

ABSTRACT
The objective of this study was to analyze trends in the tuberculosis mortality rate in Brazil (1990-2015) in an ecological time-series analysis. The indicators were obtained from the Brazilian National Ministry of Health. A joinpoint regression model was applied for the temporal analysis, with a level of significance of 5%. During the period in question, there was a trend toward a reduction in mortality in the country as a whole (p < 0.001) and in each of its five regions. The states with the highest tuberculosis mortality rates were Rio de Janeiro (7.0/100,000 population) and Pernambuco (5.0/100,000 population). Eleven states and the Federal District of Brasília showed downward trends. Only the state of Alagoas showed a significant increase (p < 0.001). The temporal behavior observed indicates that tuberculosis continues to be a major public health problem in Brazil.
Keywords: Tuberculosis/epidemiology, Tuberculosis/mortality, Mortality/trends, Epidemiologic studies
RESUMO
Objetivou-se analisar a tendência da taxa de mortalidade por tuberculose no Brasil (1990-2015) em um estudo ecológico de séries temporais. Os indicadores foram obtidos do Ministério da Saúde. Aplicou-se o modelo por pontos de inflexão para a análise temporal. Houve uma tendência significativa de redução da mortalidade no Brasil (p < 0,001) e em suas cinco regiões no período estudado. Os estados com as maiores taxas foram Rio de Janeiro (7,0/100.000 habitantes) e Pernambuco (5,0/100.000 habitantes). Onze estados e o Distrito Federal apresentaram tendência de redução da taxa. Somente Alagoas mostrou um crescimento significativo (p < 0,001). O comportamento temporal verificado indica que a tuberculose ainda figura como um importante problema de saúde pública no país.
Descritores: Tuberculose/epidemiologia, Tuberculose/mortalidade, Mortalidade/tendências, Estudos epidemiológicos
Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis. It is estimated that one fourth of the world population is infected with M. tuberculosis. 1 In 2017 alone, an estimated 10 million people developed tuberculosis and 1.3 million died from the disease. Currently, tuberculosis is the leading cause of death among infectious diseases worldwide. 2 Also in 2017, a total of 72,770 new cases of tuberculosis were reported in Brazil, translating to an incidence of 35.0 cases/100,000 population. Although the Northeast and Southeast accounted for the highest number of cases (18,884 and 33,769, respectively), in terms of disease incidence, the North ranked first (46.6/100,000 population), followed by the Southeast (38.8/100,000 population). 3 , 4
This spatial heterogeneity is even more marked when rates are analyzed state by state. The state of Amazonas had the highest incidence rate in 2017 (74.7/100,000 population), whereas the state of Tocantins had the lowest (10.0/100,000). In addition, ten states had a higher incidence rate than the national average in that same year. 4
Concern about the global epidemiological scenario has led to the development of a new global strategy for fighting tuberculosis, known as End TB Strategy. 5 Proposed by the World Health Organization and approved by the World Health Assembly in 2014, this strategy proposes targets of a 90% reduction in tuberculosis incidence and a 95% reduction in tuberculosis mortality by 2035. 5
Being one of the countries with the highest incidence of tuberculosis and being in two of the three groups of priority countries-ranking 20th regarding the burden of disease and 19th regarding the tuberculosis/HIV coinfection, Brazil has formulated the “Plano Nacional pelo Fim da Tuberculose como Problema de Saúde Pública” (Brazilian National Plan to End Tuberculosis as a Public Health Problem). 6 This plan is based on three pillars of action: integrated, patient-centered care and prevention; bold policies and supportive systems; and intensified research and innovation. 6
In addition to the commitments made nationally and internationally, the relevance of studies of tuberculosis mortality lies in the fact that tuberculosis is a preventable disease. 2 , 5 , 6 Early diagnosis and appropriate treatment are imperative in this regard, because, in countries with universal health care system coverage, the proportion of people who die from tuberculosis may be less than 5%. 2 In this regard, tuberculosis mortality also indicates deficiencies in the health care system. 2 , 5
In this scenario, the study of mortality rate trends may contribute to the management of the national plan, providing supports for public health decision making, such as identification of the most vulnerable regions and of weaknesses in the disease surveillance system. Therefore, the objective of the present study was to analyze trends in the tuberculosis mortality rate in the Brazilian regions and states for the period 1990-2015.
