

Abstract
Background:
Many patients on maintenance hemodialysis experience sleep disorders. This problem is related to depression, anxiety, hospitalizations, chronic medical conditions, decreased quality of life, and increasing mortality rate in patients on maintenance hemodialysis. The objective of this research is to determine the impact of massage therapy by hot stone on quality of sleep in patients on maintenance hemodialysis.
Materials and Methods:
This was a randomized controlled trial conducted on 60 patients on maintenance hemodialysis. They were assigned via random allocation process into two groups of study: intervention group (n = 30), or control group (n = 30). Patients in the experimental group received massage therapy by hot basalt stone for 12 séances. During the massage therapy, each of five basalt stones were placed at the sites of the fifth, fourth, third, second, and first chakra. Control group received their treatment as usual without any massage therapy. Using Pittsburgh Sleep Quality Index (PSQI), the global score and its components were computed in both groups of study, two times (before the intervention and 1 month after the intervention).
Results:
Although there were not any baseline differences between the two groups of study for the mean of global PSQI score (P = 0.92) before the study, the mean of global PSQI score in the intervention group, after the intervention decreased to 5.7 ± 3.06, but in the control group sleep quality increased to 10.7 ± 3.6. The difference between the mean of global score of PSQI among two groups of study after the massage therapy was statistically significant (P < 0.001).
Conclusion:
Applying massage therapy by hot stone in hemodialysis patients may contribute in enhancing their quality of sleep.
Keywords: Complementary, hemodialysis, massage, sleep
INTRODUCTION
Chronic kidney disease is a serious health problem all over the world. The progression of chronic renal failure toward end-stage renal disease is increasing.[1] It is reported that the rate of mortality in chronic hemodialysis is 7–8 times greater than the general population.[2]
Sleep is a dynamic behavior state that seriously influences waking periods and contributes to the mental and physical health status.[3] Poor quality of sleep can disturb motivation, thoughts, and emotions. Patients with decreased quality of sleep show many physical and psychological symptoms, such as difficulty concentrating, fatigue, low pain threshold, loss of appetite, nervousness, depression, and anxiety.[4] Sleep disorders are not only associated with poor quality of life but also related to increased number of health risks, and death in these patients.[5]
Patients with renal disease have various forms of sleep disorders.[6] The prevalence of sleep problems in these people varies from 50% to 80%.[7] Many factors such as bone pain, systolic and diastolic blood pressure, high blood urea and blood creatinine levels, parathyroid hormone level, increase the prevalence of sleep disorders in hemodialysis patients.[4] An evidence has shown that sleep-disordered breathing may be a risk factor for renal disease.[8]
Complementary and alternative medicine (CAM) includes systems and practices that are not presently a part of conventional medicine.[9] Massage therapy is known as a form of manipulative and body-based category of CAM, as determined by the American National Center for CAM.[10] Massage is a general term for rubbing, pressing, and manipulating the skin, muscles, tendons, and ligaments. Massage therapist usually use their hands and fingers for massage. The various forms of massage are aroma therapy massage, trigger point massage, deep massage, Swedish massage, sports massage, and hot-stone massage. Massage may range from light stroking to deep pressure.[11]
Although the action mechanisms of massage therapy are unknown, various physiological responses to massage therapy have been reported. Massage seems to produce local biochemical changes, which might lead to increased neural activity at the spinal cord level and subcortical nuclei, which might affect pain perception and mood. Therefore, massage therapy could potentially decrease pain, anxiety, and depression by serotonin and endorphins increasing.[12] Stimulation of acupuncture points through massage has shown to induce many physiological effects such as activation of the autonomic nervous system and decreasing anxiety level.[13]
Massage therapy by hot stone incorporates placing heated basalt stones on the specific points of the body. This therapy is a form of massage-therapy practice in such a way that massage therapist may hold the heated stone (s), apply massage oil as a lubricant, and then use them to administer massage treatment. Although applying hot-stone therapy in the massage industries over the world is prevalent, few researches on hot-stone therapy are available.[14] Based on our knowledge, no study has examined the impact of massage therapy by hot-stone on sleep quality in hemodialysis patients. So that, the objective of this research was to determine the effect of hot-stone massage therapy on quality of sleep in hemodialysis patients. We hypothesized massage therapy by hot stone would enhance sleep quality in the experimental group.
