

Abstract
Traumatic injuries accounted for substantial burden of morbidity and mortality (M and M) worldwide. Despite better socioeconomic conditions and living standards, the incidence of trauma is rising in the Eastern Mediterranean Region (EMR). Road traffic injuries are the leading cause of the high fatality rate in young economically productive adults in our region. The provision of trauma care at high-volume, accredited trauma center by a team of dedicated full-time professional health-care providers has been shown to improve the quality of care and the outcomes for trauma victims. With persistent hard work and effective leadership, in Qatar, the Trauma Section has evolved into a well-reputed and internationally recognized Center of Excellence in Trauma Care, Hamad Level 1 Trauma Center. In 2014, Qatar Trauma System was accredited with Trauma Distinction Award by the Accreditation Canada International, for high-quality trauma care of severely injured patients; first in the Middle East. The Hamad Trauma Center is committed to the advancement of trauma care in different aspects right from the immediate prehospital care to the subsequent hospital-based care, involving diagnosis, treatment, support, rehabilitation, and community reintegration of the patients and injury prevention. Our trauma system has gradually embedded with a structured and matured research unit with dedicated clinicians and academic researchers. The trauma team embodies the 21st-century paradigm of translational research and injury prevention by going well beyond the bedside, out into the populations that need it most. The trauma system's future vision relies on the evidence-based health-care service and better outcomes; state-of-the-art infrastructure and multidimensional collaborations with health care and governmental services to minimize the burden of M and M caused by traumatic injury in the State of Qatar and to fulfill the population health enhancement strategy.
Keywords: Health care, injury prevention, Middle Eastern region, research, trauma system
INTRODUCTION
According to the global estimates from the World Health Organization (WHO), traumatic injuries accounted for 9% of all deaths, and substantial burden of such fatalities are reported from the low- and middle-income countries.[1] Traffic-related injuries (TRIs) are responsible for around 50 million traumatic injuries worldwide and which is expected to increase by 65% over the next two decades unless prevented.[2] Especially, injury-related morbidity and mortality (M and M) is increasing in the Eastern Mediterranean Region (EMR), particularly affecting young adults, mostly males involving road traffic collisions and vulnerable road users.[3] In the Arab Middle Eastern region, the most common mechanisms of injury include road traffic collisions, falls from height, fall of heavy objects, and pedestrian injuries.[4] The global health estimates in 2013, predicted that there will be 595,097 injuries per year in the EMR, including Qatar, by the year 2030.[5] An earlier study from Qatar also demonstrated a higher burden of road traffic injuries (RTIs) in young economically productive adults; of them, the fatality rate was higher among nationals.[6] Moreover, among survivors, many of them will not recover completely and have substantial lifelong disability as a result.
The WHO has espoused a multipronged response to this global health problem, including a range of activities, from better surveillance, improved quality and access of trauma care to more in-depth research, and primary prevention. It has also supported much-needed efforts to strengthen the care of the injured. In 2007, the World Health Assembly (WHA) adopted resolution WHA 60.22 on trauma and emergency care services. According to this resolution, the governments and WHO should enhance the efforts for better care of the injury victims and other medical emergencies. Furthermore, there is a need to increase awareness regarding the cost-effective ways for the care of trauma and emergency services; that can be improved by sustainable organizational planning, promoting policies, and political commitment.[7]
There is a pressing need for better health-care management and the global efforts to strengthen care for the injured. For this, the National Trauma Centers of EMR should focus on the research related to the advancement of trauma care in different aspects right from the prehospital care to hospital-based care involving all aspects of care; diagnosis, treatment, support, rehabilitation of injured patients, and injury prevention both primary and secondary. Furthermore, the international organizations should provide support to countries in developing rehabilitation services for people with disabilities to ensure successful community reintegration. Moreover, the injury data should be shared among the scientific community and health-care authorities through the establishment of the National Trauma Registry, publishing high-quality research papers, conducting regular scientific meetings to highlight the priority global public concern and inform the care of these who critically injured.
The provision of trauma care at high-volume, accredited trauma centers by a team of dedicated full-time professional health-care providers has been shown to improve the quality of care and the outcomes for trauma victims.[8] Keeping this in mind, a Trauma Surgery Unit (TSU) was established in the Hamad General Hospital (HGH) of the Hamad Medical Corporation (HMC) Doha, Qatar, to provide an integrated, comprehensive, multidisciplinary patient care with several subunits and supportive programs, in November 2007 [Figure 1]. Trauma care was delivered by multi-specialty team composed of trauma surgeons, emergency physicians and nurses, anesthetists, intensivists and ICU nurses, clinical pharmacists and other allied medical personnel. Figure 2 shows the components of Hamad Trauma Center.
Figure 1.