This was an ecological time-series analysis. Mortality data were extracted from the Brazilian National Ministry of Health Mortality Database, considering codes A15 to A19 of the International Classification of Diseases, 10th revision. The following equation was utilized to calculate the indicator: number of deaths/population for the reference year × 100,000. A joinpoint regression model was applied for the temporal analysis. This model tests whether a multi-segmented line is statistically better to describe the temporal evolution of a dataset than is a straight or less-segmented line. 7 The model allows us to detect the indicator trend (whether stationary, upward, or downward) and the points where the trend changes, allowing us to calculate the annual percent change (APC) and the percent change over the entire study period, known as average annual percent change. For each trend detected, we used a 95% CI and a level of significance of 5%. The analyses were performed with the Joinpoint Regression Program, version 4.5.0.1 (National Cancer Institute, Bethesda, MD, USA).
The tuberculosis mortality rate in Brazil between 1990 and 2015 ranged from 2.2/100,000 population (in 2014) to 3.8/100,000 population (in 1994). The regression model indicated three temporal behaviors: the first one, a stationary behavior between 1990 and 1998 (APC: 0.53; 95% CI: −0.3 to 1.3; p = 0.2); the second one, a decreasing behavior between 1998 and 2003 (APC: −5.81; 95% CI: −8.0 to −3.6; p < 0.001); and the third one, also a decreasing behavior (APC: −1.88; 95% CI: −2.3 to −1.4; p < 0.001). Analysis of the entire study period showed a significant downward trend in the mortality rate in Brazil (APC: −1.9; 95% CI: −2.4 to −1.4; p < 0.001), which decreased from 3.6 deaths/100,000 population in 1990 to 2.3/100,000 population in 2015, translating to a mean rate of 3.0/100,000 population in the period in question (Figure 1).
Figure 1. Temporal evolution of mortality rate due to tuberculosis in Brazil and its regions, 1990-2015. Parameters used in the joinpoint analysis-minimum: 0; maximum: 4; selection of the model: permutation test with 4,499 replications; significance of 5%; and error autocorrelation based on data. TB: tuberculosis; pop.: population; APC: annual percent change; and AAPC: average annual percent change. *p < 0.05.
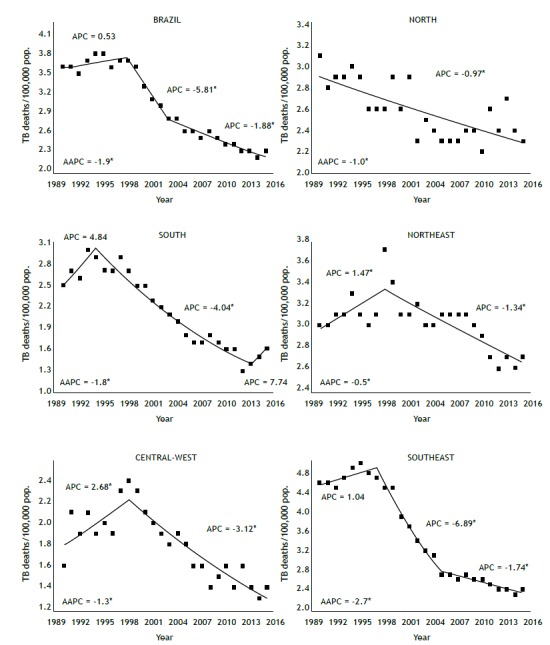
Analysis by macro-region showed that the highest mortality rates were observed in the Southeast (3.5/100,000 population) and Northeast (3.0/100,000 population). In the temporal analysis, all five regions exhibited a statistically significant decreasing behavior, with the Southeast showing the largest percent reduction (APC: −2.7; 95% CI: −3.1 to −2.2; p < 0.001) and the Northeast showing the smallest percent reduction (APC: −0.5; 95% CI: −0.9 to −0.01; Figure 1 and Table 1).