MATERIALS AND METHODS
Ethical considerations
This study obtained approval from the Research Ethics Committee of the affiliated university. Patients received written information and were allowed 3 days to consider their decision. All patients were instructed that they could withdraw from the research at any time. All participants provided their written, informed consent to take part in this research. Also, the main researcher had received a massage therapy certification from the International Complementary and Alternative Medicine Academy of Tehran University before this study.
Design of study and participants
Current study is a randomized controlled trial with a pre-post-test design. Sixty male participants (Because this research was done in an Islamic Country, the main researcher of this study was a male, and had only worked on male patients) based on the inclusion criteria were recruited. These patients had inclusion criteria such as age range between 18 and 65 years old, sleep disorders based on Pittsburgh Sleep Quality Index (PSQI),[3] hemodialysis sessions in the evening work period, absence of fractures, infections, or skin disorders in their back.
Sample size
Considering the study of Arab et al.[15] entitled “Impact of acupressure on hemodialysis patient quality of sleep”, minimum sample size for achieving power of 80% for a confidence interval of 95% based on the following formula was calculated; 29 patients were included for each groups in our study. Due to the possibility of the loss of participants, 60 patients were enrolled in this study.
Randomization
The convenience sampling method was used for study sampling. The researcher filled out the questionnaire and the informed consent sheet at the research center. If the patient was admitted at the researcher's nonattendance hours, the patient's medical records were taken by the hospital personnel. Patients met inclusion criteria were randomly selected by removing envelopes containing pairs or odds numbers, respectively, for intervention and the control groups.
Intervention
Treatment as usual
Participants in both the intervention and control group received their treatment as usual (TAU) and they have also received routine health care services and their medical appointments as required. Both groups of study participated in their conventional hemodialysis (CHD) regime, three times per week 3–5 h.
Intervention for experimental group
We used basalt stones in this study. Their size was as follows: 90 ± 2.4 mm on the major axis, 72 ± 1.5 mm on the minor axis, 323 ± 15.9 g in weight, and volume was135 ± 6.3 mL. The researcher measured volumes of these stones using Couliss Vernier (Guanglu Caliper, 111-101 HB, China) such that its measuring instinct is between 0.01 mm and 0.001 inch.
The intervention was as follows: (a) The electric pot's heat was set to 49°C–55°C; the stones were put in water in the pot for about 60 min. (b) During massage, one or three basalt stones were removed from water. (c) A dry towel was placed on the patient's back. (d) Another towel covered the stones. The patient lay in prone position and the hot stones were placed in the patient's main chakra points without any movement, for 10 min, so that their heat were applied.
In massage therapy with a hot basalt stone, one stone is placed at the site of the fifth chakra, another stone is placed in the fourth chakra, one stone is placed in the third chakra and two other stones are placed in the second and first chakra. (The first chakra is located somewhere between the anus and the genitals. The second chakra is above the genitals and is attached to the sacral bone. The third chakra is almost two fingers above the navel. Fourth chakra is in the middle of the chest, at the level of heart. The fifth chakra lies at the base of the neck and it is located between the third and fifth neck vertebrae.) In this type of massage, basaltic stones are first placed on the chakra points that mentioned. The heat stored in these stones is gradually released. Back massage using these stones was then performed for 20 min. Back massage started from the lower back and continues to the neck. Stone massage includes several steps: (1) light stroking movements, (2) Regular rubbing, (3) Regular rubbing with kneading, (4) Friction rubbing, and (5) Tapping.
This intervention was performed during 4 weeks, 3 days weekly, in total of 12 séances after hemodialysis and 1 month after the last séance of massage, patients completed the PSQI questionnaire, again.
Interventions for the control group
Massage therapy intervention was not applied for the control group and this group of study received only their routine care and TAU [Flow Chart 1].
Flow Chart 1.