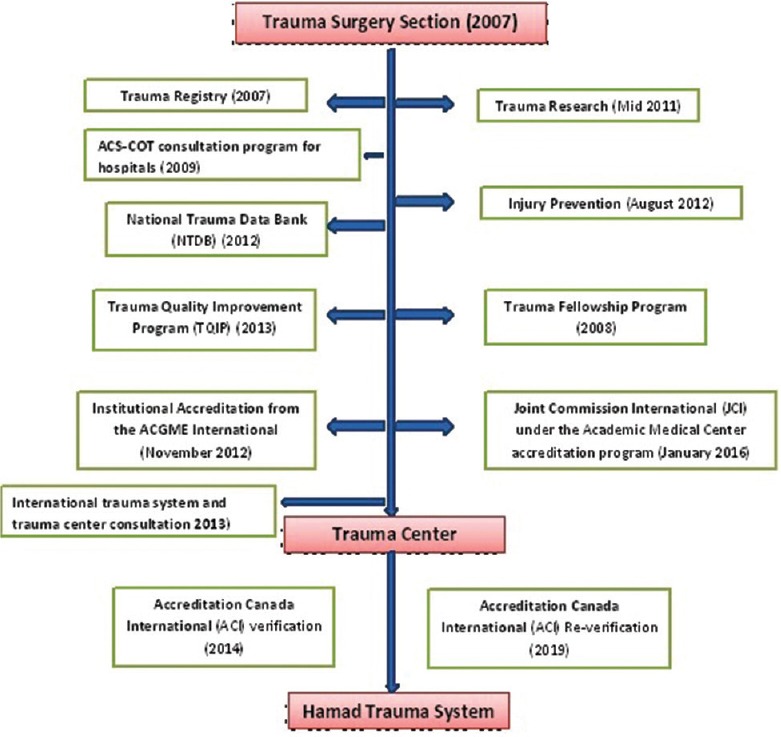
Overview of Trauma Journey
Figure 2.
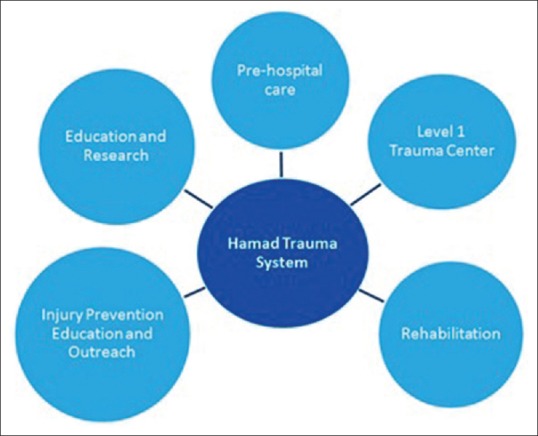
Components of Hamad Trauma System
PREHOSPITAL CARE
In Qatar, the Ambulance Service (AS) provides prehospital emergency care (both ground ambulance and air ambulance) and interfacility transfer services within the borders of the State of Qatar and occasionally beyond. In keeping with HMC's mandate, these services are provided free of charge to all the people of Qatar, whether resident or visiting. AS is being operated by the National Command Centre which uses a unified country-wide emergency number (999). The HMC-AS operates with a tiered response which deploys a minimum of two-crew member paramedic ambulance to all emergency calls with additional specialized resources being dispatched as indicated by the computerized dispatch criteria. In addition, trained call takers provide prearrival instructions to optimize the prehospital patient care. The prearrival instruction includes caller-taker-directed first-aid management of hemorrhage control, burns, and basic life support management of unconscious patients. In keeping with the National Health Strategy Response targets 75% of life-threatened patients in urban and rural areas should receive an ambulance within 10 min and 15 min, respectively, 95% percentiles are also reported.
HMC-AS comprised two levels of clinical professionals, i.e., ambulance paramedic and critical care paramedics (CCPs). The CCPs are credentialed, Emergency Medical Service personnel with critical care competence and have an advanced set of clinical skills that is supported by a complete range of medications and equipment, reflecting the latest clinical evidence in prehospital and hospital-based emergency care. The level of care provided by this emergency personnel is guided by the rigorously evaluated and up-to-date evidence-based clinical practice guidelines which are developed in conjunction with the Level 1 Trauma Center at HGH. Moreover, these guidelines are being reviewed annually and updated with any significant changes recommended as per the International Clinical Practice. This approach facilitates rapid adoption of the best clinical practice which is evident from the recent introduction of prehospital tranexamic acid administration based on the CRASH-2 study recommendations[9] and the use of a standardized prehospital Rapid Sequence Induction protocol[10] as the standard of care.
