

Abstract
Introduction:
Ectopic thyroid occurs due to aberrant development of the thyroid gland during its migration to the pretracheal region. Intrapulmonary ectopic thyroid is extremely rare and its benign transformation (microfollicular adenoma) has never been reported. This paper reports a case of ectopic thyroid microfollicular adenoma in the lung mimicking metastatic pelvic tumors.
Patient concerns:
A 76-year old female presented to our hospital because of transient unconsciousness. Pelvic ultrasound (US) and chest computed tomography (CT) showed pelvic tumors and pulmonary nodules.
Diagnosis and interventions:
The patient underwent pelvic tumors resection and CT-guided fine-needle aspiration cytology (FNAC) at the largest pulmonary nodule. Pathological description revealed bilateral ovarian serous cystadenoma and endometrioma in pelvic, and ectopic thyroid microfollicular adenoma in lung. In view of the patient's age and physical conditions, it is unanimously decided by the physicians and the family members of the patient to closely follow up this benign pulmonary lesion.
Outcomes:
During the 12-month follow-up, no pelvic tumor recurrence or metastasis was found. CT review of pulmonary nodules showed no remarkable changes. The patient was asymptomatic and euthyroid after being discharged from the hospital.
Conclusion:
Ectopic thyroid microfollicular adenoma in the lung is extremely rare and can be easily mistaken for pulmonary metastases from other sites. The case reported in this paper highlights that ectopic intrapulmonary thyroid tumor should not be overlooked.
Keywords: ectopic, thyroid microfollicular adenoma, pulmonary nodules, tumor metastases
1. Introduction
Ectopia thyroid tissue is a rare clinically condition with an estimated prevalence of 1/100,000 to 300,000 in the general population, increasing to 1/4,000 to 8,000 in patients with thyroid dysfunction.[1] It occurs as a result of a developmental abnormality during the migration of the thyroid anlage from the floor of the primitive foregut to its final position in the neck.[2] A vast majority (90%) of ectopic thyroids are found typically along the pathway of embryologic migration of thyroid tissue, while around 10% are found in other anatomical locations including the heart, aorta, lung, mediastinum, esophagus, gallbladder, duodenum, and adrenal glands.[3] To our knowledge, only 3 cases of ectopic intrapulmonary thyroid have been reported in the literature. And no case of ectopic intrapulmonary thyroid microfollicular adenoma has been reported. In this paper, a case of a 76-year-old female with ectopic thyroid microfollicular adenoma in the lung is reported.
2. Informed consent
Informed written consent was obtained from the patient to publicize this case report and corresponding images.
3. Case presentation
A female patient at the age of 76 was admitted to our hospital due to a 2-hour transient unconsciousness. Her medical history was unremarkable, and she did not show any symptoms of hypothyroidism or hyperthyroidism. No pulmonary symptoms, such as coughing, hemoptysis, and dyspnea were observed. No abnormality was found during thyroid palpation inspection. Results of thyroid function tests (free T3, free T4, and thyroid-stimulating hormone (TSH)) were within normal range. Pelvic ultrasound (US) showed a range of 13.3 × 7.9 cm, a well-defined cystic lesion with dense septations. Meanwhile, solid papillary protuberance and blood flow signals were seen in part of cysts. Thickened endometrium and multiple uterine small cysts were detected in US. Magnetic resonance imaging (MRI) showed multiple well-defined cystic mass in pelvic without obvious enhancement (Fig. 1). It appeared hypointense on T1WI, hyperintense on T2WI, and hypointense on DWI. Later on, the patient underwent laparoscopic double adnexectomy and hysterectomy. Pathological description revealed bilateral ovarian serous cystadenoma and endometrioma.
Figure 1.
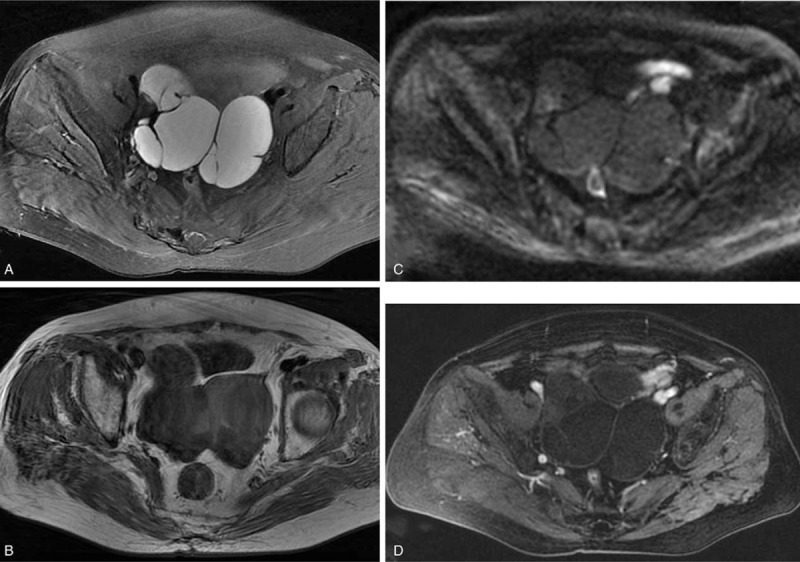
Pelvic MRI showed multiple well-defined cystic mass. It appeared hyperintense on T2WI (A), hypointense on T1WI (B), hypointense on DWI (C) without obvious enhancement (D).
