyzed using SPSS 18.0 statistical software. The measurements were expressed as mean ± standard deviation (x ± s). Comparisons between groups were performed using the one-way ANOVA followed by t-tests, and data counting was analyzed using χ2 tests. P-values less than 0.05 were considered as statistically significant different.
Results
In our study, nearly all patients had excellent recoveries except for three who had some inflammation and infection. For these three patients, the wound healed completely after 1 week of intravenous antibiotic administration and local radiofrequency physiotherapy. All patients were followed for 18-25 months (average 21.26±3.23 months). In this study, 13 patients had a large number of callus growth and bone healing at the fracture site 8 weeks after operation, while 22 patients had bone healing at the fracture site 12 weeks after operation. Ankle X-rays 12 months after operation showed that the fixation position of the titanium cable was adequate and there was no associated fracture or loosening. Additionally, no degeneration or traumatic arthritis was observed in ankle joints. Between the titanium cable and the tibiofibular bones, there were no incision or bone mineral density changes. None of the patients had delayed union or nonunion. The average AOFAS score was 97.42 12 months after operation. 24 hours post operation, non-weight bearing ankle joint flexion and extension exercises were performed. 8-12 weeks post operation, weight-bearing exercises were begun gradually with 10 patients walking with full load at 8 weeks, and 26 patients at 12 weeks. Remarkably, at 12 weeks, 23 patients had normal performance, 10 patients had close to normal performance, and 3 patients had slightly affected performance when compared to the healthy side (Table 2).
Table 2.
Post-operative outcomes
| Post-operative outcomes | |
|---|---|
| Mean Followup | 18-25 months (21.26±3.23) |
| Union time | 9-12 weeks (10.2±2.1) |
| Time to Full Weightbearing | 8-12 weeks (9.5±1.6) |
| Wound healing rate | A level 33 (91.7%) |
| B level 3 (8.3%) | |
| AOFAS Scoring at 12 months postoperatively | Pain Sub-Score 30 (16-38) |
| Functional 62.25 (57-65) | |
| Total 97.42 (82-100) |
During this study, we kept the abnormal parameter changes visualized in preoperative imaging within normal range. The X-ray examination at the 12-month follow-up showed no associated fracture or loosening failure of the titanium cable isotonic annular fixation, no degeneration or osteoarthritis in the ankle joint, and no changes in bone density at the bone contact site between the titanium cable and the tibiofibular bone. Typical preoperative and postoperative positive and lateral X-ray images are shown in Figures 3, 4, 5 and 6.
Figure 3.

Preoperative X-ray of a 36-year-old female patient shows distal tibiofibular syndesmosis separation.
Figure 4.

X-ray radiographs immediately after surgery shows the anatomical reduction and proper fixation of DTS.
Figure 5.

X-ray radiographs at 12 months follow-up shows no associated fracture or loosening failure of the titanium cable isotonic annular fixation, no degeneration or osteoarthritis in the ankle joint, and no changes in bone density at the bone contact site between the titanium cable and the tibiofibular bone.
Figure 6.
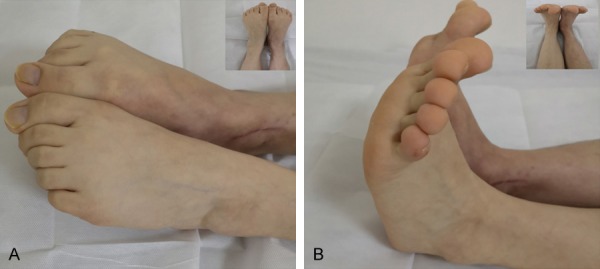
Physical examination of ankle joint at 12 months post operation shows plantar flexion (A) and consistent dorsal stretch (B) of affected and unaffected sides.
While we determined that there is no need to remove the internal fixation, 13 patients (36.11%) had removal surgery after 12 months upon their requests.