The HMC-AS follows a standard field triage criteria “trauma by-pass protocol” to allow transfer from the incident scene directly to the Level I Trauma Center at HGH. For peri-arrest patients, transportation to the nearest district hospital remains a clinical decision. However, in Qatar, the deployment of CCP provides a wider scope of care with relative short transfer times. Furthermore, round the clock availability of two CCP-staffed helicopters typically support the bypass criteria, thereby minimizing the need for subsequent interhospital transfer to the Hamad Trauma Center.
However, in cases where patients require immediate stabilization, initial transport to one of HMC's rural hospitals, Al-Khor Hospital (North), Al-Wakra Hospital (South), and The Cuban Hospital (West), may take place, with subsequent transfer to the Hamad Trauma Center as indicated by the clinical circumstances. The Hamad Trauma Team works in close collaboration with HMC-AS personnel, communicating while patients are en route, to insure timely and safe transfer of the patient to the trauma center. The specialized trauma teams take over the subsequent in-hospital emergency care of the injured patient and provide the comprehensive multidisciplinary care and management.
TRAUMA CARE UNITS
The Hamad Trauma Center is staffed with dedicated highly trained trauma and critical care surgeons, anesthetist intensivists, critical care nurses, paramedics, and other health-care professionals with specialized training in trauma, acute care surgery, and critical care medicine providing in-house coverage 24-h a day, 7 days a week. The team plays an essential role in delivering an integrated comprehensive care that is thoughtfully designed to reduce death and disability posttrauma. The Level I designation means that the Trauma Center conforms to the highest international standards with coordinated patient care by multidisciplinary team available onsite, including neurosurgery, orthopedic surgery, anesthesia, emergency medicine, radiology, vascular surgery, maxillofacial surgery, and plastic surgery. The operating rooms and personnel are also available 24 h a day, 7 days a week. Moreover, the blood bank facilities are round the clock available and capable of providing massive transfusions shipments as per the approved corporate protocols. The Hamad Trauma Center has been recognized and accredited locally and internationally, by the WHO and Trauma Distinction Award by the Accreditation Canada International, for high-quality trauma care of severely injured patients.[11]
The Hamad Trauma Center comprised three major units for patient care trauma resuscitation unit (TRU), trauma intensive care unit (TICU), TSU (trauma in-patient ward), and trauma outpatient clinic.
The trauma resuscitation unit
Consists of six trauma bays and is equipped with state-of-the-art technology and staffed by highly trained and experienced trauma surgeons and nurses; who stand ready to receive injured patients round the clock. HMC-AS ground as well as air ambulance crews can bring injured patients directly to the TRU for in-hospital care. The TRU is designed to give timely assessment of hemodynamic status as well as resuscitation of critically injured patients, supported by up-to-date point of care testing for arterial blood gas, thromboelastography, and rapid International Normalized Ratio to inform the critical decision-making processes led by the trauma team leader and/or consultant. Moreover, to optimize the trauma resuscitation, the TRU has Pyxis MedStation which readily contains all the emergency medications especially those specifically and commonly used as adjuncts to hemostatic resuscitation of critically injured and bleeding patients such as fibrinogen, tranexamic acid, prothrombin complex concentrate, antibiotics, and vasopressors. The staff credentials are kept up to date with regard to training and privileges for bedside procedures, evidence-based team dynamics training programs such as team strategies and tools to enhance performance and patient safety, advanced airway management, pediatric life support, and trauma life support, together with onsite simulation-assisted training for team resuscitation with debriefing and feedback.
To ensure that no injury is missed, every patient undergoes a detailed reexamination by a trauma surgeon within 24 h of their arrival at the TRU known as a Tertiary Trauma Survey. This patient reevaluation tool is used to identify and catalog all injuries after the initial resuscitation and operative intervention. It is an important part of the comprehensive treatment plan to identify and treat any missed injuries, extensive care, and other health-related problems or comorbidities.
The Operating theaters area is 10,000 m2 with 17 well-equipped surgical theaters and 3 hybrid operating room equipped with advanced medical imaging devices such as a magnetic resonance imaging scanner, computed tomography scanner, fixed C-arm for invasive diagnostics and endovascular intervention, brain laboratory technology, and supported by extracorporeal membrane oxygenation (ECMO) program.
The trauma intensive care unit
It is a 19bed critical care unit located on the first floor of the new operating theater building. The TICU provides special care to critically injured patients requiring close monitoring and intensive care. It contains the state-of-the-art equipment for intensive care and team of critical care fellowship trained (as subspecialty) surgeons and anesthesiologists (intensivist), critical care nurses, respiratory therapists, dietitians, and other health-care workers. The team provides integrated, multidisciplinary critical care, based on the international evidence-based clinical and best practice guidelines and established protocols. Annually, the TICU team treats more than 600 critically ill trauma patients. Moreover, there is a trauma step-down unit with a capacity of seven beds to treat the injured patients with intermediate level of care or in need for a bridge between TICU and trauma in-patient ward (TSU).