Chest CT scan showed multiple well-defined, solid nodules in bilateral pulmonary (Fig. 2), of which the largest was located in the lower-left lung at 2.7 × 2.3 × 1.8 cm (Fig. 3). High attenuation (51 Hounsfield units (HU)) was shown on a nonenhanced chest CT image and strong enhancement (114 HU) on a contrast-enhanced chest CT. Blood-supply vessels were observed around the nodule. The remaining 5 smaller nodules scattered in both lungs and were also enhanced remarkably. No enlarged lymph nodes were observed. To rule out the metastasis of pelvic tumor, CT-guided fine-needle aspiration cytology (FNAC) and core biopsy were performed at the largest nodule with the histologic diagnosis of ectopic thyroid microfollicular adenoma (Fig. 4). In view of the age and physical conditions of the patient, it is unanimously decided by the physicians and family members of the patient to closely follow-up the benign pulmonary lesion.
Figure 2.
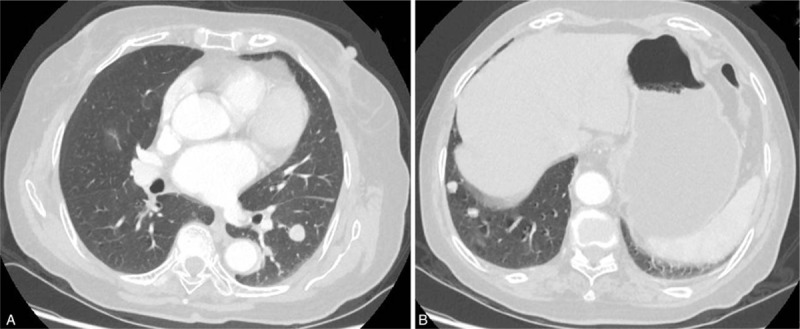
On lung window images of the chest CT scan, a 14-mm-sized, well-defined, round nodule was observed in the posterior basal segment of the left lower lobe (A). Two 10-mm and 7-mm-sized, well-defined, round nodules were observed in anterior basal segment of the right lower lobe (B).
Figure 3.
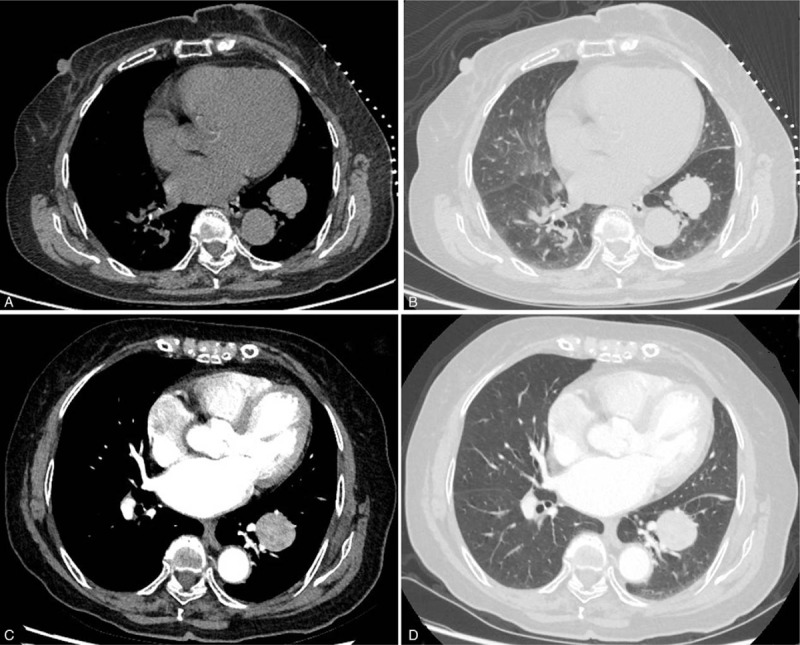
Chest CT scan showed a well-defined nodule in the lower left lung measuring 2.7 × 2.3 × 1.8 cm. The nodule was high attenuation (51 HU) on nonenhanced images (A, B) and showed strong enhancement (114 HU) (C, D).
Figure 4.

Histopathology showed thyroid microfollicular pattern in pulmonary nodule (hematoxylin and eosin, 40× magnification). The uniform follicles and follicular epithelial cells with small, round non-overlapping nuclei.