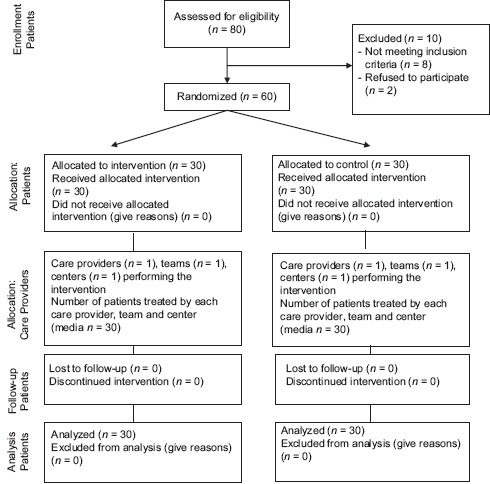
CONSORT flow diagram
Data collection and measurements
We used the researcher-made demographic information form and Persian Version of PSQI for data collection. The PSQI is used for evaluating subjective sleep quality in general and clinical populations over the previous month. The PSQI includes 19 questions that was categorized into seven components, graded on a score that ranges from 0 to 3. So, the sum of these components yields one global score, which ranges from 0 to 21, where the highest score indicates worst sleep quality. A global PSQI score >5 indicates major difficulties in, at least, two components or moderate difficulties in more than three components.[3]
The PSQI's validity and reliability was evaluated in different studies. For example, Spira et al. found evidence of the internal consistency reliability and construct validity of the PSQI and Epworth Sleepiness Scale in older men.[16] In addition, in the study of Nazifi et al., on the psychometric properties of the Persian translation of PSQI, the Cronbach's alpha coefficient was 0.55. According to the factor analysis, three factors were extracted accounting for 63.485% of the total variance. There was a significant correlation among different dimensions of the Persian version of PSQI. Concurrent validity analysis showed that PSQI and General Health Questionnaire-28 were correlated significantly.[17] In a research by Ghavami and Akyolcu, Cronbach's alpha reliability coefficient of the Persian version of PSQI scale (α) in the first measurement was 0.746 and it was calculated as 0.783 in the last evaluation.[18] Also, Farrahi Moghaddam et al. in 2012 realized Cronbach's alpha coefficient of 0.89% for the Persian version of PSQI.[19]
Two groups of study completed the PSQI and demographic data questionnaire before the intervention. In addition, PSQI was completed 1 month after the end of intervention by two groups of study.
Statistical analysis
Paired sample t-test was used to examine the quantitative variables, and Chi-square test was used to assess the qualitative variables. Paired t-test was used to compare the mean scores of each of PSQI components, and the global PSQI Score. Wilcoxon test was used for comparing of global PSQI score and components of PSQI before and after massage therapy by hot stone in intervention group. Mann–Whitney test was too applied to compare the difference of mean global PSQI scores. SPSS version 15 (SPSS 15 statistical software [SPSS Inc, Chicago, IL, USA]) was used as the statistical analysis software. Significance level of study was set at P <0.05 and in this study the values presented in mean ± standard deviation.
RESULTS
Demographic variables and clinical characteristics of participants
Patient characteristics and dialysis procedure features at baseline are summarized in Tables 1 and 2. All of the participants were compared to each other considering the demographic variables and clinical characteristics, including the cause of end-stage renal disease (including hypertension, chronic glomerulonephritis, diabetes mellitus, and other diseases), comorbidities (such as positive hepatitis B virus antigen, positive hepatitis C virus antibody, diabetes mellitus, hypertension), and initial dialysis-related data and routine biochemical parameters (including dialysis time, blood flow rate, prehemodialysis creatinine, Kt/V, albumin, phosphate, potassium, hematocrit, glucose, and monthly erythropoietin usage). No significant baseline difference was found between two groups of study regarding demographic variables, clinical characteristics and biochemical or dialysis parameters that might affect the results of this study. So, two groups of study were similar to each other (P > 0.05) [Tables 1 and 2].
Table 1.
