

SUMMARY
Height intolerance often includes various clinical conditions ranging from physiological height instability, which is a common condition, to acrophobia, considered to be a specific phobia in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V). Visual dependence is commonly reported in patients with height intolerance, and physiological mechanisms may include conflicting information from visual cues on one hand and vestibular-proprioceptive cues on the other. This study examines the physiological mechanisms underlying height intolerance and phobic-cognitive mechanisms leading to more severe clinical manifestations (i.e. acrophobia). Diagnosis mainly relies on history, while the use of specific questionnaires has been proposed in a clinical setting. Treatment includes physical therapy with the purpose of habituation to the condition; on the other hand, psychological disorders should be considered and treated. Finally, our own experience in treating patients with height intolerance is included. In a sample of 164 acrophobic patients with imbalance lasting for at least 6 months, a prevalence of females was found (59.7%); among comorbidities, motion sickness (51.8%), migraine (50.6%) and panic disorders (18.9%) were reported. Interestingly, acrophobia always preceded the first panic attack.
KEY WORDS: Fear of height, Height intolerance, Acrophobia, Vestibular system, Phobic disorders
RIASSUNTO
Il termine “mal d’altezza” comprende spesso condizioni cliniche differenti che vanno dalla fisiologica instabilità, che può essere considerata una condizione comune, all’acrofobia, che è stata inclusa tra le forme fobiche specifiche nella quinta edizione del Manuale Diagnostico e Statistico dei Disturbi Mentali (DSM-V). Una dipendenza dalle informazioni visive è comunemente descritta nei pazienti con mal d’altezza; i meccanismi fisiologici alla base del disturbo potrebbero essere le informazioni contrastanti provenienti dal sistema visivo da un lato e propriocettivo-vestibolare dall’altro. Il nostro studio esamina le pubblicazioni relative ai meccanismi fisiologici che producono il mal d’altezza e ai disturbi di tipo fobico-cognitivo che producono le manifestazioni cliniche più severe (i.e. acrofobia). La diagnosi si basa essenzialmente sulla storia clinica e l’uso di questionari specifici è stato proposto come il migliore metodo di indagine. Il trattamento comprende una fisioterapia specifica con lo scopo di abituare il paziente alla condizione; d’altro canto i disturbi psicologici che producono i quadri clinici più severi devono essere indagati e trattati. Infine, abbiamo incluso la nostra esperienza clinica sull’argomento. In un campione di 164 pazienti acrofobici e con instabilità presente da almeno 6 mesi, abbiamo trovato una prevalenza del sesso femminile (59,7%); tra le comorbidità la cinetosi (51,8%), l’emicrania (50,6%) e le patologie da panico (18,9%) erano i più comuni. Può essere rilevante notare come in questi soggetti l’acrofobia abbia sempre preceduto il primo attacco di panico.
PAROLE CHIAVE: Vertigine da altezza, Intolleranza all’altezza, Acrofobia, Sistema vestibolare, Disordini fobici
Introduction
Height vertigo or visual intolerance to height refers to psychological, neurovegetative and behavioural disorders that affect predisposed individuals following exposure to height. It is the core part of a spectrum of manifestations ranging from physiological instability to height and acrophobia 1 The predisposing factor is thought to be conflicting information arising from vestibular, somatosensory and visual cues when there is an excessive distance of the stationary reference frame at the periphery of the visual field preventing perception of the body’s oscillations, which is required for locomotion and to maintain an upright position; psychological factors may also play a role in the disorder 2. It affects about a third of the general population, and in about half of cases significantly impacts the quality of life. It can be treated with appropriate recommendations or with proper rehabilitation, psychotherapy and drugs 3.
The research was performed on PUBMED and SCOPUS. To clarify our selection criteria a flowchart is shown (Fig. 1).
Fig. 1.
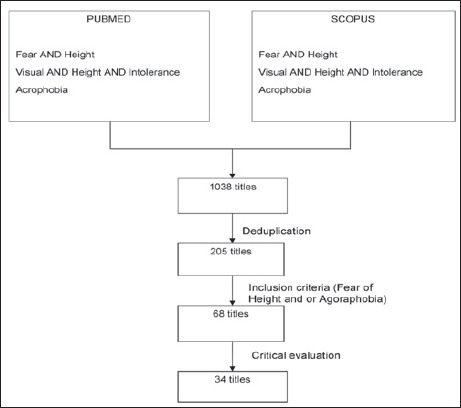
Search strategy flowchart.