Table 1. Trends in the tuberculosis mortality rate (per 100,000 population) in all Brazilian states. Brazil, 1990-2015.
| Region/state | Mortality/100,000 population | Period | APC (95% CI) | AAPC (95% CI) | ||
|---|---|---|---|---|---|---|
| 1990 | 2015 | 1990 to 2015 | ||||
| BRAZIL | 3.6 | 2.3 | 1990-1998 | 0.5 (-0.3 to 1.3) | -1.9* (-2.4 to -1.4) | |
| 3.0 | 1998-2003 | -5.8* (-8.0 to -3.6) | ||||
| 2003-2015 | -1.9* (-2.3 to -1.4) | |||||
| North | 3.1 | 2.3 | 2.6 | 1990-2015 | -1.0* (-1.3 to -0.6) | -1.0* (-1.3 to -0.6) |
| RO | 4.4 | 1.4 | 2.5 | 1990-2015 | -4.1* (-4.9 to -3.4) | -4.1* (-4.9 to -3.4) |
| AC | 3.7 | 2.2 | 3.6 | 1990-2015 | -3.7* (-5.1 to -2.3) | -3.7* (-5.1 to -2.3) |
| AM | 3.8 | 3.3 | 3.5 | 1990-2015 | -0.4 (-0.9 to 0.1) | -0.4 (-0.9 to 0.1) |
| RR | 3.9 | 0.8 | 2.5 | 1990-2015 | -9.2* (-14.4 to -3.8) | -9.2* (-14.4 to -3.8) |
| PA | 3.0 | 2.6 | 2.5 | 1990-1996 | -6.0* (-10.0 to -1.7) | -0.6 (-1.7 to 0.5) |
| 1996-2015 | 1.1* (0.4 to 1.9) | |||||
| AP | 2.5 | 1.8 | 1.9 | 1990-2015 | -1.8* (-3.1 to -0.4) | -1.8* (-3.1 to -0.4) |
| TO | 0.3 | 0.5 | 1.1 | 1990-1992 | 126.2 (-25.3 to 585.3) | 4.4 (-4.3 to 13.8) |
| 1992-2015 | -2.4 (-4.8 to 0.0) | |||||
| Northeast | 3.0 | 2.7 | 3.0 | 1990-1998 | 1.5* (0.3 to 2.7) | -0.5* (-0.9 to -0.01) |
| 1998-2015 | -1.3* (-1.7 to -1.0) | |||||
| MA | 1.9 | 2.2 | 2.3 | 1990-2009 | 3.1* (1.9 to 4.4) | 1.1 (-0.7 to 2.9) |
| 2009-2015 | -5.1 (-11.5 to 1.8) | |||||
| PI | 2.6 | 1.4 | 2.1 | 1990-1996 | -10.1* (-17.9 to -1.5) | -1.1 (-7.4 to 5.5) |
| 1996-1999 | 27.3 (-25.9 to 118.6) | |||||
| 1999-2015 | -2.3* (-4.3 to -0.2) | |||||
| CE | 2.0 | 2.3 | 2.8 | 1990-1992 | 31.5 (-5.8 to 83.6) | 1.0 (-4.7 to 7.0) |
| 1992-1995 | -13.5 (-38.0 to 20.8) | |||||
| 1995-1998 | 17.9 (-15.5 to 64.6) | |||||
| 1998-2015 | -2.1* (-3.3 to -1.0) | |||||
| RN | 2.0 | 1.9 | 2.2 | 1990-2015 | -1.0 (-2.2 to 0.3) | -1.0 (-2.2 to 0.3) |
| PB | 1.7 | 2.2 | 2.0 | 1990-2015 | 1.1 (-0.2 to 2.5) | 1.1 (-0.2 to 2.5) |
| PE | 4.8 | 4.5 | 5.0 | 1990-1998 | 2.6* (0.7 to 4.4) | -0.3 (-1.7 to 1.1) |
| 1998-2013 | -3.0* (-3.7 to -2.2) | |||||
| 2013-2015 | 9.1 (-7.4 to 28.6) | |||||
| AL | 2.5 | 2.3 | 2.7 | 1990-2015 | 1.0* (0.2 to 1.8) | 1.0* (0.2 to 1.8) |
| SE | 2.3 | 2.0 | 2.0 | 1990-2015 | 0.0 (-0.8 to 0.9) | 0.0 (-0.8 to 0.9) |
| BA | 3.8 | 2.7 | 3.2 | 1990-2015 | -1.6* (-1.9 - -1.2) | -1.6* (-1.9 to -1.2) |
| Southeast | 4.6 | 2.4 | 3.5 | 1990-1997 | 1.0 (-0.0 to 2.1) | -2.7* (-3.1 to -2.2) |