Discussion
The integrity of the DTS ligament complex is an important structure for preventing separation, rotation, and translation of the tibiofibular axis [21]. DTS injury is usually caused by trauma to the ankle joint. It usually occurs with pronation and partial supination-extroversion ankle dislocation and fracture [22]. The diagnosis of DTS separation is mainly based on preoperative X-ray. Tibiofibular space >6 mm or tibiofibular overlap <10 mm on ortho-position X-ray films, or tibiofibular overlap <1 mm on ankle acupoint X-ray films, indicates DTS separation [23,24]. Orthopaedics widely agrees on the need for surgical repair after injury. Successful treatment of DTS injury requires accurate reposition, and restoration of joint tension and stability [25,26]. Isotropic biomimetic fixation with a titanium cable system can avoid the necessary second operation for DTS screw removal. Regarding fixation strength, this method can provide sufficient DTS strength for early load-bearing activities. The DTS belongs to a fretting joint, and fatigue fracture of the fixation screw is inevitable when static fixation is employed [27,28]. Effective DTS fixation time is usually considered to be 8-12 weeks [29]. Insufficient fixation time leads to poor ligament healing, secondary widening of the tibiofibular syndesmosis space, and complications such as traumatic arthritis [30]. Delayed screw removal can cause fretting between the tibiofibular syndesmosis and loosening of the screw, which leads to screw breakage and complications such as challenging screw removal and ankle pain [31]. Some studies also suggest that early weight bearing and delayed screw removal often lead to screw breakage and associated complications [32]. Therefore, in recent years, screws are rarely used to fix inferior tibiofibular syndesmosis injury.
However, many orthopaedic doctors have recently begun to apply suture and buckle devices or annular fixation technology to the treatment of DTS, which has shown some short-term therapeutic effects [33,34]. By placing loop-type steel plates on the lateral aspects of the tibia and fibula, tightening the plates with non-absorbable wires, and elastically fixing DTS with fretting, the repair has more tension and increased durability [35-38]. However, a 12-year follow-up study showed that elastic fixators could induce local soft tissue irritation and an inflammatory reaction. In severe cases, osteolysis near implants and device loosening occurred. The incidence of complications was 27%, with 19% presenting with button irritation and 8% with infection. Only 6% of button plates needed a second operation as a result of local irritation [39].
We used a novel isotonic annular fixation of the distal tibiofibular joint to restore the function of the distal tibiofibular ligament, interosseous membrane, and isotonic strength of the distal tibiofibular joint region. After restoring DTS stability with a clamp, the tibiofibular joint was tightened and fixed with a titanium cable through 8 cortical rings using 35 N of force. Distal tibiofibular joint fixation was confirmed by C-arm fluoroscopy and HOOK test. Titanium cable tightening can restore the stability of the coronal plane of the distal tibiofibular joint, the interosseous membrane, interosseous ligament, and the anterior and posterior tibiofibular ligaments. This kind of rigid elastic fixation not only provides the effective mechanical strength fixation of the distal tibiofibular joint, but also allows for minimal joint movement [40-43].
Early weight bearing was allowed for all patients in this study. No loosening or failure of the ring fixator or re-separation of the inferior tibiofibular syndesmosis occurred during long-term follow-up. A titanium cable ring-like isotonic fixation system has the advantages of both strong screw and elastic suture fixation. Isotonic ring ligation restores the physiological and mechanical strength of the DTS, which was demonstrated as follows. First, this fixation method does not affect the fretting of the DTS, allowing patients to perform early ankle function exercises without worrying about the risk of internal plant fracture. Second, the system avoids the risk of internal plant fracture from over-tightening or over-loosening the fixation while providing adequate stability control and strength to the tibia and fibula. Third, the device restores the overall anatomical and mechanical strength of the ankle joints biomimetically by annular isotonic fixation, which allows better distal tibiofibular ligament healing. Forth, the fixation method requires only a simple, quick operation, is suitable for various types of DTS injuries, and does not require professionalism training. Fifth, patients can perform load-bearing exercises without a second surgery to remove the internal fixator, reducing patient discomfort and medical costs.
Despite the many benefits, our study also has some shortcomings. We had a small sample size, restricting statistical analysis. Secondly, the follow-up time does not allow for evaluation of long-term efficacy. Moreover, we didn’t have a surgical control group. In the future, we plan to establish a randomized controlled trial, increase our sample size, and extend our follow-up time.
Conclusions
The titanium cable isotonic annular fixation system has all the advantages of both strong screw fixation and elastic stitching. Isotonic ring ligation restores the physiological and mechanical strength of the distal tibiofibular syndesmosis. Additionally, this fixation requires only a simple operation. It is economically feasible, reliable, and produces fewer complications. It is a novel and effective option for treating DTS injuries.
