

Abstract
BACKGROUND:
This study was undertaken to ascertain the current magnitude and causes of blindness and visual impairment in persons aged 50 years and over and to assess the impact of a 10-year eye care program in Sokoto State, Nigeria.
METHODS:
A rapid assessment of avoidable blindness (RAAB) survey (in persons 50 years and over) was conducted in 2016. Participants were selected in Wurno health zone using a two-stage cluster randomized sampling with probability proportional to size. Operational definitions were based on RAAB and World Health Organization eye examination record definitions. Eye care program documents were reviewed and data from a baseline survey undertaken in 2005 were reanalyzed.
RESULTS:
A response of 89.1% (2405 of 2700 participants) was obtained in the 2016 survey. With available correction, the unadjusted prevalence of blindness was 7.7% (95% confidence interval [CI]: 6.4, 8.9). The odds of blindness were 1.8 times higher in females than males (95% CI: 1.3, 2.4; P < 0.001). Major causes of blindness were cataract (48.9%) corneal disease (20.1%), glaucoma (10.3%), and uncorrected refractive error/aphakia (8.7%). The age- and sex-adjusted prevalence of blindness has declined from 11.6% (95% CI: 7.4, 17.0) in 2005 to 6.8% (95% CI: 5.6, 8.0%) in 2016.
CONCLUSION:
The blindness prevalence is high, and the major causes are avoidable in the health zone. The findings suggest that investments in the program over the last 10 years might have led to almost a halving in the prevalence of blindness in th e population. However, the small sample size of persons 50+ years from Wurno zone in the 2005 survey necessitate caution when comparing the 2005 and the 2016 surveys.
Keywords: Avoidable blindness, eye care, impact, rapid assessment of avoidable blindness
Introduction
The World Health Organization (WHO) Prevention of Blindness Programme Global Action Plan 2014–2019 recommends generating evidence on the magnitude and causes of blindness and visual impairment for advocacy, planning, and to monitor changes in the eye health of a population.[1]
An eye care program based on the VISION 2020-Right to Sight strategy was implemented between 2005 and 2014 in Sokoto State, Nigeria, by the Ministry of Health in collaboration with Sightsavers, UK. The number of eye health workforce, infrastructure, equipment, and access to affordable eye care services was improved in the 23 local government areas (LGAs) that are grouped into four administrative health zones[2] as described in a related publication.[3]
Prior to the onset of the eye care program in 2004, the Sokoto State Ministry of Health had one eye clinic with six ophthalmic nurses (ONs) providing secondary eye care services within the state capital. There was ophthalmologist or optometrist. Cataract services were provided through occasional cataract surgical camps by visiting teams from within and outside Nigeria. By 2014, there were six ophthalmologists, two optometrists, and 36 ONs. Cataract surgery was subsidized through a grant from Sightsavers.
In 2005, a baseline survey covering the four health zones of Sokoto State reported an all-age prevalence of blindness of 1.9% with cataract-related causes accounting for 72.5% of all blindness.[4]
This study was conducted to generate data for advocacy and planning of future eye care services and to assess the impact of the 10-year program on blindness and visual impairment in Wurno health zone of Sokoto State, Nigeria. This zone had the poorest eye health indices in the 2005 baseline survey. Wurno health zone comprises six LGAs, namely Kware, Rabah, Wurno, Goronyo, Sabon Birni, and Isa, with an estimated total population of 1,143,788 in 2016.
Methods
Study design
A cross-sectional rapid assessment of avoidable blindness (RAAB) survey of persons 50 years and over was conducted in Wurno health zone of Sokoto State, Nigeria, in June and July 2016. The study clusters were selected based on two-stage cluster randomized sampling with probability proportional to size.
Sample size determination 2016 survey
A minimum sample size of 2706 persons was calculated using the RAAB software based on an estimated blindness prevalence of 10% in persons 50 years and over in Wurno health zone using data from the 2005 study, a target population of 108,806, worst acceptable estimate of 15% (precision of 1.5), 95% confidence interval (CI), design effect of 1.6 for a cluster size of 60, and nonresponse of 10%.