A proposed physiological mechanism for height intolerance
Correct postural control and correct spatial orientation are essential requirements for human survival and are the result of an evolutionary pathway that started around 6 million years ago when we gained the upright position. It requires univocal information from vestibular, somatosensory (tactile and proprioceptive) and visual cues. The tactile component is mainly represented by pressure sensors on the sole of the foot, providing information on how the foot approaches the ground, while the proprioceptive component, represented by the musculotendinous and articular receptors, informs us on the relationships between the different parts of our body (trunk, neck, limbs). The vestibular system works as a sensor for head accelerations and, more importantly, as a sensor for gravity. The visual system, both foveal and peripheral, gives us information about the external environment: the shape, size, distance and movements of the objects around us and movements of our head in the visual scene 1.
When we stand still in a static environment, our postural control is maintained through continuous small oscillations laterally and back to front. In this situation, visual information overcomes somatosensory and vestibular information, reducing oscillations by 50-100% 4.
In order to detect the displacement of an object by the eye, the image must slide on the peripheral retina by at least 20’ of arc. Knowing that we oscillate about 2 cm laterally under normal conditions, the 20’ of arc threshold is reached in a static field of view at a distance less than 3 m. If this distance increases, the amplitude of the retinal slip is reduced with resulting conflicting information between the somatosensory and vestibular systems on the one hand, perceiving our oscillations, and the visual system on the other, perceiving a static visual field 3-7. This is what physiologically happens when there are no static reference points near our field of vision, as on a mountain or on a roof or on a terrace of a tall building 2. This conflicting situation can be avoided or reduced by increasing the amplitude of postural sways in order to increase visual control. It has been calculated that the amplitude of sways of our body cannot exceed 10 cm, corresponding to a height of 20 m, which represents the threshold beyond which one is not able to maintain an upright position and increases the risk of falls 3.
The reduction or loss of visual information to postural control in all individuals (100%) provokes a variable amount of instability that can be considered physiological and defined as physiological visual instability at height. In susceptible individuals (around 30% of the general population), the same condition generates a state of discomfort and anxiety with neurovegetative and motor symptoms. This condition is considered to be pathological and is called height vertigo or visual intolerance to height. Finally, in 6.4% of the general population (8.6% of women vs 4.1% of men), this condition is so unpleasant that it becomes a genuine phobia, as defined according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V), requiring treatment: acrophobia or fear of height 8-10.
On the other hand, some individuals, known as risk takers/risk seekers, take pleasure from the feeling of danger linked to exposure to height and the resultant release of catecholamines, and look for it voluntarily 11.
Epidemiology
Height intolerance affects 28.5% of the general population; it is more common in women (32.4%) than in men (24.5%); it can begin at any age, but manifests more frequently (30%) in the second decade of life with the highest prevalence being observed in women during the fifth decade 5. It often has a familiar trait and is correlated with migraine, motion sickness, anxiety disorders and depression 12.
After initial onset, it can spontaneously improve in 31% of cases, persist unchanged in 52% and worsen in 13% 5.In about half of cases, it becomes clinically significant and considerably impacts the quality of life. In more than 20% of cases, it can cause panic attacks and in 6.4% of cases, it worsens significantly to become acrophobia 5-7. A recent study focused on general phobic aspects of height intolerance using the General Self-Efficacy Scale, a 10-item psychometric scale designed to assess optimistic self-beliefs to cope with a variety of difficult demands in life. In it, the authors demonstrated an association between this scale and height intolerance 13. Primary school children can be affected by height intolerance, although it usually remits within a few years, possibly facilitated by repeated exposure to the triggering situations 14. An overlap with agoraphobia has been supposed, possibly based on commonly shared pathophysiological mechanisms (i.e. increased visual dependence in postural control) 15. Specific phobias are more frequently associated with higher alcohol consumption; on the other hand, a recent questionnaire-based study did not provide evidence of an association in subjects with height intolerance 16.