The patient was asymptomatic and euthyroid after being discharged from the hospital. During the 12-month follow-up, no pelvic tumor recurrence or metastasis was found. CT review of pulmonary nodules after 3 months, 6 months, and 12 months also showed no remarkable changes.
4. Discussion
To our knowledge, this is the first reported case of ectopic thyroid microfollicular adenoma in lung. As a subtype of follicular adenoma, thyroid microfollicular adenoma is a kind of benign tumor with good prognosis. Ectopic intrapulmonary thyroid microfollicular adenoma is extremely rare and easily confused with primary pulmonary nodules or metastatic tumor.
Ectopic thyroid tissue may occur at any age but is particularly observed during childhood, adolescence, and around menopause. Females are more vulnerable than males with a ratio of 4:1.[4] Clinically, the majority of patients with thyroid ectopia are a symptom, making an accurate diagnosis more challenging. In this case, the patient was an euthyroid, asymptomatic, elderly female with the incidental discovery of pulmonary nodules.
After reviewing previous literature, it is discovered that benign or malignant transformation of ectopic thyroid tissue is not common, though with few cases reported, such as follicular adenoma[5] and thyroid carcinomas.[6] Therefore, they should be taken into account when making a differential diagnosis. For such infrequent manifestation, the choice of appropriate diagnostic approach is also challenging. Radiological imaging examinations are available and noninvasive tools. US is helpful in confirming the site and morphology of thyroid. CT and MRI are valuable in identifying the site of ectopic tumor, especially when it is distant from the descending pathway of the thyroid.[7] FNAC provides considerable assistance in confirming the diagnosis of ectopic thyroid tissue. FNAC is the only approach to differentiate benign and malignant nodules.[8]
It is also highlighted in this case that the patient had bilateral ovarian serous cystadenoma synchronously. Ryu HS[9] had described a case of ectopic intrapulmonary thyroid mimicking multiple pulmonary metastases from an endometrioid adenocarcinoma of the uterus. Coincidentally, the intrapulmonary nodules in our case were also mistakenly considered as pelvic tumor metastases at first. Based on the common features of both cases, further researches should be made on whether there is a correlation between pelvic tumor and ectopic intrapulmonary thyroid/thyroid tumor. This is just the assumption, and further research should be guaranteed to confirm its veracity.
Ectopic thyroid microfollicular adenoma in the lung is extremely rare and may be easily mistaken for pulmonary metastases from other sites. As proved in this case, ectopic intrapulmonary thyroid tumor should not be overlooked clinically.
Footnotes
Abbreviations: CT = computed tomography, FNAC = fine-needle aspiration cytology, HU = Hounsfield units, MRI = magnetic resonance imaging, TSH = thyroid stimulating hormone, US = ultrasound.
WZ and HZ contributed equally to this work.
Details of the patient are available in the hospital notes for the Editor-in-chief of this journal for review.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor of this journal.
The authors have no conflicts of interests to disclose.
References
- [1].Matta-Coelho C, Donato S, Carvalho M, et al. Dual ectopic thyroid gland. BMJ Case Rep 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Guerra G, Cinelli M, Mesolella M, et al. Morphological, diagnostic and surgical features of ectopic thyroid gland: a review of literature. Int J Surg 2014;12Suppl 1:S3–11. [DOI] [PubMed] [Google Scholar]
- [3].Mysorekar VV1, Dandekar CP, Sreevathsa MR. Ectopic thyroid tissue in theparotid salivary gland. Singapore Med J 2004;45:437–8. [PubMed] [Google Scholar]
- [4].Regal M, Kamel MM, Alyami H, et al. Mediastinal ectopic thyroid mass with normal thyroid function andlocation: case report. Int J Surg Case Rep 2018;52:5–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Raskin A, Castro-Dominguez Y, Mirani N, et al. Incidental ectopic thyroid follicular adenoma on myocardial perfusion imaging. J Nucl Cardiol 2016;23:153–4. [DOI] [PubMed] [Google Scholar]
- [6].Lianos G, Bali C, Tatsis V, et al. Ectopic thyroid carcinoma. Case report. G Chir 2013;34:114–6. [PMC free article] [PubMed] [Google Scholar]
- [7].Noussios G, Anagnostis P, Goulis DG, et al. Ectopic thyroidtissue: anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol 2011;165:375–82. [DOI] [PubMed] [Google Scholar]
- [8].Kousta E, Konstantinidis K, Michalakis C, et al. Ectopic thyroid tissue in the lower neck with a coexisting normally located multinodular goiter and brief literature review. Hormones (Athens) 2005;4:231–4. [DOI] [PubMed] [Google Scholar]
- [9].Ryu HS, Chung YJ, Chong, et al. Ectopic intrapulmonary thyroid tissue mimicking metastatic tissue. Thyroid 2012;22:755–9. [DOI] [PubMed] [Google Scholar]