Acknowledgements
We thank the members of our research group. All authors have approved the final version of the manuscript and read the journal’s authorship agreement. The research was supported by the fund of the young and middle-aged scientific research backbone cultivation project of Shenzhen People’s Hospital (NO. SYKYPY201903).
Disclosure of conflict of interest
None.
References
- 1.Davidovitch RI, Weil Y, Karia R, Forman J, Looze C, Liebergall M, Egol K. Intraoperative syndesmotic reduction: three-dimensional versus standard fluoroscopic imaging. J Bone Joint Surg Am. 2013;95:1838–1843. doi: 10.2106/JBJS.L.00382. [DOI] [PubMed] [Google Scholar]
- 2.Ebraheim NA, Mekhail AO, Gargasz SS. Ankle fractures involving the fibula proximal to the distal tibiofibular syndesmosis. Foot Ankle Int. 1997;18:513–521. doi: 10.1177/107110079701800811. [DOI] [PubMed] [Google Scholar]
- 3.Cedell C. Ankle lesions. Acta Orthop Scand. 1975;46:425–445. [PubMed] [Google Scholar]
- 4.Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures-an increasing problem? Acta Orthop Scand. 1998;69:43–47. doi: 10.3109/17453679809002355. [DOI] [PubMed] [Google Scholar]
- 5.Stark E, Tornetta P, Creevy WR. Syndesmotic instability in weber b ankle fractures: a clinical evaluation. J Orthop Trauma. 2007;21:643–646. doi: 10.1097/BOT.0b013e318157a63a. [DOI] [PubMed] [Google Scholar]
- 6.Yuen CP, Lui TH. Distal tibiofibular syndesmosis: anatomy, biomechanics, injury and management. Open Orthop J. 2017;11:670–677. doi: 10.2174/1874325001711010670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hermans JJ, Beumer A, de Jong TA, Kleinrensink GJ. Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. J Anat. 2010;217:633–645. doi: 10.1111/j.1469-7580.2010.01302.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Miller RS, Weinhold PS, Dahners LE. Comparison of tricortical screw fixation versus a modified suture construct for fixation of ankle syndesmosis injury: a biomechanical study. J Orthop Trauma. 1999;13:39–42. doi: 10.1097/00005131-199901000-00009. [DOI] [PubMed] [Google Scholar]
- 9.Miller SD. Controversies in ankle fracture treatment. Indications for fixation of stable weber type b fractures and indications for syndesmosis stabilization. Foot Ankle Clin. 2000;5:845–851. [PubMed] [Google Scholar]
- 10.Bava E, Charlton T, Thordarson D. Ankle fracture syndesmosis fixation and management: the current practice of orthopedic surgeons. Am J Orthop. 2010;39:242–246. [PubMed] [Google Scholar]
- 11.Schepers T. Acute distal tibiofibular syndesmosis injury: a systematic review of suture-button versus syndesmotic screw repair. Int Orthop. 2012;36:1199–1206. doi: 10.1007/s00264-012-1500-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cottom JM, Hyer CF, Philbin TM, Berlet GC. Treatment of syndesmotic disruptions with the Arthrex Tightrope: a report of 25 cases. Foot Ankle Int. 2008;29:773–780. doi: 10.3113/FAI.2008.0773. [DOI] [PubMed] [Google Scholar]
- 13.Teramoto A, Suzuki D, Kamiya T, Chikenji T, Watanabe K, Yamashita T. Comparison of different fixation methods of the suture-button implant for tibiofibular syndesmosis injuries. Am J Sports Med. 2011;39:2226–2232. doi: 10.1177/0363546511413455. [DOI] [PubMed] [Google Scholar]
- 14.Thornes B, Walsh A, Hislop M, Murray P, O’Brien M. Suture-endobutton fixation of ankle tibio-fibular diastasis: a cadaver study. Foot Ankle Int. 2003;24:142–146. doi: 10.1177/107110070302400208. [DOI] [PubMed] [Google Scholar]