| 1997-2005 | -6.9* (-7.9 to -5.9) | |||||
| 2005-2015 | -1.7* (-2.3 to -1.1) | |||||
| MG | 2.4 | 1.1 | 1.8 | 1990-2011 | -2.5* (-3.0 to -2.1) | -3.3* (-4.2 to -2.4) |
| 2011-2015 | -7.2* (-12.3 to -1.8) | |||||
| ES | 2.3 | 1.9 | 2.4 | 1990-1993 | 11.1 (-2.9 to 27.1) | -0.9 (-2.7 to 1.0) |
| 1993-2005 | -5.3* (-7.0 to -3.6) | |||||
| 2005-2015 | 1.1 (-1.0 to 3.3) | |||||
| RJ | 9.1 | 5.0 | 7.0 | 1990-1995 | 3.2 (-0.01 to 6.5) | -2.1* (-2.9 to -1.3) |
| 1995-2005 | -6.1* (-7.3 to -4.9) | |||||
| 2005-2015 | -0.6 ( -1.7 to 0.5) | |||||
| SP | 4.1 | 2.0 | 3.2 | 1990-1999 | 0.8 (-0.1 to 1.7) | -3.0* (-3.6 to -2.4) |
| 1999-2005 | -10.3* (-12.2 to -8.3) | |||||
| 2005-2015 | -1.8* (-2.6 to -1.1) | |||||
| South | 2.5 | 1.6 | 2.2 | 1990-1994 | 4.8 (-0.6 to 10.5) | -1.8* (-3.3 to -0.3) |
| 1994-2013 | -4.0* (-4.6 to -3.5) | |||||
| 2013-2015 | 7.7 (-8.9 to 27.4) | |||||
| PR | 2.0 | 1.1 | 1.9 | 1990-1998 | 3.8* (0.9 to 6.7) | -2.5* (-4.2 to -0.7) |
| 1998-2012 | -7.0* (-8.3 to -5.8) | |||||
| 2012-2015 | 3.6 (-8.9 to 17.9) | |||||
| SC | 1.1 | 0.8 | 1.1 | 1990-2015 | -2.1* (-2.8 to -1.3) | -2.1* (-2.8 to -1.3) |
| RS | 3.6 | 2.6 | 3.0 | 1990-1993 | 4.8 (-3.1 to 13.3) | -1.3 (-3.7 to 1.2) |
| 1993-2006 | -4.1* (-5.0 to -3.2) | |||||
| 2006-2009 | 2.7 (-12.2 to 20.2) | |||||
| 2009-2013 | -6.4 (-13.4 to 1.3) | |||||
| 2013-2015 | 13.9 (-2.6 to 33.2) | |||||
| Central-West | 1.6 | 1.4 | 1.8 | 1990-1998 | 2.7* (0.2 to 5.2) | -1.3* (-2.2 to -0.4) |
| 1998-2015 | -3.1* (-3.9 to -2.4) | |||||
| MS | 2.4 | 1.8 | 2.8 | 1990-2015 | -1.3* (-2.2 to -0.3) | -1.3* (-2.2 to -0.3) |
| MT | 2.2 | 2.2 | 3.0 | 1990-1998 | 7.0* (2.7 to 11.4) | -0.4 (-1.9 to 1.0) |
| 1998-2015 | -3.8* (-5.0 to -2.5) | |||||
| GO | 0.9 | 1.1 | 1.2 | 1990-1993 | 16.9 (-2.3 to 39.8) | 0.1 (-2.0 to 2.3) |
| 1993-2015 | -2.0* (-2.8 to -1.1) | |||||
| DF | 1.9 | 0.5 | 1.0 | 1990-2015 | -5.9* (-7.5 to -4.3) | -5.9* (-7.5 to -4.3) |
APC: annual percent change; AAPC: average annual percent change; RO: Rondônia; AC: Acre; AM: Amazonas; RR: Roraima; PA: Pará; AP: Amapá; TO: Tocantins; MA: Maranhão; PI: Piauí; CE: Ceará; RN: Rio Grande do Norte; PB: Paraíba; PE: Pernambuco; AL: Alagoas; SE: Sergipe; BA: Bahia; MG: Minas Gerais; ES: Espírito Santo; RJ: Rio de Janeiro; SP: São Paulo; PR: Paraná; SC: Santa Catarina; RS: Rio Grande do Sul; MS: Mato Grosso do Sul; MT: Mato Grosso; GO: Goiás; and DF: Distrito Federal (Federal District of Brasília).*p < 0.05.