Clinical features: symptoms, signs and diagnosis
Looking down from a tower or from the roof or from the balcony of a tall building, climbing or descending a ladder, walking on a bridge or on a mountain, climbing, walking on a ridge or on an exposed path, travelling on a cable car or a chairlift are all conditions that can cause height vertigo 5.
The intensity of the disorder is strongly correlated to body position: it is highest when standing, it decreases when sitting or bending the knees and becomes minimal or disappears when lying down in the prone position. Vestibular, neurological or visual disorders reducing visual acuity from afar can increase the disorder 3. It is more likely to manifest in some environmental situations that interfere with vision such as fog or semi-darkness, with some tactile and proprioceptive signals such as slippery ground, and with specific vestibular stimulations such as hyperextension of the head, which moves the macular receptors into an unnatural position. On the other hand, the somatosensory afferents that arise from leaning against a wall with your back or your side, the tactile stimulation of the hand touching a banister or a firm solid structure can relieve it. The same applies to the presence of nearby stationary reference points that are visible on the periphery of our visual field. In any case, the psychological attitude of the subject plays a lead role in the genesis of visual intolerance to height because the level of anxiety and fear of the void can overestimate height perception when looking from above 17.
The disorders arise in predisposed individuals from the interplay of postural and eye-gaze changes in a threatening situation with psychological factors. In fact, physiological postural reactions may be recorded in healthy subjects when exposed to height even if virtual 18. According to some authors, subjects with a fear of heights are probably more prone to rely on visual information in postural control, compared to normal subjects. When exposed to optokinetic visual stimuli, they exhibit higher anxiety and an increased body sway 19. Subjects with height vertigo present an alteration of the standing position and gait, and of head and eye movements that are essential in exploring the surroundings. In an experimental setting, it has been demonstrated that exposure to height provokes changes in postural control, mainly increasing co-contraction of leg muscles; moreover, the severity of these changes correlates with anxiety 20. Similarly, subjects with height intolerance walked more slowly on a 15 metre balcony, with reduced cadence and stride length; no changes were recorded when subjects performed the test walking with upward gaze or with eyes closed 21.
Likewise, changes in visual exploration have been demonstrated during height exposure. Individuals with height intolerance exhibit fewer and smaller amplitude eye-in-head saccades with a longer fixation time than in less susceptible subjects. Moreover, spontaneous head movements were reduced with all three dimensions equally affected. Gaze-in-space, which expresses the ability to explore the surroundings by coordinated eye-head movements, covered a smaller total area of the visual scene 8,22,23. A recent paper showed that the height condition affects optokinetic gain, which was increased, and smooth pursuit, supporting neuro-anatomical evidence of threat-related mechanisms influencing both oculomotor nuclei and vestibular reflex pathways; the authors emphasise how anxiety and cognitive activity may play a role in the performance of eye movements 24. Their results agree with the findings of previous studies, underlining the interference of fear on postural control and eye movements 11,25.
It could be argued that, as a consequence of these changes, subjects with height intolerance exhibit a more cautious, slow and rigid gait with reduced speed and length of steps when exposed to the triggering condition; saccades are reduced in number and amplitude, they last longer and are mainly directed on the horizontal plane. Spontaneous movements of the head are greatly reduced in number and speed in all directions and, consequently, the gaze-in-space, which represents an indicator of eye-head movement coordination, covers a smaller area of the visual field and is strictly directed (frozen) toward the horizon. Changes of gait and eye movements are often associated with distress and neurovegetative symptoms 26.
Since there is no conclusive test to diagnose height intolerance and its impact on quality of life, clinical history and above all, questionnaires are, at present, the best choice for this purpose. For evaluation of symptoms, they must be predictive of subjective dizziness, psychological distress and avoidance 27,28.
Treatment
When height intolerance becomes more severe and presents a considerable impact on quality of life, it can be included among phobias (acrophobia) based on DSM-V criteria 10 and must be treated accordingly with pharmacotherapy, psychotherapy and behavioural therapy.