- 15.Thornes B, Shannon F, Guiney AM, Hession P, Masterson E. Suture-button syndesmosis fixation: accelerated rehabilitation and improved outcomes. Clin Orthop Relat Res. 2005;431:207–212. [PubMed] [Google Scholar]
- 16.Forsythe K, Freedman KB, Stover MD, Patwardhan AG. Comparison of a novel fiberwire-button construct versus metallic screw fixation in a syndesmotic injury model. Foot Ankle Int. 2008;29:49–54. doi: 10.3113/FAI.2008.0049. [DOI] [PubMed] [Google Scholar]
- 17.Degroot H, Al-Omari AA, El Ghazaly SA. Outcomes of suture button repair of the distal tibiofibular syndesmosis. Foot Ankle Int. 2011;32:250–256. doi: 10.3113/FAI.2011.0250. [DOI] [PubMed] [Google Scholar]
- 18.Naqvi GA, Cunningham P, Lynch B, Galvin R, Awan N. Fixation of ankle syndesmotic injuries: comparison of tightrope fixation and syndesmotic screw fixation for accuracy of syndesmotic reduction. Am J Sports Med. 2012;40:2828–2835. doi: 10.1177/0363546512461480. [DOI] [PubMed] [Google Scholar]
- 19.Kitaoka HB, Alexander IJ, Adelaar AS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15:349–353. doi: 10.1177/107110079401500701. [DOI] [PubMed] [Google Scholar]
- 20.Ibrahim T, Beiri A, Azzabi M, Best AJ, Taylor GJ, Menon DK. Reliability and validity of the subjective component of the American orthopaedic foot and ankle society clinical rating scales. J Foot Ankle Surg. 2007;46:65–74. doi: 10.1053/j.jfas.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 21.Taser F, Shafiq Q, Ebraheim NA. Three-dimensional volume rendering of tibiofibular joint space and quantitative analysis of change in volume due to tibiofibular syndesmosis diastases. Skeletal Radiol. 2006;35:935–941. doi: 10.1007/s00256-006-0101-9. [DOI] [PubMed] [Google Scholar]
- 22.Grass R, Rammelt S, Biewener A, Zwipp H. Peroneus longus ligamentoplasty for chronic instability of the distal tibiofibular syndesmosis. Foot Ankle Int. 2003;24:392–397. doi: 10.1177/107110070302400503. [DOI] [PubMed] [Google Scholar]
- 23.Croft S, Furey A, Stone C, Moores C, Wilson R. Radiographic evaluation of the ankle syndesmosis. Can J Surg. 2015;58:58–62. doi: 10.1503/cjs.004214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Shah AS, Kadakia AR, Tan GJ, Karadsheh MS, Wolter TD, Sabb B. Radiographic evaluation of the normal distal tibiofibular syndesmosis. Foot Ankle Int. 2012;33:870–876. doi: 10.3113/FAI.2012.0870. [DOI] [PubMed] [Google Scholar]
- 25.Rammelt S, Zwipp H, Grass R. Injuries to the distal tibiofibular syndesmosis: an evidence-based approach to acute and chronic lesions. Foot Ankle Clin. 2008;13:611–633. doi: 10.1016/j.fcl.2008.08.001. [DOI] [PubMed] [Google Scholar]
- 26.Morris MW, Rice P, Schneider TE. Distal tibiofibular syndesmosis reconstruction using a free hamstring autograft. Foot Ankle Int. 2009;30:506–511. doi: 10.3113/FAI.2009.0506. [DOI] [PubMed] [Google Scholar]
- 27.Rajagopalan S, Craik JD, Lloyd J, Sangar A, Upadhyay V, Taylor HP. The financial impact of diastasis screw fixation versus tight-rope fixation of injuries to the syndesmosis with fractures of the ankle. Injury Extra. 2010;41:184. [Google Scholar]
- 28.Klitzman R, Zhao H, Zhang LQ, Strohmeyer G, Vora A. Suture-button versus screw fixation of the syndesmosis: a biomechanical analysis. Foot Ankle Int. 2010;31:69–75. doi: 10.3113/FAI.2010.0069. [DOI] [PubMed] [Google Scholar]
- 29.Elrayes M, Hammoda A. Screw versus staple in stabilization of diastasis of tibiofibular syndesmosis. Foot Ankle Surg. 2007;13:5–9. [Google Scholar]