Analysis by state showed that the highest tuberculosis mortality rates were observed in Rio de Janeiro (7.0/100,000 population) and in Pernambuco (5.0/100,000 population). Analysis of the temporal model showed that 11 states and the Federal District of Brasília exhibited a downward trend. Of those 11 states, 4 are in the North, 1 is in the Northeast, 3 are in the Southeast, 2 are in the South, and 1 is in the Central-West, as is the Federal District of Brasília. In contrast, 14 states exhibited a stationary pattern, of which 3 are in the North, 7 are in the Northeast, 1 is in the Southeast, 1 is in the South, and 2 are in the Central-West. Only the state of Alagoas exhibited an upward trend (APC: 1.0; 95% CI: 0.2-1.8; p < 0.001; Table 1).
The downward trend observed in the tuberculosis mortality rate in Brazil is consistent with the global temporal pattern. Between 2000 and 2015, tuberculosis mortality worldwide decreased by 29% in HIV-negative individuals and by 44% in HIV-positive individuals. However, this reduction is far from what is recommended in the End TB Strategy, whose targets are a 35% reduction in tuberculosis mortality by 2020 and a 90% reduction by 2035. 8 This is, therefore, a bold goal that indicates the size of the challenge faced by Brazil in reaching it.
Currently, tuberculosis/HIV coinfection is one of the most important factors contributing to tuberculosis mortality worldwide. 8 Therefore, reducing tuberculosis mortality should also involve public policies aimed at HIV detection in the population and adherence to antiretroviral therapy, given that maintaining immunological competence is essential in order not to develop tuberculosis, as well as in order to prevent death from tuberculosis. 5 , 6 , 9
Another factor that can significantly change the trends in tuberculosis mortality in Brazil is the implementation of the “Protocolo para vigilância do óbito com menção de tuberculose nas causas de morte” (Protocol for the surveillance of deaths with any mention of tuberculosis as a listed cause of death). 10 The purpose of this tool is to investigate deaths with any mention of tuberculosis among patients who were not reported to the Brazilian Tuberculosis Case Registry Database, reducing underreporting. 10 Therefore, the investigation of deaths, as recommended in the protocol, may result in an increase in tuberculosis mortality and incidence rates, reflecting a more realistic epidemiological scenario.
One of the most important factors in determining the risk of tuberculosis mortality is the direct influence of treatment dropout. 9 It is estimated that, in 2035, the tuberculosis mortality rate in Brazil will be 1.17/100,000 population without there being a change in the treatment dropout rate. 8 However, a 5% reduction in the treatment dropout rate would result in even lower mortality. Therefore, the tuberculosis mortality rate would be 0.94/100,000 population rather than 1.17/100,000 population, making it possible to achieve the global goal (i.e., a tuberculosis mortality rate < 1/100,000 population). 11 The adoption of measures that will result in reduced treatment dropout is a key imperative for reducing tuberculosis mortality.