Fortunately, the most common presentation of visual intolerance to height is of little clinical relevance and mostly requires suggestions and recommendations, such as avoiding exposure to heights and certain sports like climbing or mountaineering, to manage both the neurophysiological and psychological aspects of the disturbance. However, if a susceptible individual is exposed to height, some practical advice might be sufficient, such as to stop walking, to sit or lie down, to avoid looking down or far away but to fix on stable and nearby structures or to close the eyes, to reduce movement or hyperextension of the head, to lean against a fixed support even if only with the hand, to avoid wearing multifocal glasses or ski goggles, which prevent lateral peripheral vision, and to be mentally engaged in some cognitive tasks to shift attention from the apprehension of a possible fall 8,11.
Only more complex cases need rehabilitative therapy. Based on the visual dependence of these subjects, some authors have proposed exercise protocols not so different from those used in patients with agoraphobia and based on habituation; the phobic component must also be considered and treated with cognitive behavioural therapy 29-32.
Recent papers have focused on the possibility of using virtual reality in the habituation techniques, as well as using hypnosis, and these might offer an opportunity to decrease the phobic-cognitive disorders of more complex cases 33,34.
Conclusions
Height vertigo or visual intolerance to height is a very common syndrome that manifests in susceptible individuals following exposure to height that has been described since ancient times. Its relationship with vestibular disorders, in particular with persistent postural perceptual dizziness (PPPD), is still matter of debate.(35,36) It mainly presents with fear of falling or losing equilibrium, neurovegetative symptoms, reduced visual exploration and generalised contraction of antigravity muscles with a rigid and cautious attitude to standing position and gait. It originates from the interaction between psychological factors, mainly anxiety, and organic factors, such as the intersensorial conflict between visual, vestibular and somatosensory systems involved in postural control. It lies in the middle of a spectrum of disorders related to height exposure ranging from physiological visual instability to height up to acrophobia or fear of heights. Further research will allow a better understanding of the mechanisms behind this complex disorder that strongly impacts on daily activities, on interpersonal relationships, and on overall quality of life.
Our experience
In order to assess comorbidities and clinical vestibular signs, among the records of 4850 outpatients who attended the tertiary Centre for Vestibular Disorders of San Raffaele Hospital between 2006 and 2017, we found 164 subjects referring fear of height and chronic dizziness without a lifetime history of vertigo of any kind. The inclusion criterion was the presence of both disorders for at least 6 months before consultation. Subjects were included if they experienced fear of height interfering with the activities of everyday life, such as standing on a ladder or a chair; moreover, they should have referred a persistent sensation of rocking or swaying, unsteadiness and/or dizziness without vertigo that had been present at least for the last 6 months. The age of onset of both disorders was noted. The mean age of the sample was 41.5 ± 8.7 years. Ninety-eight (59.7%) were female. A full clinical history was collected before examination, in particular for motion sickness, lifetime history of migraine and panic disorders (PD). Clinical examination included otoscopy, audiometric exam, Head Impulse test (from November 2013, a video HIT was performed), full bedside examination with video Frenzel, including positional tests, head shaking test and a 100 Hz vibratory test. Moreover, a static stabilometric exam (S.Ve.P - Amplaid) was performed. Results were compared with those of 100 normal subjects chosen to overlap for age and sex with controls (mean age 42 ± 7, 60 females). The severity of dizziness was measured by the 25-item Dizziness Handicap Inventory scale, validated Italian version, which generated a total score (range zero to 100) indicating the patient’s self-perceived level of handicap associated with the dizziness 37,38. DHI was further subdivided into physical (ranging from 0 to 28 points), functional (ranging between 0 and 36 points) and emotional (ranging from 0 to 36 points) subscores. A higher score indicates a more severe handicap.
Among comorbidities, lifetime episodes of headaches with migrainous features (pulsatile, associated with phonophobia and photophobia, lasting for more than 4 hours and worsening on exertion) were reported by 83 of 164 (50.6%) subjects; it was more frequent in females, since 59 of 98 females (60.2%) reported it, whereas 24 of 66 males (36.4%) reported it. Previous episodes of panic attacks requiring therapy were reported by 31 subjects (18.9%), with no difference between the two sexes, since 19 of 98 females (19.4%) and 12 of 66 males (18.2%) referred it. An association was found between migraine and panic disorders (PD) since among 83 migraineurs, 28 reported panic disorders whereas only 3 of 81 non-migraineurs reported them (χ2 = 12.9, p = 0.0003). Among 31 PD subjects, fear of height preceded the first panic attacks in all subjects.