Demographic characteristics of participants at the baseline
| Variables | Frequency or mean±SD | Statistical tests results | ||
|---|---|---|---|---|
| All (n=60) | Control group (n=30) | Experimental group (n=30) | ||
| Basic demographics | ||||
| Age (years) | 58.26±2.59 | 59.13±2.81 | 57.43±2.36 | Independent t-test results P=0.59; df=58; t=0.463 |
| Education level | ||||
| Illiterate | 23 | 11 | 12 | Chi-square test results χ2=0.875; df=2; P=0.95 |
| Under junior high school | 23 | 12 | 11 | |
| Senior high school and above | 14 | 7 | 7 | |
| Occupation | ||||
| Retired | 18 | 9 | 9 | Chi-square test results χ2=0.539; df=3; P=0.91 |
| Nongovernmental jobs | 21 | 10 | 11 | |
| Laborer | 10 | 6 | 4 | |
| Unemployed | 11 | 5 | 6 | |
| Marital status | ||||
| Married | 56 | 28 | 28 | Chi-square test results χ2=0.85; df=2; P=0.68 |
| Body mass index (kg/m2) | 22.56±3.4 | 22.4±3.55 | 22.86±3.1 | P=0.1808 |
SD=Standard deviation
Table 2.
Clinical characteristics and biochemical or dialysis parameters of participants at the baseline
| Variables | Frequency or mean±SD | Statistical tests results (P) | ||
|---|---|---|---|---|
| All (n=60) | Control group (n=30) | Experimental group (n=30) | ||
| Medical characteristics and co-morbidities | ||||
| Duration of hemodialysis (years) | 7.19±5.29 | 7.16±5.31 | 7.22±5.28 | 0.9019 |
| The cause of end-stage renal disease | ||||
| Hypertension | 15 | 7 | 8 | 0.660 |
| Chronic glomerulonephritis | 26 | 14 | 12 | |
| Diabetes mellitus | 12 | 6 | 6 | |
| Others | 7 | 3 | 4 | |
| Comorbidities | ||||
| Positive HBV antigen | 7 | 3 | 4 | 0.5001 |
| Positive HCV antibody | 9 | 5 | 4 | 0.5039 |
| Diabetes mellitus | 12 | 6 | 6 | 1.0000 |
| Hypertension | 20 | 10 | 10 | 1.0000 |
| Physiological and biochemical variables before the intervention | ||||
| Blood flow rate (mL/min) | 288.18±40.04 | 285.67±36.91 | 290.7±42.86 | 0.1238 |
| Pre-HD creatinine (mg/dL) | 10.64±2.34 | 10.54±2.35 | 10.74±2.33 | 0.3254 |
| Albumin (g/dL) | 3.95±0.34 | 3.93±0.34 | 3.97±0.34 | 0.1892 |
| Kt/V | 1.79±0.32 | 1.79±0.35 | 1.8±0.29 | 0.6175 |
| Phosphate (mg/dL) | 4.71±1.37 | 4.63±1.33 | 4.79±1.41 | 0.1679 |
| Potassium (mEq/L) | 4.92±0.72 | 4.97±0.71 | 4.88±0.72 | 0.1469 |
| Hct (%) | 31.86±4.09 | 32.2±4.1 | 31.52±4.06 | 0.0436 |
| Glucose (mg/dL)* | 97 (85–132) | 99.5 (87–133.5) | 95 (82–129) | 0.0277 |
| Monthly EPO usage (1000 U/month)* | 16 (8–22) | 16 (8–22) | 18 (11–22) | 0.0090 |
*The variables with skew distribution were presented as median (1st-quartile–3rd-quartile) and tested with Mann–Whitney U-test accordingly. SD=Standard deviation; HBV=Hepatitis B virus; HCV=Hepatitis C virus; HD=Hemodialysis; EPO=Erythropoietin; Hct=Hematocrit; URR=Urea reduction ratio
Intervention impact measurement
Findings of this research showed that all components of PSQI, except for “sleep disturbances” improved significantly after hot-stone massage therapy intervention, including subjective sleep quality (P = 0.004), sleep latency (P < 0.001), sleep duration (P < 0.001), habitual sleep efficiency (P < 0.001), the use of sleeping medication (P = 0.01) and day-time dysfunction (P = 0.005), but also global PSQI score significantly improved after the intervention (P < 0.001) [Table 3].
Table 3.