Sampling technique
A randomized two-stage cluster sampling strategy was used. In the first stage, 45 clusters were selected from a sampling frame consisting of towns/villages located in the study local government areas (LGAs) using probability proportional to size sampling. In the second stage, compact segment sampling was used to select households in each cluster. A segment was defined as an area comprising 600 persons based on the expected number of persons aged 50 years and over (9.5%) in Sokoto State.[5] All persons aged 50 years and above in each household were enumerated until the desired cluster size of 60 was attained.
Survey teams and training
Two survey teams were trained by a certified RAAB survey trainer. An interobserver agreement of at least 0.7 was obtained between the two teams in visual acuity (VA) measurement, lens assessment, and determining causes of blindness and visual impairment. The first study cluster was jointly conducted with the trainer.
Data collection and analysis
After obtaining permission from the head of household and consent from each participant; the name, age, and gender of eligible participants in each household were recorded into the Android-based mRAAB software (Peek Vision Ltd, Hertfordshire, England).
VA was measured with a single optotype tumbling E card using standard techniques.[6] Eyes that could not see 6/18 with available correction were retested with a pinhole. The eye examination was based on the standard RAAB techniques using a ×2.5 magnifying loupe and a direct ophthalmoscope with pupillary dilation where ocular media opacity obscured the fundus view. The cause of visual impairment (<6/18) for each eye was assessed based on the coding instructions for WHO/PBL eye examination record.[7] All findings during the RAAB survey were documented in the mRAAB software and checked by the ophthalmologist. Data were analyzed using the RAAB software, which uses the WHO categories of visual impairment. CIs, odd ratios, and tests of statistical significance were calculated using Stata 14®software (StataCorp LP, Texas).
2005 survey data analysis
The 2005 survey consisted of 4848 examined participants of all ages from the four health zones selected by stratified cluster sampling.[4] The data of 190 participants aged 50+ years from Wurno health zone were reanalyzed to obtain estimates for the prevalence of blindness and visual impairment using Stata 14®software.
Using the available 2006 census data for age-sex distribution in Sokoto State, age-sex-adjusted prevalence estimates were calculated with RAAB analysis software.
Review of documents
The Sokoto State eye care programme project document 2005,[2] annual reports, and an Evaluation Report of the eye care Programme 2014[8] were reviewed. The data extracted included the number and cadre of eye health workforce, the infrastructure, and service delivery reports as reported in a sister publication.[3]
Ethical considerations
Ethical committees at the London School of Hygiene and Tropical Medicine and the Sokoto State Ministry of Health granted approval for the study. Verbal consent was obtained from the participants during enumeration, and the rights of individuals to participate or refuse were explained to participating communities.
Results
2016 rapid assessment of avoidable blindness survey
Out of 2700 persons enumerated, 89.1% (2405) were examined, with 54.2% were male. There were 63 refusals, 16 not capable of examination and 216 not available after one repeat visit. The composition of the study sample differed from the target population as it underrepresented persons aged 50–59 years and overrepresented the 60–69 age group [Figure 1].
Figure 1.
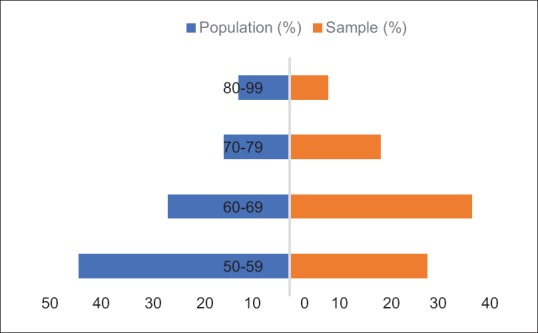
Age group distribution of the target population and study sample, Wurno health zone 2016
Prevalence of blindness and visual impairment
The unadjusted prevalence of blindness with available correction was 7.7% (95% CI: 6.4, 8.9), severe visual impairment 4.7% (95% CI 3.9, 5.6,), and moderate visual impairment 12.6% (95% CI 11.0, 14.3) [Table 1]. Females were 1.8 times (95% CI: 1.3, 2.4; P < 0.001) more likely to be blind than males. The prevalence of blindness increased with each decade of age between 50 and 80 years, from 2.2% to 5.7% to 14.6% to 20.1% (P < 0.001). The age- and sex-adjusted prevalence of blindness was 6.8% (95% CI: 5.6%, 8.0%) [Table 2]. The prevalence of unilateral blindness with available correction was 16.6% (95% CI: 15.0, 18.0).