The trauma surgery unit
It is a twenty-bed capacity in-patient ward dedicated to trauma surgery cases meant for reevaluation, treatment, and disposition of patients to home or rehabilitation services. It is located in the 4 North, Section 2 at HGH and includes four private rooms and four common rooms. The TSU is staffed by highly trained doctors and nurses and has advanced medical equipment readily available to cater urgent patient needs. The TSU staffs are trained in using the latest medical technology, committed to evidence-based practice and are regularly involved in continuing nursing education courses. The TSU multidisciplinary team critically reviews each admitted patient on a daily basis and plans for discharge accordingly. The goal is to help the trauma patient's quick, safe recovery, and to achieve the highest level of functional outcomes.
Severely injured pediatric trauma cases are being transported directly to the Hamad Trauma Center, while minor injuries are managed at Pediatric emergency center. Pediatric trauma care is collaboratively delivered by the Trauma Center, the Pediatric Surgery Service, and the pediatric intensive care unit at HGH with a formalized defined pathways and protocols. Each year, >200 severely injured children (14 years of age and below) are admitted to HGH for traumatic injuries.
Clinical psychology service
Recognizing the fact that the physical trauma is often accompanied by emotional distress to both the patient and family, the trauma center started a unique clinical psychology service to address trauma-related mental health. The involved psychologist evaluates acute patients upon admission, in the TICU, the ward and upon follow-up in dedicated outpatient clinic. The psychologist assesses patients for early distress, anxiety, support opportunity, informs physician, and enhances secondary prevention activities such as the alcohol intervention and referral to psychiatry care. Moreover, a special Handbook for Trauma Patients and their Families was produced. It is specifically designed to help ease the emotional stress related to injury, care and to help with navigating the unfamiliar hospital setting, and plans of care and decreasing stress through communicating pertinent and relevant information about trauma care at Hamad General Hospital.
Posthospital care
It is an essential step in the process of returning an injured person to good health and a productive life. Home care, rehabilitation services, family support, patient education, and other inpatient and outpatient specialized therapy, and treatments are an important part of the HMC Trauma System scope of care. HMC offers a number of outpatient rehabilitation care services to patients recovering from traumatic injury through the National Qatar Rehabilitation Institute, Trauma Outpatient and Psychiatric Clinic.
COMPONENTS OF QATAR TRAUMA SYSTEM
The integrated trauma care is supported by the Qatar Trauma Registry, the performance improvement program that is compliant with the Trauma Quality Improvement Program (TQIP) of the American College of Surgeons Committee on Trauma (ACS-COT), the Trauma and Critical Care Fellowship Program, Hamad Injury Prevention Program (HIPP), and the Clinical Research Unit.
QATAR TRAUMA REGISTRY
A major step to implement an effective and integrated system for trauma care improvement is the establishment of a trauma registry. It is a data repository composed of uniform data elements that describe the injury events, demographics, prehospital information, diagnoses, care provided and outcome of injured patients, as well as injury severity scores. It is a valuable source of information for improvements in the quality of care, policy development, identification of opportunities for injury prevention, and clinical and epidemiologic research. In 2007, the HMC Trauma Registry was setup with the start of the trauma services [Figure 3]. In keeping with the National E-Health and Data Management Strategy, transformative and continuous improvement of health care through the use of information and technologies that support the delivery of health care and clinical research Qatar Trauma Registry was launched in December 2017. Since 2011, the Trauma Registry has contributed data to the American College of Surgeons Committee on Trauma's (ACS-COT) National Trauma Databank®, is the largest aggregation of trauma registry data as an international trauma data repository. The Qatar Trauma Registry also began to contribute to the ACS- COT's TQIP® in 2013 which is the leading performance measurement tool for trauma care. The registry data are compiled and collected by TQIP® biannually and distributed to the participating institution in the form of a comprehensive hospital performance reports with comparative benchmark data [Figure 4].
Figure 3.

The structure of the Qatar Trauma Registry
Figure 4.