Comparison of global score and components of Pittsburgh Sleep Quality Index before and after hot-stone massage therapy in the intervention group
| PSQI components | Mean±SD | Wilcoxon test results (P) | |
|---|---|---|---|
| Before intervention | After intervention | ||
| Subjective sleep quality | 1±0.91 | 0.67±0.66 | 0.004 |
| Sleep latency | 1.6±0.77 | 1.1±0.71 | <0.001 |
| Sleep duration | 2.17±0.79 | 1.13±0.63 | <0.001 |
| Habitual sleep efficiency | 2.2±1.03 | 0.87±0.86 | <0.001 |
| Sleep disturbances | 1.1±0.548 | 0.97±0.32 | 0.1 |
| Use of sleep medication | 0.57±1.165 | 0.37±0.765 | 0.01 |
| Day-time dysfunction | 0.87±1.07 | 0.6±0.724 | 0.005 |
| Global PSQI score | 9.47±3.97 | 5.8±3.06 | <0.001 |
PSQI=Pittsburgh Sleep Quality Index; SD=Standard deviation
The mean of global PSQI scores before intervention in both groups of study was not statistically significant (P = 0.92) [Table 4]. But the mean of global PSQI scores increased after intervention in the control group, which indicates a worsening of sleep quality in the control group. In the intervention group, the mean of global PSQI scores decreased, indicating improved sleep quality in the hot-stone massage therapy group. Both of these changes were statistically significant (P < 0.001). Also, Mann–Whitney test showed a significant difference between the two groups of study considering the global PSQI scores after the intervention (P < 0.001) [Table 4].
Table 4.
Comparison before and after hot-stone massage therapy intervention by Pittsburgh Sleep Qualıty Index (n=60)
| Global PSQI score | Control group | Intervention group | Mann–Whitney U-test (P) | ||
|---|---|---|---|---|---|
| Mean±SD | Mean rank | Mean±SD | Mean rank | ||
| Before intervention | 1.87±1.22 | 28.17 | 2.2±1.03 | 32.83 | 0.265 |
| After intervention | 2.03±1 | 39.42 | 0.87±0.86 | 21.58 | <0.001 |
| Differences | 0.17±0.38 | 40.75 | −1.33±1.21 | 20.25 | <0.001 |
PSQI=Pittsburgh Sleep Quality Index; SD=Standard deviation
DISCUSSION
The present study was planned to clarify the effect of massage therapy by hot stone on sleep quality of maintenance hemodialysis patients. The findings of present study support our priori hypothesis that massage therapy by hot stone would improve sleep quality in the intervention group. Results of this study showed a significant deference between quality of sleep before and after the intervention (P < 0.001). So, applying massage therapy by hot stone in hemodialysis patients was effective on their sleep quality improvements.
The improvements in sleep quality of in patients on maintenance hemodialysis observed in current research is consistent with the changes seen with other complementary therapies such as auricular acupressure,[20] Benson's relaxation technique,[21] and inhaled lavender aromatherapy[22] on quality of sleep in patients on maintenance hemodialysis. Also, similar to our research the study of Malekshahi et al. on quality of sleep in patients on hemodialysis realized: foot massage therapy has a positive impact on improving sleep quality in patients on hemodialysis.[23]
Also, consistent with our study, Field et al. compared the effects of massage therapy on back pain and sleep disorders in two groups which received massage therapy or relaxation. Two 30-min massage sessions per week for 5 weeks was performed using body oil in the intervention group. The results showed that back pain and sleep disorders were significantly decreased in patients with massage therapy compared to the patients which received relaxation.[24]
In addition, consistent with our study, Afshar et al. reported guided imagery can significantly alleviate anxiety and improve sleep quality among hemodialysis patients.[25]
Furthermore, similar to our research, the study results of Momennasab et al. revealed that music can improve the sleep quality of hemodialysis patients. In addition, listening to music at bedtime is more effective than during hemodialysis in this regard.[26]
To the authors' knowledge, this was the first research to evaluate the impact of massage therapy by hot stone on quality of sleep in hemodialysis patients. Results from this study provided new insights into how hot-stone massage therapy influences sleep quality and consequently quality of life in patients on maintenance hemodialysis.
Limitations
This study had some limitations, so the study findings could not be generalized because of the following reasons: (1) Researcher had to select only male participants. (2) Participants were enrolled only from one hospital. (3) Our sample size relatively was small. (4) Although the effectiveness of the hot-stone massage therapy was significant compared to control group, it was not possible to rule out the placebo effect of the intervention itself, because there was not any placebo intervention in the control group in our study. Another limitation of this study was misclassification bias in self-reported questionnaire.