Eighty-five (51.8%) subjects reported motion sickness as children, while 59 (36.0%) still suffered from it as adults.
Finally, vestibular bedside examination was negative in 132 subjects. A long-lasting smooth bipositional apogeotropic or geotropic nystagmus was found in 18 subjects (11.0%), a positive skull vibration test in 12 subjects (7.1%) and a positive head shaking test in 2 patients (1.2%); 3 subjects presented both a bipositional nystagmus and a vibration-induced nystagmus.
Results of static stabilometry are summarised in Table I.
Table I.
Values of stabilometric parameters Length (L) and Surface (S) in the two groups in the tested conditions: eyes open (eo) and eyes closed (ec). Values are expressed as mean ± standard deviation. Length is expressed in millimeters while Surface in squared millimeters. A quotient has been calculated for the value of Leo/Lec.
| Controls (n = 100) | Patients (n = 164) | Statistical analyses | |
|---|---|---|---|
| Length eyes open | 195 ± 36 | 202 ± 58 | n.s. |
| Length eyes closed | 302 ± 44 | 449 ± 65 | .0001 |
| Surface eyes open | 186 ± 34 | 198 ± 39 | .01 |
| Surface eyes closed | 239 ± 47 | 376 ± 55 | .0001 |
| Q (Leo/Lec) | 64 ± 5 | 45 ± 4 | .0001 |
Stabilometric findings demonstrated increased values of parameters in patients above all in eyes closed conditions, underlining an increased dependence on visual cues. Results of the DHI questionnaire are reported in Table II.
Table II.
Values of the Dizziness Handicap Inventory total score and subscales in patients (n = 164).
| DHI total score | DHI subscales | ||
|---|---|---|---|
| Emotional | Physical | Functional | |
| 24.7 ± 9.4 | 6.4 ± 2.6 | 6.3 ± 2.6 | 11.9 ± 4.8 |
The DHI comprises 25 items; with a total score ranging between 0 and 100 points.
Although our results are far from being conclusive, comparing the prevalence of comorbidities with previous studies on the general population, some conclusions can be drawn. Above all in our sample, the frequency of migraineurs (50.6%) was higher than in a previous study, which reported a prevalence of 18.2% among females and 6.5% among males 39. In the same way, PD was most represented among our subjects than in the general population, in which a previous study estimated the prevalence to be in a range from 1.4% to 2.9% 40. On the other hand, it should be considered that a possible bias may arise from our inclusion criteria, since our subjects presented fear of height interfering with their daily activities and also reported chronic dizziness, so it can be argued that they presented acrophobia in a burden of symptoms of PPPD.
Figures and tables
Footnotes
Conflict of interest statement
None declared.
References
- 1.Bronstein AM, Brandt T, Woollacott M. Clinical disorders of balance, posture and gait. London: Arnold; 1996. [Google Scholar]
- 2.Brandt T, Bles W, Arnold F, et al. Height vertigo and human posture. Adv Otorhinolaryngol 1979;25:88-92. [DOI] [PubMed] [Google Scholar]
- 3.Brandt T, Arnold F, Bles W, et al. The mechanism of physiological height vertigo. I. Theoretical approach and psychophysics. Acta Otolaryngol 1980;89:513-23. https://doi.org/10.3109/00016488009127169. [DOI] [PubMed] [Google Scholar]
- 4.Bles W, Kapetyn TS, Brandt T, et al. The mechanism of physiological height vertigo. II. Posturography. Acta Otolaryngol 1980;89:534-40. https://doi.org/10.3109/00016488009127171. [DOI] [PubMed] [Google Scholar]
- 5.Huppert D, Grill E, Brandt T. Down on heights? One in three has visual height intolerance. J Neurol 2013;260:597-604. https://doi.org/10.1007/s00415-012-6685-1. [DOI] [PubMed] [Google Scholar]
- 6.Brandt T, Huppert D. Fear of heights and visual height intolerance. Curr Opin Neurol 2014;27:111-7. https://doi.org/10.1097/WCO.0000000000000057. [DOI] [PubMed] [Google Scholar]