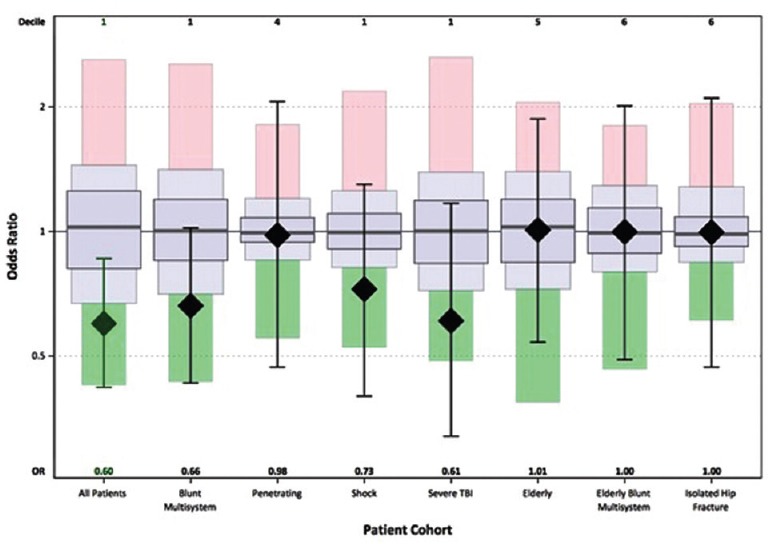
Risk-Adjusted Mortality by Cohort
Moreover, for internal validation, the registry data are audited for accuracy and completeness. Audit findings are shared with registry staff at monthly staff meetings, and relevant education is being provided.
The registry staff includes database administrator and nurse data analysts that are supervised by the Trauma Program Manager. The Trauma Registrar is responsible for the collection, entry, maintenance, and reporting of data for a Trauma Center (and in many cases other local and state regulatory agencies). Registry data are used for trauma research, epidemiology, prevention initiatives, and performance improvement. Data capture in the trauma registry has a direct impact on accurately characterizing patient care and patient outcomes.
HAMAD INJURY PREVENTION PROGRAM: EDUCATION AND OUTREACH
Trauma injury prevention education and outreach program is one of the key focus areas for the Hamad Trauma System. The HIPP was initiated to improve public health and safety by reducing the most frequent and high-risk mechanisms that cause traumatic injury. Since its establishment, HIPP has enhanced public awareness of injury prevention, garnered research funds to support injury prevention education and surveillance programs and strengthened existing relationships with important government ministries and agencies, as well as nongovernmental stakeholders for public safety.
Trauma is a leading cause of mortality among young and productive populations in most countries worldwide. Although, the long-term sequelae of survivors of trauma are not very well documented from our region. The most common causes of health burden from trauma have been taken into consideration for improved pre- and in-hospital trauma services, i.e., secondary and tertiary prevention. Many public health models of disease management and prevention espouse a problem-solving approach to trauma and injuries that involves all three levels of injury prevention, which is the foundation of the HIPP in Qatar.
The HIPP began by defining the burden of injury in Qatar through close consultation with clinical and public health leaders. It is committed for objective collection and analysis of available gray and published literature, identifying and engaging the various stakeholders in the field, and creation of a list of priority injury risk areas/mechanisms and the concomitant high-risk populations. Traumatic injury is the leading identifiable cause of death, for all ages and both sexes, in Qatar. RTIs are the significant cause of mortality among young males (10–29 years), and particularly, Qatari males from 10 to 49 years are at the highest relative risk for RTI-related deaths.[6] The HIPP proposed to implement road safety programs in Qatar according to the global plan of five-pillar matrix which includes road safety management, safer roads, safer vehicles, safer road users, and postcrash response to minimize the incidence of TRI-related deaths to 50% by 2020.[12] Analyses of the trend of trauma admissions [Figure 5] from the Trauma Registry, and epidemiologic reports on these leading causes further defined the injury problem in Qatar.
Figure 5.
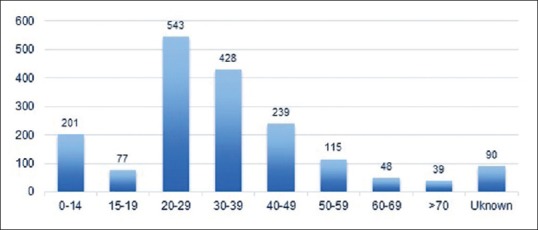
Trauma admissions (n), by age group, both sexes, Hamad Trauma Center Registry, January 1–December 31, 2017, Doha, Qatar
A summary of the priority risk areas and high-risk populations from the problem definition phase are listed below:
RTIs for young male Qatari drivers (10–49 years)
-
Occupational or work-related injuries
- Construction-related falls from height
- Construction-related falling heavy objects
- Work-related RTIs
Pedestrian-motor vehicle crashes (expatriates from right-hand drive countries)
RTIs to unrestrained child passengers.
After defining the public health problem related to trauma in Qatar, identifying the leading mechanisms of injury and the high-risk populations, the next step is to initiate various research activities to identify the root causes/contributing factors and identifying preexistent/proven programs that could be adapted to the local setting.