In the analyses by state, our findings corroborate those of studies conducted in the states of São Paulo, 12 Paraná, 13 and Santa Catarina. 14 What those studies have in common is the fluctuation in mortality rates, characterized by a period of increase followed by successive periods of decline, with a stationary behavior in the last years of the time series. However, differences in rates are observed when comparing states by region. This discrepancy might reflect the influence of social inequities that act as social determinants of health and increase the risk of tuberculosis mortality. 15 In states in the North and Northeast, where there still is persistent social vulnerability, reducing mortality becomes an even greater challenge. In addition to macro-regional social issues, there are also issues related to health care itself, such as health care coordination and epidemiological surveillance activities, resulting in difficulties in tuberculosis control by states and cities. 16 - 18
Tuberculosis mortality can be influenced by the degree of integration between epidemiological surveillance activities and the care provided, especially with regard to primary care. 17 , 18 Therefore, the gap between these two components of the health care system can explain the disparities observed in state trends. In our study, the states with the highest mortality rates also showed the largest percent reductions when compared with those with the lowest rates, whose trends were stationary.
It should be noted that the present study has limitations, especially with regard to the poor quality of mortality records, including among regions. Inadequate completion of death certificates, resulting in a large number of garbage codes; difficulties in carrying out epidemiological investigations of deaths classified as having ill-defined causes; and the lack of personnel trained to perform surveillance activities are common problems found throughout Brazil, although the North and Northeast are the most affected regions. 19 Therefore, the number of deaths may be higher than that observed, especially in those regions where health surveillance faces operational problems due particularly to the lack of (human, financial, and material) resources. 19
Although many advances have been observed in tuberculosis control in recent years, 20 the temporal behavior of tuberculosis mortality rates that was observed during the period in question and the gap among states confirms that tuberculosis continues to be a major public health problem in Brazil. Therefore, regional and local strategies that can reduce tuberculosis mortality are needed. We advocate that, in order to reduce the problem, broad strategies of intervention, focused particularly on the social determinants of health, are needed.
Footnotes
Study carried out under the auspices of the Curso de Medicina, Universidade Federal de Alagoas, Campus Arapiraca, Arapiraca (AL) Brasil.
Financial support: None.
REFERENCES
- 1.Houben RM, Dodd PJ. The Global Burden of Latent Tuberculosis Infection A Re-estimation Using Mathematical Modelling. Plos Med. 2016;13(10):e1002152. doi: 10.1371/journal.pmed.1002152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.World Health Organization . Global tuberculosis report 2018. Geneva: World Health Organization; 2018. http://apps.who.int/iris/bitstream/handle/10665/274453/9789241565646-eng.pdf?ua=1 [Google Scholar]
- 3.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde . Série histórica do número de casos novos de tuberculose. Brasil, Regiões e Unidades Federadas de residência por ano diagnóstico (1990 a 2017) Brasília: o Ministério; 2018. http://portalarquivos2.saude.gov.br/images/pdf/2018/marco/19/Casos-novos-tuberculose-1990-2017-base-JAN-2018.pdf [Google Scholar]
- 4.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde . Série histórica do coeficiente de incidência de tuberculose. Brasil, Regiões e Unidades Federadas de residência por ano de diagnóstico (1990 a 2017) Brasília: o Ministério; 2018. http://portalarquivos2.saude.gov.br/images/pdf/2018/marco/19/taxa-incidencia-tuberculose-1990-2017-JAN-2018.pdf [Google Scholar]