- 7.Nakahara H, Takemori S, Tsuruoka H. Influence of height on the spatial orientation and equilibrium of the body. Otolaryngol Head Neck Surg 2000;123:501-4. https://doi.org/10.1067/mhn.2000.107316. [DOI] [PubMed] [Google Scholar]
- 8.Brandt T, Kugler G, Schniepp R, et al. Acrophobia impairs visual exploration and balance during standing and walking. Ann N Y Acad Sci 2015;1343:37-48. https://doi.org/10.1111/nyas.12692. [DOI] [PubMed] [Google Scholar]
- 9.Brandt T, Benson J, Huppert D. What to call “non phobic” fear of heights? Br J Psychiatry 2012;190:81 https://doi.org/10.1192/bjp.190.1.81a. [Google Scholar]
- 10.American Psychiatric Association. Diagnostic and statistical manual of mental disorders. DSM-5. Fifth Edition Washington, DC: American Psychiatric Association Publishing; 2013. [Google Scholar]
- 11.Salassa JR, Zapala DA. Love and fear of heights: the pathophysiology and psychology of height imbalance. Wilderness Environ Med 2009;20:378-82. https://doi.org/10.1580/1080-6032-020.004.0378. [DOI] [PubMed] [Google Scholar]
- 12.Kapfhammer HP, Huppert D, Grill E, et al. Visual height intolerance and acrophobia: clinical characteristics and comorbidity patterns. Eur Arch Psychiatry Clin Neurosci 2015;265:375-85. https://doi.org/10.1007/s00406-014-0548-y. [DOI] [PubMed] [Google Scholar]
- 13.Grill E, Schäffler F, Huppert D, et al. Self-efficacy beliefs are associated with visual height intolerance: a cross-sectional survey. PLoS One 2014;9:e116220 https://doi.org/10.1371/journal.pone.0116220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Huppert D. [Fear of heights in primary school children]. Fortschr Neurol Psychiatr 2016;84:134-6. https://doi.org/10.1055/s-0042-103424. [DOI] [PubMed] [Google Scholar]
- 15.Davey GC, Menzies R, Gallardo B. Height phobias and biases in the interpretation of bodily sensations: some links between acrophobia and agoraphobia. Behav Res Ther 1997;35:997-1001. [DOI] [PubMed] [Google Scholar]
- 16.Huppert D, Grill E, Kapfhammer HP, et al. Fear of height and mild visual height intolerance independent to alcohol consumption. Brain Behav 2013;3:596-601. https://doi.org/10.1002/brb3.162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stefanucci JK, Proffitt DR. The roles of altitude and fear in the perception of height. J Exp Psychol Hum Percept Perform 2009;35:424-38. https://doi.org/10.1037/a0013894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cleworth RW, Chua R, Inglis TJ, et al. Influence of virtual height exposure on postural reactions to support surface translations. Gait Posture 2016;47:96-102. https://doi.org/10.1016/j.gaitpost.2016.04.006. [DOI] [PubMed] [Google Scholar]
- 19.Hüweler R, Kandil FI, Alpers GW, et al. The impact of visual flow stimulation on anxiety, dizziness and body sway in individuals with and without fear of heights. Behav Res Ther 2009;47:345-52. https://doi.org/10.1016/j.brat.2009.01.011. [DOI] [PubMed] [Google Scholar]
- 20.Wuehr M, Kugler G, Schniepp R, et al. Balance control and anti-gravity muscle activity during the experience of fear at heights. Physiol Rep 2014;2:e00232 https://doi.org/10.1002/phy2.232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schniepp R, Kugler G, Wuehr M, et al. Quantification of gait changes in subjects with visual height intolerance when exposed to heights. Front Hum Neurosci 2014;8:963 https://doi.org/10.3389/fnhum.2014.00963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kugler G, Huppert D, Schneider E, et al. Fear of heights freezes gaze to the horizon. J Vestib Res 2014;24:433-41. https://doi.org/10.3233/VES-140529. [DOI] [PubMed] [Google Scholar]