The HIPP received two research grants from the National Priorities Research Program (NPRP) to improve the quality of work-related injury data collection entitled “A Unified Registry for Occupational Injury Prevention in Qatar” (NPRP 7-1120-3-288) and compliance of child restraint use among children younger than 5 years entitled “Young Kids In Safe Seats (Y-KISS)-Qatar Program: A Randomized Study to Increase Child Restraint Use in Qatar” (NPRP 7-1681-3-429). In addition, multiple intramural research grants on pediatric injuries, alcohol screening in trauma patients, the cost of pedestrian injuries, and improving mortuary reporting of injury deaths, have been or are being conducted to improve understanding of the local epidemiology of injuries in Qatar.
Literature reviews and stakeholder consultations (CWSP3-W-0413-14042 “A Workshop for the Transportation Health Research in Children of Qatar Working Group” and International Traffic and Medicine Association 2015 Young Driver Workshop) have been used to identify preexistent and proven programs for the priority mechanisms and high-risk populations.
International stakeholder meetings are being conducted to share the best evidence and inform the creation of locally appropriate injury prevention interventions and programs. Regular communications, consultation, and meetings with the Ministries of Health (Public Health Department), Labor (Inspections Department), and Ministry of Interior (MOI) (Traffic and Media Awareness Departments) have resulted in increased education and public awareness as well as improve coordination between agencies for improvements in road and occupational safety in Qatar. The HIPP has also provided technical assistance to the National Traffic Safety Committee and has provided coordination and planning to increase Qatar's participation in global road safety efforts. The Hamad Trauma Center has led efforts to commemorate the UN Global Road Safety Week, held on every May and the World Day of Remembrance for RTI Victims, held annually in November, since 2013.
Another example of sustained collaboration is the joint efforts of Hamad Trauma Center and the MOI to lead a media campaign designed to create public awareness regarding the increased risk of RTI during the holy month of Ramadan, especially among young male drivers. The month-long campaign includes television and cinema commercials, the distribution of car stickers, and information booths at major shopping malls. It also focuses on raising public awareness on the fatal consequences of reckless driving, non-compliance of car seat belt, using mobile phones while driving, and over-speeding.
In recent years, HIPP is more focused on high-risk groups for injury, including children, pedestrians, and construction workers. In addition to community education, HIPP is working for various injury prevention education efforts, in close collaboration with government ministries, transport department, and other agencies.
Pedestrians are the most vulnerable road users in Qatar, with a greater proportion of pedestrians are being killed or injured on roads than the global average. Protecting these vulnerable road users through the education of both pedestrians and drivers is a priority for the trauma team. HIPP has collaborated with expatriate worker communities, the Ministries of Labor and Interior and Qatar University's Road Safety Studies Center to improve pedestrian safety through various awareness events.
Motor vehicle crashes are a leading cause of death among children 14 years of age and under; therefore, helping parents understand what they need to know about child passenger safety is a priority for the trauma team. The Johns Hopkins International Injury Research Unit (JH-IIRU) and HIPP are working on a 3-year grant designed to improve the compliance with child restraints in children under 5 years of age (see YKISS Qatar Program above) and in partnership with the HMC Kulluna Health and Safety Campaign, HIPP representatives train child passenger safety technicians and instructors and participate in community checkup events for families with children in car seats. The Hamad Trauma Center is committed to improve child passenger safety in Qatar.
Qatar's construction industry has gone through an accelerated growth period in recent years. Improving worker safety and preventing work-related injuries continue to be a priority for the Trauma Team. HIPP activities are focused on targeted occupational safety awareness events and activities that aim to highlight the high-risk construction site hazards, such as falls from height incidents. In addition, HIPP has partnered with the Ministry of Public Health, the Ministry of Labor, and the JH-IIRU on a project to create a linked database of all occupational injuries that occur in Qatar, and this database will help to identify the complex predisposing factors that lead to occupational injuries.
TRAUMA EDUCATION AND CRITICAL CARE FELLOWSHIP PROGRAM
The Hamad Trauma Center offers various robust, ongoing staff educational programs. It includes a weekly weekly M and M conference, fellowship lectures, surgical grand rounds and a monthly Journal Club and research activity. Outreach education is provided at all HMC hospitals, involved in trauma care such as Al-Khor, Al-Wakra, and The Cuban Hospital.
The Trauma and Critical Care Fellowship Program is an Accreditation Council for Graduate Medical Education (ACGME) structured, 2-year program approved by the Department of Medical Education at HMC. The program is a part of the commitment to support the next generation leaders of Hamad Trauma Center. The fellows are trained and evaluated according to the ACGME's six core competencies, i.e., (a) patient care and procedure proficiency, (b) medical knowledge, (c) practice-based learning and improvement, (d) interpersonal and communications skills, (e) professionalism, (f) systems-based practice. Up to seven fellows, including international candidates, participate and are trained each year from three specialties, namely, surgery, anesthesia, and emergency medicine.