Table 1.
Unadjusted prevalence of blindness and visual impairment with available correction in Wurno health zone, 2016
| 95% CI |
|||
|---|---|---|---|
| Males (%) | Females (%) | Total (%) | |
| Blindness prevalence (years) | |||
| 50-59 | 2.8 (0.8-4.8) | 1.3 (0.6-3.3) | 2.2 (0.5-3.5) |
| 60-69 | 3.6 (0.8-5.6) | 8.1 (1.3-11.0) | 5.7 (0.7-7.4) |
| 70-79 | 10.3 (1.9-14.8) | 18.8 (2.5-24.2) | 14.5 (1.6-18.0) |
| 80+ | 19.0 (3.8-27.9) | 21.2 (4.1-30.6) | 20.1 (2.8-26.3) |
| Overall blindness | 5.8 (4.5-7.1) | 9.8 (7.9-11.7) | 7.7 (6.4-8.9) |
| Moderate visual impairment | 10.1 (8.1-12.2) | 15.6 (13.4-17.9) | 12.6 (11.0-14.3) |
| Severe visual impairment | 4.7 (3.5-5.8) | 4.8 (3.9-5.8) | 4.7 (3.9-5.6) |
CI: Confidence interval
Table 2.
Age-sex-adjusted prevalence of blindness and visual impairment with available correction; Wurno health zone in 2005 and 2016
| WHO visual impairment category | 95% CI |
|||||
|---|---|---|---|---|---|---|
| 2005 |
2016 |
|||||
| Males (%) | Females (%) | Total (%) | Males (%) | Females (%) | Total (%) | |
| Normal | 55.2 (46.7-63.5) | 53.2 (38.2-67.6) | 54.7 (47.6-61.6) | 80.4 (78.2-82.5) | 73.5 (70.7-76.1) | 77.3 (75.5-78.9) |
| MVI | 17.5 (11.6-24.7) | 25.5 (13.9-40.3) | 19.5 (14.1-25.8) | 9.6 (7.6-11.7) | 13.9 (11.7-16.2) | 11.4 (9.8-13.1) |
| SVI | 15.4 (9.9-22.4) | 10.6 (3.5-23.1) | 14.2 (9.6-20.0) | 4.1 (3.0-5.3) | 4.5 (3.5-5.5) | 4.3 (3.5-5.1) |
| Blindness | 11.9 (7.1-18.3) | 10.6 (3.5-23.1) | 11.6 (7.4-17.0) | 5.9 (4.6-7.2) | 8.1 (6.2-10.0) | 6.8 (5.6-8.0) |
MVI: Moderate visual impairment, SVI: Severe visual impairment, CI: Confidence interval, WHO: World Health Organization
The main causes of blindness and visual impairment
The leading causes of blindness in 2016 were cataract-related (62%), cornea-related diseases (20.1%), and glaucoma (10.3%) [Table 3]. Treatable cataract (43.0%) and uncorrected refractive error (30.2%) were responsible for 73% of all causes of bilateral visual loss between (<6/18 – no perception of light). In the population aged 50 years and over, 95.8% of people had uncorrected presbyopia. The major causes of unilateral blindness were cataract (47.6%; 364 of 764), phthisis bulbi (9.2%), glaucoma (7.1%), cataract-intervention related complications (5.0%), and trachomatous corneal opacity (4.3%).
Table 3.