- 23.Kugler G, Huppert D, Eckl M, et al. Visual exploration during locomotion limited by fear of heights. PLoS One 2014;9:e105906 https://doi.org/10.1371/journal.pone.0105906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Naranjo EN, Cleworth TW, Allum JHJ, et al. Threat effect on human oculo-motor function. Neuroscience 2017;359:289-98. https://doi.org/10.1016/j.neuroscience.2017.07.024. [DOI] [PubMed] [Google Scholar]
- 25.Boffino CC, de Sá CS, Gorenstein C, et al. Fear of heights: cognitive performance and postural control. Eur Arch Psychiatry Clin Neurosci 2009;259:114-9. https://doi.org/10.1007/s00406-008-0843-6. [DOI] [PubMed] [Google Scholar]
- 26.Coelho CM, Wallis G. Deconstructing acrophobia, physiological and psychological precursors to developing a fear of height. Depress Anxiety 2010;27:864-70. https://doi.org/10.1002/da.20698. [DOI] [PubMed] [Google Scholar]
- 27.Steinman SA, Teachman BA. Cognitive processing and acrophobia: validating the heights interpretation questionnaire. J Anxiety Disord 2011;25:896-902. https://doi.org/10.1016/j.janxdis.2011.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Huppert D, Grill E, Brandt T. A new questionnaire for estimating the severity of visual height intolerance and acrophobia by a metric interval scale. Front Neurol 2017;8:211 https://doi.org/10.3389/fneur.2017.00211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Arroll B, Henwood SM, Sundrama FI, et al. A brief treatment for fear of heights: A randomized controlled trial of a novel imaginal intervention. Int J Psych Med 2017;52:21-33. https://doi.org/10.1177/0091217417703285. [DOI] [PubMed] [Google Scholar]
- 30.Arroll B, Wallace HB, Mount V, et al. A systematic review and meta-analysis of treatments for acrophobia. Med J Aust 2017;206:263-7. [DOI] [PubMed] [Google Scholar]
- 31.Whitney SL, Jacob RG, Sparto PJ, et al. Acrophobia and pathological height vertigo: indications for vestibular physical therapy? Phys Ther 2005;85:443-58. [PubMed] [Google Scholar]
- 32.Dreyer-Oren SE, Clerkin EM, Edwards CB, et al. Believing is seeing: changes in visual perception following treatment for height fear. J Behav Ther Exp Psychiatry 2019;62:1-6. https://doi.org/10.1016/j.jbtep.2018.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Coelho CM, Walters AM, Hine TJ, et al. The use of virtual reality in acrophobia research and treatment. J Anxiety Disord 2009;23:563-74. https://doi.org/10.1016/j.janxdis.2009.01.014. [DOI] [PubMed] [Google Scholar]
- 34.Hirsch JA. Integrating hypnosis with other therapies for treating specific phobias: a case series. Am J Clin Hypn 2018;60:367-77. https://doi.org/10.1080/00029157.2017.1326372. [DOI] [PubMed] [Google Scholar]
- 35.Bisdorff A, von Brevern M, Lempert T, et al. Classification of vestibular symptoms: Towards an international classification of vestibular disorders. J Vestib Res 2009;19:1-13. https://doi.org/10.3233/VES-2009-0343. [DOI] [PubMed] [Google Scholar]
- 36.Staab JP, Eckhardt-Henn A, Horii A, et al. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Barany Society. J Vestib Res 2017;27:191-208. https://doi.org/10.3233/VES-170622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Jacobson GP, Newman CW. The development of the Dizziness Handicap Inventory. Arch Otolaryngol Head Neck Surg 1990;116:424-7. [DOI] [PubMed] [Google Scholar]
- 38.Nola G, Mostardini C, Salvi C, et al. Validity of Italian adaptation of the Dizziness Handicap Inventory (DHI) and evaluation of the quality of life in patients with acute dizziness. Acta Otorhinolaryngol Ital 2010;30:190. [PMC free article] [PubMed] [Google Scholar]
- 39.Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache 2001;41:646-57. [DOI] [PubMed] [Google Scholar]
- 40.Weissman MM, Bland RC, Canino GJ, et al. The cross-national epidemiology of panic disorder. Arch Gen Psychiatry 1997;54:305-9. https://doi.org/10.1001/archpsyc.1997.01830160021003. [DOI] [PubMed] [Google Scholar]