It has been suggested that other studies with larger sample sizes on both genders with applying a placebo intervention in control group be conducted.
CONCLUSION
Traditionally, diminished quality of sleep encourages physicians to prescribe hypnotic drugs (usually benzodiazepines) for patients on hemodialysis which may lead to side effects, such as drug resistance, memory impairment, and dependence.[27] In this study, it was demonstrated that basalt hot-stone massage therapy can successfully contribute in reducing of sleep disturbances, improving quality of sleep, and enhancing comfort level in patients on maintenance hemodialysis.
Financial support and sponsorship
This research was supported by Urmia University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors appreciate the authorities, nurses, and patients in the hemodialysis unit of Taleghani Hospital, affiliated with Urmia University of Medical Sciences, and all who helped the researchers in this master's thesis.
This study approved by the Ethics Committee of Urmia University of Medical Sciences (Ref. No. = umsu.rec. 1394.17). Also Registration No. of study is [IRCT2015042922009N1].
REFERENCES
- 1.Shariaty Z, Mahmoodi Shan GR, Farajollahi M, Amerian M, Behnam Pour N. The effects of probiotic supplement on hemoglobin in chronic renal failure patients under hemodialysis: A randomized clinical trial. J Res Med Sci. 2017;22:74. doi: 10.4103/jrms.JRMS_614_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Taheri S, Baradaran A, Aliakbarian M, Mortazavi M. Level of inflammatory factors in chronic hemodialysis patients with and without cardiovascular disease. J Res Med Sci. 2017;22:47. doi: 10.4103/jrms.JRMS_282_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Del Rio João KA, Becker NB, de Neves Jesus S, Isabel Santos Martins R. Validation of the Portuguese version of the Pittsburgh sleep quality index (PSQI-PT) Psychiatry Res. 2017;247:225–9. doi: 10.1016/j.psychres.2016.11.042. [DOI] [PubMed] [Google Scholar]
- 4.Tel H, Tel H, Esmek M. Quality of sleep in hemodialysis patients. Dial Transplant. 2007;36:479–84. [Google Scholar]
- 5.Maung SC, El Sara A, Chapman C, Cohen D, Cukor D. Sleep disorders and chronic kidney disease. World J Nephrol. 2016;5:224–32. doi: 10.5527/wjn.v5.i3.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nigam G, Camacho M, Chang ET, Riaz M. Exploring sleep disorders in patients with chronic kidney disease. Nat Sci Sleep. 2018;10:35–43. doi: 10.2147/NSS.S125839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Turgay G, Tutal E, Sezer S. Restless legs syndrome, sleep quality and fatigue in hemodialysis patients. Turk Nephrol Dial Transplant. 2018;27:196–203. [Google Scholar]
- 8.Chu G, Choi P, McDonald VM. Sleep disturbance and sleep-disordered breathing in hemodialysis patients. Semin Dial. 2018;31:48–58. doi: 10.1111/sdi.12617. [DOI] [PubMed] [Google Scholar]
- 9.Footracer KG, Monaghan M, Wisniewski NP, Mandel E. Attitudes and practices of massage therapists as related to conventional medicine. Int J Ther Massage Bodywork. 2012;5:18–24. doi: 10.3822/ijtmb.v5i1.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lawler SP, Cameron LD. Massage therapy and complementary and alternative medicine. [Last accessed on 2018 Jun 06];NZFP. 2004 31:229–38. Available from: https://espace.library.uq.edu.au/view/UQ: 121549/UQ121549_OA . [Google Scholar]
- 11.Priscilla K, Jayavanth Santha N, Priscilla K. Massage therapy-complementary and alternative therapeutic approach. Asian J Nurs Educ Res. 2014;4:516–9. [Google Scholar]
- 12.Bervoets DC, Luijsterburg PA, Alessie JJ, Buijs MJ, Verhagen AP. Massage therapy has short-term benefits for people with common musculoskeletal disorders compared to no treatment: A systematic review. J Physiother. 2015;61:106–16. doi: 10.1016/j.jphys.2015.05.018. [DOI] [PubMed] [Google Scholar]