- 5.World Health Organization . Global tuberculosis report 2015. Geneva: World Health Organization; 2015. http://apps.who.int/iris/bitstream/handle/10665/191102/9789241565059_eng.pdf?sequence=1 [Google Scholar]
- 6.Brasil. Ministério da Saúde . Brasil livre da tuberculose. Plano nacional pelo fim da tuberculose como problema de saúde pública. 1st . Brasília: Ministério da saúde; 2017. http://portalarquivos.saude.gov.br/images/pdf/2017/fevereiro/24/Plano-Nacional-Tuberculose.pdf [Google Scholar]
- 7.Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–351. doi: 10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization . Implementing the End TB Strategy: the essentials. Geneva: World Health Organization; http://apps.who.int/iris/bitstream/handle/10665/191102/9789241565059_eng.pdf?sequence=1 [Google Scholar]
- 9.Pereira AGL, Escosteguy CC, Gonçalves JB, Marques MRVE, Brasil CM, Silva MCS. Fatores associados ao óbito e ao abandono do tratamento da tuberculose em um hospital geral do município do Rio de Janeiro, 2007 a 2014. Rev Epidemiol Control Infec. 2018;8(2):150–158. doi: 10.17058/reci.v8i2.10675. [DOI] [Google Scholar]
- 10.Brasil. Ministério da Saúde . Protocolo de vigilância do óbito com menção de tuberculose nas causas de morte. Brasília: Ministério da saúde; 2017. http://portalarquivos2.saude.gov.br/images/pdf/2017/julho/12/capa_protocolo_TB_final.pdf [Google Scholar]
- 11.Brasil. Ministério da Saúde . Boletim Epidemiológico de Tuberculose. Brasília: Ministério da Saúde; 2016. http://portalarquivos2.saude.gov.br/images/pdf/2016/marco/24/2016-009-Tuberculose-001.pdf [Google Scholar]
- 12.Feitoza DS, Clares JWB, Rodrigues LV, Almeida PC. Vigilância epidemiológica no contexto do programa de controle da tuberculose limites e possibilidades. Rev Rene. 2012;13(5):1066–1074. [Google Scholar]
- 13.Cecilio HPM, Santos AL, Marcon SS, Latorre MDRDO, Mathias TAF, Rossi RM. Tuberculosis mortality trend in the state of Paraná, Brazil - 1998-2012. Cienc Saude Coletiva. 2018;23(1):241–248. doi: 10.1590/1413-81232018231.25242015. [DOI] [PubMed] [Google Scholar]
- 14.Traebert J, Ferrer GC, Nazário NO, Schneider IJ, Silva RM. Temporal trends in tuberculosis-related morbidity and mortality in the state of Santa Catarina, Brazil, between 2002 and 2009. J Bras Pneumol. 2012;38(6):771–775. doi: 10.1590/S1806-37132012000600014. [DOI] [PubMed] [Google Scholar]
- 15.Munayco CV, Mújica OJ, León FX, del Granado M, Espinal MA. Social determinants and inequalities in tuberculosis incidence in Latin America and the Caribbean. Rev Panam Salud Publica. 2015;38(3):177–185. [PubMed] [Google Scholar]
- 16.Mello FCQ, Silva DR, Dalcolmo MP. Tuberculosis where are we? J Bras Pneumol. 2018;44(2):82–82. doi: 10.1590/s1806-37562017000000450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sousa MGG, Andrade JRS, Dantas CF, Cardoso MD. Investigação de óbitos por tuberculose, ocorridos na Região Metropolitana do Recife (PE), registrados no Sistema de Informação de Mortalidade, entre 2001 e 2008. Cad Saude Colet. 2012;20(2):153–160. [Google Scholar]
- 18.Theme Filha MM, Daumas RP, Alves LC, Leimann BCQ, Engstrom EM. Análise da tuberculose em uma unidade de Atenção Primária a Saúde na cidade do Rio de Janeiro perfil clínico, resultado de tratamento e qualidade dos registros. Cad Saude Colet. 2012;20(2):169–176. [Google Scholar]
- 19.IshitaniI LH, Teixeira RA, Abreu DMX, Paixão LMMM, França EB. Quality of mortality statistics' information garbage codes as causesof death in Belo Horizonte, 2011-2013. Rev Bras Epidemiol. 2017;20(Suppl 1):34–45. doi: 10.1590/1980-5497201700050004. [DOI] [PubMed] [Google Scholar]
- 20.Duarte R, Silva DR, Rendon A, Alves TG, Rabahi MF, Centis R. Eliminating tuberculosis in Latin America making it the point. J Bras Pneumol. 2018;44(2):73–76. doi: 10.1590/S1806-37562017000000449. [DOI] [PMC free article] [PubMed] [Google Scholar]