Principal causes of blindness and visual impairment with available correction; Wurno health zone 2016
| Cause | WHO category of visual impairment |
|||
|---|---|---|---|---|
| MVI: <6/18-6/60, n (%) | SVI: <6/60-3/60, n (%) | Blind: <3/60-NPL, n (%) | All VI/BL: <6/18-NPL, n (%) | |
| Cataract | 105 (34.5) | 64 (56.1) | 90 (48.9) | 259 (43.0) |
| Uncorrected refractive error | 160 (52.6) | 19 (16.7) | 3 (1.6) | 182 (30.2) |
| Nontrachoma corneal opacity | 5 (1.6) | 7 (6.1) | 20 (10.9) | 32 (5.3) |
| Glaucoma | 5 (1.6) | 3 (2.6) | 19 (10.3) | 27 (4.5) |
| Uncorrected aphakia | 4 (1.3) | 7 (6.1) | 13 (7.1) | 24 (4.0) |
| Cataract surgical complications | 5 (1.6) | 3 (2.6) | 11 (6.0) | 19 (3.2) |
| Trachoma | 5 (1.6) | 2 (1.8) | 10 (5.4) | 17 (2.8) |
| Phthisis bulbi | 0 | 0 | 7 (3.8) | 7 (1.2) |
| Macular degeneration | 4 (1.3) | 1 (0.9) | 0 | 5 (0.8) |
| Diabetic retinopathy | 0 | 0 | 1 (0.5) | 1 (0.2) |
| Others | 10 (3.3) | 8 (7.0) | 11 (3.6) | 29 (4.8) |
| Total | 304 (100) | 114 (100) | 184 (100) | 602 (100) |
VI: Visual impairment, MVI: Moderate VI, SVI: Severe VI, BL: Blindness, NPL: No perception of light, WHO: World Health Organization
Prevalence and causes of functional low vision
Functional low vision, defined as a corrected VA of <6/18 to perception of light caused by an irreversible condition, had a prevalence of 4.2% (95% CI: 3.4, 5.0). The major causes were glaucoma (18%) and trachoma (13%).
2005 survey data analysis
There were 190 persons aged ≥50 years from Wurno health zone examined in the 2005 survey, 22 of whom were blind, giving a prevalence estimate of 11.6% (95% CI, 7.4, 17.0) and a further 27 and 37 (14.2% and 19.5%) were severely and moderately visually impaired, respectively [Table 2].
Comparison of 2005 and 2016 survey results in Wurno health zone
Comparing the age- and sex-adjusted findings of the 2016 RAAB with the estimates for the 2005 study, suggests an increase in the proportion of persons aged 50 years and over without visual impairment from 54.7% in 2005 to 77.3% in 2016 (P < 0.001) [Figure 2]. The prevalence of blindness declined from an estimated 11.6% to 6.8%, severe VI from 14.2% to 4.3% and moderate VI from 19.5% to 11.4% [Table 2].
Figure 2.
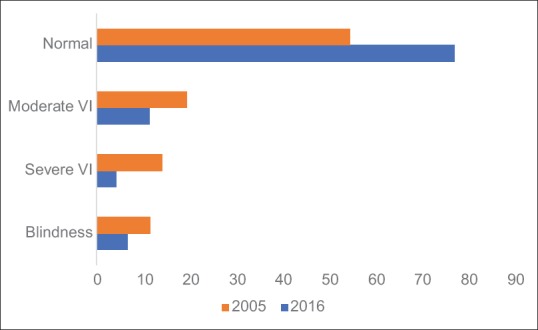
Distribution of the prevalence of visual impairment;Wurno health zone, 2005 and 2016
The age-adjusted prevalence of blindness for the total population (all ages) in Wurno health zone in 2005 was 2.0% (95% CI 1.3, 2.7), with 91% of all blind people being aged 50 years and over. Assuming that the proportion of all blindness in people 50 years and above is in the range 80%–90%, and given that persons 50 years and over now constitute 9.5% of the population, the estimated 2016 all-age prevalence of blindness in Wurno health zone is 0.71%–0.76%. This translates to a reduction in the estimated all-age blindness prevalence by more than a half from 2.0% in 2005 to approximately 0.75% in 2016.