CLINICAL RESEARCH IN TRAUMA
Contemporary literature suggests that the outcomes of trauma patient are improved with the development of a mature trauma system in an organization of which clinical research is a key component delivering evidence-based patient care. Our research program seeks to advance clinical knowledge to optimize and improve the care of injured patients. Research objectives are driven by the needs of the patient population and seek to advance clinical knowledge in order to optimize and improve the care of severely injured patients. Research in emergency settings is challenging due to barriers or circumstances that are manifested with emotional distress, time-critical nature of interventions, and appropriate decision-making. Therefore, it is crucial to identify the potential benefits and major barriers in emergency research to cater evidence-based care.[13]
Figure 6 demonstrates an overview of the research and development activities at Hamad Trauma Center.
Figure 6.
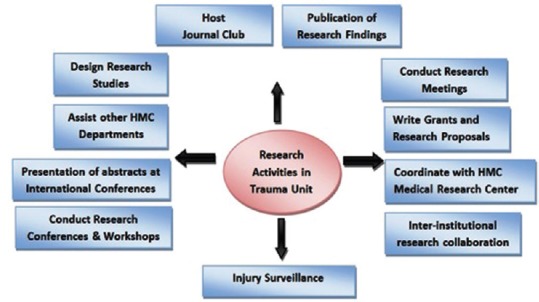
Overview of research and development activities
The Hamad Trauma Center is involved in numerous research projects covering major issues of trauma across the entire timeline of trauma patient care, from the prehospital settings to the hospital discharge. Trauma Team members are currently conducting a number of research projects, including research focused on road traffic crashes, alcohol screening, in-hospital cardiac arrest in trauma, traumatic brain injury (TBI), posttraumatic stress disorder, vascular disease, prehospital intubation, and ventilator-associated pneumonia.
The important determinants of the best clinical practice, includes implementation of clinical practice guidelines, education and training for clinical staff, and improvement of quality of care through audits and clinical review. Therefore, research analysis in trauma helps in developing competencies of junior staff to improve patient care through better management strategies. For continuing education, a regular structured research activity in the form of monthly research/journal club is being conducted by our department to present internal research projects and review recent publications on trauma and critical care to provide a forum for critique and discussion by the staff, surgical residents, nurses, and medical students. Research activities in trauma also increase the awareness and interest of trauma staff towards developing skills for evidence-based patient care.
Our research program at Hamad Trauma Center has created a real presence in scientific literature and continues to be recognized as a leader in the region and beyond. The outcomes of our research are successfully interpreted and add-up to the international literature in the form of scientific publications and presentation at international conferences. Each year, Trauma Team members publish more than thirty articles in international, peer-reviewed journals. A previous publication from our center reported that inception of the dedicated trauma research unit contributed to the major (up to 84%) proportion of trauma research publications and is an indication of progressive maturation of the Trauma Care System in Qatar.[14]
Trauma Team members also regularly contribute to the regional and international conferences. From 2014 onward, Team members have started to plan, implement, and participate in the high-quality multicenter randomized clinical trials. The Trauma Team initiated international collaborations and participated in two multicenter studies from Australia. The first important study is the randomized controlled clinical trial on Hypothermia in TBI patients (POLAR-randomized controlled trial) [clinicaltrials.gov Identifier: NCT00987688]. The other prospective multicenter study is on-going which aims to test the accuracy of a clinical prediction tool to exclude fractures of the thoracolumbar spine among patients undergoing imaging posttrauma. Another important on-going prospective study is to assess the impact of stress-induced hyperglycemia (SIHG study) on the outcome of trauma patients and investigates the association between pro-inflammatory cytokine levels and SIHG in trauma population. We are also conducting a clinical trial to look for the safety and efficacy of the second dose of tranexamic acid administration in severely injured patients at risk of bleeding. Expertise in the field of evidence-based medicine including systematic review and meta-analysis triggered the center to take a step toward collaborating with Cochrane and establish a future Cochrane center for evidence-based medicine in Qatar. Establishing a robust research infrastructure and know how at the basic, translational, and clinical levels generates a better understanding of trauma in Qatar.
During the course of time, our trauma system has gradually embedded with a structured and matured research unit with dedicated clinicians and academic researchers. Our trauma team has been recognized by the corporation with several awards for successful translation of clinical research into improved patient outcomes, continued growth in research capacity, increased trauma research collaborations, expanded policies for trauma care, and increased public awareness and safety. Our research team embodies the21st-century paradigm of translational research by going well beyond the bedside, out into the populations that need it most.
Notably, RTIs are the leading cause of death and disability in the country, so there is a need for national funding agencies to allocate grants to foster trauma research and injury prevention. This will facilitate more advanced infrastructure to establish evidence-based center for emergency medicine. In addition, it is also important to have collaboration and memorandum of understanding with different governmental and international agencies such as World Academic Congress of Emergency Medicine (WACEM) to develop a sustainable education and training hub with direct involvement of the WHO and other international authorities for trauma and emergency care.