- 13.So CS, Sarath JV, Giolli RA, Gollapudi S. The effect of thermal massage on human T Lymphocyte and natural killer cell function. Internet J Altern Med. 2008;6:4–23. [Google Scholar]
- 14.Kuge H, Mori H, Tanaka TH, Hanyu K, Morisawa T. Difference between the effects of one-site and three-site abdominal hot-stone stimulation on the skin-temperature changes of the lower limbs. J Integr Med. 2013;11:314–9. doi: 10.3736/jintegrmed2013044. [DOI] [PubMed] [Google Scholar]
- 15.Arab Z, Shariati AR, Bahrami HR, Asaiesh H, Vakili MA. The effect of acupressure on hemodialysis patient sleep quality. J Urmia Nurs Midwifery Fac. 2012;10:237–45. [Google Scholar]
- 16.Spira AP, Beaudreau SA, Stone KL, Kezirian EJ, Lui LY, Redline S, et al. Reliability and validity of the Pittsburgh sleep quality index and the Epworth sleepiness scale in older men. J Gerontol A Biol Sci Med Sci. 2012;67:433–9. doi: 10.1093/gerona/glr172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nazifi M, Mokarami H, Akbaritabar A, Kalte HO, Rahi A. Psychometric properties of the Persian translation of Pittsburgh sleep quality index. Health Scope. 2014;3:e15547. [Google Scholar]
- 18.Ghavami H, Akyolcu N. The Impact of lifestyle interventions in breast cancer women after completion of primary therapy: A randomized study. J Breast Health. 2017;13:94–9. doi: 10.5152/tjbh.2017.3342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Farrahi Moghaddam J, Nakhaee N, Sheibani V, Garrusi B, Amirkafi A. Reliability and validity of the Persian version of the Pittsburgh sleep quality index (PSQI-P) Sleep Breath. 2012;16:79–82. doi: 10.1007/s11325-010-0478-5. [DOI] [PubMed] [Google Scholar]
- 20.Wu Y, Zou C, Liu X, Wu X, Lin Q. Auricular acupressure helps improve sleep quality for severe insomnia in maintenance hemodialysis patients: A pilot study. J Altern Complement Med. 2014;20:356–63. doi: 10.1089/acm.2013.0319. [DOI] [PubMed] [Google Scholar]
- 21.Rambod M, Pourali-Mohammadi N, Pasyar N, Rafii F, Sharif F. The effect of Benson's relaxation technique on the quality of sleep of Iranian hemodialysis patients: A randomized trial. Complement Ther Med. 2013;21:577–84. doi: 10.1016/j.ctim.2013.08.009. [DOI] [PubMed] [Google Scholar]
- 22.Lillehei AS, Halcón LL, Savik K, Reis R. Effect of inhaled lavender and sleep hygiene on self-reported sleep issues: A randomized controlled trial. J Altern Complement Med. 2015;21:430–8. doi: 10.1089/acm.2014.0327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Malekshahi F, Aryamanesh F, Fallahi S. The effects of massage therapy on sleep quality of patients with end-stage renal disease undergoing hemodialysis. Sleep Hypn. 2018;20:91–5. [Google Scholar]
- 24.Field T, Hernandez-Reif M, Diego M, Fraser M. Lower back pain and sleep disturbance are reduced following massage therapy. J Bodyw Mov Ther. 2007;11:141–5. [Google Scholar]
- 25.Afshar M, Mohsenzadeh A, Gilasi H, Sadeghi-Gandomani H. The effects of guided imagery on state and trait anxiety and sleep quality among patients receiving hemodialysis: A randomized controlled trial. Complement Ther Med. 2018;40:37–41. doi: 10.1016/j.ctim.2018.07.006. [DOI] [PubMed] [Google Scholar]
- 26.Momennasab M, Ranjbar M, Najafi SS. Comparing the effect of listening to music during hemodialysis and at bedtime on sleep quality of hemodialysis patients: A randomized clinical trial. Eur J Integr Med. 2018;17:86–91. [Google Scholar]
- 27.Wu Y, Yang L, Li L, Wu X, Zhong Z, He Z, et al. Auricular acupressure for insomnia in hemodialysis patients: Study protocol for a randomized controlled trial. Trials. 2018;19:171. doi: 10.1186/s13063-018-2546-2. [DOI] [PMC free article] [PubMed] [Google Scholar]