The data extracted from the program documents indicated for Sokoto State an increase in the number of ophthalmologists from none in 2005 to six in 2014; ONs from 6 to 36 and two optometrists were recruited. In Wurno health zone, there is one facility providing regular cataract outreach surgery and four other eye clinics manned by ONs referring patients for cataract surgery. The cataract surgical coverage (VA <6/60) increased from 7.1% in 2005 to 62.1% in 2016 and the cataract surgical rate from 272 to 596 operations/million population during the study period as reported elsewhere.[3] The visual outcome of cataract surgery was good (6/18 or better) in 58% of pseudophakic eyes with available correction and this improved to 69% with pinhole correction.[3] Primary eye care was integrated into the primary health through legislation which provided access to primary health care workers who were trained as integrated eye care workers.
Discussion
General considerations
The high response rate (89%) gives confidence that the 2016 study findings are representative of the study population. However, the underrepresentation of the 50–59 years group in the 2016 survey may have overestimated the unadjusted prevalence of blindness.
Caution is required when comparing the 2005 and the 2016 surveys because of the very small sample size of persons 50 years and over in the 2005 study. However, this is the best available comparator.
The crowding phenomenon may have affected VA measurement with the Snellen's charts used in 2005, unlike the single optotype charts used in the 2016 study.
Results in 2016
The prevalence of blindness in the population 50 years and above in the RAAB survey was higher than the Nigerian national average (6.1%),[9] Madagascar (2.0%),[10] Burundi (1.1%),[11] Kenya (2.0%)[12] and Rwanda (1.8%).[13] It is also higher than that reported in Saudi Arabia (2.6%),[14] and India (3.6%)[15] and the Global Burden of Disease estimate for Sub-Saharan Africa (5.1%).[16] We expected poorer eye health indices in this health zone because of its fewer eye care facilities and difficult terrain which may explain the higher prevalence of blindness.
There was a higher prevalence of blindness in females, as reported in other studies from Nigeria[9] India (2.9% vs. 4.1%),[15] and Qatar (0.7% vs. 2.3%).[17] This was not surprising as females are less likely to access eye care services due partly to the dominant male culture of the population where permission must be granted to access services and women are more likely to be blind from trachoma. The results also support existing literature that blindness prevalence increases with age across both genders[16] as most causes of blindness are age-related.
The causes of blindness in this study are comparable to findings or estimates in the WHO African subregion,[11,12,18,19] as the leading causes are cataract, glaucoma, and corneal opacities. The leading causes of blindness in the population are avoidable.[20]
Given the burden of uncorrected refractive errors and presbyopia, a review of optical services provision with supportive eye health education is needed. Optical services should be made available in district hospitals through trained eye staff. Task shifting to ONs for management of presbyopia could improve access and uptake of optical services in the population.[21]
Glaucoma-related blindness/visual impairment is underestimated as visual fields were not assessed in this study. The findings highlight the increasing importance of glaucoma and the need to develop strategies focused on early glaucoma detection and treatment.[22] A one-off treatment strategy that can provide an effective, safe, affordable, and acceptable care has been recommended, especially for the Africa context.[23]
Trend over 10 years
The result of this study suggests an increase in the proportion of the population 50 years and above with normal vision (6/6-6/18) from 55% in 2005 to 77% in 2016, with a corresponding decrease in the overall prevalence of blindness. This improvement in eye health was most probably achieved through the development of human resources for eye care, improvement in infrastructure, appropriate technology, and supplies that have supported the eye care service to control blinding diseases, with special focus on cataract surgical services. Primary eye care has been integrated into the state primary health-care system and eye care has budgetary provision in the Sokoto State Ministry of Health annual plan; this development will potentially further decrease the magnitude of blindness and visual impairment in the population if provision of eye care services is sustained.