CONCLUSIONS
The inception of the trauma system in Qatar with multidimensional approach improved our understanding of the problem of trauma and enhanced our management approach as well as prevention of trauma compared with the international benchmarks. In addition, we focus to make an impact on the efficiency and adaptability of health-care delivery in Qatar. Evidence-based research in trauma and critical care plays an important role in providing better health-care facilities and proper utilization of hospital resources. It helps in better management of patient flow, resources of TRU, and emergency department which eventually reduces overcrowding and improves patients' satisfaction and establish international linkages of collaboration.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank the entire trauma team in the Trauma Surgery Section, Hamad General Hospital, Doha, Qatar. All authors have no conflict of interest, no financial issue to disclose, and no funding was received for this study.
REFERENCES
- 1.Peden M, McGee K, Sharma G. The Injury Chart Book: A Graphical Overview of the Global Burden of Injuries. Geneva: World Health Organization; 2002. [Google Scholar]
- 2.Paniker J, Graham SM, Harrison JW. Global trauma: The great divide. SICOT J. 2015;1:19. doi: 10.1051/sicotj/2015019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bachani AM, Zhang XJ, Allen KA, Hyder AA. Injuries and violence in the eastern Mediterranean region: A review of the health, economic and social burden. East Mediterr Health J. 2014;20:643–52. [PubMed] [Google Scholar]
- 4.Asim M, El-Menyar A, Al-Thani H, Abdelrahman H, Zarour A, Latifi R. Blunt traumatic injury in the Arab Middle Eastern populations. J Emerg Trauma Shock. 2014;7:88–96. doi: 10.4103/0974-2700.130878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.World Health Organization. Projections of Mortality and Causes of Death, 2015 and 2030. Health Statistics and Information Systems. [Last accessed on 2019 Mar 10]. Available from: http://www.who.int/healthinfo/global_burden_disease/projections/en/
- 6.Consunji RJ, Peralta RR, Al-Thani H, Latifi R. The implications of the relative risk for road mortality on road safety programmes in Qatar. Inj Prev. 2015;21:e105–8. doi: 10.1136/injuryprev-2013-040939. [DOI] [PubMed] [Google Scholar]
- 7.Strengthening Care for the Injured: Success Stories and Lessons Learned from Around the World, Wounds and Injuries – Therapy, Delivery of Health Care, Emergency Medical Services – Organization and Administration and Rehabilitation. World Health Organization, Department of Violence and Injury Prevention and Disability. 2010 [Google Scholar]
- 8.MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354:366–78. doi: 10.1056/NEJMsa052049. [DOI] [PubMed] [Google Scholar]
- 9.El-Menyar A, Sathian B, Asim M, Latifi R, Al-Thani H. Efficacy of prehospital administration of tranexamic acid in trauma patients: A meta-analysis of the randomized controlled trials. Am J Emerg Med. 2018;36:1079–87. doi: 10.1016/j.ajem.2018.03.033. [DOI] [PubMed] [Google Scholar]
- 10.Lyon RM, Perkins ZB, Chatterjee D, Lockey DJ, Russell MQ Kent, Surrey and Sussex Air Ambulance Trust. Significant modification of traditional rapid sequence induction improves safety and effectiveness of pre-hospital trauma anaesthesia. Crit Care. 2015;19:134. doi: 10.1186/s13054-015-0872-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Qatar Trauma System Becomes First to Earn Recognition from Accreditation Canada International. [Last accessed on 2019 Mar 05]. Available from: https://www.trauma-news.com/2015/02/qatar-trauma-system-becomes- first-ear-recognition-accreditation-canada-international/
- 12.Consunji R, Mekkodathil A, Abeid A, El-Menyar A, Al-Thani H, Sekayan T, et al. Applying the five-pillar matrix to the decade of action for road safety in Qatar: Identifying gaps and priorities. Trauma Surg Acute Care Open. 2018;3:e000233. doi: 10.1136/tsaco-2018-000233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.El-Menyar A, Asim M, Latifi R, Al-Thani H. Research in emergency and critical care settings: Debates, obstacles and solutions. Sci Eng Ethics. 2016;22:1605–26. doi: 10.1007/s11948-015-9730-5. [DOI] [PubMed] [Google Scholar]
- 14.El-Menyar A, Asim M, Zarour A, Abdelrahman H, Peralta R, Parchani A, et al. Trauma research in Qatar: A literature review and discussion of progress after establishment of a trauma research centre. East Mediterr Health J. 2016;21:811–8. doi: 10.26719/2015.21.11.811. [DOI] [PubMed] [Google Scholar]