- 30.Zhang P, Liang Y, He J, Fang Y, Chen P, Wang J. A systematic review of suture-button versus syndesmotic screw in the treatment of distal tibiofibular syndesmosis injury. BMC Musculoskelet Disord. 2017;18:286. doi: 10.1186/s12891-017-1645-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shur VB, Georgiev KG, Richards JJ. Internal compression screw exchange for reduction of distal tibiofibular syndesmotic injuries. Orthopedics. 2016;39:1–3. doi: 10.3928/01477447-20160201-06. [DOI] [PubMed] [Google Scholar]
- 32.Cottom JM, Hyer CF, Philbin TM, Berlet GC. Transosseous fixation of the distal tibiofibular syndesmosis: comparison of an interosseous suture and endobutton to traditional screw fixation in 50 cases. J Foot Ankle Surg. 2009;48:620–630. doi: 10.1053/j.jfas.2009.07.013. [DOI] [PubMed] [Google Scholar]
- 33.den Daas A, van Zuuren WJ, Pelet S, van Noort A, van den Bekerom MP. Flexible stabilization of the distal tibiofibular syndesmosis: clinical and biomechanical considerations: a review of the literature. Strategies Trauma Limb Reconstr. 2012;7:123–129. doi: 10.1007/s11751-012-0147-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Watson DJ, Weatherby BA, Womack JW. Dunking the knot in suture button fixation for distal tibiofibular syndesmosis injury: technique tip. Foot Ankle Int. 2012;33:686–688. doi: 10.3113/FAI.2012.0686. [DOI] [PubMed] [Google Scholar]
- 35.Xie B, Jing YF, Xiang LB, Zhou DP, Tian J. A modified technique for fixation of chronic instability of the distal tibiofibular syndesmosis using a wire and button. J Foot Ankle Surg. 2014;53:813–816. doi: 10.1053/j.jfas.2014.05.006. [DOI] [PubMed] [Google Scholar]
- 36.Johnson B, Kumar S, Sinha A. Comparison of outcome following operative fixation of the distal tibiofibular syndesmosis with diastasis screw and suture button techniques. Injury Extra. 2012;43:89. [Google Scholar]
- 37.Morellato J, Louati H, Bodrogi A, Stewart A, Papp S, Liew A, Gofton W. The effect of varying tension of a suture button construct in fixation of the tibiofibular syndesmosis-evaluation using stress computed tomography. J Orthop Trauma. 2017;31:103–110. doi: 10.1097/BOT.0000000000000737. [DOI] [PubMed] [Google Scholar]
- 38.Inge SY, Pull Ter Gunne AF, Aarts CAM, Bemelman M. A systematic review on dynamic versus static distal tibiofibular fixation. Injury. 2016;47:2627–2634. doi: 10.1016/j.injury.2016.09.032. [DOI] [PubMed] [Google Scholar]
- 39.Rigby RB, Cottom JM. Does the arthrex tightrope ® provide maintenance of the distal tibiofibular syndesmosis? A 2-year follow-up of 64 tightropes in 37 patients. J Foot Ankle Surg. 2013;52:563–567. doi: 10.1053/j.jfas.2013.04.013. [DOI] [PubMed] [Google Scholar]
- 40.Holmes CA, Edwards WT, Myers ER, Lewallen DG, White AA 3rd, Hayes WC. Biomechanics of pin and screw fixation of femoral neck fractures. J Orthop Trauma. 1993;7:242–247. doi: 10.1097/00005131-199306000-00008. [DOI] [PubMed] [Google Scholar]
- 41.Hitchon PW, Brenton MD, Black AG, From A, Harrod JS, Barry C, Serhan H, Torner JC. In vitro biomechanical comparison of pedicle screws, sublaminar hooks, and sublaminar cables. J Neurosurg. 2003;99:104–109. doi: 10.3171/spi.2003.99.1.0104. [DOI] [PubMed] [Google Scholar]
- 42.Schrayer A, Morris RP, Patton AG, Buford WL, Lindsey RW. A biomechanical comparison of conventional versus cable pin fixation for transverse patellar fractures. Curr Orthop Pract. 2017;28:52–57. [Google Scholar]
- 43.Li J, Wang D, He Z, Shi H. Treatment of patellar lower pole fracture with modified titanium cable tension band plus patellar tibial tunnel steel “8” reduction band. J Invest Surg. 2018;8:1–5. doi: 10.1080/08941939.2017.1417517. [DOI] [PubMed] [Google Scholar]