Use of rapid assessment of avoidable blindness survey methodology
The findings of this study support the use of RAAB survey methodology in identifying changing trends in eye care service indicators and planning for future service provision. Similar trends have been documented in Paraguay with a decline in blindness rate from 3.1% in 1999 to 1.1% in 2011;[24] in Oman from a national prevalence of 10.3% in 2005–7.5% in some Omani governorates by 2010;[25] and in the Gambia from a national prevalence of 0.7% to 0.42% from 1986 to 1996.[26]
Conclusion
The study found that the prevalence of blindness in the population aged 50 years and above in Wurno health zone of Sokoto State was 7.7%, being 9.8% in females and 5.8% in males; the leading causes of blindness and visual impairment were treatable. The result of this study has shown that investment in the Sokoto State eye care programme over the last 10 years has improved the vision and eye health status of the study population with 77.3% of people aged 50 years and above having normal VA in 2016 compared to 54.7% in 2005. This survey has provided information for advocacy with policy-makers on the benefits derivable from investing in eye care. It also provides important information for planning eye care in Sokoto State for the next 5–10 years.
Financial support and sponsorship
The study was financially supported by Sightsavers UK and Commonwealth Eye Health Consortium/The Queen Elizabeth Diamond Jubilee Trust.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors acknowledge the support received from Clare Gilbert and the Sokoto State Ministry of Health for this study and also like to thank the study participants and team members for their support.
References
- 1.World Health Organization. Universal Eye Health – A Global Action Plan 2014-19. World Health Organization. 2014:28. [Google Scholar]
- 2.Sightsavers International Kaduna Nigeria. Sokoto State Eye Care programme Project Document 2005 – 2009. Sightsavers International Kaduna Nigeria. 2005:48. [Google Scholar]
- 3.Muhammad N, Adamu MD, Caleb M, Maishanu NM, Jabo AM, Rabiu MM, et al. Changing patterns of cataract services in North-West Nigeria: 2005-2016. PLoS One. 2017;12:e0183421. doi: 10.1371/journal.pone.0183421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Muhammad N, Mansur RM, Dantani AM, Elhassan E, Isiyaku S. Prevalence and causes of blindness and visual impairment in Sokoto state, Nigeria: Baseline data for vision 2020: The right to sight eye care programme. Middle East Afr J Ophthalmol. 2011;18:123–8. doi: 10.4103/0974-9233.80700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.2006 National and State Population and Housing Tables – Priority Tables I. Abuja, Nigeria: National Population Commission; 2010. National Population Commission; p. 347. [Google Scholar]
- 6.Kuper H, Polack S, Limburg H. Rapid assessment of avoidable blindness. Community Eye Health. 2006;19:68–9. [PMC free article] [PubMed] [Google Scholar]
- 7.World Health Organization. Coding Instructions for the WHO/PBL Eye Examination Record (version III) Geneva: World Health Organization; 1988. p. 1. [Google Scholar]
- 8.Abiose A, Tureta S, Alhassan M, Adekeye O. Strategic Evaluation of the Sokoto State Eye Care Programme, Nigeria Sight Savers Supported from 2005-2014. Kaduna Nigeria: Sightsavers; 2014. p. 73. [Google Scholar]
- 9.Kyari F, Gudlavalleti MV, Sivsubramaniam S, Gilbert CE, Abdull MM, Entekume G, et al. Prevalence of blindness and visual impairment in Nigeria: The National Blindness and Visual Impairment Study. Invest Ophthalmol Vis Sci. 2009;50:2033–9. doi: 10.1167/iovs.08-3133. [DOI] [PubMed] [Google Scholar]
- 10.Randrianaivo JB, Anholt RM, Tendrisoa DL, Margiano NJ, Courtright P, Lewallen S. Blindness and cataract surgical services in Atsinanana region, Madagascar. Middle East Afr J Ophthalmol. 2014;21:153–7. doi: 10.4103/0974-9233.129767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kandeke L, Mathenge W, Giramahoro C, Undendere FP, Ruhagaze P, Habiyakare C, et al. Rapid assessment of avoidable blindness in two northern provinces of Burundi without eye services. Ophthalmic Epidemiol. 2012;19:211–5. doi: 10.3109/09286586.2012.690493. [DOI] [PubMed] [Google Scholar]
- 12.Mathenge W, Kuper H, Limburg H, Polack S, Onyango O, Nyaga G, et al. Rapid assessment of avoidable blindness in Nakuru district, Kenya. Ophthalmology. 2007;114:599–605. doi: 10.1016/j.ophtha.2006.06.057. [DOI] [PubMed] [Google Scholar]
- 13.Mathenge W, Nkurikiye J, Limburg H, Kuper H. Rapid assessment of avoidable blindness in Western Rwanda: Blindness in a postconflict setting. PLoS Med. 2007;4:e217. doi: 10.1371/journal.pmed.0040217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Al Ghamdi AH, Rabiu M, Hajar S, Yorston D, Kuper H, Polack S. Rapid assessment of avoidable blindness and diabetic retinopathy in Taif, Saudi Arabia. Br J Ophthalmol. 2012;96:1168–72. doi: 10.1136/bjophthalmol-2012-301874. [DOI] [PubMed] [Google Scholar]
- 15.Neena J, Rachel J, Praveen V, Murthy GV. Rapid Assessment of Avoidable Blindness India Study Group. Rapid assessment of avoidable blindness in India. PLoS One. 2008;3:e2867. doi: 10.1371/journal.pone.0002867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bourne RR, Flaxman SR, Braithwaite T, Cicinelli MV, Das A, Jonas JB, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob Health. 2017;5:e888–97. doi: 10.1016/S2214-109X(17)30293-0. [DOI] [PubMed] [Google Scholar]
- 17.Al Gamra H, Al Mansouri F, Khandekar R, Elshafei M, Al Qahtani O, Singh R, et al. Prevalence and causes of blindness, low vision and status of cataract in 50 years and older citizen of qatar-a community based survey. Ophthalmic Epidemiol. 2010;17:292–300. doi: 10.3109/09286586.2010.508350. [DOI] [PubMed] [Google Scholar]
- 18.Flaxman SR, Bourne RR, Resnikoff S, Ackland P, Braithwaite T, Cicinelli MV, et al. Global causes of blindness and distance vision impairment 1990-2020: A systematic review and meta-analysis. Lancet Glob Health. 2017;5:e1221–e1234. doi: 10.1016/S2214-109X(17)30393-5. [DOI] [PubMed] [Google Scholar]
- 19.Lindfield R, Griffiths U, Bozzani F, Mumba M, Munsanje J. A rapid assessment of avoidable blindness in Southern Zambia. PLoS One. 2012;7:e38483. doi: 10.1371/journal.pone.0038483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96:614–8. doi: 10.1136/bjophthalmol-2011-300539. [DOI] [PubMed] [Google Scholar]
- 21.Blanchet K, Gilbert C, de Savigny D. Rethinking eye health systems to achieve universal coverage: The role of research. Br J Ophthalmol. 2014;98:1325–8. doi: 10.1136/bjophthalmol-2013-303905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cook C. Chronic glaucoma case finding and treatment in rural Africa: Some questions and answers. Community Eye Health. 2001;14:43–4. [PMC free article] [PubMed] [Google Scholar]
- 23.Kyari F, Gilbert C, Blanchet K, Wormald R. Improving services for glaucoma care in Nigeria: Implications for policy and programmes to achieve universal health coverage. Br J Ophthalmol. 2017;101:543–7. doi: 10.1136/bjophthalmol-2016-310040. [DOI] [PubMed] [Google Scholar]
- 24.Duerksen R, Limburg H, Lansingh VC, Silva JC. Review of blindness and visual impairment in Paraguay: Changes between 1999 and 2011. Ophthalmic Epidemiol. 2013;20:301–7. doi: 10.3109/09286586.2013.821497. [DOI] [PubMed] [Google Scholar]
- 25.Khandekar R. Where are we in elimination of avoidable blindness after ten years of implementing 'VISION 2020 the right to the sight' in Oman? Oman J Ophthalmol. 2012;5:73–4. doi: 10.4103/0974-620X.99366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Faal H, Minassian DC, Dolin PJ, Mohamed AA, Ajewole J, Johnson GJ. Evaluation of a national eye care programme: Re-survey after 10 years. Br J Ophthalmol. 2000;84:948–51. doi: 10.1136/bjo.84.9.948. [DOI] [PMC free article] [PubMed] [Google Scholar]